
Abstract
Background:
Telehealth has long offered promise for improving health care access, but due to restrictive regulations and technology limitations, historic use has been low. Despite telehealth’s unprecedented expansion during the COVID-19 pandemic, economic questions remain, raising uncertainty about telehealth’s future.
Methods:
We used an economics lens to conduct a narrative review of the vast medical literature and nascent economic literature on telehealth. We reviewed evidence on demand-side and supply-side forces influencing telehealth adoption and evidence on telehealth’s impact on health care use, costs, effectiveness, and equity.
Results:
Current evidence is sparsely distributed across care types, telehealth modalities (e.g., phone, video, secure messaging), models of telehealth delivery, and pre- and post-pandemic periods. While the literature provides some signals that patients and clinicians are responsive to monetary costs of telehealth, more robust studies are needed, including studies on patient and provider time costs. Telehealth adoption appears to modestly increase outpatient care use, but evidence of its impact on costlier emergency or inpatient care use is needed. There is a lack of studies on monetary costs of telehealth, particularly the impact of telehealth on production costs. Importantly, there is a lack of high-quality studies on the comparative effectiveness of modalities. While there is a growing literature on disparities, studies that address confounders are needed to assess if telehealth can deliver on its promise to improve access for underserved populations.
Conclusion
: Our review paves the way for a stronger economics literature on telehealth, highlighting areas of future research.
Introduction
Tasks, such as getting groceries or depositing checks, are increasingly being completed using personal electronic devices such as smart phones, tablets, or laptop computers. 1,2 This use of technology for improved access to services and convenience has also become increasingly common in health care via telehealth, 2 which refers to the use of electronic information and telecommunication technologies to support remote delivery of health care. 3
Telehealth, with roots dating to the late 1950s, has held substantial promise for improving access to health care, especially for underserved areas grappling with provider shortages. Telehealth can connect patients in underserved areas with providers located in another area. 1 However, widespread adoption of telehealth had long been hindered by restrictive regulations and technology limitations. 4 Underlying economic considerations have for years been the most frequently cited reason for restrictive telehealth policies. 1,3,5 –7 Private and public insurers were, and still remain, concerned that generous coverage and reimbursement for telehealth services would increase costs if telehealth visits are less efficient than standard in-person care and if generous coverage would influence or distort patient and provider incentives in ways that increase overall health care spending.
Due to the social distancing measures implemented to prevent the spread of COVID-19, many of the laws governing telehealth were loosened during the pandemic to enable health care delivery. Policymakers are now questioning whether to reinstate prepandemic regulations or to make some pandemic-era policies permanent. 8,9 Telehealth advocates, including patients and providers, argue that reverting to prepandemic era policies could hurt care delivery. 8 Rigorous health economics research can inform policymakers’ longstanding cost concerns about telehealth.
Despite telehealth being around for decades, there is a dearth of economics studies of telehealth. In contrast, there has been a vast medical and health services literature on telehealth, which has grown precipitously in recent years due to the large-scale adoption of telehealth during the COVID-19 pandemic. The disciplinary gap between medical/health services (MHS) literature and economics literature is large and difficult to navigate. With the rapid growth of the telehealth sector and looming policy uncertainties, bridging this disciplinary gap is crucial. The purpose of this narrative review is to use an economics lens to synthesize the voluminous body of work focused on telehealth. Specifically, we use a demand-side and supply-side framework to highlight gaps in the literature where economic theory and econometrics can be used to inform long-term federal and state policies guiding telehealth. This review focuses predominantly on telehealth in the United States (U.S.). Nevertheless, the heterogeneity in policies, geographic variation, access issues due to large distances, many rural communities, and the disjointed nature of health care in the U.S. allow for diverse insights relevant for many contexts grappling with telehealth implementation. This is the first narrative review of telehealth literature using a formal economics lens.
The remainder of this article is organized as follows: First, we summarize recent policy changes, followed by a brief background on telehealth. We then synthesize demand-side literature and supply-side literature, including discussion of the effect of telehealth adoption on health care costs and utilization. The next two sections focus on effectiveness of telehealth and health equity implications. Finally, we highlight important avenues for future economics research. Information on data for conducting empirical evaluations of telehealth is available in the supplements.
A New Era for Telehealth
The onset of the COVID-19 pandemic in March 2020 forced telehealth to the forefront of health care delivery, something that even 30 years of physician advocacy could not achieve. 2,4 In March 2020, when the first state-wide shelter-in-place orders were issued, the use of telehealth increased dramatically. Telehealth use peaked in April 2020 (Fig. 1), accounting for 29% of Medicare claims, 11,12 45% of U.S. Veterans Health Administration (VA) a health care visits, 10,15 –19 13% of private insurance claims, 14 and approximately 4−18% of Medicaid claims, depending on the state. 13 Although telehealth use began decreasing as COVID-19 restrictions were lifted, its use continued to exceed prepandemic levels. 14

Percent of services delivered via telehealth by insurance type, March 2019–February 2021. Notes: Graph redrawn using data from Rose et al., 10 Office of Inspector General report OEI-02-20-00520, 11 U.S. GAO report GAO-22-104454, 12 U.S. GAO report GAO-22-104700, 13 and FAIR Health Monthly Telehealth Regional Tracker. 14 Commercial and Medicare define telehealth as video, phone, store-and-forward, and remote patient monitoring. Veterans Health Administration (VA) data presented here includes video and phone telehealth visits only and does not include the estimated <0.1% telehealth for VA-purchased care outside VA. Medicaid data are based on state definitions of telehealth: Arizona, California, Maine, and Missouri include video, phone, store-and-forward, and remote patient monitoring, while Mississippi includes video and remote patient monitoring only. State telehealth policies available from the Center for Connected Health Policy: https://www.cchpca.org/). The Medicaid states were chosen by GAO based on achieving a range of total population, total rural population, the percentage of the state’s population without broadband internet, and geographic variation. 13 GAO, Government Accountability Office.
Prior to the pandemic, insurance reimbursement policies favored telehealth for specific types of care (e.g., psychiatric care), in limited settings (e.g., underserved, mostly rural areas), among populations facing severe supply shortages (e.g., prison populations and rural populations), or in case of emergencies. 4 To enable telehealth care during the pandemic, U.S. regulators loosened several policy restrictions and expanded coverage of telehealth services. Table 1 provides a summary of the key policy changes.
U.S. Policies Governing Telehealth Care Loosened During the COVID-19 Pandemic
Prior to the pandemic, the VA was the only exception to these licensing restrictions as the VA had loosened its out-of-state licensing restrictions in 2018, exercising its federal preemption to override state-specific telehealth laws.
CMS, Centers for Medicare and Medicaid Services; HIPAA, Health Insurance Portability and Accountability Act.
Although the COVID-19 Public Health Emergency ended on May 11, 2023, most federal pandemic-era telehealth policies were extended through September 2025. 23 However, the future of many telehealth policies, especially those governing nonmental health care, remains uncertain.
Telehealth is now a large industry, with a valuation estimated at $48.8 billion in 2023, 24 and estimates suggest that by 2030, the telehealth industry could be generating $144.2 billion in revenue. 25 Companies such as Amazon and Walmart 26 see the potential opportunities and are trying to gain market share through direct-to-consumer services. Given the expected growth and pressures on regulators, we highlight the central economic questions to inform telehealth policies and practices and avenues for future economics research on telehealth.
Background on Telehealth Care
Before we explore the demand- and supply-side factors affecting telehealth, a brief background is warranted. Telehealth is a broad label of services, and it is important to understand the different modalities and models commonly used for delivering telehealth care. In addition, telehealth is not a homogenous, single-use commodity. Its expected value depends on the health care bundle of services being consumed over time. Below, we describe what we mean by a health care bundle and highlight the three issues (modality, model, and bundle) that should be considered for a policy-relevant discussion of telehealth.
TELEHEALTH MODALITIES
There are various forms of telehealth, 2 broadly categorized into three types or modalities: asynchronous, synchronous, and remote monitoring. Services that do not use real-time communication between providers and patients are asynchronous. These include store-and-forward services and secure messaging, where information is transmitted to physicians or clinicians for review at a later time. These services have been around for over 30 years. 3 An example would be a primary care clinician sending an image to a dermatologist for consultation on a skin infection. The dermatologist then responds when available. Remote patient monitoring allows providers to track health care data for patients in a continuous or periodic manner. These patients can be in their homes or in other facilities, such as intensive care units. Synchronous telehealth involves real-time communication using interactive audio and audiovisual equipment, such as phone calls or video conferences between patients and providers. Interactions via synchronous video telehealth can more closely mimic traditional in-person appointments, but without the physical travel, synchronous audio and video telehealth grew in popularity during the COVID-19 public health emergency. 4,11,27 Health care treatment may require use of all three types of telehealth, as well as services that do not fall squarely into these categories. The distinction among telehealth modalities is important, as costs of each modality and their effectiveness 28 or acceptability can differ (e.g., some research indicates greater satisfaction with video compared with audio-only telehealth), 29,30 and relatedly, reimbursement policies can differ based on modality.
MODELS OF TELEHEALTH CARE DELIVERY
There are several models of telehealth care delivery. Hub-and-spoke models are considered the traditional form of telehealth, where providers located at a “hub” facility provide care to patients visiting local “spoke” facilities, often in medically underserved areas (Fig. 2). 31 –33 The hub-and-spoke telehealth model has been used to deliver care for opioid use disorder, 34 acute stroke care, 31 emergency care, 32 chronic pain care, and primary care. 35

Two distinct models of health care delivery: Hub-and-spoke model and home-based telehealth.
Home-based telehealth, where patients can stay in their homes or locations convenient to them and directly connect with providers (Fig. 2), grew dramatically during the pandemic. There are two paths for connecting patients directly with providers. The first is traditional “brick-and-mortar” providers, practices or health systems who typically provide care through in-person visits, also offering care via video and/or audio-only technology. 36 These visits are typically scheduled with a provider who has access to the patient’s medical records and can schedule an in-person follow up, if needed. 37 In contrast to “brick-and-mortar” providers offering telehealth, consumers also have the option to access direct-to-consumer telehealth. Direct-to-consumer telehealth is on-demand access to a health care provider for minor health care, typically provided through private companies. 5,37
However, not everyone has technology at their home to support home-based telehealth. To facilitate home-based telehealth, some health systems and communities have experimented by providing patients with smart devices such as phones or tablets. One example is VA’s tablets initiative, where video-enabled tablets or iPads were distributed to patients with barriers to accessing in-person care to facilitate patients’ participation in home-based telehealth. 38 Other health systems have also begun to leverage tablets to enable greater access to telehealth care for patients. 39,40 The Federal government also initiated efforts to connect patients with affordable internet access or affordable computer/smart devices with the 2023 Affordable Care Program (ACP); a survey from the program found that 72% of respondents used their ACP service to schedule or attend health care appointments. 41
Different telehealth models or programs may be aimed at addressing slightly different problems. For instance, hub-and-spoke models may aim to address staffing shortages in the local area while home-based telehealth and device distribution initiatives offer reduction in travel costs or logistical burden for patients in a way hub-and-spoke models do not. Thus, different models and programs have different impacts on health care access, care quality, and costs.
BUNDLED GOOD AND TYPES OF CARE
A health care visit is a bundled good. Grossman (1972) generalized the bundle as part consumption and part investment. 42 We extend this to note that a health care visit may include a diagnosis, a treatment, prevention activities, information exchange or a combination of these components. This bundle can vary over time and across patient needs; some visits may be focused mostly on treatment, while others may be focused entirely on information exchange. The types of care defined in existing medical or health economics literature, such as primary care, mental health care, or specialty care, may dictate or be correlated with the nature of a patient’s health care bundle. Adoption and effectiveness of telehealth may vary based on the composition of the health care bundle. For example, when interactions between providers and patients are discussion-based, such as for mental health care therapy and counseling or diagnostic visits in primary care, telehealth may be just as effective as in-person care. 43,44 This will not be the case for surgery, lab visits, and visits where physical exams are required. 45,46
However, in developing a robust economics literature on telehealth, it may be beneficial to directly discuss the underlying health care bundle, for which type of care is likely only a proxy. Conceptualizing health care visits as bundled goods can allow for examination of bundles across and within the traditional types of care and allow examination of the relationship between heterogeneity of the health care bundle and the adoption and efficacy of telehealth. For example, it may be easier to disentangle the effectiveness of telehealth in health care bundles with greater homogeneity such as for mental health care. One can conceive of other such homogenized bundles in health care settings within or outside mental health care. On the flip side, it is possible that there is lower adoption and effectiveness of telehealth for more heterogenous health care bundles, but these patterns have not been evaluated.
Furthermore, the composition of a health care bundle is often not known prior to the visit, and such uncertainty can affect the expected value of telehealth. Economic theory can contribute to the use of improved frameworks, such as the health care bundle described here, to guide more productive empirical hypotheses related to telehealth. Nevertheless, to synthesize the telehealth literature as it currently stands in medical and health services journals, we describe below the observed patterns of telehealth use across the traditional types of care.
Telehealth is most often used in outpatient settings (i.e., care that usually does not involve an overnight stay and has no written order to be admitted to a hospital) rather than inpatient settings (i.e., formal admission to a hospital typically involving overnight medical care). 47 A large literature in medicine describes telehealth by type of outpatient care and indicates that use of telehealth across care types is not uniform, with telehealth being used most frequently for mental health care. Before the COVID-19 pandemic, a study of commercial and Medicare Advantage data found that 4–5% of mental health providers delivered outpatient care via telehealth, compared with less than 2% of providers in all other specialties. 48 At the VA, mental health care alone comprised half of prepandemic video telehealth encounters. 49 During the pandemic, telehealth use grew dramatically across all care types: 18 49% of primary care providers used telehealth at least once during the pandemic, and use among specialty care providers ranged from 1% (chiropractic) to 68% (endocrinology). 48 However, mental health continued to comprise the largest proportion of telehealth encounters and had the largest percentage of visits occurring via telehealth. 18,48
Influence of Demand-Side Telehealth Factors on Health Care Use
Economists’ concept of fully-informed consumers rationally deciding on the quantity of health care services to purchase is clearly a simplification. 50,51 Nonetheless, this simplified model has proven useful as it allows us to understand incentives and behaviors in a complicated health care market. 50,51 In this section, we examine the influence of demand-side factors including patient preferences and costs to patients, and we discuss income and substitution effects on telehealth use.
PATIENT PREFERENCES
In MHS research, patients have generally expressed positive attitudes toward telehealth 29,52 –55 and patients report being open to the continued use of telehealth after the pandemic. 54 However, when studies have specifically asked about patient preferences for telehealth versus in-person care, in many instances, the majority report preferring in-person care. 29,45,56,57 As such, satisfaction with telehealth services may not imply a preference for telehealth versus in-person care.
Furthermore, preference for telehealth also depends on the type of care or the purpose of the visit (e.g., discussion of lab results vs. wound evaluation), 58 patient factors such as number of chronic conditions, 59 or the telehealth modality, with some research indicating greater satisfaction with video compared with phone only. 29,30
Medical research has shown that patient preferences for telehealth may differ by demographics. 60,61 A study of patient choice for in-person, video, or phone visits from 2018 to 2019 found that women versus men patients, Black versus white patients, and those aged 18–44 versus 45+ were more likely to choose telehealth (both phone and video), while Asian versus white patients were more likely to choose video telehealth, and Hispanic versus white were less likely to choose video telehealth. 60 When asked about their preferences for continued video use, research from 2020 indicates that older patients and Hispanic patients were less likely to prefer future telehealth visits. 61 However, observed telehealth use patterns do not always align with stated patient preferences. For example, while some studies found that Black patients are less likely to use video telehealth, others have shown that Black patients preferred telehealth over in-person visits. 60,62,63
The evidence may appear mixed because several underlying factors need to be teased apart. That is, the pattern of these reported preferences by demographics could be signaling underlying barriers or facilitators in adoption of telehealth. While telehealth use has grown dramatically during the pandemic, 18,27 barriers to adoption of telehealth for some patients remain, and may include factors such as lack of technical literacy, 64 physical impairments, 65 lack of reliable internet or a device, 66 –68 and lack of physical examinations. 54 It can be difficult to disentangle whether these groups are not able to use telehealth, do not prefer telehealth, or are facing underlying access issues. Conversely, some factors that motivate telehealth use include patient unease in a particular health care setting or lack of confidence in their ability to advocate on their own behalf, 59 greater cost-sharing burden for in-person care, 60,69 or longer travel distance or other transportation issues. 60
For instance, telehealth use is generally seen to be lower among older adults in the MHS literature. However, prior work utilizing quasi-experimental survey data have shown that older adults were just as likely as (and sometimes more likely than) younger adults to use electronic health information when there is an intervention that gives them the opportunity to do so. 70 Recent papers evaluating telehealth interventions using econometric techniques have similarly shown that when the same groups considered to have low uptake historically are given the opportunity to access telehealth, they adopt similarly to everyone else. 38,71 Another recent economics study which utilized a difference-in-difference approach found that telehealth care increases during the pandemic were driven by older individuals with preexisting conditions. 72 These findings suggest that employing causal inference methods may lead to a reversal of traditionally held notions based on MHS literature in some cases. Findings also suggest that more equitable and widespread adoption of telehealth is possible if there are tailored strategies to address barriers affecting patient adoption. 65,73
Economics research can disentangle the extent to which patient preferences, barriers, abilities, needs, and the type of health care bundle drive use of telehealth by employing causal inference techniques and discrete choice experiments aimed at eliciting patient preferences. 74 –77 For example, a discrete choice experiment conducted in the United Kingdom in 2018 found that “busy young professionals” (younger, nonwhite women who worked full-time and were unmarried), expressed a lower strength of preference for face-to-face visits and placed a higher value on convenience with telehealth visits, providing a more nuanced understanding of the type of patient who may prefer telehealth. 57 Furthermore, given the majority preference of in-person over telehealth visits, it is likely that other aspects of telehealth, such as logistical convenience or privacy offered in telehealth visits, contribute to patients’ use of telehealth over in-person care. Economics research can contribute by isolating the effects of these various factors. In addition, as telehealth is unlikely to replace in-person visits altogether, it will be important to study the optimal mix of care modalities for varying health care bundles. 78
Patients’ Cost or Price of Telehealth
MONETARY COSTS
As a result of health insurance, a central feature of health care markets is that patients do not bear the full costs of the health care they consume, 79 resulting in the classical problem of moral hazard. 80 Because health insurance shields patients from the direct costs of care, patients are likely to consume more health care than they would have if they faced the prices paid by insurers. Patients’ monetary price of telehealth is defined as their out-of-pocket payment, which for insured patients is the amount paid out-of-pocket through copayments, deductibles, or coinsurance.
There is considerable variability in coverage and patient out-of-pocket costs for telehealth visits across different insurance providers and states. Table 2 provides an overview of patient cost sharing requirements and coverage for telehealth by various insurers.
Patient Costs of Telehealth by Insurance Type
For DTC telehealth, visits without insurance start around $89 in 2025. 89 For uninsured patients, this is lower than the cost of an in-person physician’s office visit, and much lower than an emergency department (ED) visit. 5 However, while lower per visit cost may make health care more accessible for patients without insurance, if DTC telehealth leads to a greater number of visits, these cost savings may be limited. 5
NONMONETARY COSTS
When measuring patient costs of telehealth, it is also important to consider opportunity costs associated with the choice of modality for a health care visit. Cost avoidances related to time, travel, and employment are benefits of selecting telehealth appointments over in-person care. Nonmonetary patient costs that have been considered in existing MHS literature include missed paid work, travel time, and in-person access barriers. 3 For instance, Jacobs et al. found that 45% of survey respondents reported that tablets for video-based health care saved them paid time. 90 Berlin et al. used patient address data from March to May 2020 to estimate a median per-person travel cost savings of CAD$136.5 (public transportation) to CAD$142.9 (private transportation). 53 Reed et al. found that patients who had to pay for parking for in-person visits were more likely to choose telehealth. 60
While these types of nonmonetary costs are important from the patient perspective, they have not been included in the majority of existing telehealth cost studies, which have largely been conducted from a health care payer perspective. 77,91 However, a 2010 systematic review found significant differences in conclusions surrounding telehealth cost savings depending on whether or not these costs were included. Whenever costs from the patient perspective, including consideration of nonmonetary costs, were included in analyses, telehealth interventions were found to be cost-saving, whereas when the health care payer perspective alone was adopted, the proportion of studies reporting cost savings reduced to half. 92
INCOME AND SUBSTITUTION EFFECTS OF TELEHEALTH
Economic theory broadly suggests that higher income and/or lower prices would increase consumers’ or patients’ use of health care. 51 This framework of income and substitution effects is also useful as we consider below the effects of price changes of telehealth care and of income changes on the demand for telehealth care.
EVIDENCE ON INCOME EFFECT
Many MHS studies on telehealth discuss income effects. Comparing patients living in lower socioeconomic areas with patients living in higher socioeconomic areas, a majority of studies found higher socioeconomic status to be correlated with greater telehealth use. 93 –96
Studies looking at telehealth by modality have found lower video use (vs. phone) among those with lower socioeconomic status. 60,62 Studies also indicate that insurance type is associated with telehealth use, with patients covered by commercial insurance being more likely to use video telehealth. 62 In a comparison of video versus phone telehealth visits, studies have found patients with Medicaid (vs. commercial insurance) were less likely to complete a video visit. 62 However, not all research supports this income effect. Qian et al. used data from Kaiser Permanente Southern California and found that low-income groups experienced the greatest increase in telehealth (video and/or phone) during the COVID-19 pandemic. 97
While several studies signal that there are income effects for telehealth care, the existing evidence compares outcomes between individuals in richer or poorer areas or individuals in different income quartiles, such that there may be confounding differences across these groups. This evidence can be strengthened through quasi-experimental methods or through randomized experiments.
EVIDENCE ON SUBSTITUTION EFFECT
While there is evidence in the economics literature that greater monetary cost-sharing decreases health care use broadly, 98 the number of studies analyzing the effect of prices patients face for telehealth care (e.g., copayments) on health care use is limited. Two studies using Kaiser Permanente data found that patients were more likely to choose telehealth when faced with higher copayments for in-person visits. 60,69 Using a willingness-to-pay analysis, Predmore et al. found that among those who preferred in-person care for nonemergent services, 50% maintained their preference even at a higher cost, while among those who preferred telehealth for nonemergent services, only 19% continued to do so when the cost increased. 56 While these studies suggest that patients’ lower cost of using telehealth may impact their choice to use telehealth more frequently, Tauscher et al.’s willingness-to-pay analysis focusing specifically on substance use disorder treatment, found that participants were willing to pay $4.38 more a week for home-based video telehealth counseling versus in-person care. 76 Additional studies and more robust methods can greatly complement this literature.
Future Demand-Side Research
With multiple policy changes in recent years to encourage telehealth use during the COVID-19 pandemic, there are ample opportunities for economics studies to contribute to understanding the effect of demand-side factors such as insurance coverage expansions on telehealth adoption. 99 As policymakers consider optimal insurance coverage policies that avoid distorting patient incentives to curb health care costs, it is necessary to understand the causal impact of both monetary and nonmonetary price changes faced by patients on the adoption of telehealth. There is also room for more studies, with better causal identification, on the income effects of telehealth. Studies should also utilize controlled experiments and econometric strategies to evaluate causal impact of the changes in insurance or government policies (e.g., the COVID-19 pandemic era policies) to elucidate patients’ responsiveness to income changes and insurance or price changes related to telehealth care. 99 Estimation of telehealth demand elasticities among different conditions, health care bundles, and telehealth models can inform future reimbursement, patient cost-sharing, and coverage recommendations.
Influence of Supply-Side Telehealth Factors on Health Care Use
PAYERS OF HEALTH CARE, MORAL HAZARD, AND ADVERSE SELECTION
Many of the central concerns from standard health economics literature are also paramount when discussing the economics of telehealth, including patients’ imperfect information, moral hazard, and other distortions of patient and provider incentives due to health insurance, supplier induced demand, and adverse selection. In the sections below, we first describe the providers’ role in delivering telehealth care, as well as their incentives and preferences. We then discuss the cumulative cost concerns of payers or insurers.
Providers, Their Perceptions of Telehealth, and Incentives
THE ROLE OF PROVIDERS
In the U.S., insurers generally pay for care that is deemed medically appropriate. Thus, physicians or clinicians with medical expertise typically determine treatment appropriateness or the relative merits of health care treatments. 51 Supply-side economic models typically assume patients are uninformed agents who largely trust their providers with medical expertise to determine the right treatment. 51 Providers may thus be seen as imperfect agents for patients, such that provider utility depends on the benefits to the patient, as well as providers’ own net benefits, that is, provider fees earned minus the costs of providing those services such as malpractice-related costs 100 and practice-related costs, which include general overhead expenses such as supplies, equipment, and billing costs. 51,101 Practice costs specific to telehealth may include factors such as laptops with webcams and virtual visit software. 101
Much like the large role providers play in determining treatments for patients, providers also play an important role in patients’ use of telehealth. 102 Providers likely use their clinical judgement to assess whether telehealth is appropriate, 103 taking into account a patient’s medical condition and specific care needs. The provider considers the telehealth modality and model, among available options, and the health needs bundle for each patient. Thus, insurers’ concern about health care costs increasing due to potentially provider-induced demand remains a prevalent concern in the case of telehealth care. However, the extent to which medical expertise is required for the choice of telehealth versus in-person modality is unknown. The extent to which the modality decision rests with patients vs. with providers also remains unknown. This is an important future area of research as the information asymmetry that typically complicates the health care market due to required medical expertise may be a less critical a factor for decisions about treatment modality (telehealth vs. in-person or phone vs. video telehealth) as it is for treatment choice. Rigorous research on the effectiveness of modalities may reduce such information asymmetry and may thereby reduce, though not altogether eliminate, potential provider-induced demand.
PROVIDERS’ PERCEPTIONS
The empirical evidence in MHS literature on providers’ attitudes suggests that much like patients, providers express positive attitudes toward telehealth. 53,102,104 Studies have found that the majority of clinicians preferred to continue providing some care via telehealth after the COVID-19 pandemic. 105 However, provider perceptions and use of telehealth can be dependent on factors related to the technology itself such as audio/image quality, 104 broadband coverage in the area, 106 ease of use, and prior telehealth experience. 102,106 Provider use of telehealth can also depend on factors such as provider type (physician or nurse), 58 provider specialty, 46 location of care (e.g., outpatient, inpatient, ED), 105 and purpose of visit. 45,58,107
Taken together, the current MHS research indicates that providers have positive feelings toward telehealth, although they generally indicate that video telehealth is preferable to phone telehealth, 103 and in-person care is superior to any telehealth. 45,102,104 Given that physician exams are a key factor in the preference for in-person care, these preferences could change depending on the type of care and health care bundle. To date, provider preferences have not been investigated in the economics literature.
PROVIDERS’ MONETARY INCENTIVES
Despite the push for more value-based payment models, a 2022 study of health system-affiliated provider organizations found that volume-based payments, rather than value-based payments, were still the most common form of base compensation for physicians, and increasing service volume was the most commonly reported action providers could take to increase their compensation. 108 Given the current prevalence of fee-for-service model among Medicare, Medicaid, and commercial insurers, payers are particularly concerned about cost increases due to telehealth. The concern is that volume-based payments under fee-for-service encourage additional and potentially inefficient use of telehealth care. Concerns about provider-induced demand are thus exacerbated in the case of telehealth. That is, self-interested providers being paid under a fee-for-service system may be incentivized to offer more care visits through potentially inefficient use of telehealth. Furthermore, generous insurance coverage of telehealth may also offer strong incentives for providers to compete by employing innovative yet costly telehealth technologies. 50
However, the extent to which providers respond to payments for telehealth care is not well-researched. In one qualitative study of primary care patients, providers expressed positivity toward the fact that telehealth reimbursement now allows them to bill for evaluation services, such as calling patients with test results, that they would typically provide without reimbursement after an in-person visit. 107 Existing research in the MHS literature indicates that telehealth payment parity is associated with greater telehealth utilization. 109 However, these studies are unable to make causal claims due to the methods used, 109 and robust studies are needed. There is also a need to distinguish between increases in necessary vs. unnecessary care due to telehealth use.
PROVIDERS’ NONMONETARY INCENTIVES
Just as it is important in the case of telehealth to consider patients’ time and travel costs, it is also important to consider these costs for physicians or other clinical staff. 3 For instance, a study of telepsychiatry for rural nursing home residents found the program saved between $84,347 and $232,000 in physician travel costs and 35 days of travel time for 278 encounters. 55 If clinicians save time through their use of telehealth, and use these time savings toward providing more care, then telehealth use offers efficiency gains in the form of clinician productivity. If providers’ use of telehealth saves them personal time, then these personal time savings should also be considered in cost analyses conducted from a societal perspective. Providers’ leisure time savings could also affect their incentives 110 to adopt and use telehealth. Telehealth may also pose additional psychological malpractice concerns for clinicians, but this topic has been rarely discussed in prior work. 100,111 There is very limited MHS literature and no economics literature on the impact of telehealth on provider productivity, and the existing medical research evidence is mixed. 112,113 There are also virtually no studies on the topic of how leisure time savings or travel time savings for providers may affect their adoption of telehealth.
HOW DOES THE INTRODUCTION OF TELEHEALTH AFFECT PAYERS?
Governments and private health insurers who reimburse providers for their medical services are particularly concerned with adding features to health care delivery that will increase costs without commensurate benefits. These concerns are the most widely cited reasons for the historical lack of policies covering telehealth services. 1,3,5 –7 There are three key mechanisms of cost increases that concern payers: (1) telehealth care may be inefficient or less effective than in-person care for the same purpose, requiring additional follow-up visits, (2) moral hazard, that is, patients may be incentivized to consume more health care if their costs are lower when using telehealth, and (3) under fee-for-service payment models, providers may be incentivized to provide low-value care via telehealth to generate higher revenue.
Telehealth may be less efficient compared with an in-person visit for certain types of care, increasing the cost of care per episode. For instance, telehealth may be particularly efficient when a patient wants information 114 and/or seeks discussion-based treatments, such as psychotherapy. Telehealth can be less efficient than in person care when the clinician needs to make a diagnosis or there is ambiguity in the reason(s) for the patient to seek care.
In the context of telehealth, moral hazard could arise through a couple different mechanisms. If patients respond to changes in nonmonetary costs, then the reduced time costs of telehealth may lead to overconsumption of telehealth care. 5 Decreasing monetary costs for patients in the form of reduced copayments, deductibles, and coinsurance could also exacerbate this moral hazard problem. Furthermore, if telehealth and in-person care are complements, then increased use of telehealth due to lower monetary or nonmonetary costs could lead to increased use of in-person care, increasing total health care costs. 5,115
Adverse selection can also arise when patients select into health plans. In an economics study, Grandchamp et al. demonstrated that in a Swiss health insurance plan, a mandatory telehealth call before an in-person visit led to lower expenditures on average because healthier patients selected into this type of plan. 116 While the use of telehealth for triage in this case led to adverse selection which lowered costs for the insurer, the reverse is also possible. For instance, high-users of expensive telehealth technologies self-selecting into insurance plans with higher coverage of telehealth 77,116 may increase costs for insurers if insurers cannot achieve adequate pooling or balance of high and low users of telehealth. Such self-selection also poses problems for researchers evaluating telehealth initiatives. If high-users of telehealth are less sick than patients who need in-person visits, and these patients select into more generous telehealth coverage plans, the effectiveness of telehealth may be overstated without addressing this type of selection.
Given that there are several cost-increasing mechanisms due to widespread adoption of telehealth, the reluctance and skepticism of payers is understandable. However, payers may not see investments in telehealth as a lost cause if telehealth can lead to cost savings through (1) an overall reduction in utilization, 3 (2) a substitution of physician office visits and ED visits with less expensive virtual visits, 5 (3) a reduction in production costs through efficiency gains, or (4) if telehealth results in cost-effective improvements in patient outcomes.
Production Costs
Producing health care involves variable costs (i.e., labor and supplies) and fixed costs (i.e., capital investments in space, technology, and overhead). Telehealth has the potential to change the production costs for providers. While we outline the key types of costs below and highlight the existing MHS literature, formal economic modeling can be particularly helpful for elucidating the costs and their dynamics and for building an empirical literature on strong foundations.
Fixed Costs
A health care provider will need to invest in telehealth technology, which will increase their fixed costs. At the same time, using telehealth instead of seeing patients in brick-and-mortar offices can help providers save time and costs of renting space to run a medical practice. 3 Telehealth may also reduce overhead and administrative costs. A scoping review found that cost savings from telehealth occurred only after a certain caseload was exceeded, offsetting the initial investment costs. 7 However, research evidence on fixed costs of telehealth remains limited. 112,117
Variable Costs
Variable costs, or costs that fluctuate based on volume of activity, could be potentially decreased through improved factor productivity or through economies of scale. A 2021 study using VA data from 2010 to 2018 found that clinicians who provided high levels of care via telehealth also had the highest levels of productivity based on relative value units (RVUs), compared with non-telehealth providers. 113 Another study found lower costs per episode of care delivered via an online clinic Virtuwell compared with care delivered in clinics, and urgent/emergency care settings. 118 Telehealth may also reduce missed appointments and no-shows (which some estimates suggest cost the U.S. health system $150 billion/year) 119 and also improve clinical efficiency. 120,121 By increasing input or clinician productivity and clinical efficiency, telehealth can reduce variable costs for the same level or quality of care but further research is needed.
Implementation Costs
Implementation costs may include both fixed and variable costs. Implementing telehealth not only requires specialized technology to meet information security standards, but staff need to be trained and monitored, and then systems need to be modified to handle regulatory changes. High training costs or resource-intensive collaborative telehealth programs can lead to increased health system costs. 122 Estimates of implementation costs are severely lacking in the telehealth literature.
Input or Factor Prices
Input or factor prices may include both variable and fixed costs. Telehealth offers opportunities for some health care providers to reduce the cost of production by taking advantage of lower factor prices elsewhere. Heath care providers in high-wage areas such as San Francisco and Boston can save money by employing clinical staff in lower wage markets to handle telehealth care.
The “gig economy” has flourished in part because it enables organizations to change the costs of production. 123 Start-ups are looking at health care with the same opportunity. 124 If telehealth can be staffed with contractors using their own homes, then telehealth has the potential to reduce fixed and labor costs. Very few studies have rigorously examined the impact of telehealth on input or factor prices.
Evidence on Telehealth’s Impact on Total Health Care Use
In the sections below, we consider the empirical evidence on the impact of telehealth care on total outpatient visits and then consider the impact on costlier or more downstream ED and inpatient visits. To allow for a 15-year evaluation period, we limited our review to articles published from 2009 to 2024, focusing on studies that evaluated utilization or cost impacts due to telehealth introduction. We prioritized inclusion of studies with more robust study designs. Although the goal was to conduct a selective narrative review, we ensured that this review represents the state of the evidence broadly.
Impact of Telehealth on Outpatient Care. Is Telehealth a Substitute or Complement?
As described earlier, a key economic concern for payers is the extent to which use of telehealth increases total care. Telehealth may merely substitute for in-person care, but there are concerns that it could increase total care, by either increasing complementary in-person care or complementary telehealth care or both.
Fig. 3 provides an overview of 32 studies reporting on the impact of outpatient telehealth service use on total outpatient utilization, signaling whether telehealth was a substitute for in-person care or a complementary form of care (detailed summary is provided in Supplementary Table A1 in Supplementary Appendix). The rapid expansion of telehealth during the pandemic has been accompanied by a growing body of MHS literature on telehealth as well as a nascent economics literature. However, many of the newer studies relied on data prior to the pandemic. 28 studies were from the MHS literature while 4 studies were published in economics journals. The studies comprised 2 randomized controlled trials (RCTs), 2 patient survey studies, and 28 studies analyzing administrative and clinical data.

Overview of studies reporting on telehealth as a substitute or complement. RCT, Randomized Controlled Trial.
Clinical trials largely found telehealth to be a substitute for in-person care, with modest increases in total care. 121,125 Studies relying on patient surveys broadly found telehealth to be substituting for in-person care. 118,126 Hypothetical bias may be present in some survey studies because respondents were being asked to discuss their decision-making process for a decision they never actually faced. Psychology and behavioral economics suggest that people who ultimately took an action such as elected to use telehealth may be more likely to report that they would have taken another action such as going to another care setting instead of not taking any action at all. 5 This bias can lead to over reporting of telehealth as a substitute rather than telehealth as a complement in survey studies. Additional RCTs and survey studies that employ quasi-experimental techniques can improve the current evidence base.
As studies of administrative and clinical data dominate the evidence, we describe these more closely in Fig. 4. Among these 28 studies, most studies (n = 15) were from the prepandemic period. Next, relatively few studies focused on underserved populations. 6,35,38 As telehealth has long promised improved care access for underserved populations, examining underserved populations when considering the impact on total care is important to inform policies. We found that studies were distributed across several types of care and across various telehealth modalities. A total of 15 studies focused on various types of primary care, 5,35,37,78,127 –137 5 focused on mental health care, 6,38,138 –140 and 1 on specialty care; 141 while others did not distinguish between the different types of care. 27,142 –146 Among the 28 studies, only 10 evaluated synchronous video telehealth as distinct from other modalities, but 14 studies combined video with phone and other modalities (Supplementary Table A1 in Supplementary Appendix). There were virtually no studies isolating the impact of phone telehealth. Given recent policies increasing coverage of phone telehealth, it is important to examine how phone telehealth impacts total care and costs. Isolation of telehealth modalities was especially difficult in studies of clinical and administrative data prior to the pandemic and early into the pandemic due to evolving telehealth codes (Supplementary Appendix). As the data improves, new studies isolating the effect of different telehealth modalities within each care type are needed to provide actionable insights.

Overview of studies relying on clinical and administrative data.
Among studies that utilized at least some postpandemic data but had different conclusions about whether telehealth was a substitute or both a complement and a substitute, a key methodological difference was whether they evaluated utilization pre–postpandemic or pre–post telehealth exposure. Studies that compared utilization patterns pre–postpandemic, typically found telehealth to be a substitute for in-person care, meaning they found no increase in the total volume of care (Supplementary Table A1 in Supplementary Appendix). However, as utilization was declining postpandemic, it may be more appropriate to use methods that compare utilization pre–post telehealth exposure while also adjusting appropriately for the effects of the pandemic. In studies that evaluated the effect of telehealth on total care using strong methods that compared treatment and control groups before and after telehealth exposure (Fig. 5), telehealth care was associated with increases in total outpatient care, regardless of care type or analysis period. 5,38,78,130,137,141,148
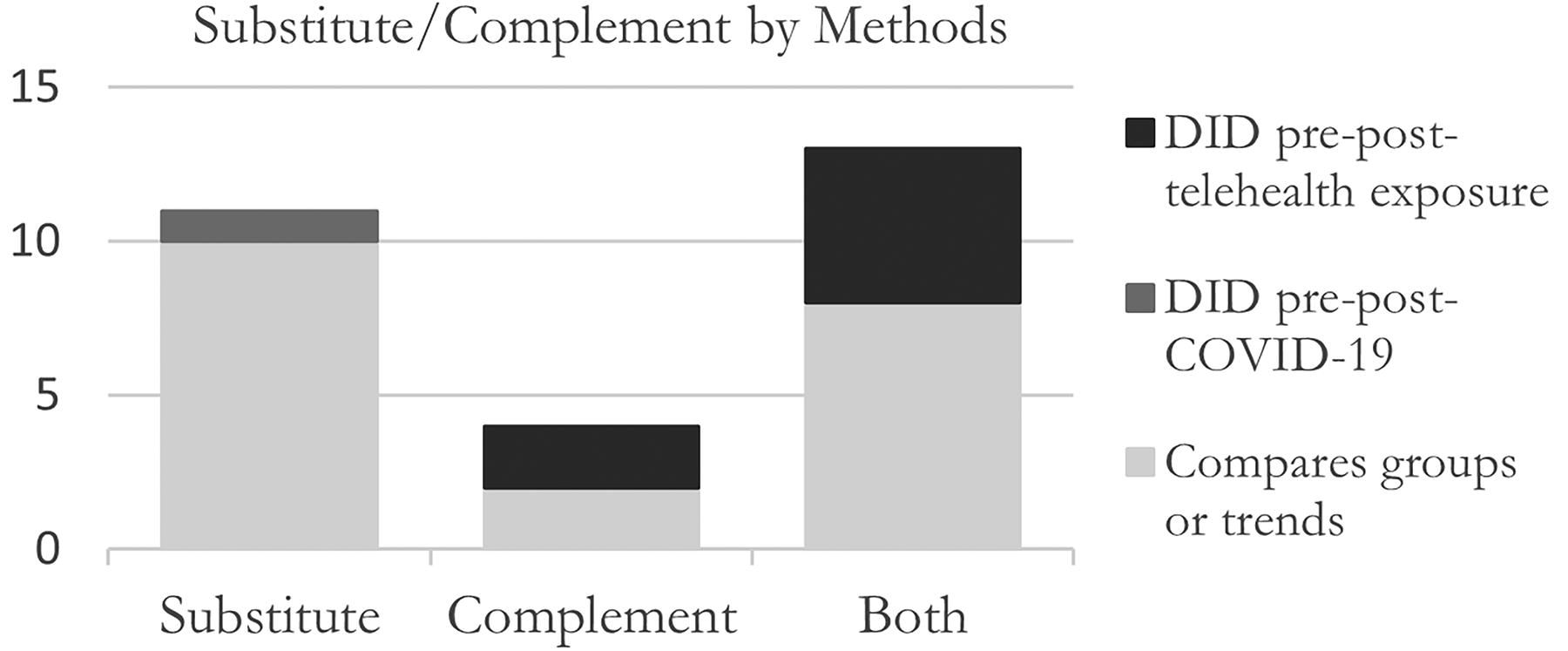
Telehealth as a substitute or complement, by study methods. We included Liu et al., 147 which compares groups or trends, as a “complement,” reflecting their findings across most types of care, but they find telehealth to be a substitute for mental health care. DID, difference-in-difference.
While some prepandemic studies indicated large increases in outpatient care, it is at least somewhat reassuring that in studies of more recent data, when telehealth use is associated with new or additional care visits, the increase is generally modest; for, Chen et al. found one additional visit per year 127 and Zeltzer et al. found a 3.5% increase in the volume of primary care visits. 78
Impact of Telehealth on ED and Inpatient Use and Costs
Next, we consider evidence on telehealth’s impact on costly ED and inpatient care, where reduction of ED and inpatient care may also signal the effectiveness of telehealth care, highlighting an area of positive patient health benefits from telehealth. We found 22 studies addressing this question in the MHS literature and 3 studies in economics journals (Supplementary Table A2 in Supplementary Appendix). A 2023 RCT evaluating data prepandemic found that telehealth lead to reduced hospitalizations and ED visits, 149 consistent with earlier prepandemic reviews focused on clinical trials. 150
Among 22 studies utilizing administrative and clinical data to examine telehealth’s impact on ED or inpatient care (Supplementary Table A2 in Supplementary Appendix), 11 utilized data only from the prepandemic period and 11 used at least some postpandemic data. While studies of prepandemic data broadly found that ED or inpatient care decreased, drawing conclusive insights is difficult, because only five of the prepandemic data studies 88,134,151 –153 used strong methods like the difference-in-difference (DID) design which have the advantage of addressing unobserved confounders and pre-exposure levels of ED and inpatient care. In addition, settings of outpatient telehealth care varied and many of the prepandemic studies focused on asynchronous modalities or lumped together asynchronous and phone-and video-based care.
Fig. 6 summarizes the 22 studies by methods, including studies of pre- and post-pandemic data. Only 10 of the 22 studies used a DID design to compare a telehealth exposure group and a control group in a pre–post exposure setting. 38,78,88,134,137,148,151 –153,155 Studies with more rigorous methods found no impact on emergency or inpatient care. However, additional studies with newer data and the ability to isolate telehealth modalities used in outpatient settings are critically needed.

Telehealth’s impact on ED and inpatient visits, by study methods. Note: Peters et al. 154 is included as a single RCT but this article is a systematic review and meta-analysis. In their meta-analysis of 76 RCTs that evaluated risk of all-cause hospitalization, they found that telehealth reduced the risk of all-cause hospitalization by 18 per 1000 patients. They did not analyze the downstream effect on ED visits. DID, difference-in-difference; ED, emergency department; RCT, randomized controlled trial.
Net Impact of Telehealth across Outpatient and Inpatient Care and Costs
The literature to date does not provide a consensus on the overall cost savings of telehealth compared with in-person care. 7 Certain costs are consistently lower with telehealth, particularly savings from reduced patient and provider travel costs. 7,156 However, as described earlier in the patient costs section, patients’ nonmonetary costs have largely been overlooked, as most studies have been conducted from a health care payer perspective, 77,91 and telehealth interventions were more often found to be cost-saving when the patient perspective was included. 92
From the perspective of insurers, the impact of telehealth on monetary costs is closely tied to the utilization patterns discussed above, and it is important to balance the costs impact of telehealth on increases in total outpatient visits and any reduction in follow-up care or costly ED and inpatient care. Our review of the current evidence for outpatient and inpatient health care utilization suggests that telehealth adoption can modestly increase overall outpatient health care use and costs but the evidence on its impact on downstream costlier ED or inpatient use is currently mixed. Furthermore, as described earlier in the production costs section, there is a lack of analyses examining how telehealth can alter production costs or efficiency, although the limited evidence that exists hints that telehealth may achieve saving in production costs once a certain threshold is hit. 156
Effectiveness of Telehealth
It is critical to discuss the effectiveness of telehealth, as this is a topic of concern for all stakeholders: patients, clinicians, and payers. Patients and clinicians (imperfect agents for patients) want the care provided through telehealth to improve patient health, and payers’ concerns of telehealth offering low-value care can be reduced if telehealth care is effective or high-value. Even if value-based payments become the future dominant payment model for health care services, which can reduce payers’ concerns about distorted clinician incentives driving up low-value care expenditures, the quality of the care delivered through telehealth still needs to be evaluated.
Although studies have demonstrated the feasibility and acceptability of telehealth for many types of care, 150,156 there remains a lack of comparative effectiveness studies in both MHS and economics literatures showing that telehealth is just as effective as in-person care across different care types. 73 Even within mental health domains where many clinicians consider telehealth to be just as effective, recent medical evidence syntheses point to weaknesses in the study methods. 157,158 Moreover, there is also a critical lack of high-quality studies comparing the effectiveness of video versus phone telehealth. 157,158 Our own review of studies examining ED and inpatient care use, described earlier, found that studies with strong methods were sparsely distributed across care types, modalities and pre- and post-pandemic periods, making it difficult to draw strong conclusions about ED and inpatient care use.
There is also a lack of studies linking the modality of care (in-person vs. any telehealth or video vs. phone) to clinical health outcomes. A recent economics study 151 found that greater access to telehealth via laws that equalized cost-sharing for telehealth and in-person care decreased mortality rates by approximately 6–9%, driven by decreases in ischemic heart disease deaths. Additional studies evaluating health outcomes are needed.
Further, differential effectiveness across telehealth modalities can also have important health equity implications for patients without access to video telehealth. 159 As use of phone- and video-based care has grown dramatically post-onset of the COVID-19 pandemic, it is paramount to evaluate the effectiveness of greater reliance on these telehealth modalities across the different care types or for different health needs bundles for individuals in the postpandemic era. Such studies will be critical for shaping policy discussions as they will enable understanding of the clinical value provided by telehealth, which can then be weighed alongside the costs of telehealth.
Health Equity Implications of Telehealth
Telehealth has long held the promise of expanding access to high-quality health care, overcoming not only geographic but sociodemographic barriers. 3 MHS literature has long suggested that telehealth can reduce health care access barriers related to distance and travel, enabling improved access to care for patients in rural or underserved areas. 38,49,160 MHS studies have also found greater use of telehealth among women, 161 signaling that telehealth may ameliorate barriers to care access disproportionately faced by women, such as logistical and travel difficulties and greater time constraints due to caregiving burden. While one economics study has shown that increased telehealth access improved health outcomes among nonmetropolitan patients, 88 additional economics studies are needed to understand the access and equity implications of telehealth.
Rapid and large-scale reliance on telehealth in the postpandemic era may also exacerbate health disparities due to patients’ differential access to technology or broadband internet. A rapidly emerging MHS literature has shown that technology necessary for video telehealth varies by sociodemographic characteristics. Studies comparing video vs. phone telehealth use during the COVID-19 pandemic have found lower odds of video visits among Medicaid or Medicare recipients, 162 older patients, 62,63,162,163 Black patients, 62,63,162 Hispanic patients, 62,63,162,163 patients with limited English proficiency or who were Spanish-speaking, 63,164 lower-income patients, 62,63 patients with lower educational attainment, 63 and people residing in rural areas. 163
Studies comparing telehealth (video or phone) to in-person visits generally found similar patterns, with the key difference being that when studies defined telehealth as either phone or video telehealth, they found higher telehealth vs. in-person use among Black patients compared with other groups, 62,165 suggesting that Black patients may be more reliant on phone-based care. This difference by modality may be partially explained by differential access to video telehealth technology: A 2024 study found that while telehealth narrowed the gap in health care utilization by race for Black and Hispanic patients, this advantage was limited to those with access to high speed internet. 166 At the same time, among those with high speed internet access, disparities by sex, rurality, and income still persisted. 166 indicating that technology access alone does not explain the disparities in telehealth use.
Despite the recent and rapid emergence of a vast MHS literature on telehealth and disparities, the evidence offers some mixed insights and varies across settings of care, telehealth modalities, and types of telehealth programs. There is a dire need for high-quality cost-effectiveness studies comparing visit modalities among important sociodemographic groups. 73 A 2021 study looking at hospitalizations following primary care telehealth visits found that among those who used telehealth, Black patients and patient age 85+ had greater odds of an avoidable hospitalization. 165
Studies utilizing econometric techniques can disentangle the effects of telehealth programs or policies for different sociodemographic groups. For example, recent evaluations utilizing difference-in-difference methods suggest that distribution of VA tablets, which remove the barrier of owning a smart device, improved mental health care among rural Veterans, Black Veterans, and women Veterans. 38,71 This research suggests that improved access to telehealth technologies and broadband internet have some potential to level the field for historically disadvantaged groups through producing roughly equivalent increases in health care use for all sociodemographic groups.
Federal programs such as Lifeline and the 2023 Affordable Connectivity Program are now offering discounts on phone and internet bills as well as one-time discounts for laptops, tablets, or desktop computers for eligible low-income households. Econometric methods can be used to examine the impact of greater technological and internet access enabled through these interventions on telehealth adoption and on health disparities. Furthermore, as discussed earlier, there are signals of income effects for using telehealth. Economics studies can contribute to designing optimal policies that counterbalance such income effects to ensure that low-income households can access the benefits of telehealth. Without targeted policy efforts for underserved populations, telehealth may never achieve the promise of reducing health inequities and could instead exacerbate disparities. A recent economics literature on technological advances in the field of artificial intelligence raises similar concerns about rapid adoption of technology and the importance of designing policies aimed at reducing related inequities. 167 Acemoglu and Johnson argue that “there is nothing automatic about new technologies bringing widespread prosperity. Whether they do or not is an economic, social, and political choice.” 167
Conclusions
In this article, we presented the central economic concepts of telehealth care and summarized the relevant empirical evidence. The existing telehealth literature is sparsely distributed across types of care, telehealth modalities such as video or phone telehealth, and telehealth models such as direct-to-consumer or regional hub-and-spoke telehealth programs. The vast MHS literature lays strong foundations for developing an economics literature on telehealth. Addressing the telehealth modality and model, as well as the bundled nature of medical care, can greatly enhance telehealth literature. Economics studies can contribute significantly toward building a policy-relevant evidence base through elucidating costs and benefits of telehealth. There are ample opportunities for quasi-experimental studies and randomized controlled experiments. Theoretical economic modeling can also be used to improve frameworks and empirical hypothesis development, such as by studying the dynamics of decision-making and considerations of incomplete information.
We described numerous policy changes in telehealth coverage, patient cost-sharing, reimbursement policies, privacy restrictions and expansions of telehealth programs in recent years. The widespread uptake of telehealth across health systems and the multiple policy changes offer many opportunities for policy evaluations of telehealth using large-scale data. Economics literature has slowly begun to explore these avenues, with recent research suggesting that telehealth coverage parity can reduce health care expenditures, 168 and even decrease mortality rates. 151 Other recent studies utilizing econometric techniques are similarly providing important insights, and in many cases challenging and reversing conventional notions on the topic. 38,71,78,88,112,168
The historic landscape of telehealth suggests that supply-side incentives, in particular payers’ incentives, have been the greatest driver of the role of telehealth in health care delivery. It is likely that these incentives will continue to play an important role even in the postpandemic era. The primary concern payers have is whether greater use of telehealth will drive up low-value health care use and increase health care costs. To address payers’ concerns about distorted patient and provider incentives, an important area to study is patients’ responsiveness to price and income changes. Economics research is needed for estimating the monetary and nonmonetary price elasticities of demand, as well as income elasticities of demand. Demand elasticities can inform payers’ concerns about moral hazard and contribute to recommendations for demand-side cost-sharing as well as targeted policies for low- or high-income patient groups. Economics studies examining the impact of monetary and nonmonetary incentives for clinicians to estimate the elasticity of supply can lead to recommendations for provider reimbursement policies.
In addition to concerns of distortion of patients’ and providers’ incentives, payers worry that telehealth visits are less efficient than in-person visits and will thus result in more follow-up visits and costs, where the additional visits may occur via telehealth or in-person and may occur in outpatient or inpatient settings. We examined the current evidence on this topic and found that most rigorous studies of administrative and clinical data, from the prepandemic era as well as the postpandemic onset period, found that exposure to outpatient telehealth care often led to increases in total outpatient care, albeit modest in most cases. These studies found that while exposure to telehealth led to substantial substitution of in-person visits with telehealth visits, telehealth visits also led to complementary or follow-up care whether through in-person or telehealth visits. As such, we expect there to be some increases in the cost of outpatient care due to telehealth adoption.
It is possible that expected increases in outpatient costs may be offset by decreases in costlier downstream care or by decreases in production costs due to economies of scale, 150,156 but additional evidence from large scale rigorous studies is needed. Despite a vast telehealth MHS literature, there are virtually no studies describing the monetary costs of the technology and infrastructure needed and no studies considering the impact of reduced input or labor costs if telehealth providers are regionalized and located in low cost-of-living areas, provided those areas are still attractive enough for providers to reside and settle in. It is also possible that adoption of telehealth can improve efficiency of care delivery by reducing no-shows and related costs, by increasing provider productivity, or by reducing overhead or administrative costs, but evidence on these topics is limited. Studies examining production costs of telehealth care are a fruitful area for formal economic modeling and for empirical investigation.
Next, it is possible that care delivered through outpatient telehealth improves access in important ways or is effective enough to reduce severity of outcomes such that there is reduced need for downstream care at ED or inpatient settings, which are also costlier settings of care. 169 We found that studies with strong methods that examined impact on ED or inpatient care were sparsely distributed across outpatient care types, modalities and pre- and post-pandemic periods, and offered mixed insights. As reduction in downstream ED and inpatient care is considered a key cost-saving mechanism and can also signal improved health for patients, rigorous studies examining telehealth’s potential to reduce ED and inpatient care are critically needed.
Importantly, we also noted a lack of comparative effectiveness studies showing that telehealth is just as effective as in-person care across different care types. 73 Even for mental health care, where practitioners consider telehealth to be just as effective as in-person care, our own review and other recent evidence syntheses point to weak study methods. 157,158 There is an even greater lack of high-quality studies comparing the effectiveness of video-based care to phone-based care, and virtually no studies isolating the effect on phone-only care on total care and costs despite recent policy discussions focusing on coverage of phone-only care. The results of video versus phone comparisons are also likely to have important health equity implications, as people from historically disadvantaged groups and those who reside in underserved areas may have lower access to video-based care.
While ED and inpatient care are useful and pragmatic indirect measures of patient health benefits, these benefits can also be captured using quality-adjusted life years, healthy-years-equivalent or other patient utility outcomes. 170 Payers must take these benefits into account when deciding on pay structures and coverage for telehealth. Further, greater clarity on the effectiveness of different telehealth modalities and models across a range of health care needs may reduce the need for medical expertise in choice of care modality. As the need for medical expertise for treatment choice creates problematic information asymmetries between providers and patients that lead to concerns of provider-induced demand for health care, stronger and actionable research evidence on the effectiveness of telehealth may reduce such problematic information asymmetries.
As the literature currently stands, we believe that the expectation of monetary cost-savings alone may not justify the adoption of telehealth, consistent with other scholars’ views on this topic. 7 Instead, costs should be considered alongside long-term health benefits enabled by potentially improved health care access. Nonmonetary considerations like patients’ and providers’ convenience, savings in time and travel costs, patients’ existing health care access barriers and health equity implications will likely be important factors driving the value of telehealth care. Consistent with calls by other economists evaluating health care information technology, 171 experimental studies and econometric techniques can elucidate the causal impact of telehealth. While the pandemic-era adoption of telehealth has led to the burgeoning of a MHS literature on health disparities, the current evidence is extremely mixed and can mislead policy recommendations.
Existing studies report patterns that could be misinterpreted to mean that racial and ethnic minorities or older adults are less likely to use telehealth. Randomized controlled experiments or quasi-experimental studies can be used to disentangle the effects of preferences, prices, income, ability, and barriers to adoption to inform sound policies. New advances for understanding heterogeneous treatment effects using machine learning 172 can also be leveraged to examine the impact of various telehealth modalities and models for underserved populations versus the general population to provide more specific and actionable policy insights.
Finally, it is important to acknowledge the dependency of telehealth on technology and broadband internet access, 160,173 Telehealth care will require investment from other government entities and companies, often beyond the control of the health care provider. While this may be seen as a constraint to implementing telehealth, the need to improve access to computers/smart devices and broadband internet for underserved communities is not a unique need for telehealth care. Instead, there is a clear need to bridge the digital divide in the United States for many reasons. 174 Internet access is a critical social determinant of health 173 and has been shown to have important impacts also on education 175 and economic growth. 176 Disparate technological advancement creates critical rural-urban divisions 176 with potentially significant political ramifications. 167,177,178 As urban areas rely more on smart technology for a more convenient lifestyle in the coming years, such rural–urban divisions can deepen. 179 Internet access should be seen as a public good, 180 and communities should not be left behind. With similar goals in mind, the U.S. government has implemented programs such as Lifeline and 2023 Affordable Connectivity Program in recent years to address the lack of internet access or lack of devices such as computers or tablets. 41 Thus, instead of seeing technological or broadband access as a necessary barrier to telehealth implementation, we believe telehealth should be seen as another reason that reinforces the push for policymakers to tackle the harder problem of improving technological and internet access in rural areas and for historically disadvantaged populations.
Footnotes
Authors’ Contributions
K.G. and T.H.W. conceived of the work. K.G. and S.I. contributed to the acquisition and analysis of the data. All the authors contributed to the interpretation of the data and drafted and revised the work.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the position or policy of the Department of Veterans Affairs or the United States government.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This work was funded by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research. K.G.’s time was funded by VA’s National Career Development Award (#CDA-22-197), VA’s Sierra Pacific Network Early Career Award Program, and VA's Office of Connected Care Researchers & Evaluators in Residence Program. J.C.J.’s time was funded by a VA Career Development Award (#CDA-19-120). T.H.W’s time was funded by VA’s Research Career Scientist Award (#RCS-17-154).
Supplementary Material
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.