
Abstract
Background:
With the growing adoption of telehealth in allied health disciplines, establishing clear training and education standards is crucial. This review aims to map the current training and education that has been delivered to support development of telehealth competencies in allied health professionals. This scoping review extends our previous review with an updated search.
Methods:
The Population Concept Context framework was used, and the following databases were searched: MEDLINE, CINAHL, PsychInfo, Cochrane, EMBASE, Web of Science, PEDro, United Kingdom Health Forum, WHO, Health Education England, and all U.K. and Australian Allied Health Profession (AHP) professional bodies.
Results:
Out of 1,05,980 articles, 12 met the inclusion criteria. Training and education differed greatly, with no definite pattern in teaching approaches. Three articles used standardized questionnaires for training and education assessment, while the remaining articles used author-designed assessments. Eight articles reported that participants achieved the targeted telehealth competencies, and five reported improved attitudes toward telehealth following training and education. Articles recommended various factors that may improve telehealth training and education outcomes, which included a combination of online and face-to-face methods, interprofessional training, consolidation of their skills through supervised clinical work, and separating video and telehealth competencies.
Discussion:
This scoping review represents the first comprehensive exploration of telehealth training and education across allied health disciplines. While articles yielded generally positive outcomes, the absence of standardized methods prompts questions about its efficacy. Research should focus on developing evidence-based curriculums informed by pedagogic practices tailored to allied health needs.
Introduction
Background
The term telehealth refers to the delivery of health care services using information and communication technologies for assessment, management, and prevention of health-related conditions. 1 Relatively rapid improvements in technology during the Information Age and Fourth Industrial Revolution have enabled increasingly sophisticated interactions between service providers and users. However, there is significant variability in utilization of telehealth within, and between, the respective Allied Health Professions (AHPs). 2 The utilization of telehealth as a delivery mode, alongside and integrated with in-person services, will continue to evolve over time, particularly as technologies mature and the broad benefits of telehealth including convenience and increased service availability are recognized by both service users and AHPs.
The continued implementation and development of telehealth services requires support from all stakeholders connected to health service delivery. At a health service organization level, these include ensuring the AHP workforce possesses the required skills, knowledge, and behaviors to provide safe, efficient, and effective telehealth services, underpinning by a clear strategy and determination of roles and responsibilities across the organization. 3
During the COVID-19 pandemic, many clinicians had limited or no prior experience using telehealth4,5 and hence had not considered or acquired the required competencies, leading to feelings of uncertainty, fear, and apprehension. 6 To deliver safe and effective telehealth services, AHPs require additional skills and behaviors to those required for in person consultations. There is an additional need to educate AHP students in the use of telehealth. 7 Bridgman et al. 8 synthesized the literature related to the perspectives of allied health students on clinical placements that incorporated telehealth. Although little has been published on this topic, a key finding was that considerable preparation is needed for students to use telehealth safely and professionally.
Our recent scoping review 9 mapped telehealth competencies published by allied health disciplines and derived a set of competency themes currently in use. Eight overarching themes emerged that were related to the delivery of telehealth consultations, namely clinical reasoning, communication, effectively using technology, person-centered care, practice-based assessments and intervention knowledge, skills and behaviors, privacy, security, and safety, professionalism, and setting up the technology. There were three additional competency themes that outlined considerations related to health service management: digital infrastructure, informing practice, and management.
Objectives
The current article aims to extend our recent review 9 by addressing the question “What training or education (inclusive of practice placements) has been delivered to support development of telehealth competencies in AHPs?” We believe that this review is the natural progression of our previous work 9 and will provide a foundation for AHP regulators, peak bodies, and training institutions to consider how to define or develop individual discipline (and potential cross-disciplinary) competency standards related to telehealth.
Methods
A summary of the scoping review method is described below, with the detailed method of this scoping review reported in an earlier published article. 9
Ethics statement
It is a literature-based study; therefore, neither approval by the institutional review board nor the obtainment of informed consent is required.
Study design and eligibility criteria
A scoping review was undertaken using the Population Concept Context framework 10 and registered with Open Science Framework (https://osf.io/vrp62). This review included articles from 2012 to August 2023 that focused on at least one AHP, as specified by U.K.-based11,12 and Australian-based sources13,14 in Table 1. Competencies were broadly defined as the knowledge, skills, and behaviors needed to deliver AHP services efficiently and professionally. 15 Telehealth technology must have been used synchronously, and all study designs and gray literature were included. Theses and books were excluded. Articles must have included AHP telehealth training and/or education.
Allied Health Professions Included in This Scoping Review
Information sources and search strategy
The following databases were searched: MEDLINE, CINAHL, PsychInfo, Cochrane, EMBASE, Web of Science, and PEDro. The websites of United Kingdom Health Forum, World Health Organisation (WHO), Health Education England (now called National Health Service England (NHSE)), and all United Kingdom (U.K.) and Australian AHP associations were also searched. Please see the Supplementary Data for search strategy and terms.
Selection process and data synthesis
Following the search, all identified references were reviewed using the online Rayyan tool. 16 After removal of any duplications, titles and abstracts were divided and screened independently by the coauthors against the inclusion criteria. The research team includes experts from multiple AHP areas: physiotherapy, podiatry, speech pathology, and occupational therapy. This ensured article selection and analyses were not based on the perspective of a single profession. An agreement check was conducted after the abstract screening, where each team member was paired and checked 10% of each other’s screening. To ensure that cultural understanding was aligned, a U.K. team member was paired up with a team member from Australia. The full texts of potentially eligible studies were assessed independently by each coauthor against the inclusion criteria. Any disagreements between team members were resolved through discussion. Figure 1 displays our PRISMA flowchart.
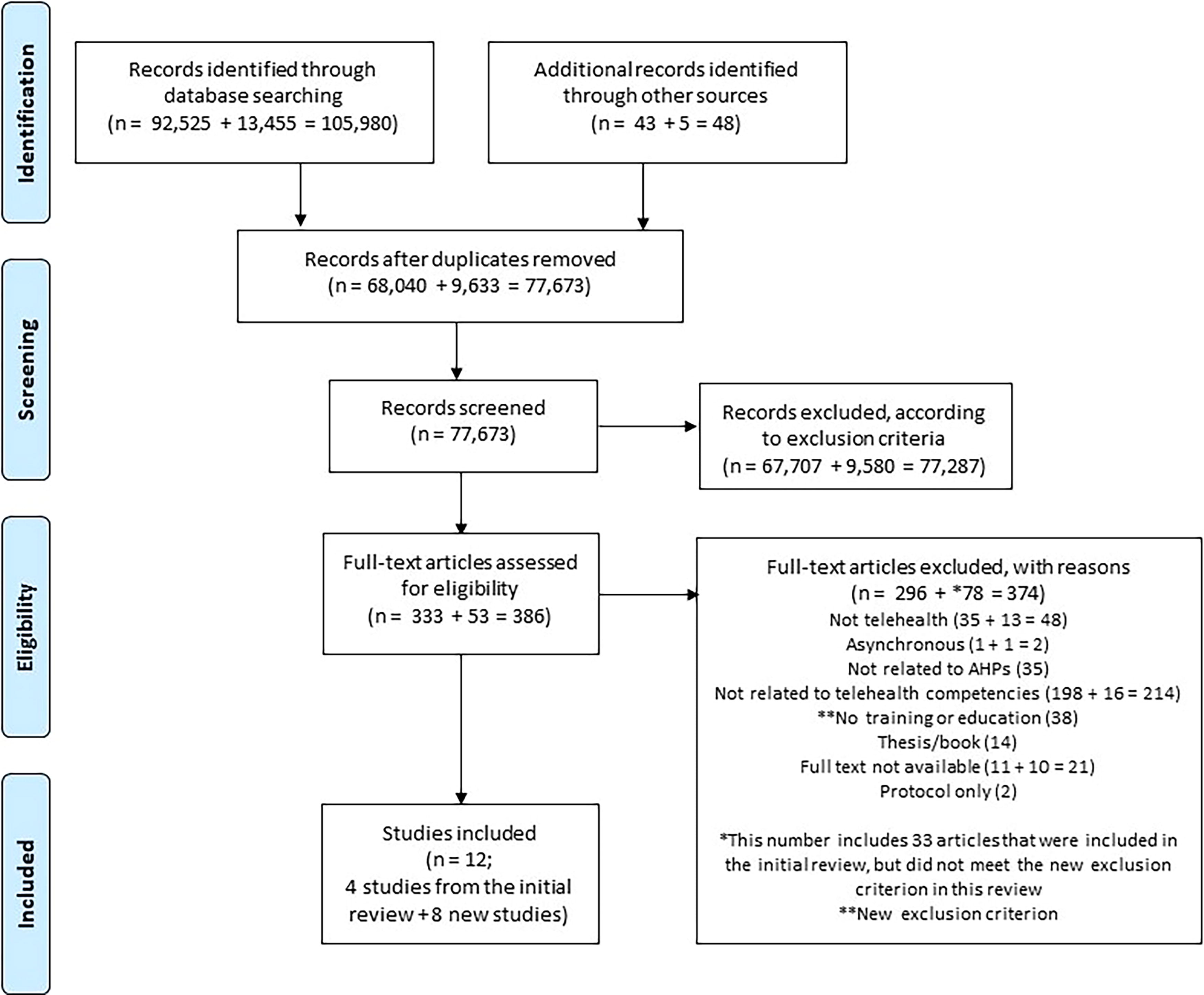
PRISMA flowchart of included articles; the initial search produced 1,05,980 articles that were carefully screened and resulted in 12 final articles.
Narrative data extraction was conducted using an Excel spreadsheet to extract data about telehealth training and education related to training/education description and schedule, context, use of any assessments/measurements, technology used, and related competencies. Any disagreements between team members were resolved through discussion. The findings are presented narratively in the results section aided by appropriate tables and figures.
The Hawker et al. 17 critical appraisal tool was used to assess the included articles, which is useful to compare studies with different designs, as is the case with the current review. The tool assigns a total score based on the quality of the following: abstract and title, introduction and aims, method and data, sampling, data analysis, ethics and bias, generalizability, and implications. The scores are then divided into low (9–17), fair (18–26), and high (27–36).
Results
Twelve articles were included in this scoping review (Fig. 1, see Table 2 for article characteristics, including quality scores). This number includes articles identified by the previous review 9 (n = 4) and articles identified by the updated search (n = 8). Ten articles were research studies, which included cohort studies19,23,25,27,28 (n = 5), quasi-experimental studies18,22 (n = 2), case studies24,29 (n = 2), and a cross-sectional study. 26 The remaining two articles were reports that described telehealth training and education without any evaluation.20,21 The majority of the articles originated from the United States18,19,21,23,25–29 (n = 9), and the remaining articles originated from Israel, 22 the United Kingdom, 20 and Vietnam. 24 The 10 research articles were assessed for their quality, where seven articles were deemed “Fair”18,19,22,24–27 and three were “High.”23,28,29 The studies classified as “Fair” had insufficient consideration to potential biases in their study design and unclear generalizability of their training and education procedures. This was primarily due to the minimal reporting on the rationale for learning outcomes selection. The studies rated as “High” had robust methods, coherent reporting of findings, and clear implications. Overall, these quality scores highlight the need for more articulated methods and clear justification for telehealth training and educational outcomes in ensuring the reliability and applicability of the results.
Article Characteristics
Competency themes
Tables 3 and 4 outline the competency themes described in our previous article. 9 The framework showcases a consolidation of telehealth knowledge, skills, and behaviors from the articles within our scoping review rather than formally agreed competencies. Therefore, they are referred to as “competency themes” rather than “competencies.” Table 3 presents competency themes regarding the delivery of telehealth consultations, while Table 4 presents competency themes regarding telehealth service management. Two new competency themes were identified within this review and are underlined within Table 3. They relate to adapting resources for telehealth and developing a therapeutic alliance with service users.
Competency Themes Relating to the Delivery of Telehealth Consultations
Competency Themes Relating to the Management of Telehealth Services
Telehealth training and education
Table 5 presents details of the telehealth training and education reported within the included articles of this review, showing a variety of different training and education approaches. Some descriptions are more detailed than others, and some articles reported the teaching of one or two competencies while others taught several competencies. In addition, length of the training and education differed greatly across the included articles, and there was no definitive pattern in teaching approaches. Three articles25,28,29 used different standardized questionnaires to assess whether their participants acquired the targeted telehealth competencies.
Training and Education Details Reported
Outcomes
Two main outcomes were evident across the included articles. First, eight studies18,19,22–25,28,29 reported that their evaluated competencies were achieved through a training and education program. Second, five studies19,22,23,25,27 reported that participants’ attitudes toward telehealth, such as self-confidence and satisfaction when providing telehealth services, increased after training and education. These two outcomes highlight the potential benefit of a structured telehealth training and education program. However, not all studies reported that telehealth training and education was beneficial. Pittman et al. 25 did not find a significant increase in teamwork-related competencies and suggest that this was because of a lack of in-person interaction during COVID-19 lockdown restrictions. This is in contrast to Baalman et al.’s 18 finding where their participants, who were a mixed cohort of health professions students, scored the highest on team communication compared to other skills and knowledge. The reason for this contrast is unclear; however, a potential explanation may be due to the difference in training and methods used to assess their communication competency. In-person training, 28 practice with real patients, 22 and more intraprofessional discussions 22 also appeared to benefit telehealth training and education.
Gaps in research
According to authors of the included articles, the primary gap in the research was the evaluation of telehealth training and education implementation19,21–23 in authentic settings. Examining whether certain features would improve learning during training and education, such as the inclusion of video vignettes, 23 scenarios with specific interventions, 28 and simulations that allow for mistakes, 18 were also suggested. Other gaps included understanding the nuances of telehealth training and education, such as assessing social and emotional development, 29 and examining the impact on patient experience and telehealth service outcome. 25
Recommendations
Most recommendations from the included articles related to the features of telehealth training and education. One article recommended that all students should have the same level of telehealth understanding before engaging in any training and education. 28 Telephone communication was suggested as needing its own distinct training element, 27 and that a single video vignette should only include one or two telehealth competencies at most. 23 Other recommendations stated that clinical experience is needed to deliver telehealth training and education, 20 clinical staff should share telehealth service duties as staff do not want to solely work in telehealth, 20 and that the evolution of technology should be monitored to ensure delivery of up-to-date telehealth services. 26
Article conclusions
Two studies emphasized the need to enhance telehealth training and education by incorporating a combination of online and face-to-face methods to optimize learning.24,28 Others concluded that interprofessional training facilitated communication learning18,19,28 through active teamwork, while students should have the opportunity to consolidate their skills through supervised clinical work, 20 and telephone and video competencies should be separated.20,27 The remaining conclusions highlighted the need for organizational support 23 and involvement of diverse stakeholder involvement 22 for the successful development of telehealth training and education.
Discussion
Interpretation
This is the first scoping review to examine telehealth training and education across allied health disciplines and complements our previous review on allied health telehealth competencies 9 where a paucity of literature in this field was identified. This review showcases the wide diversity of approaches to teaching telehealth competencies, with generally reported positive learning outcomes, despite no common teaching or evaluation method used across the included articles. There was limited rigorous evaluation of these programs and a lack of detail regarding the educational design and underpinning pedagogy. Consequently, it is unclear if the efficacy of the education relates to the quality of the instruction, the learning activity, or the degree of ease or difficulty in learning the targeted telehealth competencies. Furthermore, no pedagogical theories or frameworks were used in any of the articles to develop the telehealth training and education. It may, therefore, be possible that the education design and delivery influenced the learning outcomes. This prompts a call for an evidence-based curriculum design that can be adapted to the various allied health professions and education contexts. This would allow the acquisition of telehealth competencies to be the study focus and reduce the impact of the education design as a confounding variable.
An important consideration is the potential for bias within the included articles. The quality assessment showed that many studies did not sufficiently report on how bias was addressed within their study designs or outcomes. Specifically, the absence of established frameworks or theories, as noted above, may have introduced experience or profession-based biases. For example, the comfort or experience a participant may have with technology may have skewed results. AHPs often have distinct practices and priorities. Differences in professional outlooks, patient interactions, and disciplinary focus may lead to biases in how participants engage with and apply telehealth competencies. This highlights the need for future studies to adopt rigorous methodologies and reinforces the need for an evidence-based curriculum design.
Comparison with previous studies
One study reported that in-person training 28 was beneficial for teaching telehealth competencies, although the reason for this finding was unclear. It may be that a well-designed curriculum might not be affected by the delivery method, or there might be a methodological bias influencing this conclusion. Certain elements of telehealth training and education may be better suited for in-person teaching while others are well-suited for technology-enabled learning. This is reflected by the telehealth competency of determining suitability of telehealth versus in-person services, as demonstrated by Vyas et al. 29 and Rohrig et al. 26 as outlined in this review. Further research is needed to understand the features that optimize telehealth learning, and to determine when it is appropriate to use face-to-face teaching, technology, or a combination of both.
Limitation
This scoping review has limitations. Although an extensive updated search was conducted, it targeted published, peer-reviewed literature. It is possible that there are more telehealth training and education articles that have not been published and hence not included. The search strategy was biased toward the English language, where non-English relevant articles may have been missed.
Implications
The review findings indicate that telehealth competencies are an explicit skill set and need to be directly targeted by training and education. This is consistent with our previous scoping review findings that telehealth competencies need to be specifically taught. 9 No articles in this review compared methods of education and training, making it difficult to conclude whether there is a “best” way of designing and implementing telehealth education and training. The competency themes identified here need further refinement before real-world implementation. By developing specific telehealth training alongside the refinement of these competency themes, explicit telehealth competencies and appropriate measures of success can be used to upskill AHPs in telehealth delivery.
Conclusions
In conclusion, this scoping review represents the first comprehensive exploration of telehealth training and education across allied health disciplines. While diverse teaching approaches yielded generally positive outcomes, the absence of standardized methods prompts questions about its efficacy. Moreover, the emphasis of explicit telehealth competencies highlights the need for targeted training interventions. However, further refinement is necessary to ensure relevance in practice settings. Moving forward, research efforts should focus on developing evidence-based curriculum designs informed by high-quality pedagogic practices and tailored to AHP needs. By refining telehealth competencies and adopting appropriate measures of success, we can better prepare students and professionals for telehealth practice.
Footnotes
Authorship Contribution Statement
K.A., A.B., K.B., S.E., J.F., C.M., C.R., S.A.: Conceptualization; K.A.: Data curation; K.A., A.B., K.B., S.E., J.F., C.M., C.R., S.A.: Methodology/formal analysis/validation; K.A.: Project administration; Funding acquisition: Not applicable; K.A.: Writing—original draft; K.A., A.B., K.B., S.E., J.F., C.M., C.R., S.A.: Writing—review and editing.
Data Availability
None.
Author Disclosure Statement
No potential conflict of interest relevant to this article was reported.
Funding Statement
None.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.