
Abstract
Background:
Ensuring patients’ responsiveness to, acceptance of, and adherence to any telehealth service is essential before its implementation.
Objectives:
The aim of this pilot study was to assess patients’ responsiveness toward telemonitoring and telehealth coaching within a telenutrition weight-loss program.
Study Design:
Twenty-five overweight and obese participants were enrolled in a weight-loss program that was supported by weekly telemonitoring and monthly telehealth coaching sessions. The response rate of participants to telemonitoring and their attendance rate at the telehealth coaching sessions were measured throughout a 6-month period (totaling 36 weeks), in addition to the examination of correlations and trends in both health and quality of life measures.
Results:
The findings showed that participants’ response rate (%) for telemonitoring was at its highest rate (92%) in week 1, but this decreased dramatically and reached 19% in week 36. Meanwhile, 88% of the participants attended the first telehealth coaching session, followed by a slight decrease in the attendance rate (%) to 64% at the last session. The data indicate significant correlations between weight loss and improvements in Circle of Life (CoL) satisfaction rates, particularly between creativity, fun, and social life, confirming the positive benefits of integrative approaches to weight management. Most importantly, the data confirmed that attending more telehealth coaching sessions had a significant effect on weight loss, physical activity (measured in steps), and satisfaction with CoL aspects such as creativity, education, fun, social life, and spirituality.
Conclusions:
Thus, our findings highlight that participants were more committed and responsive to telehealth coaching than telemonitoring during long-duration weight management interventions. Thus, future studies should consider exploring the potential of telehealth devices to enhance patients’ responsiveness to telemonitoring.
Introduction
Telemedicine platforms have recently been utilized by many health care providers. 1 However, several barriers have been identified, including technical issues, staff being resistant to using telemedicine, and the age and level of education of the patients. Technical issues are a significant obstacle, such as limitations in internet connectivity, which are particularly common in rural and undeveloped areas. Staff resistance is due to their hesitation to move to digital health platforms and due to the time and effort required to learn how to use these new technologies and ensure compliance with digital health standards. In addition, patient age and level of education play crucial roles in the effectiveness of telemedicine systems, because older adults may have limited familiarity with digital devices and online systems, making their use more challenging.2,3 Thus, demographic factors create disparities in telemedicine access and effectiveness, highlighting the need for targeted support and training programs to bridge these gaps. 4 The literature confirms that telemedicine platforms increase clients’ satisfaction, in comparison with clients that do not have access to telemedicine platforms. 5 Other studies have highlighted that clients were highly satisfied with their experience due to their ability to access health care services. 6 One of the crucial parts of telemedicine is “telemonitoring,” which is defined as self-recording relevant information; this supports participants’ commitment and the responsiveness of clients to consultations, follow-ups, and monitoring. 7 A study was carried out to assess patients’ compliance with telemonitoring; the results showed a significant withdrawal rate, as it is a challenge to self-record and engage with telemonitoring continuously. 8 A study showed that telemonitoring and video consultations resulted in high compliance with measuring weight, heart rate, and blood pressure. 9 Thus, to enhance the commitment and engagement of clients, health coaching, also known as “telehealth coaching,” may be a supportive tool for follow-up, guidance, and providing health education. The use of telehealth coaching has been confirmed to have a positive impact on workers’ mental health. 10 Other studies have highlighted the positive impact of telehealth coaching provided by nurses on the management of diabetic patients, which was correlated with improvements in several health parameters, such as HbA1c, systolic blood pressure, weight, and body mass index (BMI). 11 Health coaching has recently emerged and has been integrated with nutrition. Integrative nutrition is defined as an emerging type of nutrition intervention, supported using health coaching approaches, that aims to be able to identify the root causes of poor health and lifestyles. Several parameters are involved in integrative nutrition; one of these parameters is the Circle of Life (CoL) tool proposed by Joshua Rosenthal, which is defined as “a valuable tool for better understanding your unique needs and how to find balance when you’re feeling stuck. By becoming more self-aware of what areas feel nourished and which could use more attention, you will discover how to continuously take care of your body, mind, and soul.” 12 This tool, named the “Circle of Life Satisfaction Scale,” has been validated and translated into Arabic for utilization by health care professionals; it enables them to assess lifestyle factors associated with their clients, to identify any associations with obesity, to support health coaching aimed at tackling the challenges and struggles associated with supporting weight loss, and to improve health and well-being. 13 This approach has been shown in the literature to have a significant impact on weight and behavior, leading to a healthier and happier life. 14 Promising outcomes have been reported following the use of telemedicine for nutrition consultations; namely, a higher percentage of referrals for weight loss and weight maintenance was seen. 15 The Academy of Nutrition and Dietetics has recognized telenutrition as a useful tool for use in the context of dieticians’ activity and has defined it as “the interactive use by an RDN of electronic information and telecommunications technologies to implement the Nutrition Care Process with patients or clients at a remote location, within the provisions of the RDN’s state license as applicable.” 16 In the literature, several studies investigated the positive impact of applying telehealth on weight management, which was explored in a “telemedicine-based health coaching” trial, the results of which showed positive outcomes for weight reduction and an increase in physical activity. 17 Another study also confirmed that weekly video conferencing and health education can be used as a telemedicine tool, causing a significant impact on weight reduction among obese patients. 18 Our research team published the primary outcomes of the current study,19–21 and the findings were also shared in the Clinical Nutrition ESPEN congress in Milan, 2024, 22 indicating that the personalized “integrative nutrition” approach is effective for weight loss, for improving patients’ general nutrition knowledge, and for reducing anxiety levels among obese and overweight individuals in a pilot telenutrition weight-loss program. In the same study, five case reports confirmed that integrative nutrition is essential for supporting clients’ mental health and well-being through health coaching, enabling them to achieve their dietary and weight-loss goals. 23 Thus combining both telemonitoring and health coaching in weight management programs has been evidenced, in a recent literature review, to exhibit great potential for weight loss and reduce the risk of chronic diseases. 24 However, few studies have studied the responsiveness of clients toward telemonitoring and telehealth coaching, and its relationship with health parameters and lifestyles.
The current study considered is examining secondary aims, which are assessing clients’ responsiveness to weekly telemonitoring and monthly telehealth coaching during a telenutrition weight-loss program. In addition, we investigate the association of improvements in health measures, such as weight, blood pressure, step count, and heart rate, with quality of life, which is operationalized as the CoL satisfaction rate. Furthermore, we identified a significant correlation between the number of telehealth coaching sessions attended and an improvement in health and satisfaction rates (CoL).
Materials and Methods
Study design and participants
A detailed study protocol is available in the British Journal of Nutrition. 25 Twenty-five participants enrolled in a telenutrition weight-loss program supported with telemonitoring and telehealth coaching. The sample size was calculated based on a power of 80% and a significance level of 0.05. 26 The study was approved by the Research Ethics Committee at the Unit of Biomedical Ethics, Faculty of Medicine, King Abdulaziz University (NCBE Registration No: [HA-02-J-008] and Trial Reference No: [Reference No 527-21]) and, accordingly, a filled-in informed consent form was obtained from all the participants, which explained the aim of the study, the primary and secondary outcomes, and the inclusion and exclusion criteria. The participants were obese or overweight adults, aged 20–50 years, of all genders. We excluded participants who were not familiar with using the online applications required for the study, such as WhatsApp and Zoom. The exclusion criteria also included participants with no/weak internet connections and/or devices that were not WhatsApp-/Zoom-compatible devices. In addition, pregnant or lactating women, patients with a history of chronic diseases (metabolic syndromes, cancers, or any other chronic conditions that require specific medical nutrition therapy), and patients who had joined weight-loss programs or had used medication to lose weight within the past 3 months were excluded from the study. Participants received a tailored hypocaloric diet planned by a registered dietitian via telenutrition, based on their preferences, nutrient needs, allergies, and intolerances, with each participant also receiving a diet guide showing portion sizes, meal plans, and recipes. The main goal was to achieve an initial weight loss of 5–10% of their baseline weight within 6 months; participants also underwent 10–14 follow-up meetings to reach their goals, including six educational sessions that were given once each month. This telenutrition weight-loss program was supported throughout the 6-month period with weekly telemonitoring and monthly personalized telehealth coaching sessions from an integrative nutrition health coach.
Weekly telemonitoring
Telemonitoring was implemented using the messaging platform WhatsApp (Meta Platforms, Menlo Park, California) via smartphones. All participants were given a training session on how to engage in weekly telemonitoring, which involved self-recording and sending weekly health measure results and CoL satisfaction ratings. Each participant received a “telemonitoring bag,” containing measurement devices and brochures to take home; the measurements were divided into two types, as follows:
Health measures: for self-recording weight, a weighing scale (Beurer GmbH, PS240) was provided; for self-recording blood pressure, an upper arm blood pressure monitor (Geratherm Medical AG) was provided; for self-recording total weekly step count, a pedometer (SPACARE SPAPEDW24) was provided. The CoL Satisfaction Scale: for self-recording CoL satisfaction rates, participants received a validated and translated CoL Satisfaction Scale assessment tool,
13
to assess their satisfaction with the following 12 key aspects in life: spirituality, creativity, finances, career, education, health, physical activity, home cooking, home environment, relationships, social life, and joy.
12
Key aspects of the CoL were formulated into questions to measure satisfaction across various life dimensions. The development process included steps such as introducing the tool, defining research questions, and selecting rating scales. Patients were provided with three response options for indicating their satisfaction with each CoL dimension: “completely satisfied,” “slightly satisfied,” or “not satisfied,” an adaptation based on previous telemonitoring research. The CoL dimensions encompass spirituality, creativity, finances, career, education, health, physical activity, home cooking, home environment, relationships, social life, and joy, as defined by the Institute of Integrative Nutrition. To support easy responses, a color-coded system was implemented: green for “completely satisfied,” yellow for “slightly satisfied,” and red for “not satisfied.” The research assistants ensured that all participants had downloaded WhatsApp onto their smartphones and had access to the internet.
Monthly telehealth coaching
Telehealth coaching was provided using the video conference platform Zoom (Zoom Video Communications, San Jose, California). All participants were given a training session on how to log into Zoom and attend the sessions. Six telehealth coaching sessions were provided for each participant, which included sessions on health history, goal setting, guidance, and follow-up. Sessions lasted a total of 45 min and were delivered in different settings, both individually and in a group, via Zoom. The health coaching approach used followed that of the Institute for Integrative Nutrition, which focuses on ratings of participants’ satisfaction with their quality of life; this includes the 12 components of the CoL, namely spirituality, creativity, finances, career, education, health, physical activity, home cooking, home environment, relationships, social life, and joy. 12 In addition, physical activity was a core aspect that was measured for all participants who attended the telehealth coaching sessions, as it had previously been identified as a challenge for the target audience.
Statistical analysis
Statistical analysis was carried out using IBM SPSS v26, applying the following tests. Descriptive statistics was used to give an overall descriptive summary for the whole sample or a segment of it, using mean, standard deviation (SD), and frequency distribution. Multilevel analyses were carried out for every participant who provided repeated measures data for 36 weeks, to check that the association between two variables (or even their interaction) was consistent across all participants. For the correlation analysis, Pearson’s r was used to assess the linear relationship between any two variables. R software was partially used to compare any two correlations (specifically, whether they were different or not) using the “cocor” package. Note that all tests were conducted under a 0.05 level of significance.
Results
Sample characteristics and demographics
Table 1. demonstrates the sample characteristics, which is compromised of 26 participants, of which 38.46% (n = 10) were males and 61.54% (n = 16) were females. The average age of the sample was around 33 years old (SD = 10.05). The average values of various body measurements were as follows: 131.9 (SD = 15.8) for blood pressure (BP) (sys); 78.52 (SD = 13.04) for BP (dia); 95.78 (SD = 21.18) for weight (kg); 166.24 (SD = 9.74) for height (cm); 34.86 (SD = 6.39) for BMI; 1764.65 (SD = 371.0) for RM (Kcal); 44.95 (SD = 7.65) for fat %; 24.85 (SD = 4.28) for muscle %; 12.38 (SD = 5.45) for vis. fat (g); and 102.06 (SD = 19.01) for WC (cm).
Participants Characteristics
BMI, body mass index; BP, blood pressure; N, number of participants (%); M, average value; SD, standard deviation.
Participants’ response rate toward telemonitoring over 36 weeks
Figure 1 shows that there was a significant (p-value <0.001) difference in attendance (%) over time; attendance was highest in week 1 (92%) and decreased to 19% in the last week (week 36). It can also be noted that there was no attendance (0%) in week 14 and weeks 25–29.

Participants’ response rate toward telemonitoring over 36 weeks.
Participants’ attendance rate in telehealth coaching sessions over 36 weeks
Figure 2 shows that there was a significant (p-value <0.001) difference in attendance rate (%) over time; attendance was highest in the first session delivered (88%) but reduced in the second (68%), third (68%), fourth (56%), and fifth sessions (48%), before increasing to 64% in the last session.

Participants’ attendance rate in telehealth coaching sessions over 36 weeks.
Health measures over 36 weeks
Figure 3 shows that, with the exception of weight, the health measures showed a roughly constant average over 36 weeks. This is supported by the p-value for the correlation between time and these variables (it is <0.001 for weight and >0.05 for other measurements). This is also demonstrated in Table 2. In terms of descriptive statistics, the average weight started at 90.74 kg in week 1 and ended at 79.12 kg for week 36. Regarding the other measurements, the average fluctuated within the following ranges: 107.93–128.14 for BP (sys); 55.4–82.25 for BP (dia); 14.34–34.82 thousand steps for step count; and 72.63–84 for HPR.

Health measures over 36 weeks.
Association Between Attending Health Coaching Sessions, Health Measures, and CoL Satisfaction Rates
The time-trend (of the study variables) in each group and the difference between the two groups. R software was partially used only to compare any two correlations using the “cocor” package. Noting that all tests were conducted under 0.05 level of significance.
Significant at 0.05.
Significant at 0.01.
CoL, Circle of Life.
CoL satisfaction rates over 36 weeks
Figure 4 further summarizes Table 3 by showing the averages for each 10-week period (resulting in three periods). As the figure shows, for more than half of the CoL variables, there is an increase over time (i.e., over the three periods) for satisfaction rate, namely for the following variables: cooking (54%/60%/64%), creativity (61%/78%/85%), education (72%/80%/83%), fun (60%/81%/85%), social life (73%/90%/90%), spirit (73%/92%/90%), and sports (43%/59%/54%). This is supported by the p-value of the trend (which can be found at the bottom of Table 3), which is <0.05 for each of these seven variables. On the other hand, the graph does not show a clear trend (neither increase nor decrease) over time for the rest of the CoL variables (this is supported by the p-value for the trend being >0.05 in Table 3). For the variables with a non-significant correlation with satisfaction % over time, we may describe the fluctuation of satisfaction (taken from the min/max in Table 3) as follows: health (sat. % fluctuating in the range of 57%–100%), home (sat. % fluctuating in the range of 50–100%), job (sat. % fluctuating in the range of 20–69%), money (sat. % fluctuating in the range of 20–75%), and sports (sat. % fluctuating in the range of 14–86%).
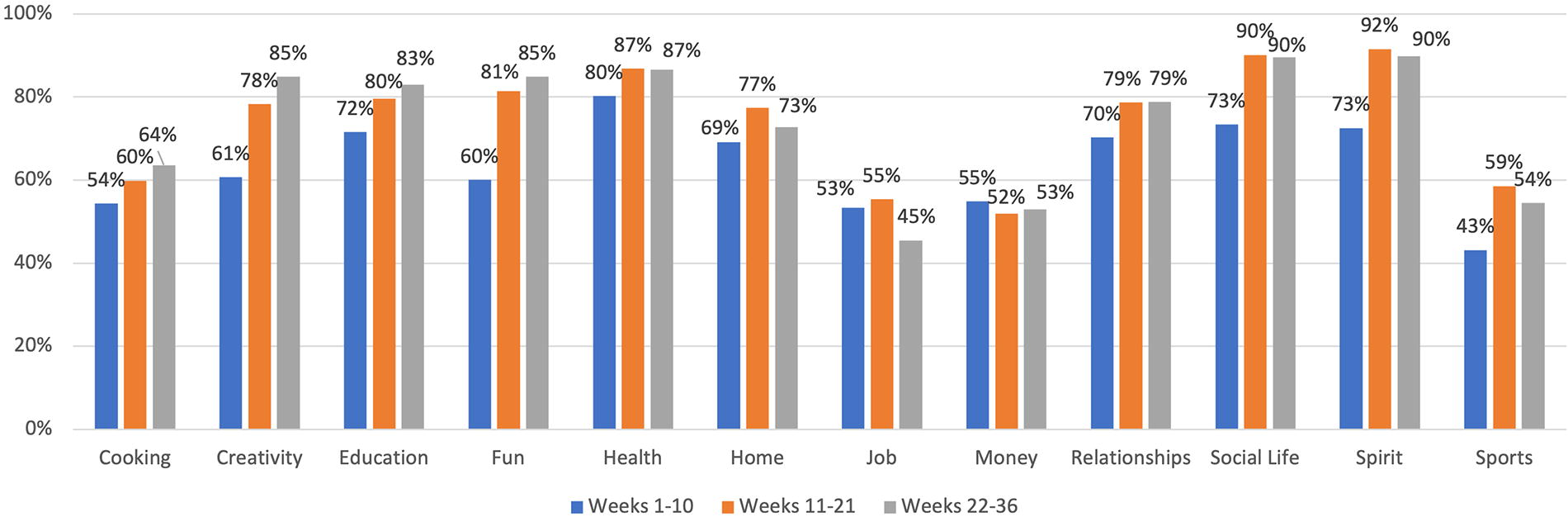
Circle of Life satisfaction rates over 36 weeks.
Satisfaction Rate (% of Satisfied Participants) with Regard to All CoL Variables Over the 36 Weeks
Significant at 0.05.
Significant at 0.01.
Significant at 0.001.
The correlation between CoL aspects and health measures
Table 4 demonstrates a statistically significant correlation between CoL aspects and health measures, expressed as having a p-value of <0.05 or 0.01, which is indicated with * or **, respectively. For weight versus creativity/fun/social life, Pearson’s r value ranges from −0.177 to −0.130: since all seven of these correlations are negative, it means that being satisfied in these aspects of CoL is associated with weight loss. The correlation between step count and social life (r = 0.145) is positive; this means that being satisfied with one’s social life is associated with a higher step count.
The Correlation Between Circle of Life (CoL) Satisfaction and Health Measures
Pearson’s r for the correlation between CoL variables and health measurements.
Significant at 0.05.
Significant at 0.01.
Association between the number of health coaching sessions attended and both health and CoL satisfaction measures
Attendance at the telehealth coaching sessions was recorded per participant (e.g., no attendance, once, twice, etc., up to a maximum of six times). Based on this, participants were classified into two groups: those who attended fewer than four coaching sessions and those who attended more than four coaching sessions (the cutoff point of four is the mid-point between zero and six). Table 2 shows the correlation (Pearson’s r) between the listed variables and time, split into the high-attendance (more than four sessions) and low-attendance (fewer than four sessions) groups. The last column (summarized by p-value) shows the significance of the difference between each pair of correlations (the correlation for the high-attendance group, and the correlation for the low-attendance group). The data show that there is a significant (p-value of <0.05) difference between the two groups over time, regarding step count, home environment, finances, and job.
Discussion
The current pilot study was conducted in Saudi Arabia and aimed to provide evidence on the effectiveness of weekly telemonitoring and monthly telehealth coaching for patients, by measuring the difference in adherence to telemonitoring (via WhatsApp) and telehealth coaching (via Zoom), by assessing the responsiveness rate and attendance rate, as well as the impact of such engagement on several aspects of health and quality of life. Descriptive data from the study demonstrated that the response rate for telemonitoring was less than that of the attendance rate for telehealth coaching sessions, throughout the 36-week intervention. The data showed promising health outcomes in the data gathered weekly via telemonitoring. First, significant correlations between weight loss and improvements in satisfaction rates of CoL components were seen, in particular, for the aspects of creativity, fun, and social life. In addition to this, participants who attended four or more telehealth coaching sessions experienced a more significant increase in weight loss, physical activity (steps), and satisfaction with several CoL aspects such as creativity, education, fun, social life, and spirituality. However, maintaining the participants’ commitment to documenting weekly data was a challenge, as their motivation reduced over the intervention time. This was compounded by the 6-month duration of the intervention, which is longer than many previous studies. A previous study was carried out in Saudi Arabia on the effectiveness of daily self-recording for a virtual physical, educational, and motivational program, which showed that participants had high commitment over an 8-week duration. 27 The positive outcomes related to weight management seen in this study are consistent with those of previous studies that integrated both telemonitoring and telehealth coaching.17,18,26 This justifies that telehealth coaching may play a crucial role in retaining clients in telemedicine programs and in supporting weight management. One of the reasons for this is that telehealth coaching works on improving patients’ behavior and attitudes toward eating habits, diet, and exercise. 28 A randomized controlled trial (RCT) confirmed that telehealth coaching improves long-term weight loss for obese people, in comparison to usual care. 29 A recent literature review categorized weight-loss RCTs by duration, identifying long-term programs as those extending beyond 12 months and short-term programs as those lasting up to 6 months. Variations in program duration significantly impacted outcomes, particularly in modifying chronic disease risk factors, which are more likely to show improvement in long-term interventions. In contrast, shorter programs may be sufficient to achieve initial weight loss but are less effective in sustaining health benefits associated with chronic condition management. 24 This is consistent with our findings, which demonstrated that attending four or more telehealth coaching sessions was significantly associated with weight loss, physical activity (step count), and satisfaction rates for the creativity, education, fun, social life, and spirituality aspects of CoL. In 2022, Larsen et al. investigated the impact of telehealth coaching on physical activity levels among patients with chronic conditions, and their results were consistent with our study findings; they found a significant increase in step count,30,31 with both quality of life and physical activity being main factors associated with a healthy lifestyle and lower obesity levels. 32 Based on the literature, our study is one of the few studies that have looked at weight management using a holistic approach. One of the distinctive measures in the current study is the CoL tool, which is an integrative nutrition model that was developed by Joshua Rosenthal (2018) to support individuals with their diet and well-being. 12 Previous studies have confirmed that telehealth coaching may also improve mental health as well. 10 In five distinct case reports presented by our research team, 23 a significant negative correlation between weight and satisfaction with specific CoL aspects, such as life enjoyment, home cooking, spirituality, physical activity, and work, was observed. Thus, these participants achieved optimal weight-loss outcomes and enhanced well-being by utilizing an integrative nutrition approach. The primary strength of this pilot study lies in examining innovative approaches within weight management programs, where client responsiveness to each method can guide health professionals in selecting optimal strategies to enhance adherence and support progress toward weight-loss goals. The current study, along with all related articles published by the same research group, represents the first research in Saudi Arabia to examine the effects of telenutrition, telemonitoring, and telehealth coaching on weight management.
Conclusion
In conclusion, this study provides additional evidence of clients’ responsiveness to both telemonitoring and telehealth coaching and these approaches’ effectiveness in weight-loss programs among overweight and obese individuals. While the findings align with the literature on telemedicine’s role in weight management, they also highlight the importance of tackling CoL aspects that influence patients’ food choices, eating patterns, and lifestyle, an approach that is defined as “integrative nutrition.” Our strategy shows potential for use in dietary weight management programs, wherein telehealth coaching is crucial to maintain motivation and solve other associated issues. Still, several limitations have been identified in the current study. The main limitation is the small sample size; because the study was a pilot study, only 10–30% of the targeted sample size was included. Another limitation of the study is the absence of telehealth devices, such as wearable devices used to track physical activity and body measurements,33–36 the future use of which may strengthen future research. These tools are usually used to track participants’ physical activity and body measurements in real time. This absence may have influenced the accuracy and consistency of self-reported data. Furthermore, the study’s 6-month duration posed a challenge in maintaining participant engagement. As observed, the response rate for telemonitoring declined over time, indicating a possible drop in motivation or commitment over time. Participants’ high-attendance rates for telehealth coaching sessions demonstrated more motivation and commitment in this area than for telemonitoring. Additionally, the study was only carried out in the Saudi populations, which may limit the generalization of the outcomes. Therefore, future full-scale studies must aim to have a larger and more diverse sample, in order to make the sample more representative. Additionally, both extended and varied program durations may reveal the ideal timeframes needed for significant behavior changes. It is also essential to find suitable telehealth tools for weight management.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of The Research Ethics Committee (REC) at the Unit of Biomedical Ethics, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia NCBE Registration No: (HA-02-J-008) and Trial Reference No: (Reference No 527-21).
Footnotes
Acknowledgment
This research work was funded by Institutional Fund Projects under grant no. (IFPRC-206-141-2020). Therefore, authors gratefully acknowledge technical and financial support from the Ministry of Education and King Abdulaziz University, Jeddah, Saudi Arabia.
Authors’ Contributions
Conceptualization: N.M.S.E., E.A.A., S.E., R.R.S., and K.M.Q. Data curation: S.E. Formal analysis: S.E. Funding acquisition: N.M.S.E., E.A.A., S.E., R.H.M., R.R.S., K.M.Q., and S.M.S.E. Investigation: E.A.A., K.M.Q., and S.M.S.E. Methodology: N.M.S.E., S.E., R.R.S., and S.M.S.E. Project administration: N.M.S.E. Resources: R.H.M. Supervision: N.M.S.E. Validation: R.H.M. and R.R.S. Visualization: R.H.M. Writing—original draft: N.M.S.E. Writing—review and editing: N.M.S.E., E.A.A., S.E., R.H.M., R.R.S., K.M.Q., and S.M.S.E. All the authors have read and agreed to the published version of this article.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author:
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research is funded by the Institutional Fund Projects under grant no. IFPRC-206-141-2020.