
Abstract
Background:
The establishment of tele-cardiology in mobile clinics improves patient access to pediatric cardiology service in remote locations.
Objectives:
The aim of this article is to describe the design of tele-consultation for pediatric cardiology in mobile clinics at our institution.
Materials and Methods:
Patients with limited healthcare access presenting to community pediatric mobile clinics for care are evaluated by a pediatrician in the field. Those patients with findings warranting cardiac evaluation return for tele-cardiology consultation. Consultation takes place in a portable tele-clinic system on mobile unit equipped with encounter management software, customized medical devices, and videoconferencing. At tertiary center, a broadband-enabled computer with videoconferencing software allows for real-time tele-cardiology consultation. Videoconferencing, tele-auscultation, tele-electrocardiography, and tele-echocardiography are incorporated into the evaluation to replicate an outpatient cardiology evaluation.
Results:
Since establishment of tele-echocardiography at our institution, 30 patients have undergone tele-cardiology consultation including a screening echocardiogram. Patients ranged from 4 to 19 years age (mean: 9.6 years). Indications for referral were cardiac murmur (n = 14), chest pain (n = 4), syncope (n = 2), high blood pressure (n = 2), atrial septal defect (n = 1), patent foramen ovale (n = 1), ventricular septal defect (n = 2), and VATERL association (n = 1). Structural anomalies were detected in 6 patients: patent foramen ovale (n = 1), secundum atrial septal defect (n = 1), aortic regurgitation (n = 1), aneurysmal septum primum (n = 1), and ventricular septal defect (n = 2). Two patients were referred for in-person cardiac evaluation for potential intervention: secundum atrial septal defect and aortic regurgitation.
Conclusion:
Tele-consultation for pediatric cardiology with a smooth workflow is successfully established in mobile clinics at our institution.
Introduction
Established in 1992 as a response to Hurricane Andrew, the University of Miami Pediatric Mobile Clinic has provided medical care to uninsured children in need for nearly three decades. The Mobile Clinic provides comprehensive care, which includes linking patients to subspecialty care as needed. Because pediatric cardiology is particularly suitable for telemedicine, we developed a tele-cardiology clinic that provides evaluations in the field. In the initial phase of the clinic, the evaluation consisted of a history conducted by the cardiologist via videoconferencing with the parent and patient, a physical examination including tele-auscultation, and a tele-electrocardiography. We attempted to organize echocardiography clinics in the field with a certified sonographer using a fully diagnostic portable echocardiography machine in the mobile clinic. Patients were scheduled to undergo an echocardiography if it was deemed necessary. However, owing to multiple logistical challenges, we were able to accomplish this with very few patients. We have since added on-site hand-held screening echocardiography with good results. The aim of this review is to describe the design of tele-consultation for pediatric cardiology in pediatric mobile clinics at our institution and to demonstrate the feasibility of performing tele-echocardiography with a handheld device.
Materials and Methods
The architecture and work flow of tele-consultation for pediatric cardiology in mobile clinics at our institution are detailed below (Figs. 1 and 2). This study was approved by the investigational review board of the University of Miami. Uninsured patients with limited access to healthcare present to a mobile clinic for care. The patients were evaluated by a pediatrician from the mobile clinic team. Patients with a history and/or physical finding warranting pediatric cardiac evaluation were scheduled for tele-cardiology consultation in the mobile clinic. The American College of Cardiology published a joint report on appropriate use criteria (AUC) for outpatient pediatric echocardiography. 1 Patients needing echocardiography based on AUC are scheduled for tele-echocardiography. The consultation takes place using AGNES Interactive (Massachusetts, USA), a commercial telemedicine software on a mobile unit equipped with complete encounter management software, customized medical devices, and videoconferencing. The pediatric cardiologist at the tertiary care center uses broadband-enabled desktop videoconferencing computers established at the Pediatric Cardiology Division, University of Miami/Jackson Memorial Hospital, Miami. The internet speed was about 26 Mb/sec at the mobile clinic and 188 Mb/sec at the receiving tertiary care center. With the earlier mentioned internet speed at either end, we experienced a high-definition quality streaming of the teleconferencing session and the tele-echocardiogram.
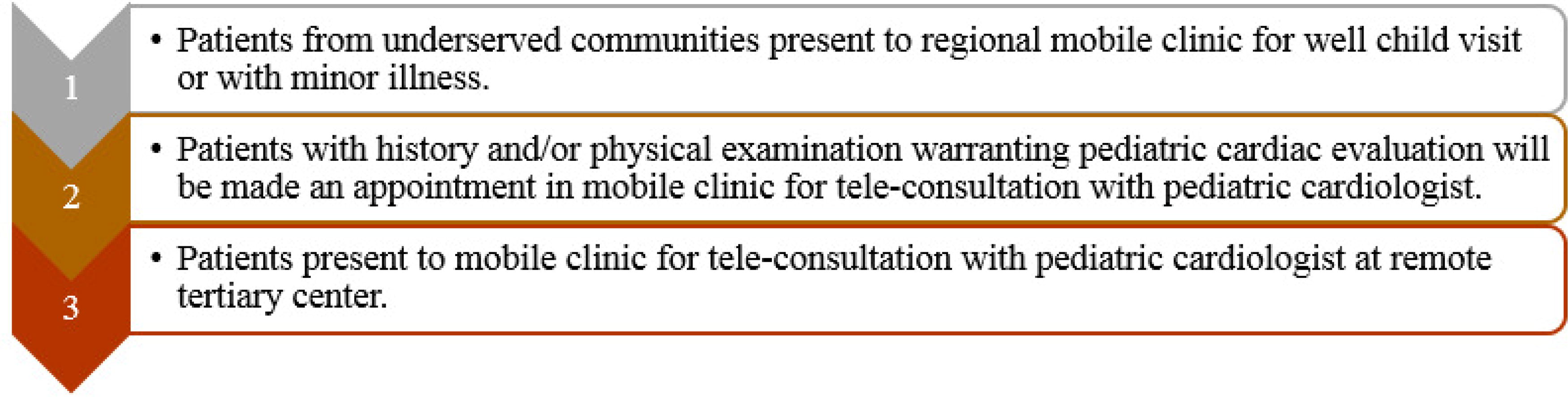
Illustration of mobile clinic work flow.

Illustration of teleconsultation work flow.
Teleconference
Teleconference is enabled with AGNES interactive (Massachusetts, USA) web-based commercial telemedicine software. With the help of AGNES interactive (Massachusetts, USA), live two-way videoconferencing was established, allowing interaction between physicians or parents at the mobile clinic and the pediatric cardiologist at the tertiary care center. History and physical examinations, including tele-auscultation, are performed by a pediatric nurse practitioner in the mobile clinic and are documented in the electronic medical record, which is accessible in the field and at the tertiary center. Each patient and each clinical presentation are unique, and the need for electrocardiography and echocardiography was considered in the context of comprehensive clinical assessment. The medical device diagnostics relevant to tele-cardiology includes a digital stethoscope for tele-auscultation, 12-lead digital electrocardiography for tele-electrocardiography and hand-held echocardiography for tele-echocardiography which are described below.
Tele-auscultation
Tele-auscultation was performed with AMD-3750 (Massachusetts, USA), a PC-based digital stethoscope with a direct USB connection to the computer (Fig. 3). Software-based controls enable easy adjustment of the volume and frequency range based on the bell, diaphragm, or extended modes. Audio streams through the AGNES interactive (Massachusetts, USA) web-based portal telemedicine software. It provides a remote healthcare provider with live stethoscope sounds in real time, eliminating the need for stethoscope hardware or software at the receiving end.

Tele-auscultation:
Tele-electrocardiography
Tele-electrocardiography was performed using a Welch Allyn resting digital 12-lead electrocardiograph system. It is a PC-based system enabled with automatic ECG measurements and on-screen reporting functions (Fig. 4). The system is integrated with AGNES workstation, a commercial software (Massachusetts, USA), which enables monitoring, reviewing, storing, and printing of ECG reports. A 12-lead electrocardiography was printed and scanned in the patient’s electronic medical records.

Tele-electrocardiogram:
Tele-echocardiography
Tele-echocardiography was performed by a third-year pediatric cardiology fellow trained in acquiring and interpreting the echocardiographic images. Studies were performed using Philips Lumify probe, a high-quality portable app-based cardiac ultrasound probe. Lumify is compatible with the latest encryption and data security systems and is designed to comply with enterprise data security policies. Three simple steps were involved in obtaining the images (Fig. 5):

Tele-echocardiogram: Philips Lumify portable app-based cardiac ultrasound probe is used to obtain focused cardiac images with three steps involved:
Lumify app is downloaded to compatible smart device.
Lumify transducer is connected through a simple USB connection.
The probe connected to the smart device is ready to acquire images.
The probe was integrated with Reacts, a tele-ultrasound solution, that enables two-way audio-visual calls with live ultrasound streaming.
By turning a compatible smart device into an integrated tele-ultrasound solution, this intuitive integrated system connects physicians at tertiary care centers in real time. The sonographer can switch to a front-facing camera on the smart device to show the position of the probe. Lumify ultrasound images can be shared so that both parties can view the live ultrasound image and probe positioning simultaneously. Images were obtained using a focused protocol directed by history and physical examination. Echocardiography may include one or more of the following views: subcostal, apical, parasternal, and suprasternal. The cardiologist at the tertiary center directed the sonographer to obtain more images if further clarification was deemed necessary. For the purpose of this study, all the studies were performed by the same third year pediatric cardiology fellow, and interpreted by the same pediatric cardiologist at the tertiary care center. The echocardiographic images obtained were transmitted in real-time using the 802.11 videoconferencing protocol. The frame rate for the transmitted images ranged from 27 to 33 frames per second. With an internet speed of approximately 26 Mb/sec and 188 Mb/sec at the receiving tertiary care center, there were limited interruptions with no drop in the resolution of the echocardiographic images. Following acquisition, the studies were uploaded to the university’s reporting and archiving system in Digital Imaging and Communications in Medicine, Philips IntelliSpace, and picture archiving and communications systems. All handheld echocardiography (HHE) examination results were documented in the patients’ electronic medical records. The smart device is not designed as a long-term storage device.
Results
Patient population
Patients who underwent echocardiographic evaluation at a mobile clinic were in the age range of 4–19 years (mean: 9.6 years). The indications for referral to the mobile clinic for cardiac evaluation were cardiac murmur in 14 patients, chest pain in 5, high blood pressure in 2, syncope in 2, ASD in 1, PFO in 1, VSD in 2, and VACTERL association in 1 patient.
Data collection and results
Thirty patients were screened with echocardiography in a mobile clinic, of which 22 echocardiograms did not detect any structural anomalies. Structural anomalies were detected in 6 patients, including patent foramen ovale (n = 1), secundum atrial septal defect (n = 1), aortic regurgitation (n = 1), aneurysmal septum primum (n = 1), and ventricular septal defect (n = 2).
Of the 14 patients referred for heart murmur, VSD was noted in 2 patients, secundum ASD was noted in 1 patient, and aneurysmal atrial septum in 1 patient. Of the 5 patients referred for chest pain and 2 patients referred for syncope, all had normal findings on HHE including normal coronary artery origins. Of the 2 patients referred for high blood pressure, one of them was noted to have mild aortic regurgitation on HHE.
All six patients noted to have structural anomalies were appropriately referred to the tertiary care center for standard TTE. PFO was noted to be small on standard TTE, and patient was discharged from follow-up. Patient with secundum ASD was referred for transcatheter ASD closure. Aortic regurgitation was confirmed to be mild on standard TTE, and therefore patient was followed periodically. Patient with aneurysmal atrial septum was noted to have no atrial level shunting and was followed. Out of the two patients with VSD, one was a small anterior muscular VSD and the other was a small mid-muscular VSD, and they were followed periodically. Patients and their families appreciate the remarkable medical, economic, and social benefits of tele-cardiology in mobile clinics.
Discussion
Telemedicine, defined as the remote diagnosis and treatment of patients using telecommunications technology, has a humble origin with deep roots in the medical specialties of cardiology and radiology. The History of Telemedicine by Bashshur and Shannon provides a historical summary of telemedicine from ancient history to the present.2,3 The origin of telemedicine was traced back to Europe, where Willem Einthoven, a Dutch physician, made a long-distance transfer of electrocardiograms in 1905. The first radio consultations began in Europe in the 1920s, followed by clinical telemedicine programs in the United States in the late 1950s. The first clinical use of telemedicine in cardiology dates back to the year 1989. Since its origin, telemedicine has become a dynamic evolutionary field with rapid advances. Clinical echocardiography dates back to 1950s and was credited by Carl Helmuth Hertz and Inge Edler. Ever since the concept of ultrasonic stethoscope in 1970s, miniaturization of echocardiography is rapidly emerging over the last few decades.4–6
One of the most frequent reasons for pediatric cardiology referral is a cardiac murmur. Several studies have concluded a good agreement between in-person and tele-auscultation using electronically transmitted heart sounds. 7 ASE-REWARD study is one of the largest community outreach projects in a rural setting in northwestern India, where ∼1000 patients underwent tele-echocardiography, demonstrating the feasibility of mass triage in the community. 8 A comprehensive scientific statement on telemedicine in pediatric cardiology was published in 2017 by the American Heart Association. 9 The statement summarizes about 33 publications in pediatric tele-echocardiography from various parts of the world, the first being from Nova Scotia by Finley et al. in 1989, the majority of which describe the use of echocardiography in a hospital setting with no pediatric cardiologist on-site and studies performed by trained sonographers.
Pediatric tele-cardiology service has evolved in the last few decades, and the COVID-19 pandemic has accelerated telemedicine use. 10 Several studies have been published in the recent years reviewing the application, merits, and challenges of telemedicine in pediatric cardiology.5,11–14 However, not very many studies detailed the architecture and workflow of tele-cardiology in pediatric mobile clinics.
Tele-consultation was successfully established at the mobile clinic at our institution, with a high success rate and smooth work flow for acquisition and transmission. Second- and third-year pediatric cardiology fellows at our institution undergo training in acquiring and interpreting images obtained using HHE. The next steps include training certified sonographers to facilitate the tele-cardiology service in mobile clinics. Once the training is complete, it might be feasible for the sonographers to perform HHE studies without live feedback from the pediatric cardiologist. A pilot project is underway at our institution comparing the sensitivity of HHE to standard TTE performed with an Intersocietal Commission for the Accreditation of Echocardiographic Laboratories (ICAEL)-approved protocol in our pediatric cardiology clinic.
Conclusion
Successful establishment of tele-cardiology enables us to serve underserved population with limited access to cardiac evaluation.
Footnotes
Acknowledgments
The authors thank the patients’ families for their participation in this study. The authors thank Ms. Evette Torres, APRN, for her expertise and assistance in coordinating the tele-cardiology consultation in our mobile clinic.
Authors’ Contributions
The authors confirm contribution to the article as follows: Study conception and design: Mohanageetha Ardhanari. Data collection: Mohanageetha Ardhanari, and Mary C. Sokoloski. Analysis and interpretation of results: Mohanageetha Ardhanari, and Mary C. Sokoloski. Draft article preparation: Mohanageetha Ardhanari, Lisa Gwynn, Richard E. Kardon, and Mary C. Sokoloski. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
The authors state that there was no relationship with any industry and there are no conflict of interest.
Ethics Compliance
All procedures performed and studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable medical status.
Funding Information
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Access Statement
All relevant data are within the article and its Supporting Information files.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The entire study was conducted at Miami, Florida.