
Abstract
Background:
The COVID-19 pandemic exposed significant frailties of the U.S. healthcare system, especially inequities facing rural areas during surges when critical access and small community hospitals could not transfer patients to referral centers that were already overcapacity. Many clinicians suffered moral injury from managing these patients beyond their scope of practice or from the need to triage care.
Methods:
The National Emergency Tele-Critical Care Network (NETCCN) sought to provide a lifeline of free, ad hoc consultation to clinicians who needed help – a critical care “911” system – by using mobile devices and easy-to-use applications designed to help clinicians rapidly communicate with experts.
Results:
NETCCN provided 1,863 days of coverage to 60 hospitals in 17 states and U.S. territories at a fraction of the cost of boots-on-the ground emergency support.
Conclusions:
We review our experience delivering this support and provide recommendations to guide future development and integration of telemedicine programs into the National Disaster Medical System.
Introduction
The COVID-19 pandemic presented immense challenges to the United States (U.S.) health care system. Half of all U.S. counties lack intensive care unit (ICU) beds and critical care (CC) trained clinicians to manage severe COVID-19 patients. 1 Health care facilities in these counties, accustomed to transferring critically ill patients to referral centers, were unable to do so when the referral centers were overwhelmed by COVID-19 surges. 2–3 Media reports reflect the burden placed on doctors and nurses who, lacking the expertise and capabilities to manage these patients, tried desperately to find the care patients needed by exhaustively calling multiple referral centers. 4–5
Many states, facing overwhelming patient volume during surges, requested help from the federal government through the Federal Emergency Management Agency (FEMA). FEMA adjudicates these requests through the Emergency Services Function Eight Committee chaired by the
Inspired by others who delivered telemedicine during disasters, 6 the NETCCN imagined that tele-critical care (TCC) could expand the capability and capacity of clinicians lacking CC training or experience. We have previously described the development and initial launch of NETCCN, as well as some of the barriers faced. 7,8 By linking remote CC expertise to frontline clinicians using secure, privacy-compliant applications on mobile devices, the system provided 24/7, “911-like” support to health care teams in need.
Experience
Table 1 shows the differences between NETCCN site activations (i.e., sites that received support) and sites that were requests only (i.e., sites that did not receive support). NETCCN received 131 support requests throughout the pandemic (Fig. 1) from state hospital associations, individual hospitals, and clinics. NETCCN was activated to provide on-demand CC expertise at 60 sites (45.8% of requests). Requests from critical access hospitals (CAHs) were more likely to activate than requests from non-CAHs (35/63 [55.6%] vs. 25/68 [36.8%], p = 0.018). NETCCN provided services in 15 states and 2 U.S. territories. Requests came from generally small population centers, and hospitals supporting smaller populations were more likely to activate than those supporting larger populations (median population 7,611 [977–253,536] vs. 10,822 [1,371–240,000], p = 0.027).
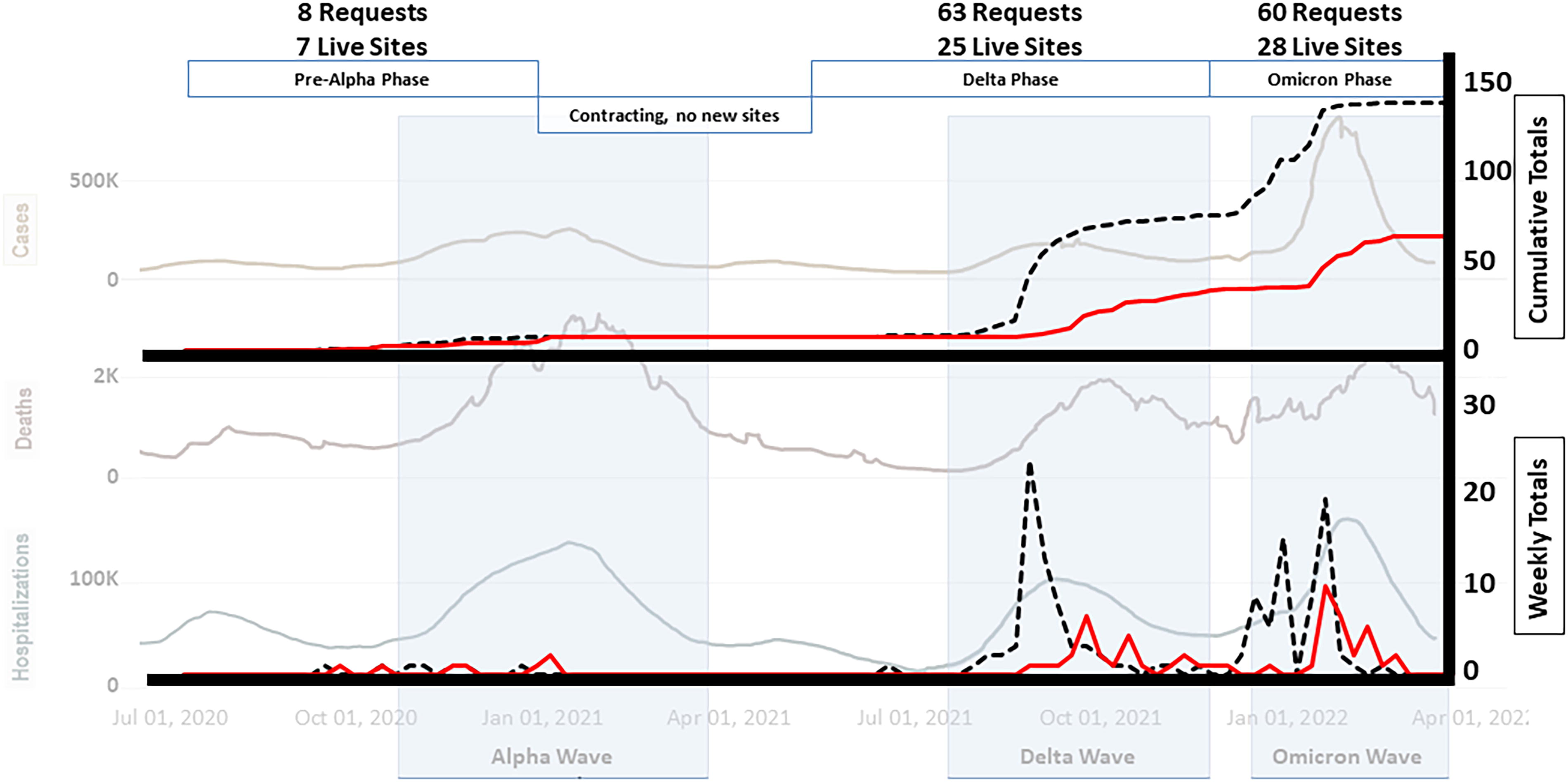
The National Emergency Tele-Critical Care Network (NETCCN) Timeline. Efforts began to establish a project in March 2020 and were approved for seed funding by the Defense Health Agency in May 2020. The project started on 15 June. Details about the early development are available in Pamplin et. al. (2021, reference # 7). Bold solid lines represent NETCCN requests (top = total, bottom = monthly). The dotted lines represent NETCCN activations (top = total, bottom = weekly). Background solid slide represents national COVID-19 cases (top), deaths (middle), and hospitalizations (bottom).
NETCCN Support Requests vs. Activations
Hospital bed capacity pertains to critical access, short-term acute care, and 1 VA hospital. ICU bed capacity, number of intensivists, and ICU nurses pertain to critical access and short-term acute care hospitals only.
Fisher’s exact test comparing CAH activation vs. all other site activations including coordinating agencies (n = 7, 0 activations), clinics and EMS services (n = 10, 2 activations).
Mann–Whitney U test of mean ranks for sites with activations vs. requests only.
t test of mean values for sites with activations vs. requests only.
Chi-square test comparing probability of activation vs. request only by high vs. low SVI.
CDC, Centers for Disease Control and Prevention; ICU, intensive care unit; NETCCN, National Emergency Tele-Critical Care Network; SVI, social vulnerability index.
There were no differences in Centers for Disease Control and Prevention (CDC) COVID-19 hospitalization rates per 100,000 population for hospitals that activated versus those that did not (mean 24.7 ± 18.5 vs. 29.6 ± 19.0, p = 0.257). Although there was also no difference in hospital activations vs. requests only according to the county social vulnerability index 9 (SVI, high or med-high or U.S. territory vs. low-medium or low, p = 0.232), nearly 55% of locations requesting help and 43.3% of activations were in counties with a medium-high or high SVI (or were U.S. territories). Most sites that requested and ultimately received help were small (median beds, activated 25 [0–40] vs. request only 40 [9–828], p = 0.19), had no ICU beds (median ICU beds, activated 0 [0–40] vs. request only 0 [0–247], p = 0.20), no CC trained physicians (median intensivists, 0 [0–3] vs. 0 [0–36], p = 0.54) and no CC trained nurses (median ICU nurses, 0 [0–25] vs. 0 [0–850], p = 0.133).
Table 2 summarizes NETCCN activations, including care models, days to start services, coverage days, and available patient demographics (not collected during pre-alpha activations). During pre-alpha and Delta wave activations, we used proactive and reactive care models; 10 in Omicron activations, we used only the reactive care model. The average days to activate service after a request was 27.3 ± 8 days (range 1–75 days). NETCCN completed its fastest activation within hours to provide expert consultation to a CAH for a patient with life-threatening renal failure who could not be transferred. The most time-consuming activity between request and activation was local credentialing, which took on average 22.9 ± 16.2 days (range 1–57 days). Delays in activation often meant that NETCCN services became available after local surges passed. The average coverage days per site were 38.9 ± 25.5 days (range 4–105 days). Total coverage days were 1863 days (259 days during pre-alpha wave, 889 days during the Delta wave, and 752 days during the Omicron wave).
Descriptive Statistics Regarding Service, Encounters and Patients for Sites That Activated NETCCN, by Cohort
Eight patients were missing information on age.
NA, not applicable; NR, not reported.
Only 55% of activated sites reported encounter-level data. Delta site activations had more patients per site (mean 10/site, range 1–204) than Omicron sites (mean 1/site, range 1–52). This difference was driven by the difference in care models: proactive vital signs monitoring during the Delta wave did not become clinical consultations in most cases and led to using only the reactive care model during the Omicron wave. The total number of unique patients with encounter data during the Delta wave was 971. There were 178 physician consultations, 431 tele-nursing encounters, 2,805 vital sign checks, and 2,078 other encounters (primarily admissions and discharges). During the Omicron wave, 90 unique patients received 103 physician consultations, 5 nursing encounters, and 53 other encounters (mainly respiratory therapy and palliative care). Patients with encounter data were considerably more ill during Omicron activations because no proactive vital signs monitoring was performed on less ill patients. Table 3 illustrates the approximate clinical costs of the NETCCN program.
Approximate Contracted Clinical Costs for NETCCN Services and FEMA Medical Assistance Team Deployments
FEMA, Federal Emergency Management Agency.
Anecdotal reports from hospital clinicians who received NETCCN support suggest that the services were highly valued and helped patients at those locations receive better care than would have been available without NETCCN, especially in cases where facilities could not transfer patients to referral centers (see video at https://www.tatrc.org/netccn/videos.html).
Discussion
NETCCN provided thousands of hours of CC coverage to hospitals that needed this expertise and could not obtain it through other means. Our case experience and anecdotal reports suggest that NETCCN helped these hospitals provide better care for patients suffering from COVID-19 than would have been provided without NETCCN and allowed local clinicians critical rest periods, potentially reducing burn-out. Although the service only supported a small number of critically ill patients, it did so for those in some of the smallest and most socially vulnerable hospitals in the United States. These hospitals needed access to expertise and NETCCN was able to offer its services at a fraction of the cost of a physical disaster medical team deployment.
Extrapolating this limited exposure, specifically for CAHs, NETCCN helped an average of nine patients per day over an average of 61 days per CAH location or 0.15 patient per day. If NETCCN were available at all CAHs in the United States, this would represent 200 patients per day across 1,353 CAHs in the United States. Every critically ill patient managed in a CAH instead of a referral center represents two beds of capacity within the system (one at the CAH and one at the referral center, unused by the CAH patient). If every CAH could manage critically ill patients, an immediate 2% increase in national ICU bed capacity could be realized for every patient managed.
Similarly, during one of the NETCCN COVID-19 activations, 30 patients received monitoring at home. Ten of these patients required oxygen therapy, which was also initiated at home. Only five of these patients (50%) ultimately required hospital admission, three of whom were discharged back to home monitoring within 48 h of admission. These admissions were directly admitted to the hospital without emergency department evaluation. At scale, this type of intervention—home monitoring during a disaster—has the potential to significantly increase hospital bed and emergency room capacity but requires significant pre-disaster planning to establish the relationships and infrastructure necessary to support patient home-care needs (like oxygen delivery) as well as consistent cellular network services at the patient location to maintain communications. While this pilot occurred with patients in their homes, a similar model where patients are co-located in a nonhospital location (e.g., a gym or hotel) could reduce the burden on home health services.
The costs of virtual CC services (monitoring and consultation) appear reasonable and scalable. Current models for the National Disaster Medical System (https://aspr.hhs.gov/NDMS/Pages/default.aspx) to support hospitals in need include sending physical teams of clinicians and support staff (ten to hundreds of individuals), such as Disaster Medical Assistance Teams (DMATs). During selected response missions (Table 3) where complete assignment data are publicly available from 2018 to 2023, estimated weekly costs of a fully supported 30–40 person DMAT were $850,000 ($280,000–$2,800,000). 11 In contrast, NETCCN weekly services to cover 100–150 patients per day cost approximately $52,000. If the NETCCN services deployed during COVID-19 covered all CAHs with at least one patient per day (1,353 patients), the weekly cost would be $470,000–$700,000 (1,353 patient/100–150 × $52,000/week). Providing telemedicine support to low-volume, socially vulnerable locations at a fraction of the cost of physical systems represents a significant improvement in equity for patients whose care at these locations is their only option.
Although no data were collected about the following, our steering committee and leadership teams often discussed observations about successful and unsuccessful activations. Successful activations were defined by effective local hospital leadership, multidisciplinary stakeholder engagement (i.e., clinical and administrative champions), and well-identified needs. Local hospitals with supportive information technology teams (IT) were also more successful than sites where local IT was skeptical or confrontational. Finally, hospitals with well-described, standardized emergency privileging processes were more likely to activate and receive consultation than locations without these processes. Locations that failed to activate were those with misaligned or unobtainable expectations (i.e., electronic health record integration within weeks, patient management by remote clinicians without local clinician partners) and those where the request for help was driven by administration without clinician buy-in.
Recommendations
The NETCCN leadership, in consultation with many experts in telemedicine and disaster response, makes the following recommendations for academic, commercial, nonprofit, and government stakeholders to consider concerning integrating telemedicine into disaster medical responses: Hospitals, especially CAHs, should explore establishing and periodically utilizing telemedical support with a percentage of in-patient bed capacity (10%) as part of local, regional, and federal disaster response systems. Teams outside of the local-regional geography should provide remote services. In-home infrastructure or emergency-established remote patient monitoring locations should be developed and exercised periodically as part of a disaster medical plan to offload in-patient and emergency room physical services. States should establish regional coordinating centers for managing in-patient beds across hospitals and hospital systems to optimize load-balancing during times of stress. The federal government should sustain an on-demand emergency telemedicine response system as a contingency for hospitals that “fall through the cracks” or fail during unexpected disaster contexts as an alternative or adjunct to physical disaster medical response teams (e.g., to provide support before, during, after or in lieu of physical team response). To provide an effective response, these telemedicine services must be made available in near real-time. The federal government should establish standardized reporting requirements for disaster telemedicine services.
Conclusions
The NETCCN project demonstrated that the government could provide access to expertise safely and within hours to locations without previously established telemedicine services. The safe and effective management of patients using telemedicine and remote monitoring in “nonstandard” locations demonstrated by NETCCN offers an under-appreciated and unexplored opportunity to increase health care system capacity during disasters. While not likely to replace physical medical disaster response teams, this telemedicine paradigm provides a cost-effective alternative to explore further.
Prior Presentations
This work has been presented at the following conferences: (1) The Healthcare Information and Management Systems Society 2021, Las Vegas, NV; 2022, Orlando, FL; 2023, Atlanta, GA. (2) The American Telemedicine Association 2022, Boston, MA. (3) The Military Health System Research Symposium 2022, Kissimmee, FL. (4) Center for Medicare and Medicaid Services Grand Rounds 2022, virtual. (5) Biodetection Technologies Summit 2021 (virtual), 2022 (virtual), 2023 (virtual). (6) AWS re:Invent 2023, Las Vega, NV. (7) Congressional Health Equity Roundtable 2023, WA, D.C. (8) The Society of Critical Care Medicine Annual Congress 2021 (Virtual) and 2023, Phoenix, AZ. (9) National Association of City and County Health Officials (NACCHO) Preparedness Summit 2023, Atlanta, GA.
Footnotes
Authors’ Contributions
J.CP.: Conceptualization, methodology, validation, formal analysis, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, project administration, and funding acquisition. M.T.Q.: Conceptualization, methodology, validation, resources, writing—review and editing, visualization, supervision, project administration, and funding acquisition. J.R.L.: Conceptualization, methodology, writing—review and editing, supervision, project administration, funding acquisition. D.P.: Writing–review and editing supervision, project administration, and funding acquisition. B.K.S.: Conceptualization, methodology, validation, formal analysis, data curation, writing—original draft, writing—review and editing, and visualization.
Contributors but not authors:
NETCCN team participants (italics indicate regular participation in delivering and coordinating NETCCN services; bold indicates significant contributions to planning, developing, and providing services; asterisks indicate team leads):
In addition, we thank Dr. Stephanie Fonda, PhD, for her help with the statistical analysis of our data.
We utilized the AI tool Grammarly© to check spelling and grammar and improve this article’s overall readability and clarity.
Disclaimer
The views, opinions, and findings contained in this research/presentation/publication are those of the author(s)/company and do not necessarily reflect the views of the Department of Defense and should not be construed as an official DoD/Army position, policy or decision unless so designated by other documentation. No official endorsement should be made.
Institutional Clearance
25 July 2024.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Administration for Strategic Preparedness and Response; U.S. Army Military Infectious Disease Research Program (MIDRP) Award Number CV20TA001.