
Abstract
Introduction:
Digital technologies, such as telemedicine and wearable devices, are transforming health care by enhancing cross-sectoral care and targeted health responses. Despite these advancements, challenges such as data protection, lack of interoperability, reimbursement, and financial costs hinder telemedicine’s broader implementation, especially within the German health care system. This study explores the use, acceptance, and barriers of telemedicine among cardiologists, internists, and general practitioners in Germany.
Methods:
A web-based survey was conducted from October 2023 to January 2024, targeting cardiologists, internists, and general practitioners. The survey assessed current telemedicine usage, acceptance, and barriers. Data analysis included descriptive statistics and exploratory cluster analysis.
Results:
Of the 172 physicians analyzed, 76.2% were cardiologists. Telemonitoring (45.9%) and wearable devices (26.2%) were the most used telemedicine applications, whereas video consultations (11.0%) and apps (19.2%) were less common. Despite high costs (57.7%), insufficient technical expertise (20.8%), and lack of system interoperability (45.8%), respondents rated telemedicine positively and saw several chances and potentials. Cluster analysis identified four user groups: The pioneers, the focused practitioners, the using skeptics, and the uninformed distanced, each with unique needs and challenges.
Discussion:
The acceptance of elemedicine among physicians indicates recognition of its benefits for patient care. Only half of the respondents felt reasonably well informed about telemedicine. Overall, our study shows the current use of telemedicine as well as the acceptance, barriers, and challenges perceived in the German ambulatory sector. It underlines the increasing importance of telemedicine for patient care and highlights existing barriers to enable wider implementation in the outpatient sector. The results show that telemedicine in Germany is on a promising path. The biggest obstacles still appear to be reimbursement and the technical infrastructure.
Introduction
Digital technologies, including telemedicine and wearables, have led to notable changes in health care, facilitating cross-sectoral care, and more targeted responses to health-related issues during and after COVID. 1 –7 Nevertheless, there are various challenges and barriers regarding the use of telemedicine. Challenges appear to lie primarily in the areas of data protection, the lack of interoperability, cost coverage, and the need for training. 8 –11 Overall, many telemedicine initiatives do not progress beyond the research phase or fail to become sustainable. 12 –14 The known factors which condition the successful implementation are numerous such as the technological infrastructure, financial aspects, and legislative burdens. 9,14 –17 Despite these barriers, telemedicine is established in various settings such as cardiology and shows great efficiency regarding different aspects raging from hospital readmissions, hospitality, improvement of quality of life, or resource efficiency. 8,18 –24
In Germany, the application of telemedicine in cardiology ranges from remote monitoring, to telecardiology consultations or the use of wearables. 8,25 Recent studies have shown improvements such as reduction in hospital stays, detecting arrhythmias, and enhancing patient safety in ambulant patient care due to monitoring. 21,23,26 These studies led to a resolution by the statutory health insurance funds (German abbreviation: “GBA”), which for the first time provided reimbursement for telemedical heart failure monitoring for cardiologists, internists, general practitioners, and others. 27,28
Numerous studies have explored the attitudes of health care professionals and patients, revealing heterogeneous results. 25,29 –36 Furthermore, evidence indicates that physicians in ambulatory practices exhibit greater reluctance toward telemedicine compared to their counterparts in inpatient settings. 37 Research shows high patient satisfaction with telemedicine services in Germany due to convenience and better accessibility. 38 The same does account for other European countries or the United States showing a level of acceptability and satisfaction with telemedicine—apart from that, there is a need for adequate technical infrastructure, digital and financial resources, and training and education to conduct telemedicine care. 39 –41
Regarding the acceptance of telemedicine in Germany, Mühlensiepen et al. showed varying acceptance among cardiologists, internists, and general practitioners in Berlin and Brandenburg and the different user types of telemedicine, showing a general acceptance and willingness among the responding physicians despite existing barriers, which is also shown in other studies. 25,42,43
Therefore, it is of interest to explore the use of telemedicine in Germany in the ambulatory sector. Following, we conducted a survey among cardiologists, internists, and general practitioners in Germany aiming to assess the current use, acceptance, as well as barriers.
Methods
STUDY DESIGN
A web-based survey addressing cardiologists, internists, and general practitioners investigated their needs and attitudes toward telemedicine as well as barriers and facilitating factors.
Survey development and data collection
The survey was developed by the research team. Initial items ware developed based on existing literature as well as the care experiences among the Telemedicine Center of the Technical University of Munich (TUM). The initial items were grouped into themes and areas of interest. The questionnaire covered a range of topics regarding the current usage, chances, challenges, and barriers as well as needs. The questionnaire contained 32 items (on 23 pages). Adaptive questioning was applied as certain items were only relevant for cardiologists. The survey was pretested and revised multiply within the interdisciplinary research team. A completeness check was done.
The survey was coded into SoSci (SoSci Survey GmbH), a common, well-established, and specifically designed web-based application for scientific data collection. To participate, physicians had to meet the following eligibility criteria: working in the ambulatory sector; cardiologist, internist, or general practitioner; informed consent. At the beginning of the survey, participants were asked to select their specialty (options: Cardiology, Internal Medicine, General Medicine, or None of the Above). If the option “None of the Above” was selected, the survey was immediately ended, as the data collection was intended to focus exclusively on these three fields.
The survey was distributed via professional associations (German Cardiac Society, Association of registered Cardiologist, and the German Society of General Practice and Family Medicine; see Acknowledgments) or subgroups of those and the network of the TUM Telemedicine Center via email, letter or website. Both contained a direct link (web link and QR-Code) to access the open survey and provide consent. The access to the survey was available from October 3, 2023, until January 31, 2024. All study participants consented prior to the survey. If no consent was given, there was no access to the survey. Participants received information on the purpose, duration, and handling of the data. No reward was given for participation. Participants were able to review and change their answers. The survey is included in the Supplement (see Supplementary Data S1).
This study received approval by the Ethics Committee of the Medical Faculty of the TUM (Reference number 2023-437-S-SB) on August 7, 2023.
DATA ANALYSIS
The statistical analyses were conducted in two steps: First, a descriptive analysis and second, an exploratory analysis via cluster analysis. Data analysis was primarily conducted using the IBM Statistical Package for Social Sciences (SPSS) software (Version 29.0.1.0). 44 In addition, Python was used for data preprocessing, Z-score transformations, and the creation of a scatterplot with 95% confidence ellipses as well as boxplots, employing the libraries pandas, numpy, matplotlib, and seaborn.
As reporting guideline we used the Checklist for Reporting Results of Internet E-Surveys checklist (CHERRIES), which is uploaded with the submission (see Supplementary Data S10). 45
Descriptive analysis
Descriptive analysis included quantities, percentages, median scores, and ranges for ordinal variables. Free text fields under “Other” were—if possible—added to the existing answer options (e.g., “Home monitoring ICD, CRT devices” was added to the Monitoring category).
Exploratory cluster analysis
Data preparation and Variable construction: Primary data variables were used for the analysis, representing various aspects such as acceptance, opportunities, barriers, and challenges. Sum scores were calculated for each category, summarizing the cumulative values from the individual items, resulting in the new variables Acceptance, Opportunities, Barriers, and Challenges, which were used for further analysis and cluster formation. The variables Level of Informedness and Number of Different Types of Telemedical Applications (TMA) Used (Number of TMA Types) were also considered. All variables were scaled such that higher values indicate a more positive evaluation, enabling uniform interpretation of scales across all variables. These variables were also used for cluster formation.
DATA IMPUTATION
To minimize the impact of missing data, data imputation was carried out using the Multiple Imputation function in SPSS. This method allowed the adequate replacement of missing values in the five variables mentioned above to ensure the integrity of the dataset for subsequent analyses.
PRINCIPAL COMPONENT ANALYSIS
To reduce dimensionality and extract the main variables from the scaled data, a principal component analysis (PCA) was performed. The PCA reduced the data to two main dimensions, represented as the variables PCA_Dim1 and PCA_Dim2, based on the variables Acceptance, Opportunities, Barriers, Challenges, Level of Informedness, and Number of TMA Types, enabling clearer visualization and interpretation of group separation.
CLUSTER ANALYSIS
Using k-means cluster analysis, the data were segmented into 2, 3, and 4 clusters. This method was applied to the two principal components derived from the PCA (PCA_Dim1 and PCA_Dim2) used to explore cases’ natural grouping and determine which cluster count best represented the data structure. For each cluster solution, centroids were calculated, and the homogeneity within the clusters and heterogeneity between the clusters was analyzed. As part of this process, three new variables were created to assign cases to their respective clusters for the 2-cluster, 3-cluster, and 4-cluster solutions.
Multivariate analysis of variance
To assess the differences between the groups formed by the k-means cluster analysis, a multivariate analysis of variance (MANOVA) was conducted for all cluster (2-cluster, 3-cluster, and 4-cluster) solutions. The cluster membership, represented by the three new variables indicating assignment to 2-cluster, 3-cluster, and 4-cluster solutions, served as the dependent variable. The principal components (PCA_Dim1 and PCA_Dim2) derived from the PCA were used as independent variables. This analysis aimed to verify whether the assumed clusters exhibit statistically significant differences in the independent variables.
The assumptions for the MANOVA were rigorously tested to ensure the validity of the results. The groups for these tests were defined using the 4-cluster solution, as this configuration provided the most nuanced representation of the data structure based on preliminary evaluations. Normality was assessed using the Shapiro–Wilk test. For PCA_Dim1, normality was confirmed for clusters 1, 3, and 4, whereas a deviation was observed in cluster 2 (p = 0.005). For PCA_Dim2, normality was met in clusters 1, 2, and 3 but not in cluster 4 (p < 0.001). Given sufficient sample sizes (n ≥ 20 per group), the MANOVA remains robust to these deviations. 46 The homogeneity of variance–covariance matrices was tested using Box’s M test, which was not significant (Box’s M = 2.435, p = 0.984), supporting this assumption. Levene’s test confirmed the equality of error variances across the groups (PCA_Dim1: p = 0.556; PCA_Dim2: p = 0.922). The linearity between dependent variables was validated using scatterplots, and the near-zero Pearson correlation (r = 0.000) between PCA_Dim1 and PCA_Dim2 reflects the orthogonal nature of the PCA-derived dimensions. Pillai’s Trace was selected as the primary test statistic due to its robustness against deviations from normality and its sensitivity to detecting multivariate differences.
SUPPLEMENTARY VISUALIZATIONS
To complement the MANOVA, Z-score standardized boxplots were created for the following key variables: Acceptance, Opportunities, Barriers, Challenges, Level of Informedness, and Number of TMA Types. Z-scores were calculated using Python by standardizing each variable to a mean of 0 and a standard deviation of 1, enabling direct comparisons across different measurement scales. The boxplots illustrate the median, interquartile range (IQR; 25th to 75th percentiles), and whiskers (extending to 1.5 times the IQR). The medians are indicated by a black line. Outliers were excluded from the visualization using the showfliers=False parameter, focusing the presentation on the main data distribution within each cluster. Potential outliers were retained in the data for all calculations to ensure the validity of the results. These boxplots provide additional descriptive insights into the distribution and variability of variables within the clusters, supplementing the results of the MANOVA.
To further enhance interpretability, the mean composite scores (for summated scales Acceptance, Opportunities, Barriers, Challenges) and simple means (for individual variables such as Level of Informedness and Number of TMA Types) and their 95% confidence intervals (CIs) were computed using SPSS for each variable within the clusters of the 4-cluster solution. These descriptive statistics summarized the central tendencies and variability, serving as a numerical complement to the MANOVA and boxplot analyses.
SCATTERPLOT WITH CONFIDENCE ELLIPSES
A scatterplot was created using Python to visualize the distribution of the clusters from the 4-cluster solution on the two principal components (PCA_Dim1 and PCA_Dim2). Each cluster is represented by distinct markers and colors. To emphasize variability and cluster separation, 95% confidence ellipses were calculated based on the covariance matrix of PCA dimensions for each cluster, using the matplotlib librar. These ellipses visually highlight within-cluster variability and overlap between the clusters. The scatterplot complements the MANOVA results by providing a two-dimensional visual representation of intercluster relationships.
Results
In total, 222 physicians responded to the questionnaire. Twenty-nine were excluded as they were not cardiologists, internists, or general practitioners. Twenty-one were not included in the analysis because less than half of the questions were answered. Thus, 172 were included for data analysis.
CHARACTERISTICS OF RESPONDENTS
Most participants were cardiologists (n = 131; 76.2%), followed by internists (n = 26; 15.1%) and general practitioners (n = 15; 8.7%). In total, 73.8% of the participants were male (n = 127). The great majority of participants were older than 40 years (40–49 years, 22.1%; 50–59 years, 41.9%, over 60 years, 29.1%). All demographic data and characteristics of the participants are shown in Table 1. For a graphic representation of the distribution of participants by federal states, see Fig. 1.
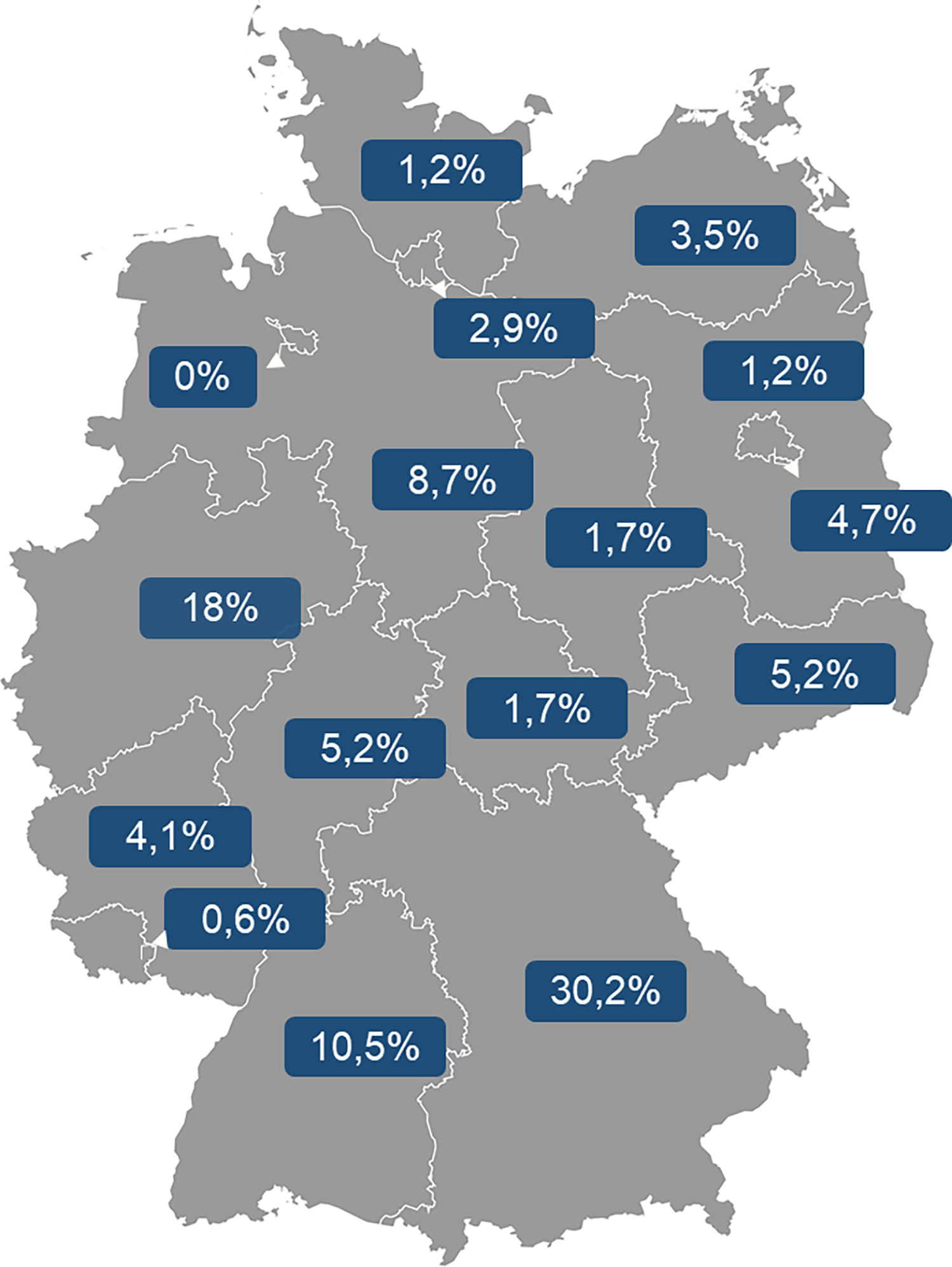
Distribution of participants by federal states.
Demographic Data and Participants’ Characteristics
CURRENT USE OF TELEMEDICINE
Monitoring (45.9%) and Wearables (26.2%) are used most often; Video Consultations (11.0%) and Apps (19.2%) are used less. Other applications were specialists’ consultation (e.g., dermatology) or communication with the patient (see Supplementary Data S2). In total, over 13 different platforms for telemedicine applications were named by the participants.
Of the responders (n = 47), 27.3% stated that they have already founded a Telemedicine Center following the resolution on the guidelines for methods of care by the statutory health insurance-accredited physician in Germany. Those respondents were, for the most part, over 50 years (50–59 years; 42.6%; over 60 years, 17.0%) and worked mostly in communal practices (74.5%) and less in single practices (19.1%) or Medical Service Centers (4.3%). They tend to be located in large cities (over 100,000 inhabitants, 46.8%; more than 500,000, 12.8%) in 13 Federal States all over Germany.
When asked whether the participants would like to learn about and use (new) telemedicine applications (e.g., in the form of research projects), 31.4% (n = 54) stated that they would be interested and 33.1% (n = 57) stated that they would be willing to do so under certain circumstances.
INFORMEDNESS AND NEED FOR INFORMATION
The self-assessed level of information is not rated as good overall. Only more than half of the respondents (61.2%) consider their level of information on telemedicine to be fairly good to good, whereas 38.6% consider it to be fairly poor to poor. The main sources of information are professional associations and medical journals. Health insurance companies, colleagues, and congresses were named as poor sources of information. The need for information in terms of the question of who respondents would like more information from shows a heterogeneous picture. For further details regarding the informedness, see Supplementary Data S3.
CHALLENGES AND BARRIERS
A majority of respondents (85.7%) are convinced of the future of telemedicine in patient care, but 14.3% are still critical of it. The technical equipment of the practices does not stand in the way of use in 79.2% of the respondents, but 20.8% still have difficulties with technical expertise.
However, 57.7% state that the acquisition and use of telemedical applications are associated with excessive costs. In total, 83.3% of respondents are able to integrate telemedicine equipment into the existing operating system. Nevertheless, 45.8% still complain about the burden of having too many different portals for use, meaning that the systems are not interoperable in almost half of the cases. In total, over 30 different practice management systems were named. For further details regarding challenges and barriers, see Supplementary Data S4.
Currently, 80.1% of colleagues experience insufficient reimbursement as the greatest barrier to the use of telemedicine in their practice (total agree: 61.6%; rather agree: 18.5%). Over half of the respondents (57.5%) generally rate the introduction of new digital applications in health care as challenging, with 59.6% citing the effort required to connect to relevant clinics and service providers and 57.5% identifying a lack of technical infrastructure as an obstacle, whereas 61.6% consider data protection to be a barrier. The lack of expertise of medical staff only deterred just under half of the respondents (45.2%). For details, see Supplementary Data S5.
ACCEPTANCE OF TELEMEDICINE
Overall, the respondents showed a great acceptance of telemedicine rating the possibilities and chances for patient care predominantly positive (see Supplementary Data S6).
In general, the respondents consider patient acceptance of the use of telemedicine to be rather indifferent (acceptance: rather disagree = 26.0%; neither = 28.0%; rather agree = 28.7%). Although the acceptance shown is perceived as mixed, the respondents tend to believe that there are subjective benefits for their patients; examples include: (a) an improvement in everyday quality of life (quality of life: totally agree =16%, rather agree = 40% vs. rather disagree = 14%, totally disagree = 7.3%), or b) a feeling of safety (telemedicine gives patients a feeling of safety: totally agree = 26.8%, rather agree 45.6%, rather disagree = 6.7%, totally disagree = 2.7%).
There is a slight positive trend in the area of the doctor-patient relationship (42.6% rather or totally agree vs. 30% rather or totally disagree, whereas 24.7% stated neither). 61.8% (42.3% + 19.5%) see increased patient compliance and adherence and 52.7% (32.7 + 20) see increased health literacy of the patients treated with the use of telemedicine. Over a third (40%) do not see telemedicine as a helpful support for patients to address critical or taboo health issues. For details, see Supplementary Data S7.
Overall, the future use of telemedicine is rated as increasing in general (see Supplementary Data S8).
CLUSTERS OF USERS OF TELEMEDICINE
Using the variables Acceptance, Opportunities, Barriers, Challenges, Level of Informedness, and Number of TMA Types and applying k-means cluster analysis and MANOVA, we identified four clusters: The pioneers, The focused practitioners, The using skeptics, and The uninformed distanced.
Results of the MANOVA
Among the clustering solutions tested, the 4-cluster solution demonstrated the most significant differences between groups (see Table 2). Pillai’s Trace and Wilks’ Lambda confirmed the strength of this solution, with Pillai’s Trace prioritized due to its robustness against assumption violations. The 4-cluster solution exhibited the clearest separation between groups, as indicated by Pillai’s Trace (p < 0.001) and Wilks’ Lambda (p < 0.001).
MANOVA Results for Different Cluster Solutions
The centroids for each cluster revealed high intracluster homogeneity and intercluster heterogeneity. Pillai’s Trace values were highest for the 4-cluster solution, indicating stronger separation and robustness. The associated F-values further supported this differentiation, with significant results for both Pillai’s Trace (F[15, 492] = 29.350, p < 0.001) and Wilks’ Lambda (F[15, 447] = 40.341, p < 0.001), testing the effect of cluster membership on the dependent variables. These results highlight the suitability of the 4-cluster solution as an optimal choice for further analysis.
Results: Descriptive Statistics and Boxplots
The mean composite scores and their 95% CIs for key variables across clusters, along with Z-score standardized boxplots, provide a comprehensive overview of the distribution and variability within and between clusters (see Table 3 and Fig. 2).
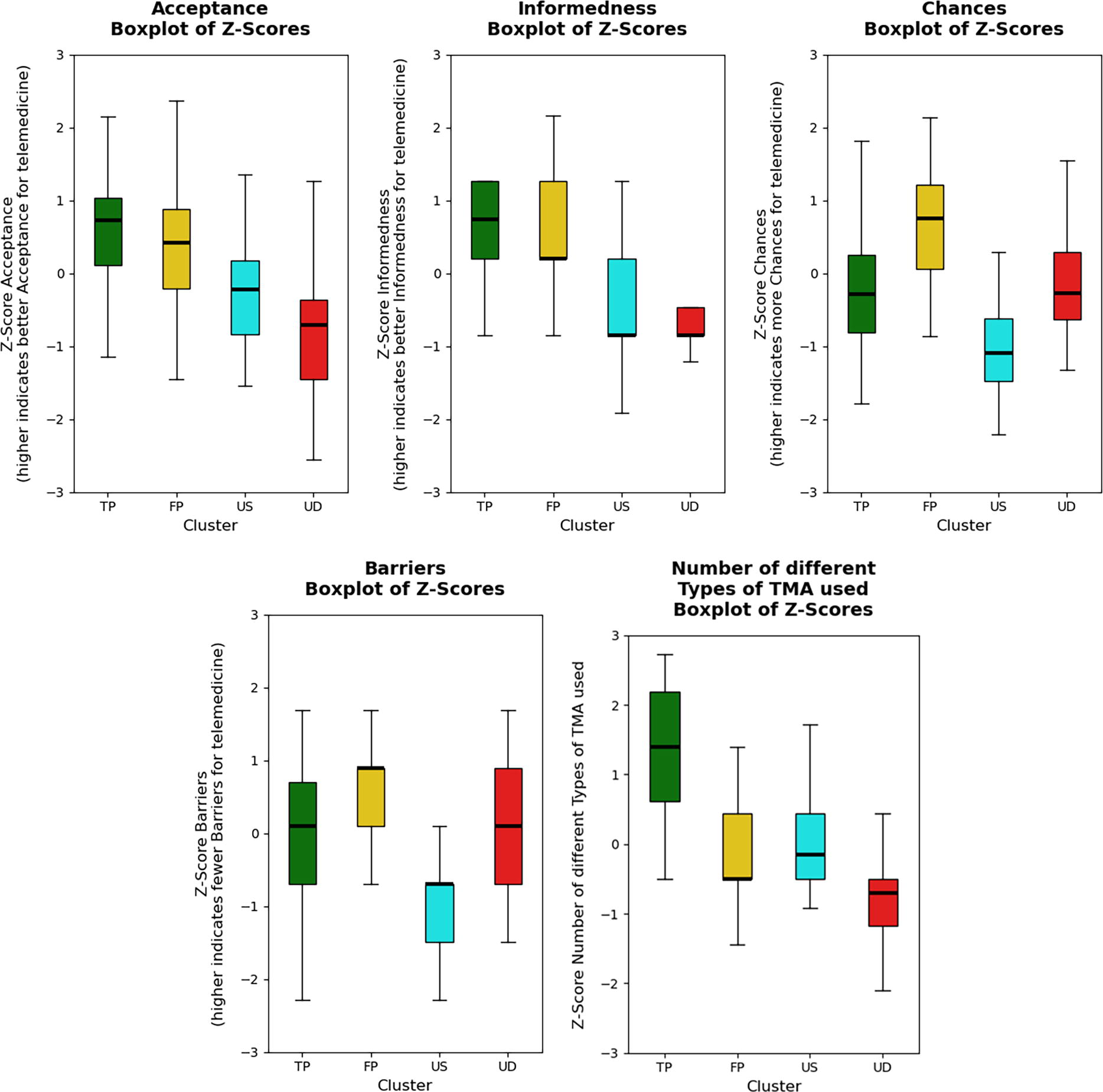
Boxplots of Z-scores.
Mean Composite Scores and 95% Confidence Intervals
Higher value indicates greater acceptance of telemedicine.
Higher value reflects being better informed about telemedicine.
Higher value indicates more perceived opportunities related to telemedicine.
Higher value suggests fewer perceived barriers to using telemedicine.
Indicates how many different types of TMA are being utilized.
Cluster “The pioneers” (TP) consistently exhibited the highest mean scores for variables such as Acceptance (M = 20.29, 95% CI: 18.66–21.92) and Number of TMA Types (M = 2.96), as reflected in both the numerical results and the higher medians observed in the boxplots. In contrast, cluster “The uninformed distanced” (UD) displayed the lowest scores (e.g., Acceptance: M = 10.67, 95% CI: 8.75–12.58), which aligns with their lower medians in the boxplots.
Clusters “The focused practitioners” (FP) and “The using skeptics” (US) demonstrated intermediate scores with narrower CIs, indicating greater homogeneity within these groups. These patterns, highlighted in both Table 3 and Fig 2., underscore the distinct behavioral and attitudinal differences between clusters, emphasizing the consistency of the descriptive and visualized data.
Results: Scatterplot with Confidence Ellipses
The scatterplot illustrates a clear separation between the four clusters in the two PCA dimensions, with minimal overlap observed for most clusters. “The pioneers” and “The uninformed distanced” exhibit the most distinct separation, whereas moderate overlap is evident between “The focused practitioners” and “The using skeptics.” The 95% confidence ellipses provide a visual approximation of each cluster’s internal variability and dispersion along the two principal components. Larger ellipses suggest greater within-cluster variance, whereas smaller ellipses indicate more homogeneous groupings. Fig 3. shows the visualization of the clusters formed.
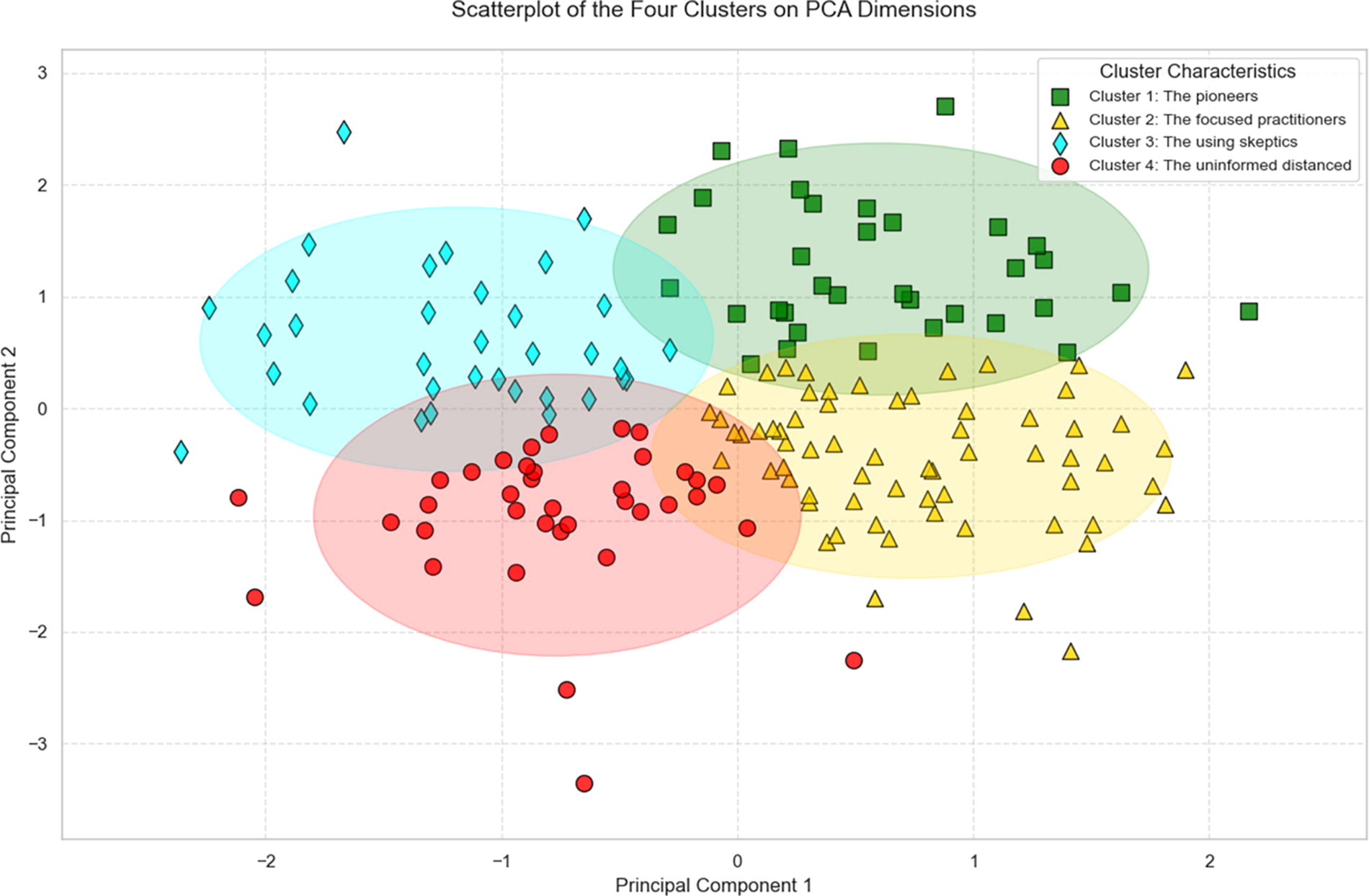
Visualization of the four clusters formed.
DETAILED CHARACTERIZATION OF THE FOUR CLUSTERS
Cluster 1: The pioneers
Cluster 1 comprises 20% (n = 34) of all (n = 170) participants, similar in size to clusters 3 and 4. Members of this cluster demonstrate the highest acceptance (mean = 20.29; 95% CI = 18.66–21.92) and exhibit the highest level of informedness about telemedicine (mean = 3.36; 95% CI = 3.11–3.61). They use an average of 2.96 different TMA, the most among all clusters. They rate the opportunities moderately (mean = 6.94; 95% CI = 5.60–8.28), placing them third, whereas recognizing significant barriers (mean = 3.6; 95% CI = 3.29–4.08) due to their extensive use and familiarity with the technology.
Cluster 2: The focused practitioners
Cluster 2 comprises 38.24% (n = 65) of all participants and is almost twice the size of the other three clusters. Members of this cluster demonstrate high acceptance (mean = 18.68; 95% CI = 17.31–20.06) and a high level of informedness (mean = 3.19; 95% CI = 3.00–3.38), using an average of 1.33 TMA (95% CI = 1.17–1.48), and rate its opportunities (mean = 10.45; 95% CI = 9.59–11.30) the highest, while perceiving the fewest barriers (mean = 4.65; 95% CI = 4.45–4.84).
Cluster 3: The using skeptics
Cluster 3 comprises 20% (n = 34) of all participants. Members of this cluster demonstrate moderate acceptance (mean = 14.02; 95% CI = 12.30–15.74) and moderate informedness (mean = 2.22; 95% CI = 1.94–2.50). They use an average of 1.53 different TMA (95% CI = 1.29–1.78), slightly more than those in Cluster 2. This cluster perceives the fewest opportunities (mean = 3.50; 95% CI = 2.56–4.44) and recognizes the most barriers (mean = 2.41; 95% CI = 2.05–2.78).
Cluster 4: The uninformed distanced
Cluster 4 comprises 21.76% (n = 37) of the participants. Members of this cluster exhibit the lowest acceptance (mean = 10.67; 95% CI = 8.75–12.58) and the lowest level of informedness (mean = 2.15; 95% CI = 1.87–2.43). Their use of different TMA is also minimal, averaging 0.55 (95% CI = 0.33–0.78). The perceived opportunities (mean = 7.57; 95% CI = 6.26–8.88) and barriers (mean = 4.00; 95% CI = 3.67–4.34) are moderately rated within this cluster.
For further characteristics (Age, Sex, and Specialty) of the clusters, see Supplementary Data S9.
Discussion
This study analyzes the use, acceptance, and barriers of telemedicine among 172 physicians—in majority cardiologists—in the German health care system in 2023. This major medical discipline may have a potentially higher affinity, need, or both of this specialty for telemedicine. This may be due to the fact that cardiology patients often require regular monitoring and follow-up, which can be facilitated by telemedicine applications. The high proportion of male participants and predominantly older physicians may reflect a certain bias in the sample but corresponded with the statistical information from the 2022 Federal Medical Register of the KVB. 47
The cluster analysis provides valuable insights into how telemedicine can be implemented more effectively across different user groups. For Cluster 1 (The pioneers), who demonstrate high acceptance and are well-informed, targeted strategies should involve these users as advocates and mentors, encouraging their participation in pilot programs and feedback loops. Cluster 2 (The focused practitioners), with high acceptance but a narrower range of applications, could benefit from interventions aimed at expanding their use of telemedicine tools to enhance patient care. Cluster 3 (The using skeptics) show moderate acceptance but face significant barriers; for them, building trust and addressing concerns, such as technology issues and perceived lack of value, will be key to increasing their engagement. Finally, Cluster 4 (The uninformed distanced), with the lowest acceptance and informedness, requires educational initiatives, focusing on basic training and overcoming technological barriers to improve adoption. To tailor telemedicine services, more advanced features should be introduced to Cluster 1 and Cluster 2, whereas simpler tools should be prioritized for Cluster 3 and Cluster 4 to ensure ease of use. Policymakers and health care providers should allocate resources toward educational campaigns and training, particularly for Cluster 4, to boost telemedicine uptake. Regular feedback mechanisms from Cluster 1 and Cluster 3 could help identify specific barriers, enabling continuous improvements. These actionable insights provide a clear roadmap for implementing telemedicine more effectively, making the findings practical and accessible for stakeholders in health care. It is crucial to develop structures and processes based on real-world practice, as understanding the actual handling of all its differences and variances is essential. This heterogeneity is clearly reflected in the data, highlighting the need to adapt policy measures to accommodate the diverse needs and experiences of users. This knowledge should form the foundation for policy measures, ensuring that telemedicine implementation is not only practical but also adaptable to varying user profiles.
In Germany, data from the Association of Statutory Health Insurance Physicians (KV) indicated that by 2021, 61% of general practitioner practices offered digital services, including video consultations (37%) and online appointments (21%), reflecting a 29% increase likely driven by the COVID-19 pandemic. However, nearly half of these practices reduced their digital services as pandemic restrictions eased. 48 The “Practice Barometer Digitalization 2023” similarly reported that 37% of practices across all medical disciplines used video consultations, but other telemedicine offerings, except for digital communication channels and appointment tools, were not widely mentioned. 49 In contrast, our survey found that only 11% of physicians utilized video consultations, possibly due to the need for on-site diagnostics in cardiology, technical or organizational barriers, and financial disincentives related to the capping of video consultation numbers and negative advance payments by the “Kassenärztliche Vereinigung.” 50 In comparison to international data, a 2021 survey by the American Medical Association revealed that 85% of surveyed U.S. physicians were already using telemedicine, primarily through video consultations (93%) and audio-only calls (69%), with only 8% utilizing remote patient monitoring technologies. 51,52
Despite significant barriers such as high costs (56.4%), insufficient technical expertise (20.3%), and lack of system interoperability (44.8%), 87% of respondents in our study rate telemedicine positively and promisingly for the future. In addition, full acceptance may be hindered by concerns over misdiagnoses and patient safety, as well as unfiltered additional workload from an extra communication channel, potentially without compensation in the worst case. This cost–benefit ratio is increasingly seen as an obstacle to digitalization not only in our survey but also from physicians at the Practice Barometer. 49
The high acceptance of telemedicine among the respondents of this study shows that physicians recognize the benefits of telemedicine for patient care. However, concerns regarding misdiagnoses and perceived patient safety need to be addressed to foster full acceptance. The mixed perception of patient acceptance suggests that it is important to select suitable patients, involve patients more directly in the telemedicine implementation process and take their concerns seriously. However, the use of telemedicine seems to be related not only to sociodemographic factors and personal attitudes but also to the care structure at the patient’s place of residence. Nationwide billing data from statutory health insurance physicians from 2020 show that the number of patients receiving telemedicine care for the first time was lowest in large, independent cities and highest in sparsely populated rural areas. 53 In addition, the “typical” patients in German practices 2021 receiving telemedicine routinely are mainly female, young, and living in urban areas. 53
Although these obstacles are challenging, they are not seen as insurmountable and emphasize the need for resources, knowledge, and uniform standards to facilitate effective telemedicine adoption and implementation, with the diverse attitudes and behaviors across clusters highlighting the importance of tailored approaches to address the specific needs and challenges of different user profiles. The Pioneers and Focused Practitioners demonstrate high levels of engagement and acceptance, driven by informedness and perceived opportunities. In contrast, the Using Skeptics and Uninformed Distanced groups highlight the need for interventions addressing perceived barriers, enhancing technical expertise, and improving system interoperability. This divergence of attitudes and experiences of physicians is also shown in various other studies. 39,42,43 Since 2016, quarterly telemedical remote monitoring of patients with implanted defibrillators or CRT systems has been reimbursed and well-implemented under the German “Einheitlichen Bewertungsmaßstab,” and with the 2022 GBA decision, telemonitoring for heart failure patients using internal or external devices has also been incorporated into the reimbursement system in Germany. 54
STUDY LIMITATIONS
This study has several limitations. With 222 surveyed physicians and only 172 analyzed questionnaires, the sample size is relatively small and may not be representative of all physicians in Germany. The study’s sample is predominantly composed of cardiologists, which limits the generalizability of its findings to a broader population of telemedicine practitioners, such as internists and general practitioners. Participation in the survey was voluntary, potentially leading to self-selection bias. Physicians with a pre-existing interest in or positive experiences with telemedicine may have been more likely to participate. On the contrary, physicians who are critical of telemedicine or have less experience with it might be underrepresented, potentially skewing the results. As the study employs a cross-sectional design, it cannot establish causal relationships between the variables studied as it only provides a picture of current opinions and practices. The results are based on self-reported data, which may be influenced by social desirability and recall biases.
In addition, the reliance on self-reported data inherently carries the risk of subjective bias, which may affect the precision and reliability of the clustering results. To enhance the validity of future analyses, it would be beneficial to complement self-reported data with actual usage data, administrative claims data or routine health care data. For instance, incorporating actual telemedicine usage data and relevant statistical records of practices or clinics, where available, could provide a stronger and more accurate basis for conducting comparisons, refining clustering methods, and interpreting the clusters with greater confidence. When interpreting the results, it should be noted that this study contains several parts of the survey and does not contain all items. In addition, it is worthwhile to mention the fact that this study is not an investigation or discussion of the telematic structure (TI) or the service communication in the medical sector (KIM) in medical practices in Germany. The study does not delve deeply into specific technical barriers and solutions that could affect the implementation of telemedicine and only focusses on attitudes and the acceptance of the respondents.
In addition, albeit the survey contained definition where necessary, there may be differences in the definition and application of telemedicine. Although the survey was conducted in 2023, after the COVID-19 pandemic, the experiences and adjustments made during the pandemic could still influence attitudes and practices regarding telemedicine. The long-term acceptance and use of telemedicine under current conditions need further investigation to provide robust conclusions. In addition, we have notably explored the perspectives of physicians in the ambulatory sector. There is an urgent need to also investigate the patients’ perspective on telemedicine as well as the perspectives of further health care professionals delivering telemedicine care such as medical/physicians assistants and technicians and (newly developed) professions such as discharge heart failure nurses.
Future research should aim to include larger and more representative samples to gain more comprehensive and generalizable insights also contrasting and expanding the case of Germany as it is presented here.
Conclusions
Overall, our study shows the current use of telemedicine as well as the acceptance, barriers, and challenges perceived by physicians in the ambulatory sector in Germany. It underlines the increasing significance of telemedicine for the future of patient care and highlights the necessity of addressing existing barriers to enable broader implementation and acceptance in the ambulatory sector. Although the results indicate that telemedicine in Germany is on a promising path, optimization is still required. The biggest barriers seem to remain reimbursement and the technical infrastructure of the overall health care system in Germany.
Footnotes
Acknowledgments
The authors would like to thank the German Cardiac Society (German DGK: Deutsche Gesellschaft für Kardiologie - Herz- und Kreislaufforschung e.V.), the Association of registered Cardiologist (German BNK: Bund niedergelassener Kardiologen), and the German Society of General Practice and Family Medicine (German DEGAM: Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin) for distributing our survey. The authors also want to thank the working group Rhythmology at the Department of Internal Medicine I at TUM School of Medicine and Health for earlier discussions of the results presented here. The authors would like to express their gratitude to all physicians who took part in the survey.
Authors’ Contributions
All authors have made substantial contributions to the conception or design of the study and have contributed to the drafting of the article including critical revisions.
Ethical Approval and Informed Consent Statement
This study received approval by the Ethics Committee of the Medical Faculty of the Technical University of Munich (reference number 2023-437-S-SB) on 07.08.2023. Respondents of the survey gave written consent before starting the survey.
Data Availability Statement
The full dataset is available from the corresponding author on reasonable request.
Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this study.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6
Supplementary Data S7
Supplementary Data S8
Supplementary Data S9
Supplementary Data S10
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.