
Abstract
Abstract
The treatment of persistent uterine bleeding in those patients who identify as transmasculine or nonbinary is often straightforward, but can be difficult in a subset of patients. This article reviews the physiology of the normal menstrual cycle and the hormonal influences on the endometrium, and then explores options for the treatment of persistent bleeding for people both already on testosterone and for those who are either not ready for or who do not desire testosterone.
Introduction
Uterine bleeding can be a source of distress in those for whom their gender identity is incongruent. Clinical experience shows that depressive symptoms and self-harming behaviors may peak during menstrual bleeding. Menstrual cycling is typically suppressible with hormonal therapy, although in a significant proportion of individuals it may persist. This review article addresses the most common treatment options for persistent uterine bleeding.
A normal menstrual cycle requires an intact hypothalamic–pituitary–gonadal axis and adequate estrogen and progesterone at the level of the endometrium. The hypothalamus secretes gonadotropin-releasing hormone (GnRH) in a pulsatile fashion; this causes release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the pituitary gland, which promote ovarian follicle development and estradiol secretion. At the level of the endometrium, estrogen's primary action is to promote growth while progesterone limits proliferation by stabilizing the glands and halting mitotic division. 1 Local uterine factors whose contributions are less clearly defined, including prostaglandins, nitric oxide, and others, are likely responsible for the variability in flow, volume, and duration of bleeding.2–4 The rapid decline in both progesterone and estrogen in the absence of a fertilized egg is the trigger for shedding of the lining of the uterus, but only if estrogen has been present. 1 The anovulatory uterus may be susceptible to erratic bleeding, which is thought to be due to insufficient levels of progesterone.
When considering hormonal manipulation to halt menstrual cycling it is important to obtain a menstrual history. A typical menstrual cycle is between 25 and 35 days, although just after menarche the range may be from 21 to 45 days. 4 Endometria of patients with menorrhagia may require a high dose, local form of progestogen (e.g., intrauterine device), whereas normally cycling patients may respond to a continuous low-dose oral progestin. 2 Additionally, when counseling patients it is critical to remember that there will be individual differences, even between people with regular menstrual cycles. Persistent bleeding despite adequate therapy should prompt consideration of alternate etiologies, including coagulation defects, thyroid disease, structural abnormalities (e.g., endometrial polyps), infection, trauma, and/or pregnancy. 5
We typically avoid giving any form of estrogen, as most often this is the hormone that most patients would like to avoid, however, the use of estrogen combined with progesterone is a highly effective way to stabilize the endometrium and avoid breakthrough bleeding; it remains a viable option for those who are not averse to taking it.
Testosterone
For those adolescents who have met criteria for gender-affirming hormone use, testosterone (T) is typically highly effective for induction and maintenance of amenorrhea within 6 months of its initiation, although may be effective as early as 1 month. 6 Greater than 90% of transmen using either biweekly intramuscular or weekly subcutaneous forms of testosterone achieve amenorrhea within 6 months (Table 1).6,7
T, testosterone.
Testosterone acts directly on the endometrium, causing both endometrial and vaginal atrophy as shown by examination of the endometria of transmen who had been on androgen therapy for at least 6 months. 8 Histological analysis of endometrial samples of transmen on testosterone for at least 1 year is similar to that of postmenopausal women. Both groups expressed similar levels of Ki-67, a marker of endometrial proliferation. 9 There is, however, controversy as some studies have shown an active endometrium and hypertrophic myometrium in some individuals. 10
While the effects of testosterone on the uterus itself are fairly clear, less is understood about its effects on the hypothalamus and pituitary. Reports of unplanned pregnancies while on testosterone support a lack of inhibition of ovulation in at least some individuals. 11
There does appear to be a dose-dependent amenorrheic response to T, which supports a trial of increased dose or frequency in cases of persistent bleeding. An increase of dose or dose frequency was shown by Nakamura et al. to be effective in inducing secondary amenorrhea. 6 The recommended therapeutic range for testosterone levels is 350–700 ng/dL. 12 However in conditions in which the sex hormone binding globulin levels may be low (e.g., obesity and polycystic ovarian syndrome) total testosterone levels may appear subtherapeutic while free testosterone levels are in the normal range for adult males. Current guidelines recommend monitoring total testosterone levels only. 12
Progestogens
Progestogens, comprised of natural, micronized progesterone and synthetic progestins, are an important class of medications for induction of amenorrhea in the transmasculine and nonbinary adolescent. They may be considered in the postmenarchal adolescent not yet ready for or desiring of masculinizing hormones, but may be less effective in inducting amenorrhea than combined oral contraceptive pills that contain estrogen. Progesterone and progestins are available in different formulations, including oral, injectable, implantable, and intrauterine (Table 2). In our practice we typically start with norethindrone or norethindrone acetate.
Progestogens exert most of their effects peripherally at the level of the endometrium primarily through changes in angiogenesis. Systemic forms at higher doses may also suppress the hypothalamic–pituitary–gonadal axis by inhibiting GnRH activity 13 and therefore induce hypothalamic amenorrhea. Both forms counteract the effects of estrogen by inhibiting the proliferation of the endometrium and reducing the mitotic rate of the glands and stromal tissue,14–16 through reduction of the estrogen receptors on the glands. 17 In normally menstruating women, exposure to a low-dose progestogen may cause disturbances in endometrial angiogenesis and cause low-volume irregular bleeding. 2 Prolonged use typically leads to endometrial atrophy. 18 Oral medroxyprogesterone has been used historically to suppress the hypothalamic–pituitary–gonadal axis and may be a more cost-effective option in some areas compared with GnRH agonist (GnRHa). 19 The progestin-only contraceptive pill norethindrone may inhibit ovulation in some women; although up to 40% of cis-females have been reported to continue ovulating. 20 Intrauterine levonorgestrel may lead to partial suppression of ovulation, but thought to act more locally at the endometrium. 21 Although ovulation may be disturbed to some extent, estradiol levels are normal limiting the concern for impact on bone health compared with injectable medroxyprogesterone. 22
With any of the progestogens, irregular and unpredictable bleeding is relatively common and may lead to discontinuation of the agent, particularly in the first few months of treatment. This is due to vascular changes in the endometrium rather than hormonal fluctuation. 23 Frequent and prolonged but light bleeding occurs in a large percentage of patients. 1 When classified by histological samples (pseudodecidualization and reduction of mitotic index), the most potent progesterone is medroxyprogesterone acetate. 24 There has, however, been concern about the long-term use of medroxyprogesterone acetate and bone health, first raised by Cundy et al. who reported a significant decrease in bone mineral density (6.6% at the femoral neck and 7.5% at the spine) compared with menopausal controls. 25 Other studies have supported this finding. In a large population-based study in Washington, Scholes et al. reported a 2.2% difference at the spine and 2.5% difference at the femoral neck compared with premenopausal controls. Eighteen to twenty-one year olds, however, had the most impact to their bone mineral density, on average 10.5% lower compared with controls. 26 This was a cross-sectional study and length of use ranged from 1 to 33 months. Consensus statements issued from the World Health Organization, the American Society for Adolescent Medicine, and others do not recommend avoidance of this agent. They do recommend counseling on advantages and disadvantages.27–29
Adverse effects of progestins include bone health concerns and androgenic effects of lower high-density lipoprotein cholesterol, fluid retention, headaches, and mood disturbance. Natural progesterones' side effects are limited to fatigue and sedation30–32 and should be taken at bedtime. A major benefit to this class of hormone is that there is no increased risk for thromboembolic events; it is recommended for contraception by the WHO even in individuals with a history of thrombosis and vascular disease. 33
For those minority of patients who are having continuous bleeding and are not averse to taking estrogen, a combination of micronized estrogen (Estrace 1.5 mg daily) for 25 days combined with continuous low-dose micronized progesterone (100 mg daily) has been shown to control endometrial proliferation, although this does not fully suppress mitotic activity. 14 This regimen may be more acceptable than a traditional combined oral contraceptive pill given continuously, which will achieve the same result. In practice, given its increased effectiveness over progestins in leading to menstrual suppression, a combined oral contraceptive pill may be amenable to some patients and is commonly used by some practitioners over progestins. Oral contraceptive pills containing first- and second-generation progestins have a higher androgenic profile and lower risk of venous thromboembolism and may be preferable preparations for this population compared with oral contraceptive pills containing later generation of progestins.
Aromatase Inhibitors
These agents inhibit Cytochrome P450 aromatase enzyme that converts testosterone to estradiol and androstenedione to estrone. This enzyme is active in peripheral tissues throughout the body, including skin, bone, brain, and adipose tissue. 34 Aromatase inhibitors (AIs) are used most often in hormone receptor–positive breast cancer in postmenopausal women. 35 They are also effective at increasing testosterone levels in cis-men. 36 In the pediatric population they have been used in hyperestrogenic states such as McCune–Albright syndrome, hyperandrogenic states such as familial male-limited peripheral puberty, pubertal gynecomastia, short stature, and/or pubertal delay in cis-gender males. 37
Third-generation AIs, including anastrozole and letrozole are the most potent, selective, and least toxic AIs available. These agents may be of particular benefit in the obese patient, as aromatase is highly expressed in adipocytes. In many obese trans-patients with low T, increasing the T levels may only serve to be converted to estradiol in adipocytes. 38 Although generally well tolerated, menopausal-like side effects may occur, including fatigue, headache, hot flashes, and vaginal dryness. The serum testosterone level is expected to increase and therefore there may be an increase in hematocrit, and decrease in high-density lipoprotein. In a growing adolescent there is a concern for adverse impact on bone health, decrease in height velocity, and delayed epiphyseal maturation. 36
Selective Estrogen Receptor Modulators
These agents interact with intracellular estrogen receptors in target organs as estrogen receptor agonists or antagonists in a tissue-specific manner. 39 Tamoxifen, the oldest member of this class, is a competitive inhibitor of estrogen at the breast, but an agonist in the endometrium. For this reason, there is a risk of endometrial hyperplasia, polyps, carcinoma, and uterine sarcoma as well as ovarian cysts, which is thought to be highest in postmenopausal cis-women. 40 Other side effects may include menopausal-like symptoms and increased risk of thrombosis. 39 For these reasons, these are not commonly used in the treatment of uterine bleeding in transmen.
Selective estrogen receptor modulators (SERMs) are typically used in infertility treatment, estrogen receptor–positive breast cancer, and in the prevention and treatment of osteoporosis in postmenopausal cis-women. 41 In the pediatric population SERMs have been used successfully for gynecomastia in adolescent cis-males.42,43 It has been used with limited clinical experience to help induce amenorrhea (personal correspondence, Norman Spack), which was inspired by a small cohort of McCune–Albright patients who demonstrated a reduction in vaginal bleeding.44,45
GnRH Agonists
GnRHa mimic the hypothalamic hormone GnRH; when given continuously they act as an inhibitor of the pituitary gonadotropins LH and FSH; they also cause downregulation of the GnRH receptors on the pituitary gland, thus affecting the downstream products of LH and FSH, or gonadal steroids (testosterone and estrogen). In practice, this is a highly effective way to halt production of estradiol or testosterone. GnRHa are available in intramuscular 1-, 3-, and 6-month formulations, as well as an intradermal capsule that typically is effective for greater than 1 year.
GnRHa are typically used in pediatrics for treatment of central precocious puberty 46 ; for adults they are used for the treatment of metastatic prostate cancer or other sex steroid-fueled malignancies. In the transgender population, they are commonly referred to as “puberty blockers” as they are used to halt and/or prevent development of secondary sexual characteristics of the assigned gender. 12
Side effects are primarily local and related to the type of insertion used, although there are concerns about bone health as this has been shown to decline in both transgirls and transboys on GnRHa. 47 When used in a precocious puberty population, there seem to be no long-term consequences on fertility or bone health. 48 In an individual who has already experienced puberty, and sex steroids (gender affirming or endogenous) are not present, people may experience symptoms similar to those seen in menopause such as hot flashes. We do not recommend routine use in patients who desire a prolonged agonadal state; the lack of sex steroids in these individuals is detrimental to bone health, as inferred by the observation that men without estrogen receptors and those with very delayed puberty have poor bone health.49,50
Hysterectomy
Performed with or without salpingectomy/oophorectomy, this is a definitive option for the elimination of uterine bleeding. Hysterectomy may be performed abdominally, laparoscopically, robotically, or transvaginally. 51 Current guidelines set forth by the World Professional Association for Transgender Health recommend persistent, well-documented gender dysphoria, the capacity to make a fully informed decision and consent to treatment, well-controlled mental health or medical concerns if significant, and 1 year of gender-affirming hormones unless not desired or medically contraindicated for the individual. 51 Additionally it is recommended that the patient be the age of majority and have two letters of referral from mental health professionals. 52 The Endocrine Society Practice Guidelines recommend the risks and benefits be evaluated by the individual. 12 In the National Transgender Discrimination Survey, 21% of transmen surveyed had undergone hysterectomy, 58% desired a hysterectomy at some time in the future, and 21% had no desire for a hysterectomy. 53
Conclusion
Management of uterine bleeding is vital for the mental health of the transmasculine or nonbinary patient who desires amenorrhea. Our typical work flow is presented in Figure 1. Progestogens may be initiated early in medical transition if they are not ready for or not desiring testosterone. If, while on testosterone amenorrhea is not achieved, a trial of an increased dose or change in dose frequency is usually the first step. For persistent bleeding, particularly in the obese individual, a trial of an AI may be beneficial. Other options remain viable, but a decision to utilize them must be the result of an informed discussion and consent between the treating physician and patient.
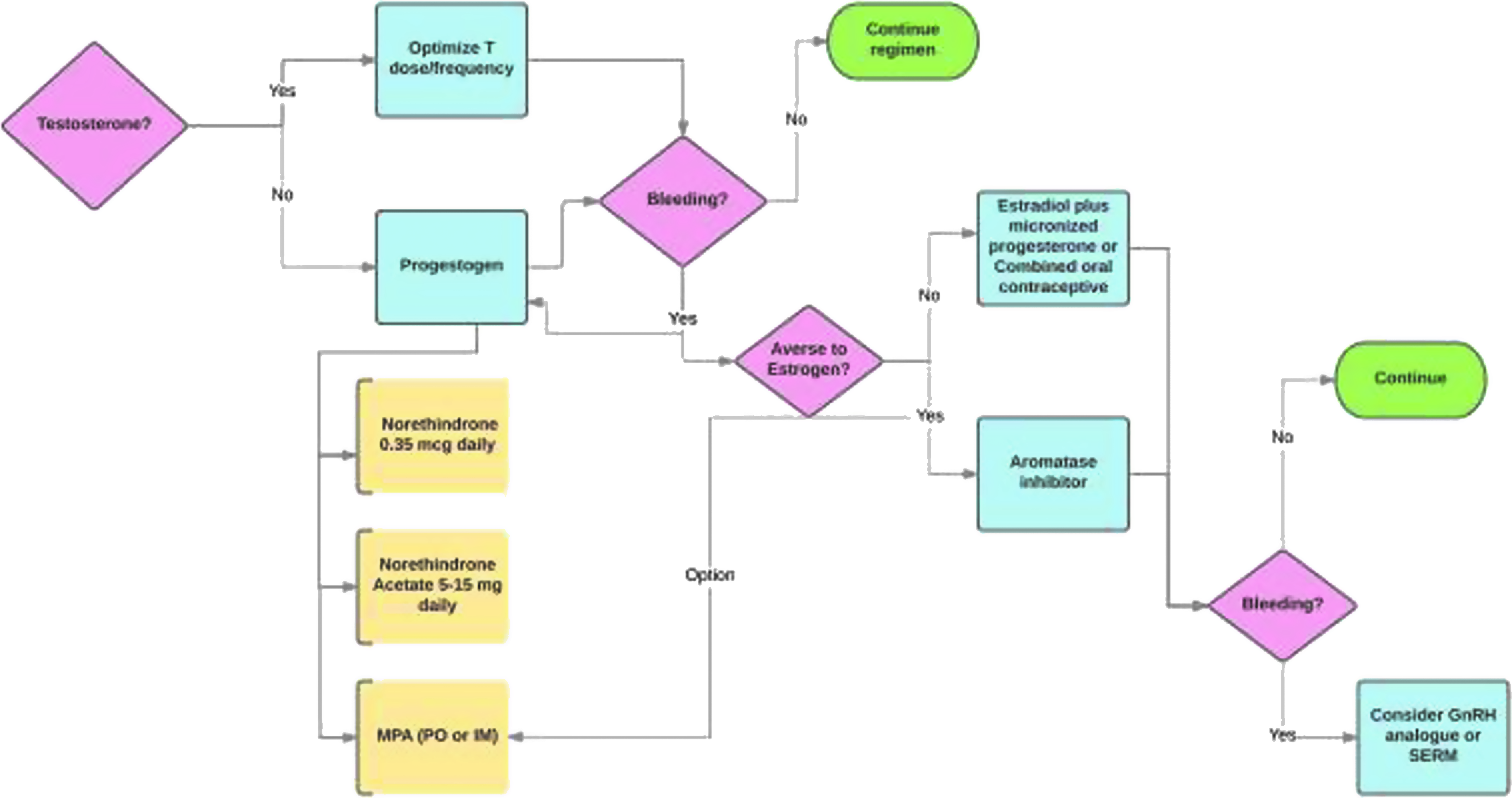
A simplified flowchart for inducing and maintaining amenorrhea. SERM, selective estrogen receptor modulators.
Footnotes
Acknowledgment
The authors would like to thank Norman Spack, MD, for his expert guidance, patience, and wisdom in treating adolescent patients and imparting his knowledge.
Author Disclosure Statement
No competing financial interests exist.