
Abstract
Objective:
Analyze the impact of COVID-19 on outpatient mental health (OP-MH) utilization patterns, particularly telehealth, across eight different MH conditions with a 2-year follow-up.
Methods:
This population-based cohort study uses a 5% random sample of Medicare beneficiaries aged ≥18 and newly diagnosed with one of the eight MH disorders: psychotic, depressive, bipolar, anxiety, trauma-related, substance-use, other MH disorders, and two or more MH disorders. Monthly OP-MH utilization patterns were compared among patients in 2020–2021 newly diagnosed in 2019 to comparable prepandemic cohorts newly diagnosed in 2017. Multiple logistic regression models were conducted to examine differences in telehealth utilization across MH conditions.
Results:
Across groups, patients were mostly aged 65–84 (n = 39,749 [72.4%] in 2017 and n = 40,513 [75.5%] in 2019), female (n = 33,387 [60.8%] in 2017 and n = 32,193 [60.0%] in 2019), and White (n = 48,314 [88.0%] in 2017 and n = 47,282 [88.1%] in 2019). Total OP-MH utilization dropped (a 27.5% decrease at its lowest) for all MH conditions at the pandemic’s onset compared with the nonexposure group. Although utilization increased postpandemic, slight disruptions remained until the end of 2021. Telehealth visits rose from 0.5% in January 2020 to 55% in April 2020, decreasing to 18% by December 2021. Regression analysis showed that patients with psychotic, bipolar, or trauma-related, and two or more MH disorders had higher odds of telehealth usage compared with those with anxiety, while patients with substance-use disorders had lower odds. Rural residents, older adults (65+), and men had lower odds of using telehealth, with residents of the Northeast and West regions showing higher odds compared with the South. Telehealth disparity profiles were uniquely associated with different MH conditions.
Conclusion and Relevance:
Findings highlight the need for tailored telehealth strategies among Medicare beneficiaries to address specific demographic and geographical disparities across MH conditions.
Introduction
Approximately one in four Medicare beneficiaries has a mental health (MH) condition, such as depression, anxiety, schizophrenia, and bipolar disorder. 1 The COVID-19 pandemic led to an increased need for MH services while simultaneously causing large disruptions in the care provided to these patients. 2 –4 In March 2020, in response to the pandemic, the Medicare program increased telehealth coverage for the duration of the public health emergency, through the Coronavirus Aid, Relief, and Economic Security Act and other legislation. 5 –7 However, legislation authorized an extension of many of these Medicare telehealth flexibilities through December 31, 2024. 8 Following these changes, telehealth has continued to evolve and integrate into mainstream health care and become a critical component of MH care delivery. 9
As telehealth utilization is now a health care mainstay, it is crucial to understand its impact on MH care. In particular, understanding how telehealth utilization for MH treatment may have changed in the wake of the COVID-19 pandemic is necessary to determine if patients across demographic characteristics and MH conditions were equally responsive to this change in health care delivery. Whereas past research has demonstrated that telehealth usage post pandemic has differed by both demographic and MH conditions, 10 these studies have been limited in that they have assessed telehealth usage patterns for only patients with severe MH illnesses (i.e., schizophrenia and bipolar disorder), 11 –14 for just a single year follow-up period, 15 –17 or across only specific locations within the United States. 18 –21
This study extends this literature by providing a comprehensive analysis of telehealth utilization patterns across eight MH categories including psychotic, depressive, bipolar, anxiety, trauma-related, substance-use, other MH disorders, and two or more MH disorders diagnosed prepandemic. We used a cohort study design of a national sample of adult Medicare beneficiaries with a 2-year washout period and 2-year follow-up period. We investigated outpatient MH (OP-MH) utilization patterns, with a focus on those conducted via telehealth, following the onset of the COVID-19 pandemic, until the end of 2021, among the eight mutually exclusive MH conditions. Additionally, we focused on potential disparities across telehealth use, with a focus on demographic, geographical, and clinical differences in OP-MH utilization.
Methods
The Texas A&M University institutional review board (IRB) determined this study as nonhuman subjects research according to the Common Rule definition (IRB2022-0569). The study followed the Strengthening the Reporting of Observational Studies in Epidemiology guideline for cohort studies. 22
STUDY COHORTS
This study uses a 5% random sample of Medicare beneficiaries in the Centers for Medicare & Medicaid Services (CMS) Limited Data Set covering the years 2015–2021. We compared utilization for the 2 years following the onset of COVID-19 (2020 and 2021) among a cohort newly diagnosed with a MH condition in 2019 (exposure group) and a 2-year washout period (no prior MH diagnosis in 2017 and 2018), with a similar cohort diagnosed with a MH condition in 2017 (nonexposure group: study period 2018–2019; washout period 2015–2016). Patients were defined as newly diagnosed if they had either a single MH-related hospitalization or two MH-related outpatient visits on different dates during the 1-year diagnosis period 12 with no recorded MH diagnosis 2 years prior to their diagnosis period (2-year washout period). This also ensured no overlap of patients between the exposure and nonexposure group.
To increase generalizability, eligibility for this study was limited to being age ≥18 years and being continuously enrolled in the Medicare fee-for-service program for 5 consecutive years (2015–2019 for the nonexposure group and 2017–2021 for the exposure group) to ensure comparability between both groups. Patients were classified into eight mutually exclusive groups: psychotic, depressive, bipolar, anxiety, trauma-related, substance-use, other (any MH condition not previously specified), and two or more MH disorders using a modified Clinical Classifications Software (CCS) and the CCS Refined (CCSR) (Supplementary Tables S1 and S2 and Figure S1 in Supplementary Data). 23,24
OUTCOMES
We examined OP-MH utilization patterns for the 2-year study period for both the exposure and nonexposure groups. Visits were defined as OP-MH if they had a primary or secondary MH diagnosis and procedure codes indicative of an OP visit as defined in Busch et al. 12 Consistent with similar analysis, we only counted one OP-MH visit per day. 12 We also examined the utilization patterns and proportion of OP-MH visits conducted via telehealth for the exposure group for the years 2020 and 2021 as the use of telehealth for the previous years was negligible.
DEMOGRAPHICS AND CHARACTERISTICS
All demographic, geographical, and clinical characteristics were recorded at the time of each patient’s first MH visit during the diagnosis year (2019 or 2017). Demographic characteristics included documented sex, age group (<65, 65–74, 75–84, 85+), race and ethnicity, census region, Medicaid dual eligibility (indicating lower-income patients), and geographical location (rural versus urban) as recorded in the Medicare enrollment file. Beneficiaries were classified as urban if they resided in a metropolitan statistical area (population ≥50,000) and as rural if in a micropolitan area (population 10,000–49,999) or outside a Census Bureau core-based Statistical Area. 25 Clinical characteristics included MH disorders and all medical comorbidities recorded throughout the 12 months preceding a patient’s first MH visit, defined using an adjusted Elixhauser Comorbidity Index 26 excluding any MH conditions due to multicollinearity (i.e., alcohol abuse, drug abuse, psychoses, and depression).
STATISTICAL ANALYSIS
We began by comparing the monthly percentages of patients with at least one OP-MH visit in each group. We examined 95% confidence intervals (CIs) of the percentage point difference between both groups. We then described these trends for each MH condition separately. We also described the OP-MH telehealth utilization trends for the exposure group for all MH conditions as well as for each MH condition separately. Then we depicted the proportion of OP-MH visits conducted via telehealth and compared the trends across each of the eight MH categories.
We fit eight multivariable logistic regression models, one for each quarter (Q1–Q8) in 2020 and 2021, for the exposure group to examine the likelihood of having an OP-MH visit conducted via telehealth during the respective quarter. Patients included in each model were those who had at least one OP-MH visit (in-person or telehealth) within the respective quarter. For example, a patient with an OP-MH visit in Q1 but no visit in Q2 would be included only in the Q1 model. The primary outcome studied was the likelihood of telehealth utilization across different MH condition categories, with MH condition category being the primary independent variable. Demographic and clinical characteristics were incorporated as covariates to examine disparities across these groups. To account for any differences in the frequency of visits within each quarter, a categorical variable representing the frequency of OP-MH visits was included as a covariate. Visits were categorized into 0–3, 4–9, 10–16, and 16+ visits based on clinical recommendations (M.J.B.). Additionally, we conducted separate models for each MH condition across the eight quarters to examine disparities specific to each MH condition. Inferences of statistical significance were adjusted for multiple comparisons using the false discovery rate method. 27,28
Analyses were conducted in SAS version 9.4 (SAS Institute) and R version 4.4.0. Statistical significance was set at p < 0.05.
Results
SAMPLE CHARACTERISTICS
The exposure group, diagnosed in 2019, included 53,655 beneficiaries while the nonexposure group, diagnosed in 2017, included 54,917 beneficiaries. The demographic and clinical characteristics were comparable between the two groups (Table 1). Most beneficiaries were aged 65–74 (43.2% in 2017 and 44.1% in 2019), with the smallest proportion being those aged 85+ (10.5% in 2017 and 10.3% in 2019). Females made up about 60% of both cohorts. The majority identified as White (88.0% in 2017 and 88.1% in 2019) or Black (7.6% in 2017 and 7.1% in 2019). Most beneficiaries were not dually eligible for Medicaid (87.1% were not in 2017 and 88.2% were not in 2019). The Southern region had the highest representation (41.9% in 2017 and 40.6% in 2019), and around 20% of beneficiaries lived in rural areas (23.8% in 2017 and 22.5% in 2019). Regarding clinical characteristics, anxiety was the most common category of MH diagnoses (26.8% in 2017 and 26.5% in 2019), followed by depressive disorders (22.0% in 2017 and 21.5% in 2019). The least common categories were psychotic (0.8% in 2017 and 0.7% in 2019) and bipolar (0.6% in 2017 and 0.5% in 2019) disorders. The adjusted Elixhauser Comorbidity Index indicated that nearly half of the beneficiaries had four or more non-MH comorbidities (48.4% in 2017 and 49.3% in 2019).
Sample Demographics and Characteristics
aRace and ethnicity as documented in the Medicare enrollment file.
bGuam, Puerto Rico, and the Virgin Islands.
cExcluding alcohol abuse, drug abuse, psychoses, and depression.
OUTPATIENT MENTAL HEALTH UTILIZATION PATTERNS
Total mental health service utilization
Figure 1 and Supplementary Table S3 present the OP-MH utilization patterns for all patients in the exposure and nonexposure groups. In general, total utilization patterns (in-person or telehealth) were similar between both groups in the first 2 months. In March, utilization dropped by 16.3% in 2020 relative to 2018 with a 2.0 (95% CI: [−2.4 to −1.6]) percentage point decrease. The largest drop occurred in April, reaching 27.5%, followed by 20.1% in May, with a percentage point decrease of 3.4 (95% CI: [−3.7 to −3.0]) and 2.4 (95% CI: [−2.8 to −2.1]), respectively. After this drop, there was an increase in utilization in the exposure group; however, OP-MH remained slightly below prepandemic levels by the end of 2021 compared with 2019. These patterns were also observed for each of the eight MH categories separately. Although more variations were observed for patients with psychotic and bipolar disorders, this was likely attributable to their small sample sizes (Supplementary Fig. S2).
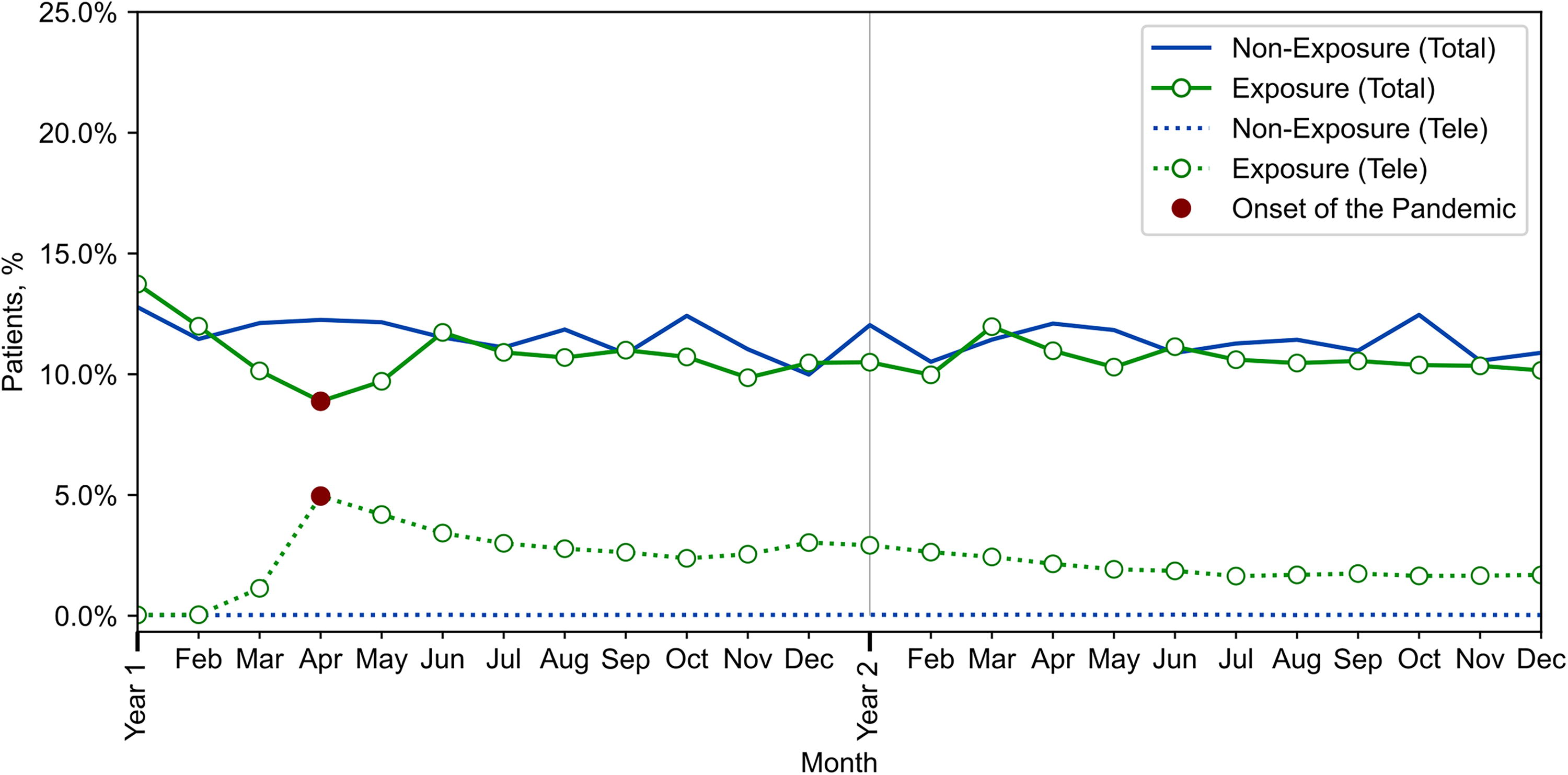
Percentage of patients with at least one outpatient mental health (total and telehealth) in the exposure and nonexposure groups for all mental health patients. Year 1: First year of the study period (2018 for the nonexposure group and 2020 for the exposure group). Year 2: Second year of the study period (2019 for the nonexposure group and 2021 for the exposure group). Total: Mental health utilization patterns for in-person and/or telehealth. Tele: Mental health utilization patterns for telehealth only.
Telehealth utilization
The substantial rise in telehealth utilization during the pandemic was evident when examining the proportion of total OP-MH visits conducted via telehealth (Fig. 2). Given that most telehealth usage was conducted via video (i.e., only 4% were audio-only services), we could not separate them. The percentage of visits conducted via telehealth in the years preceding the pandemic (nonexposure group: 2018–2019) was negligible, around 0.3%. In the exposure group (2020–2021), the percentage of visits conducted via telehealth increased from approximately 0.5% in January–February 2020 to 55% in April 2020, then gradually decreased, reaching 18% by the end of 2021. Telehealth utilization rates differed across each MH condition, with the highest percentages observed for patients with trauma-related, bipolar, and psychotic disorders and those with two or more MH conditions, while the lowest percentages were observed for patients with substance-use disorders (Supplementary Fig. S3).
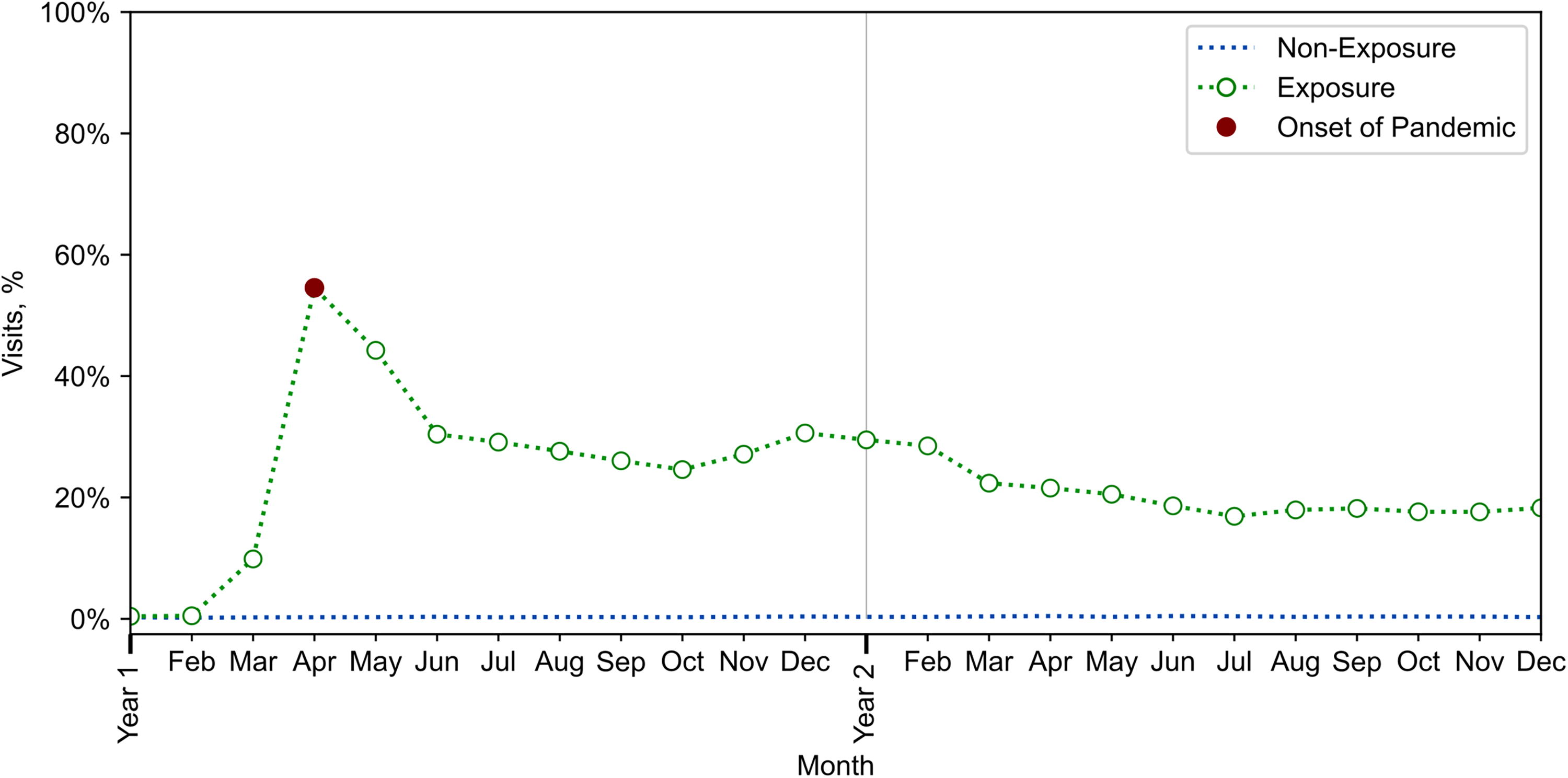
Percentage of outpatient mental health visits conducted via telehealth for all mental health patients. Year 1: First year of the study period (2018 for the nonexposure group and 2020 for the exposure group). Year 2: Second year of the study period (2019 for the nonexposure group and 2021 for the exposure group).
Multivariable logistic regression models
The first multivariable logistic regression analysis including all MH patients (Table 2) revealed distinct patterns in OP-MH telehealth utilization across various demographics and clinical characteristics throughout the different quarters. Patients with psychotic, bipolar, and trauma-related, and two or more MH disorders consistently exhibited higher odds of receiving telehealth visits compared with those with anxiety disorders. For example, patients with trauma-related disorders had higher odds of receiving a telehealth visit in Q3 than those with anxiety, with an odds ratio (OR) of 1.55 (95% CI: [1.27–1.88]); these odds increased to 1.67 (95% CI: [1.31–2.11]) by the end of 2021 (Q8). Conversely, individuals with substance-use disorders demonstrated significantly lower telehealth utilization during Q2 with an OR of 0.82 (95% CI: [0.72–0.93]), and this trend remained stable through Q8. Age disparities were evident, as patients aged 65 and older generally had reduced odds of telehealth use compared with those under age 65 and disabled. Rural residents had lower telehealth usage compared with urban residents with an OR of 0.75 (95% CI: [0.68–0.82]) in Q2; this trend remained similar throughout the remaining quarters. Patients residing in the Northeast and West regions had significantly higher odds of receiving a telehealth visit compared with those residing in the South across all quarters with an OR of 2.02 (95% CI: [1.97–2.45]) in Q2 and 1.75 (95% CI: [1.52-2.02]) in Q8 for patients in the Northeast, and an OR of 1.36 (95% CI: [1.23–1.51]) in Q2 and 2.09 (95% CI: [1.82–2.41]) in Q8 for patients in the West.
Multivariable Logistic Regression Model Results
CI, confidence interval; OR, odds ratio; Q2–Q8, Quarter 2–Quarter 8.
Furthermore, patients with higher comorbidity scores, as measured by the adjusted Elixhauser Comorbidity Index, exhibited lower odds of having telehealth visits compared with those with no comorbidities. For example, the odds of receiving a telehealth visit for a patient with an adjusted Elixhauser Comorbidity Index of 4 or higher compared with a patient with an index of 0 (no comorbidities) was 0.83 (95% CI: [0.71–0.98]) in Q2 and dropped to 0.75 (95% CI: [0.61–0.91]) in Q8. In general, no significant racial differences were observed.
The multivariable logistic regression models subsampled by each MH condition (Table 3 and Supplementary Table S4) revealed generally increased odds of OP-MH telehealth utilization for beneficiaries residing in the Northeast and West compared with the South for most MH conditions. However, significant variations in other disparities were noted across different MH conditions, particularly those with variables consistently observed across the eight quarters. Patients with psychotic and bipolar disorders were excluded from the subsampled models due to their small sample sizes (Supplementary Table S4).
Representation of Significant Variables After FDR Adjustment for Each Mental Health Condition Model (35 Model Results; Statistical Significance Set at p < 0.05)
Variables with odds ratios <1 indicated within parentheses ().
Sample sizes for each mental health condition model from Q2 to Q8 are indicated in Supplementary Table S4.
FDR, false discovery rate; MH, mental health; MW, Midwest; NA, North American Native; NE, Northeast; Q2–Q8, Quarter 2–Quarter 8; W, West.
In general, among patients with trauma-related and substance-use disorders, men were significantly less likely to use telehealth compared with women, whereas the effect of patient sex was not significantly associated with telehealth use for other MH conditions. For patients with depressive, anxiety, and two or more MH disorders, we observed significantly decreased odds of OP-MH telehealth utilization for those in rural areas compared with urban areas. For patients with depressive, anxiety, substance-use, and two or more MH disorders, older adults had significantly decreased odds of OP-MH telehealth utilization. Moreover, lower odds of utilizing telehealth for patients with high comorbidities (four or more) were only observed among patients with two or more MH conditions. Notably, no statistically significant differences were consistently observed for different races within each MH subsample across the quarters.
Discussion
This cohort study examined OP-MH utilization patterns, with a focus on those conducted via telehealth, among eight mutually exclusive categories of MH disorders: psychotic, depressive, bipolar, anxiety, trauma-related, substance-use, other MH conditions, and two or more MH conditions. Consistent with past work, the results revealed a sudden decrease in total OP-MH utilization (in-person or telehealth) at the immediate onset of the pandemic, accompanied by a surge in the proportion of visits conducted via telehealth, peaking at 55% in April 2020 and decreasing to 18% by the end of 2021. These findings align with the CMS report, which indicated that general telehealth use peaked at 47% of Medicare users in the second quarter of 2020 and leveled off to 16% by the end of 2021. 29
In addition, our findings highlight that certain groups of beneficiaries may be less likely to use telehealth. Consistent with past work, 10,29,30 older populations and rural residents demonstrate lower utilization of telehealth services, reinforcing the need for targeted interventions to address these disparities. Prior work has shown that older adults tend to prefer lower-tech treatment options, 30 which may contribute to older adults being less likely to be offered and/or to accept telehealth utilization opportunities. As older adults may be at higher risk for barriers to access, interventions designed to increase older adults’ comfort with telehealth utilization may be beneficial.
Our findings of increased telehealth usage in the Northeast and West regions compared with those residing in the South is consistent with other work, and is potentially attributable to the higher availability as well as the higher acceptance of telehealth offerings in these regions. 29,31 –33 Area of the country may also intersect with rurality, which was also associated with lower rates of telehealth utilization. Finally, the observed disparities in telehealth usage between men and women have been widely documented, 10,32,34,35 with men showing significantly lower odds of utilizing telehealth services compared with women. Future work aimed at understanding barriers to telehealth usage among male beneficiaries, particularly those located in geographic locations associated with lower rates of utilization, is needed to increase access.
Importantly, this study also revealed disparities in OP-MH telehealth utilization across different MH conditions. Our analysis shows that after the onset of COVID-19, patients with psychotic, bipolar, and trauma-related disorders had consistently higher odds of receiving a telehealth visit compared with those with anxiety disorders. Our work extends these findings by demonstrating that telehealth utilization does not just differ by demographic characteristics or MH conditions independently, but rather by subgroups within each condition. For example, although men were less likely to use telehealth than women for trauma-related disorders, there was no effect of rurality for beneficiaries with this condition. Our findings, therefore, highlight that tailored interventions across both demographic and clinical characteristics are needed to address access concerns for all beneficiaries.
Limitations
This study is not without limitations. First, the findings may not be generalizable to all populations, as the sample was limited to Medicare beneficiaries. Second, we excluded those who died or those who were not continuously enrolled in Medicare fee-for-service, which may have led to selection bias due to loss to follow-up. Third, the sample size for individuals with psychotic and bipolar disorders was relatively low compared with other studies, 11 –14 precluding examination of differences in telehealth use within these disorders. The small sample size may be attributed to the fact that beneficiaries with psychotic and bipolar disorder in our sample had the highest percentages of comorbidity with the other MH categories included (62.6% and 60.4%, respectively), which meant they were considered in the two or more MH group. Finally, we also note that disparities in telehealth utilization may also be influenced by factors such as internet bandwidth limitations, patient and provider acceptance, and digital literacy, which are not captured in the Medicare dataset used for this analysis. 36
Conclusions
This cohort study highlights the OP-MH disruptions caused by the COVID-19 pandemic and how telehealth was used to address it. It depicts the new service-use patterns after the pandemic among Medicare beneficiaries with eight mutually exclusive MH disorders, emphasizing the increased usage of telehealth. While telehealth adoption increased after the pandemic, significant differences in usage were observed across different MH conditions, demographics, and geographic locations. More importantly, telehealth disparity profiles were uniquely associated with different MH conditions, suggesting the need for targeted interventions tailored to each MH condition. Future research should focus on the long-term effects of these disruptions and develop targeted strategies to bridge the gaps in telehealth access and MH utilization, ensuring that all patients with MH conditions receive the care they need.
Footnotes
Acknowledgment
The authors gratefully acknowledge the contributions of Sachin Iyer, a student at the Indian Institute of Science Education and Research, for his assistance in refining visual representations and final results.
Authors’ Contributions
M.A.H., H.-C.K., S.P., and R.O. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. M.A.H., H.-C.K., S.P., and M.J.B.—Concept and design. M.A.H., H.-C.K., S.P., R.O., M.A.L., and M.J.B.—Acquisition, analysis, or interpretation of data. M.A.H., H.-C.K., and M.J.B.—Drafting of the article. M.A.H., H.-C.K., S.P., R.O., M.A.L., and M.J.B.—Critical revision of the article for important intellectual content. M.A.H., H.-C.K., and S.P.—Statistical analysis. M.A.H., H.-C.K., and M.A.L.—Obtained funding. H.-C.K.—Administrative, technical, or material support. M.J.B. and H.-C.K.—Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors gratefully acknowledge financial support from the Texas A&M President’s Office X-grant initiative, National Science Foundation Engineering Research Center for Precise Advanced Technologies and Health Systems for Underserved Populations (PATHS-UP) and Industrial Student Seed Fund project from the Industry Board Fees of the NSF PATHS-UP ERC [Grant Number 1648451], and Population Informatics Lab at Texas A&M University. The authors would also like to acknowledge the Texas A&M University Research Development Fund for supporting the project through the Texas Virtual Data Library (ViDaL) infrastructure. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.