
Abstract
Background:
The impact of telemedicine on health care costs and utilization has not been comprehensively assessed across diverse health care settings. This scoping review aimed to explore these impacts, focusing on the variations in intervention types.
Methods:
A literature search followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews guidelines, covering the last 10 years in PubMed/Medline, Web of Science, and Scopus. The Population, Intervention, Comparison, Outcome framework was employed to define the population (patients), intervention (telemedicine/telehealth), comparator (standard care or pre-telemedicine), and outcomes (health care costs and utilization). Both randomized controlled trials and observational studies were included in the search. The search focused specifically on health care institutions or hospitals as the level of inquiry. Telemedicine interventions were characterized using the TOAST framework’s six layers, while the four phases of the health care process (prevention, diagnosis, treatment, and recovery) were incorporated to further contextualize the interventions. Studies were synthesized and presented in tables and figures to provide an organized summary of the findings.
Results:
From 4,454 articles, 14 met inclusion criteria, with 12 examining costs and seven utilization. Six studies reported significant cost reductions with telemedicine compared with standard care. In utilization, four out of seven studies showed significant improvements.
Conclusion:
This review indicates that telemedicine may reduce health care costs and enhance resource utilization during the treatment phase compared to traditional in-person visits.
Introduction
Digitalization plays a pivotal role in advancing health systems and achieving sustainable development goal (SDG)-3, which focuses on promoting good health and well-being. 1 This is particularly evident in the aftermath of the COVID-19 pandemic, where digital health solutions have gained increasing importance in health care delivery. Telemedicine, a key component of digital health, includes various technologies aimed at delivering health care services at a distance. According to the World Health Organization (WHO), telemedicine can be defined as the delivery of health care services using information and communication technologies for diagnosing, treating, preventing disease, conducting research, and educating health care professionals. 2
Telemedicine has the potential to enhance access to health care services across all stages of the health care process, including prevention, 3 diagnosis, 4 treatment, 5 and recovery. 6 It helps address barriers such as extended wait times, geographical distance, and health care personnel shortages, especially in remote areas, including low- and middle-income countries (LMICs). The wide adoption of telemedicine is seen as beneficial for all stakeholders, including patients, health care providers, institutions, and governments, with significant momentum in its adoption following the COVID-19 pandemic. 7 –9
While many studies have documented the benefits of telemedicine from various perspectives—patients, 10 physicians, 11 and policy-makers 12 —the scope of these studies has often been limited to specific disease categories (e.g., chronic disease 13 and cancer 14 ) or hospital departments (intensive care units 15 and emergency prehospital care 16 ). The diversity in telemedicine modalities and health care contexts has led to fragmented findings, limiting the ability to generalize conclusions about telemedicine’s impact.
There is a need for a broader investigation into the comprehensive impact of telemedicine on health care costs and utilization across a wider array of telemedicine modalities, disease categories, and health care settings. While previous studies have highlighted the benefits of direct-to-consumer (DTC) telemedicine, which facilitates remote consultations 17 and follow-up visits 18 —particularly for chronic diseases and mental health—there remains a gap in understanding its broader implications for health care costs and system utilization.
This scoping review aims to address this gap by examining the potential impact of telemedicine on health care costs and utilization across different contexts based on the DTC.
Methods
STUDY DESIGN
This scoping review is part of the work under the WHO–Royal Thai Government Country Cooperation Strategy on Converge Digital Health, 2022–2026. 19 The present scoping review followed the 5-stage method outlined by Arksey and O’Malley 20 and was consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews checklist. 21
ELIGIBILITY CRITERIA
The Population, Intervention, Comparison, Outcome (PICO) framework was applied to guide the inclusion criteria for studies in this review. The population under consideration consisted of patients with any type of health condition.
For the intervention, we focus on DTC telemedicine, which involves interactions between telemedicine providers and patients within the same health care institution or practice. These interactions could occur through a variety of modalities, such as telephone calls, videoconferences, web portals, smartphone applications, or mixed modalities. If multiple modalities were employed in a study, the outcomes derived from each modality had to be reported separately and could not be aggregated into a single outcome. Additionally, studies in which interactions occurred solely between the telemedicine platform and patients (i.e., without the involvement of a human intermediary) were excluded. Furthermore, any use of telemedicine not directly related to patient treatment (e.g., for administrative purposes) was excluded. The comparator was defined as either a standard face-to-face clinical visit or a before-and-after self-comparison. The key outcomes of interest were (1) health service utilization was identified by parameters (readmission, hospitalization, primary care visits, emergency room visits, outpatient clinic visits, specialist visits, and consultation time) and (2) health care cost was identified by parameters (total cost reduction and direct and indirect costs). The level of search was focused on health care institutions or hospitals. Further details, such as the specific types of studies included, are provided in Table 1.
The Inclusion and Exclusion Criteria
INFORMATION SOURCES AND SEARCH
Searches were performed in the PubMed/Medline, Scopus, and Web of Science databases for the past 10 years (2013–2023) using MeSH terms and broad search terms. Given that the purpose of this review was to provide an overview of the large and disparate body of evidence about telemedicine for use by decision-makers and/or stakeholders, both telemedicine and telehealth were used as keywords for identifying relevant studies. The search terms used and the number of results for each database are listed in Supplementary Appendix A1.
SELECTION OF SOURCES OF EVIDENCE
The literature search results were exported into Endnote (Clarivate Analytics, Philadelphia, USA) to find and remove most duplicates. Covidence systematic review software (Veritas Health Innovation, Melbourne, Victoria, Australia) was subsequently used to review the titles, abstracts (round 1), and full texts (round 2).
The round 1 and round 2 study reviews were conducted by a six-person team with a multidisciplinary health education background (S.K., P.G., T.S., C.S., T.A., and S.L.), and the inter-reviewer Cronbach’s alpha values were 0.85 and 0.90 for rounds 1 and 2, respectively. 22 We employed a single-blind approach by giving a code to each team member to reduce bias throughout this scoping review. All studies were screened for eligibility by two researchers independently. Two senior researchers (W.I., N.K.) resolved any conflicts. Any conflicts regarding studies or contradictions were discussed further among the team until a consensus was reached. Exclusion criteria were based on the PICO sequence, along with study design, language, publication type, and date.
DATA CHARTING PROCESS AND DATA ITEMS
The data were extracted using a predefined data extraction table in Microsoft Excel following comprehensive explanations and discussions among team members. The data were collected by five team members (S.K., P.G., T.S., C.S., and T.A.), and the same reviewer (L.S.) validated the data.
In addition to extracting study characteristics such as the title, publication year, country, income level (upper middle income and high income), data sources (national level, state level, and hospital level), study design (cohort study and randomized controlled trial [RCT]), and study duration (months), this review followed a framework for telehealth services based on our prior work. 23 The TOAST framework comprises six distinct structural layers: (1) the technology employed (tool), (2) health-related outcomes (what), (3) application (for what), (4) service provider (who), (5) time (when), and (6) setting (where), as depicted in Supplementary Appendix A2. To align with the framework of telehealth services and contextual levels used in previous studies, 24 we examined the characteristics of telemedicine interventions across three levels: care setting (urban and not available/applicable), patient population (clinical focus, patient type), and telehealth (service provider, technology employed, and application). Additionally, the four phases of the health care process were also included in this study.
SYNTHESIS OF THE RESULTS
The data from the included studies were tabulated, and a narrative synthesis was conducted. The data were visualized by grouped and stacked bar plots.
Results
SEARCH RESULTS
Fig.1 illustrates the study selection process using the PRISMA flow diagram. The initial search identified 4,454 studies published between 2013 and June 2023 from the three databases, of which 970 were duplicates. After reviewing the titles, 3,484 studies were excluded, and after reviewing the abstracts, 822 additional studies were excluded. The top three reasons for excluding studies were an out-of-context outcome, an out-of-context intervention, and an out-of-context comparator. After screening, 14 studies were included in the analysis.
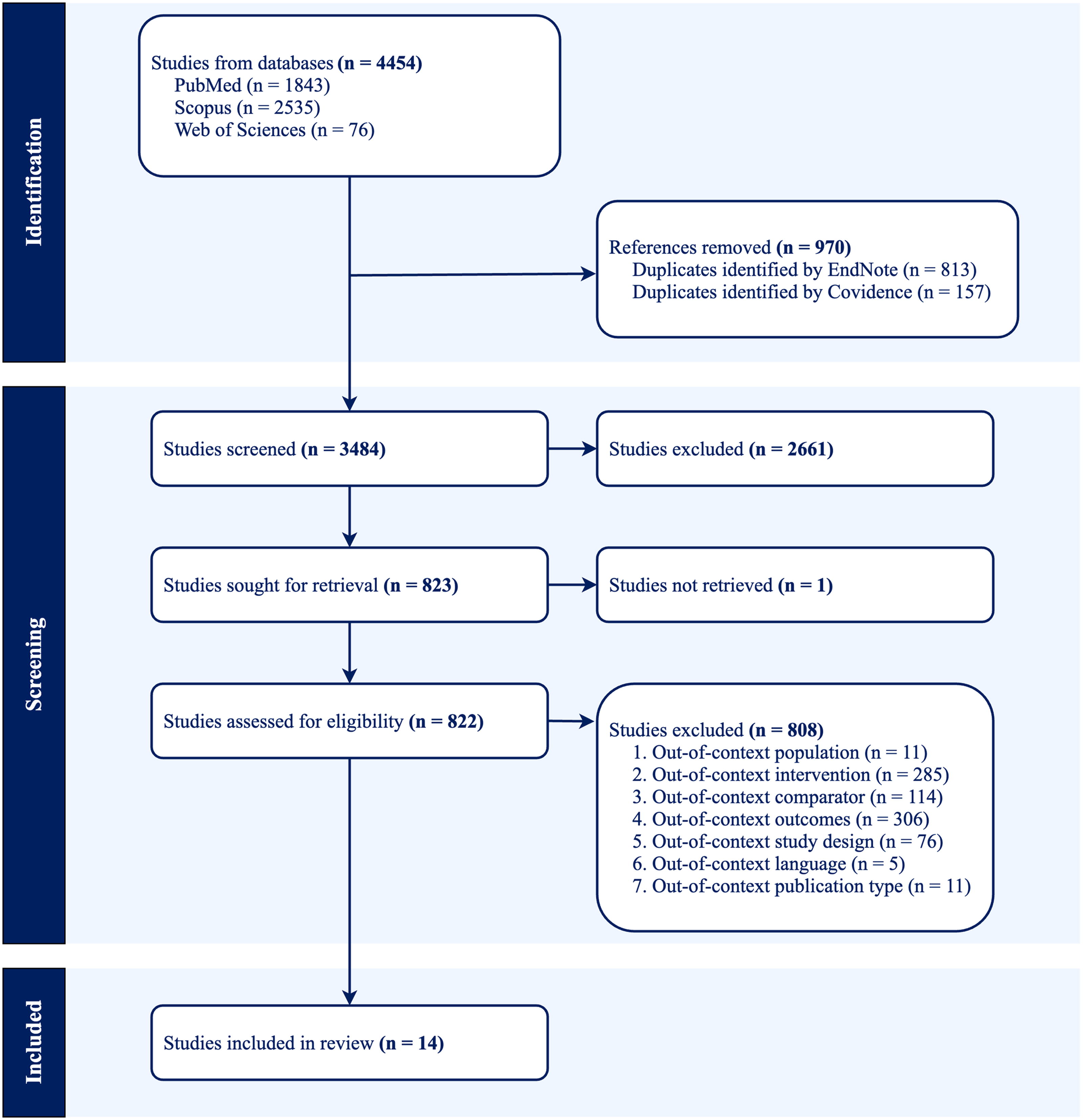
The PRISMA flow diagram.
STUDY CHARACTERISTICS
A substantial portion of the studies were published in 2018 (29%) and 2020 (22%). According to the World Bank’s 2022 classification 25 for a country’s income level, all except one study (93%) was conducted in high-income countries, with the United States being the dominant contributor (36%). One study (7%) was conducted in China, which was classified as an upper-middle-income country. Most of the studies (72%) collected data at the hospital level. Five studies used electronic health records data at the hospital level (7%), state level (21%), and national level (7%). Regarding study design, almost half of the studies (50%) employed an RCT design. Additional details can be found in Supplementary Appendix A3.
OVERVIEW OF CHARACTERISTICS OF TELEMEDICINE INTERVENTIONS
In this review, most of the study settings were located in urban areas (64%). Almost half of the studies had durations exceeding 12 or 24 months (57%). Notably, the review predominantly involved outpatient individuals (86%) with chronic conditions (50%). The primary support team comprised clinicians (50%) and nurses (21%), predominantly utilizing telephone-based methods (43%) for delivering telemedicine services. Telemedicine functioned as an approach for teleconsultation (29%), telemonitoring (21%), and teletherapy (14%), facilitating interactions between clinicians or nurses and patients. During the four health care processes, the treatment phase (64%) dominated. Additionally, nearly 9 out of the 10 studies used standard face-to-face clinical visits as the comparator (86%). The principal outcome measure in the majority of the included studies was health care costs (57%). Furthermore, more than two of five studies employed univariate and multivariable analyses as statistical methods (43%).
Table 2 reports the characteristics of telemedicine interventions on health care costs and utilization. Diverse cohort study designs were employed, including exposed and control group designs, 26,30,34,38 before and after designs, 28,33 and mixed designs. 37 The shortest (3 months) and longest (27 months) studies involved patients who underwent subacromial decompression surgery 31 and those with cancer, 27 respectively. The chronic conditions under examination were broad and included heart failure, 26,36 hypertension, 30 and either a single 38 or multiple active chronic diseases. 28 Similarly, a wide range of sample sizes was observed, varying from 18 patients 31 to 238,943 patients. 37
Characteristics of Telemedicine Interventions for Health Care Costs and Utilization
Most of the telemedicine interventions involved prevalent patterns, including home-based telemonitoring, 26,28,30,36 clinician-led initiatives, 27,29,30,32,34,37,38 and telephone follow-up. 26,28,29,33,34,39 The health care team engaged in online interactions involving clinicians, patients, and administrative staff 26 or adopted a personalized medicine approach led by a nurse. 28 Beyond hospital-based entities, third-party involvement in telemedicine service provision was evident, represented by technology companies 35 facilitating interactions between administrators and patients. Regarding the health care process, nine interventions utilized telemedicine during the treatment phase, 26 –28,30,32,34 –37 three during combined diagnosis and treatment phases, 29,33,38 and one during the prevention 39 and recovery 31 phases.
WHAT IS THE POTENTIAL IMPACT OF TELEMEDICINE ON HEALTH CARE COSTS AND UTILIZATION?
Table 3 offers a comprehensive overview of the health care cost and utilization outcomes derived from the included studies, revealing a diverse array of results. Health care cost was identified by parameters such as total cost reduction and direct and indirect costs. Health service utilization was identified by parameters such as readmission, hospitalization, primary care visits, emergency room visits, outpatient clinic visits, specialist visits, and consultation time.
Impact of Telemedicine Interventions on Health Care Outcomes
Not available for direct or indirect costs.
 ,
,  , statistically significant increase or reduction.
, statistically significant increase or reduction.
 , no statistically significant difference.
, no statistically significant difference.
 , reduction with no available p-values.
, reduction with no available p-values.
Among the 12 studies that examined health care cost outcomes, six indicated that, compared with standard care, telemedicine substantially reduced costs. Two studies supported these findings, although the p-values were not significant. Two studies reported no statistically significant difference between the two groups. Notably, an additional two studies demonstrated a cost-saving trend in the standard care group. Specifically, Adler et al. concentrated on the initial consultation among breast cancer patients in the diagnosis and treatment phase. 33 Furthermore, four studies assessed direct costs, two evaluated indirect costs, and three considered both indices to measure cost outcomes.
In relation to utilization outcomes, four out of seven studies examining health care utilization reported a significant difference between the telemedicine group and the standard care group in terms of different indicators. Porath et al. observed a significant reduction in hospitalization days among elderly patients with complex chronic conditions compared to those in the standard care group. 28 Jones et al. reported that telemedicine significantly reduced consultation time among women with urinary incontinence. 29 Jiménez-Marrero et al. revealed a significantly lower incidence of the first occurrence of the primary endpoint among patients with chronic heart failure in the telemedicine arm than in the control arm. 36 Adler et al. observed a significant increase in outpatient visits among breast cancer patients after the initial consultation. 33
Beyond visualizing the results in Table 3, we provided a narrative in Supplementary Appendix A4. The study by Jiménez-Marrero et al. demonstrated the most significant change in health care costs, showing a difference of €3314 between telemedicine and usual care in hospitalization costs (€6064 vs. €2750, p = 0.006). 36 This study also highlighted telemedicine’s real benefits through detailed event reporting. Telemedicine significantly reduced the risks of heart failure-related (10 vs. 29 events, p = 0.011), cardiovascular-related (13 vs. 37 events, p = 0.009), and all-cause hospitalizations (21 vs. 51 events, p = 0.017) compared with usual care.
Discussion
RELEVANT FINDINGS
This scoping review synthesizes evidence from studies assessing the impact of telemedicine on health care costs and utilization across diverse settings. Overall, our review supports the growing body of evidence suggesting that telemedicine can potentially reduce health care costs, particularly in the treatment phase, and enhance health care access and utilization. While the evidence is consistent in indicating positive trends, the heterogeneity in study designs, health care settings, and disease categories means that conclusions about the overall economic impact of telemedicine remain cautious. For instance, studies like that of Jiménez-Marrero et al. 36 found significant cost savings, especially related to hospitalization, while other studies, such as those examining teleconsultations in oncology, indicated minimal cost reduction.
These findings point to the need for a more nuanced understanding of the economic impact of telemedicine. While there is some consensus on the potential for cost reductions, especially in managing chronic conditions, the evidence is fragmented when it comes to specific modalities, such as m-health versus traditional telemedicine or telemedicine in low-resource settings.
LINK WITH EXISTING LITERATURE
The findings of this review are consistent with earlier systematic reviews on the topic, which have highlighted telemedicine’s cost-effectiveness, particularly for chronic disease management. For example, systematic reviews on chronic neurological diseases have shown that telemedicine can reduce hospital admissions and improve outcomes, thus saving costs. 40,41 Similarly, our review confirms that telemedicine interventions are typically more cost-effective than in-person care, though the extent of these savings is dependent on factors such as disease category and patient demographics.
To better understand the impact of telemedicine on health care utilization, this review included four phases of the health care process: prevention, diagnosis, treatment, and recovery. The diagnosis phase, such as in the study by Adler et al., 33 showed increased costs in the telemedicine group, which was attributed to patients seeking further treatment after the initial consultation. Telemedicine consistently has overwhelmingly positive patient benefits and enhances productivity across various services. 42 Compared with the treatment and recovery phases, heightened health care utilization during the prevention and diagnosis phases not only leads to better health outcomes but is also smarter and more sustainable. Telemedicine is becoming integrated into our daily lives and is anticipated to be increasingly utilized in the future.
IMPLICATIONS FOR POLICY, RESEARCH, AND PRACTICE
The findings from this review underscore the potential of telemedicine to transform health care delivery, particularly in resource-limited settings. For policymakers, the evidence supports the growing role of telemedicine in improving access to health care, reducing costs, and optimizing resource utilization. However, while telemedicine shows promise, its broader adoption—especially in LMICs—requires careful consideration of the infrastructure and training needs.
From a research perspective, the review identifies several gaps, particularly in understanding the long-term economic impact of telemedicine and the costs associated with indirect outcomes, such as patient satisfaction and quality of life. Further research is also needed to examine the comparative effectiveness of telemedicine across different health care settings and disease categories.
For practitioners, the review highlights the need to consider telemedicine as part of an integrated health care strategy. While telemedicine shows clear advantages in reducing costs and improving health care access, it is not a one-size-fits-all solution. The integration of telemedicine into the treatment process should be tailored to specific patient needs and health care settings. As telemedicine becomes more embedded in health care systems, clinicians will need to develop the skills to optimize its use.
LIMITATIONS
This scoping review has several limitations that must be acknowledged. Firstly, due to the heterogeneous nature of the included studies, it was not possible to conduct a detailed statistical comparison of outcomes across studies. The lack of standardization in reporting “direct” and “indirect” costs also limited our ability to make concrete conclusions regarding the economic impact. Secondly, the analysis was constrained by the relatively small number of studies and the focus on only two key outcomes: health care costs and utilization. Further studies should consider additional outcomes, such as clinical outcomes and patient satisfaction. Additionally, this review focused on studies published within the last decade and did not explore gray literature, which may have provided additional insights into the impact of telemedicine. Finally, while we examined telemedicine interventions in isolation, future research could investigate the effectiveness of integrated interventions, such as combining telemedicine with in-person visits or other digital health technologies.
Conclusions
This scoping review showed that, compared with standard face-to-face clinical visits, telemedicine has the potential to decrease health care costs and optimize health service utilization in various health care settings.
Footnotes
Acknowledgments
We are thankful to our colleague Siobhan Botwright for contributing to this scoping review and article.
Authors’ Contributions
Conceptualization: W.I. Data curation: S.L., S.K., P.G., T.S., C.S., and T.A. Formal analysis and software: S.L. Funding acquisition: W.I. and N.K. Methodology: S.L. Project administration: S.L. Supervision and validation: W.I. and N.K. Writing—original draft: S.L. Writing—review and editing: All authors.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
The Health Intervention and Technology Assessment Program (HITAP) is a semiautonomous research unit in the Ministry of Public Health, Thailand, and supports evidence-informed priority-setting and decision-making for health care. HITAP is funded by national and international public funding agencies. HITAP is supported by the Health Systems Research Institute, Thailand (HSRI.66–074), among others. The funders had no role in the design of the study; in the collection, analysis, or interpretation of the data; in the writing of the article; or in the decision to publish the results.
Supplementary Material
Supplementary Appendix A1
Supplementary Appendix A2
Supplementary Appendix A3
Supplementary Appendix A4
Supplementary Appendix A5
Supplementary Appendix A6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.