
Abstract
Background:
Telemedicine is an effective method to monitor patients at home and improve outcomes of heart failure (HF), especially HF with reduced ejection fraction (HFrEF). However, little is known about the impact of telemedicine on the quality of life (QoL) among outpatients with HFrEF in lower-middle-income countries (LMICs).
Methods:
In this single-center, prospective, randomized, controlled, open, and parallel-group clinical trial in northern Vietnam, patients with HFrEF were allocated to either telemedicine or control groups. Participants in the experimental arm underwent a home-based telemedicine program with regular telephone follow-ups and consultations. Participants in the control group received usual care. Both groups were followed for 6 months. The primary outcome was the change in Minnesota Living with Heart Failure Questionnaire (MLHFQ) score from baseline. The analysis was conducted on an intention-to-treat basis.
Results:
A total of 223 participants were randomized into two groups—the telemedicine group and the usual care group. Of the 223, 170 patients [mean age: 61.5 ± 15.0 years; female: 122 (71.8%)] completed follow-up and were included in the final analysis (87 in the telemedicine group and 83 in the usual care group). At baseline, the MLHFQ scores were equivalent between the two groups (median [interquartile range]: 81 [73–92] vs. 81 [74–92]; p = 0.992). After 6-month follow-up, the telemedicine group showed greater improvement in MLHFQ total scores than the usual care group (mean change in MLHFQ score: −15.5 ± 14.0 vs. −1.3 ± 6.2; difference in change: −14.2 [95% confidence interval, CI: −17.5, −11.0]; p < 0.0001). Similar results were found for the MLHFQ physical dimension score (difference in change: −5.8 [95% CI: −7.4, −4.1]; p < 0.0001) and the MLHFQ emotional dimension score (difference in change: −3.2 [95% CI: −4.2, −2.2]; p < 0.0001).
Conclusions:
In this study, a telemedicine intervention significantly improved QoL compared with usual care among patients with HFrEF in an LMIC.
Introduction
Chronic heart failure (CHF) is a common problem that is associated with impaired quality of life (QoL) and health-related quality of life (HRQoL), as well as high rates of morbidity and mortality. CHF imposes a high burden on health care systems, especially those in lower-middle-income countries (LMICs). 1 Poor QoL, measured by the Minnesota Living with Heart Failure Questionnaire (MLHFQ), is associated with an increased risk of all-cause death as well as the combined endpoint of cardiac death or readmission for decompensated heart failure (HF). 2 In addition to hospitalizations and mortality, QoL is a key target in the management of patients with CHF. 3,4
In outpatient care in most LMICs, patients with HF manage their daily therapy independently, without ongoing support or monitoring from health care professionals. The combination of an aging population and an escalation in health care costs has amplified the need for alternative care strategies for these patients. The World Health Organization (2010) defined telemedicine as “the delivery of health care services by all health care professionals using information and communication technologies for the exchange of valid information for the diagnosis, treatment, and prevention of disease and injuries, where distance is a critical factor.” 5 It offers an opportunity for the delivery of specialist services closer to patients’ homes, reduces costs, and boosts adherence. Telemedicine without routine clinical and home visits has yielded favorable health outcomes, especially QoL for patients with CHF. A meta-analysis conducted on 26 studies with 7,066 participants found that telemedicine markedly enhanced overall QoL for patients with HF when compared with standard care. 6 In the DIAL (Randomized Trial of Telephone Intervention in Chronic Heart Failure) trial, which included 1,518 outpatients in Argentina with stable CHF and optimal drug treatment, the telemedicine group experienced a higher QoL and a significant reduction in admissions for HF compared with the usual care group. 7
Despite the increasing prevalence of CHF in Vietnam, there are few published studies about health-related QoL in this population. In 2023, an initial report revealed notably low HRQoL in Vietnamese patients undergoing outpatient treatment for CHF using the SF-36 questionnaire. 8 Benefits have been observed with the use of telemedicine among patients with CHF in different countries in the world, though not extensively in LMICs. 9 –11 Therefore, this study was conducted to examine the effects of telemedicine on HRQoL in Vietnamese patients undergoing outpatient treatment for CHF.
Methods
STUDY DESIGN
Our prospective, randomized, controlled, open (with randomization concealment), and parallel-group clinical study was conducted at the Vietnam National Heart Institute (VNHI), Bach Mai Hospital, Hanoi. The trial protocol was approved by the
STUDY POPULATION, RECRUITMENT, AND RANDOMIZATION
We recruited consecutive patients with CHF in the specialized HF program at the outpatient department (OPD) from February 2023 to October 2023. The inclusion criteria were as follows: (1) age ≥18 years, (2) CHF with New York Heart Association (NYHA) classification of II-III or NYHA class IV in the last week or NT-proBNP (N-terminal pro-B-type natriuretic peptide) ≥300 ng/mL 12 in the last 12 months or HF hospitalization within 1 year, (3) left ventricular ejection fraction (LVEF) ≤40%, and (4) confirmation of capability and consent to continue treatment with guideline directed medical therapy (GDMT) for HF based on current guidelines. We excluded patients with acute HF, acute exacerbation of CHF, pregnancy, mental illness, and other severe medical conditions that could affect participation. Patients who were unable to use a smartphone and/or tablet or unable to provide their own informed consent were also excluded. In cases where the patient or patient’s family members could not be contacted, we excluded patients due to loss of follow-up.
Potentially eligible patients were screened for eligibility by their treating cardiologists and referred to the research team if deemed suitable for enrollment. Subsequently, the research team confirmed their eligibility, and those who agreed to participate were asked to provide written informed consent. Enrolled participants who completed baseline measurements and assessments were then randomly assigned to either the telemedicine group or the usual care group using a web-based, computer-generated randomization tool.
In the telemedicine group, patients were asked to report daily to their monitoring doctor their weight, blood pressure, heart rate, and any unusual symptoms if present (such as cough, fever, dyspnea, fatigue, chest pain, and palpitations) as per the Self-Check Plan for HF management by the American Heart Association. 13 Based on the measurements and symptoms reported by patients, the clinical team classified the patients’ conditions into two groups: stable and unstable. An unstable condition was defined as patients exhibiting medical alert indicators suggestive of acute decompensated HF that could not be managed at home and required more intensive support: these included frequent dry, hacking cough, shortness of breath at rest, increased swelling in the lower body, sudden weight gain of more than 0.9–1.4 kg (in a 24-h period or 2.3 kg a week), new or worsening dizziness, confusion, sadness or depression, loss of appetite, increased trouble sleeping, inability to lie flat (due to dyspnea), systolic blood pressure (SBP) <90 mmHg, heart rate ≥100 bpm, or BP >180/110 mmHg. 13 –15 In such cases, the clinical team would consult with the patient’s treating cardiologist to provide final recommendations, which could include accessing a local laboratory for necessary blood testing or seeking assistance from the nearest cardiology clinic or emergency service. Patients with a stable condition who did not have any of these conditions were advised by the clinical team to make changes in medications, diet, lifestyle, or exercise at home as necessary. Throughout the study period, two cardiologists and four nurses participated in the telemedicine program. One telemonitoring cardiologist and three nurses worked full-time during daytime hours (Monday to Sunday, from 8:00 am to 5:00 pm), while the remaining cardiologist and nurse provided additional support during periods of increased patient demand. For night shifts (daily from 5:00 pm to 8:00 am), the physicians and nurses alternated to ensure that one cardiologist and two nurses were always available on call from home.
Participants allocated to the control group (usual care) received treatment as determined by their treating physicians, following current guidelines. There was no mandated schedule for visits, medication adjustments, or any type of instruction regarding exercise and diet, as these were determined by the standard practices of the HF clinical team in the OPD. According to the protocol used in OPD, each HF patient was scheduled for a follow-up appointment after a period of 1–3 months, depending on health conditions and specific needs.
STUDY SAMPLE SIZE
Based on our prior pilot study, a total sample size of 166 participants was estimated to achieve 80% power to detect a clinically meaningful 5-point difference in the change of MLHFQ scores, with a two-sided type I error rate set at 5%. To account for an estimated 25% loss to follow-up or refusal rate among participants, each group would need to enroll at least 111 participants, totaling 222 participants.
DATA COLLECTION AND FOLLOW-UP
The clinical research assistant responsible for assigning participants to interventions did not participate in measuring study outcomes. Data on baseline demographics, anthropometrics, clinical history, medication lists, NYHA functional classification, physical signs, and data from electrocardiograms, echocardiograms, and lab tests were collected by study personnel who were blinded to patient randomization status. A 6-month follow-up survey was designed to be collected using one of two methods: in-person administration at VNHI, Bach Mai Hospital, or by phone interview. Participants were followed by dedicated cardiologists and nurses via direct contact in the outpatient setting if the participants attended in-person visits at VNHI. Alternatively, phone interviews were conducted to complete the MLHFQ assessment when participants were unavailable for an in-person visit.
OUTCOME
The primary outcome of our study was the change in the MLHFQ score from baseline. The MLHFQ is one of the best-characterized instruments for assessing health-related QoL 16 and has been highly rated in systematic reviews. 17 –19 The MLHFQ consists of 21 questions specific to HF and appraises HR-QoL over the previous month. Questions are answered using a Likert scale from 0 to 5, where 0 indicates that the question has no impact on the patient or is not applicable, and 5 indicates the greatest adverse effect. The total score ranges from 0 to 105, where 0 represents the best QoL and 105 the worst, with a minimal clinically important difference of 5 points. A total score of <24 signifies good QoL, a score between 24 and 45 signifies moderate QoL and a score of >45 signifies poor QoL. The MLHFQ also provides scores for the overall (full 21 items, range 0–105), physical (8 items, range 0–40), and emotional (5 items, range 0–25) dimensions. 16,17 The questionnaire was used to evaluate the stability of the patient’s health status at the time of enrollment and was repeated after a 6-month follow-up. All clinical outcomes were determined by an independent researcher blinded to patient randomization. Both the English and Vietnamese versions of the MLHFQ show adequate reliability and validity. 20
STATISTICAL METHODS
Descriptive statistics were tabulated at baseline. These include the demographics, clinical history, echocardiograms, and health-related variables. Continuous variables were presented as mean (±standard deviation [SD]) or median (interquartile range [IQR]) and were compared using analysis of variance or Wilcoxon rank sum test depending on the distribution. Categorical variables were presented as frequency and percentage and were compared using the Pearson χ 2 test or Fisher’s exact test. Paired Student’s t tests or Wilcoxon signed-rank tests were conducted to compare data from baseline and after the study within both the telemedicine and usual care groups.
Intention-to-treat analysis was performed with all randomized participants who completed the follow-up for the outcomes of interest. The overall effect of the intervention for the trial was measured by the difference in the change in the MLHFQ score from baseline to the end of follow-up. Multilevel mixed effects linear regression models were used to estimate the intervention effect by comparing MLHFQ scores over time. Fixed effects terms included group assignment and time while subjects were treated as random effects to account for the correlated measurements for each patient.
Stata 17 MP (StataCorp, College Station, TX) was used as the statistical analysis program. A two-sided p-value <0.05 was considered to indicate statistical significance.
Results
CHARACTERISTICS OF THE PARTICIPANTS
The characteristics of patients at baseline are presented in Table 1. From February 2023 to April 2023, a total of 223 outpatients with CHF were enrolled and randomized (112 in the telemedical group and 111 in the usual care group). During the follow-up period, 14 patients were identified as having died, 35 patients were lost to follow-up, and 4 patients requested to withdraw from the study. The final analysis set consisted of 170 patients, with 87 assigned to telemedicine and 83 assigned to usual care (Fig. 1).
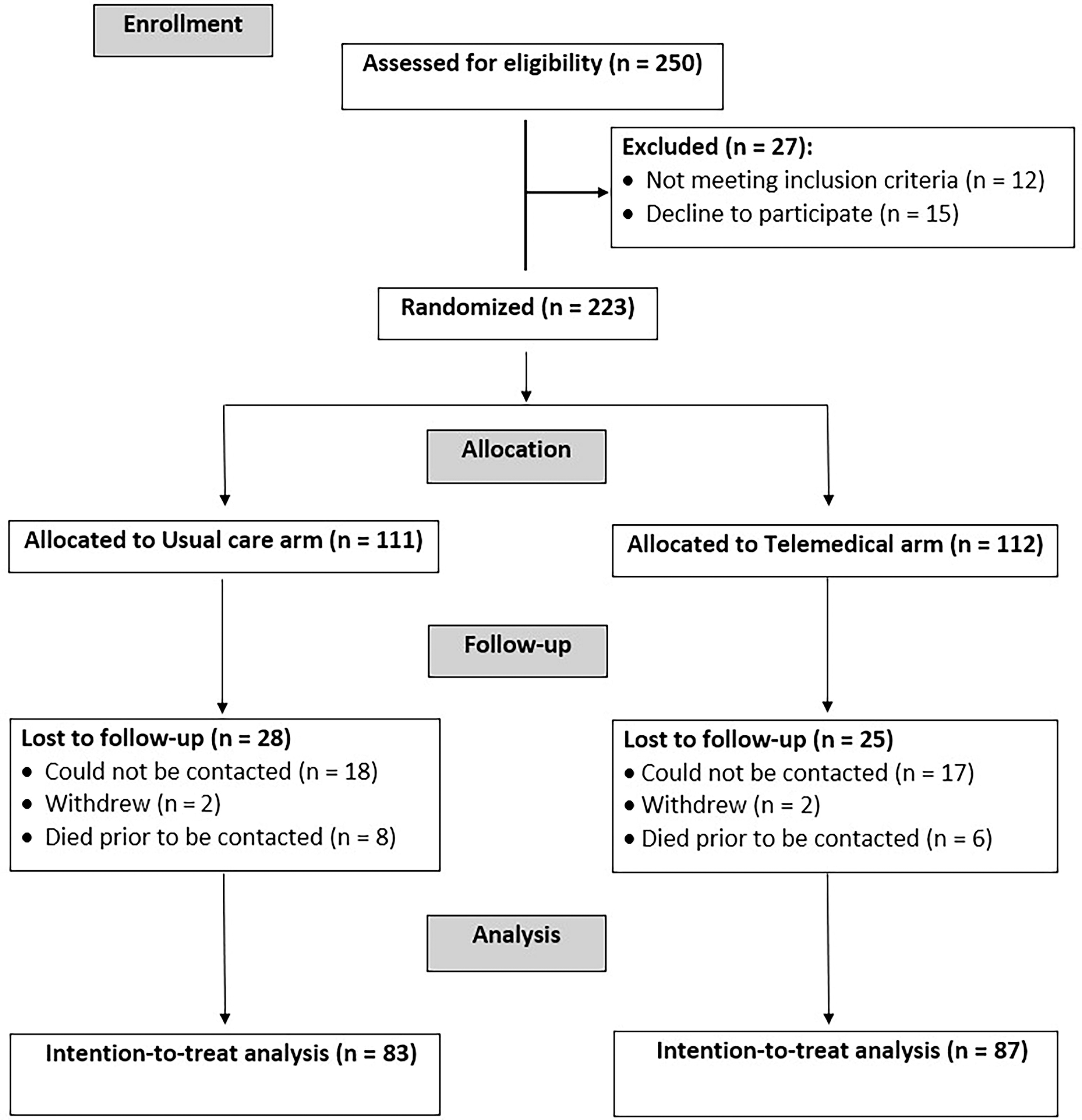
The study population flow diagram.
Baseline Demographic and Clinical Characteristics of the Participants
ACEIs, angiotensin converting enzyme inhibitors; ARNI, angiotensin receptor-neprilysin inhibitor; ARBs, angiotensin receptor blockers; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; LVEF, left ventricle ejection fraction; MRAs, mineralocorticoid receptor antagonists; NYHA, New York Heart Association; SGLT2i, sodium-glucose cotransporter-2 inhibitors; SD, standard deviation.
The mean age of the patients was 61.5 years (SD = 15.0), and 71.8% of the patients were male. The mean left ventricular ejection fraction was 33.2%. Over half (62.9%) were in NYHA functional class II, and 37.1% were in class III. Nearly 70% of the patients at baseline were treated optimally with at least three pillars of HF with reduced ejection fraction (HFrEF) therapy. There were no significant differences between the control and telemedicine groups with respect to patients’ demographic and clinical variables (p > 0.05).
HEALTH-RELATED QOL
At baseline, patients in the control group and intervention group had a similar MLHFQ total score of 81 (74–92), in which physical scores were 34 (32–39) and emotional scores were 20 (17–23), with no statistically significant difference between two groups (p > 0.05).
With a median total score of 80, HF-related QoL of the patients at baseline was poor. After 6 months, there was an improvement in MLHFQ scores in the telemedicine group (median [IQR] mmHg baseline MLHFQ score, 81 [73–92]; at 6 months, 68 [56–78]; p < 0.0001) but not in the usual care group (median [IQR] baseline MLHFQ score, 81 [74–92]; at 6 months, 82 [71–90]; p = 0.013). Improvements in QoL were greater in the telemedicine group (mean change in MLHFQ score: −15.5 ± 14.0) compared with the control group (mean change in MLHFQ score: −1.3 ± 6.2) after 6 months. The analysis revealed a −14.2 point difference [95% CI: −17.5, −11.0) in the MLHFQ total scores between the two groups; p < 0.0001) (Table 2).
Minnesota Living with Heart Failure Questionnaire Quality-of-Life Scores and the Intervention Effect Between Groups
MLHFQ, Minnesota Living with Heart Failure Questionnaire.
Improvement in the MLHFQ physical dimension score was significantly higher in the telemedicine group, compared with the usual care group (there was a −5.8 point [95% CI: −7.4, −4.1] difference in the change in MLHFQ physical scores; p < 0.0001). The MLHFQ emotional dimension score after 6 months improved only in the telemedicine group (there was a −3.2 point [95% CI: −4.2, −2.2] difference in the change in MLHFQ emotional scores; p < 0.0001) (Fig. 2).
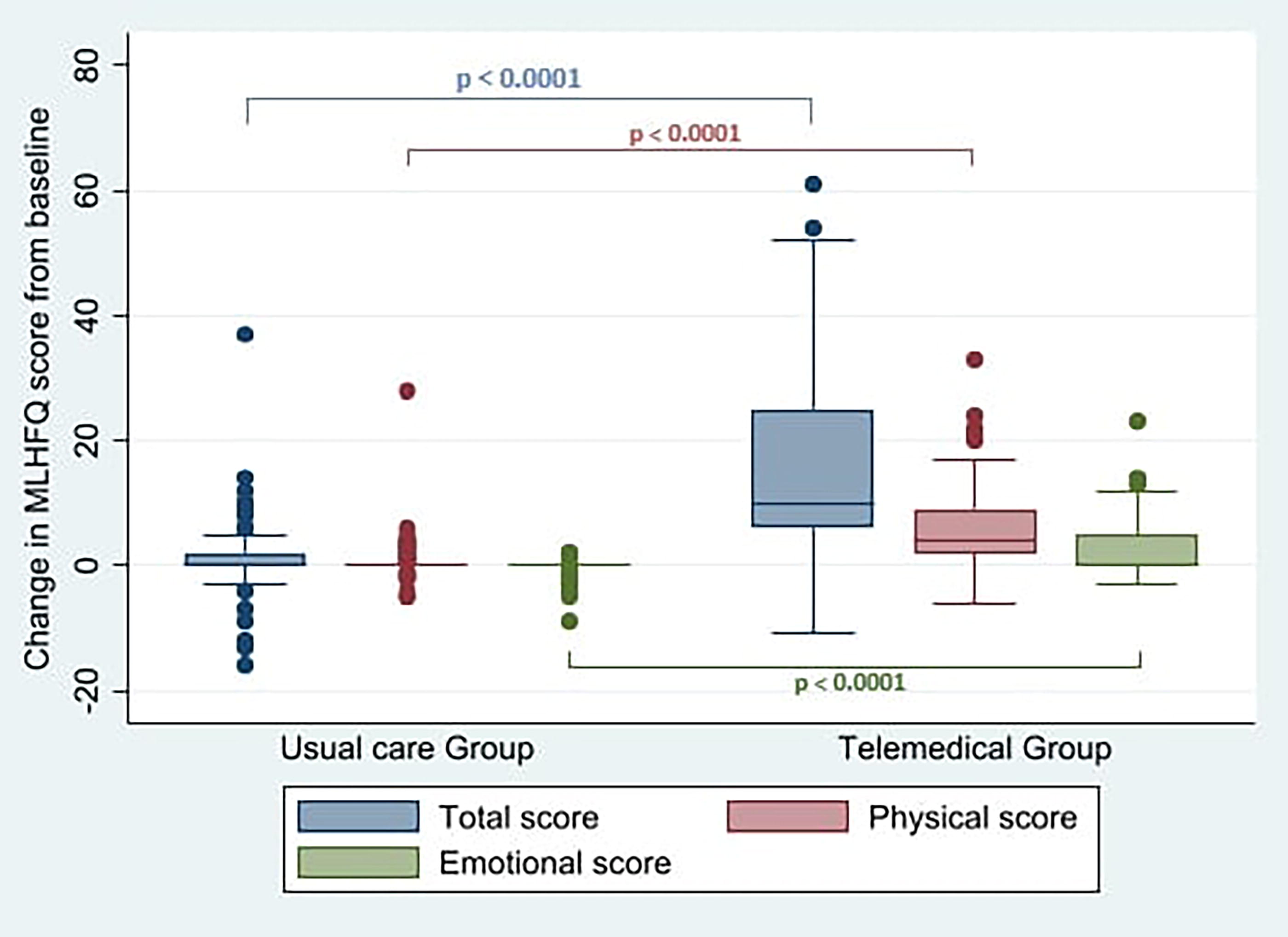
The change in Minnesota Living with Heart Failure Questionnaire (MLHFQ) quality-of-life scores between groups.
During the 6-month study period, the crude mortality rate was higher in the nonintervention group (8 deaths, 7.3%) compared with the intervention group (6 deaths, 5.5%). However, this difference was not statistically significant (p = 0.593).
Discussion
The main finding of our study suggests that telemonitoring leads to improvement in QoL in patients with CHF. After 6 months, QoL measured by the MLHFQ improved significantly in the intervention when compared with the usual care group. Physical score decreased from 34 (31–39) to 29 (24–32), emotional score decreased from 20 (18–23) to 18 (15–20), and overall score decreased from 81 (73–92) to 68 (56–78) (p < 0.0001). This result is similar to the Rehabilitation Enablement in Chronic Heart Failure (REACH-HF) study in 2019 21 on 216 HF patients testing an at-home cardiovascular rehabilitation program through both telephone consultation and face-to-face meetings. REACH-HF showed a significant reduction in MLHFQ score of 5.7 points (95% CI: −10.6, −0.7) (p = 0.025) compared with the control group. Another study by Canadian authors showed that MLHFQ scores decreased in all three domains: overall, physical, and emotional from 53.2 ± 26.3 to 43.4 ± 26.0, 22.9 ± 11.8 to 17.4 ± 11.9, and 12.0 ± 7.5 to 10.2 ± 7.6 (p < 0.001). 22 This result is also in line with Ware et al.’s study when the overall MLHFQ, physical, and emotional scores all decreased by 9.78 ± 2.54 (p < 0.001), 5.44 ± 1.18 (p < 0.001), and 1.51 ± 0.74 (p = 0.04) after 6 months. 22 Telemedicine without regular clinical and home visits has resulted in positive effects on health outcomes in patients with CHF. Clark et al. conducted a meta-analysis including 14 randomized controlled trials of remote monitoring to investigate its effects in patients with CHD and found decreased HF admissions, reduced all-cause mortality, improved QoL, and reduced health care costs. 23
Patients with HF are often symptomatic and have poor QoL. 27,28 Improving QoL is acknowledged as a fundamental goal of HF management. 12,13 In order to improve outcomes such as QoL of patients with CHF, various multidisciplinary projects have been developed over the previous years. Hole et al. demonstrated that reduced QoL, as assessed by the MLHFQ score among elderly HF patients in Norway, is a strong predictor of death. 24 Remote monitoring and consultation have shown effectiveness in improving QoL because of the following reasons. First, patients are promptly diagnosed with precipitations of acute decompensated HF because of rapid identification of worsening edema, sudden weight gain, loss of appetite, decreased urination, frequent cough, stroke, and/or myocardial infarction. Identifying these signs and symptoms early helps doctors prescribe timely treatment before these conditions become critical and lead to hospitalization. Second, the close connection between doctors and patients facilitates early interventions.
Although our study did not comprehensively collect detailed data due to resource limitations, findings from similar telemedicine models have clearly demonstrated the extent of interaction and the impact of telemedicine on the monitoring and management of patients with HF. Specifically, after 12 months of follow-up in the Telemedical Interventional Management in Heart Failure II (TIM-HF2) trial, the median (IQR) number of detailed patient assessments conducted by physicians was 36.0 (0–273), the median number of contacts made with patients to assess key vital parameters was 4.0 (0–37), the median number of medication adjustments was 3.0 (0–57), the total number of times patients were advised to visit the emergency department was 30 (out of 765 managed patients), and the total number of cardiovascular-related hospital admissions was 57 (out of 765 patients). 25 More recently, a clinical trial evaluating the effectiveness of a remote patient management platform in optimizing guideline-directed medical therapy for patients HFrEF demonstrated that after 6 months of implementation, remote monitoring and GDMT titration in this population was effective, safe, feasible, and increased the proportion of patients achieving target doses (82% in the telemedicine group compared with 54% in the usual care group, p = 0.001). 26 This outcome was achieved through close management in the telemedicine group, with an average of 5.23 ± 2.57 remote titration contacts per patient. Furthermore, the telemedicine group also showed a statistically significant reduction in the number of in-person visits (mean number of visits in the telemedicine group was 1.62 ± 1.09 compared with 2.42 ± 1.65 in the usual care group, p = 0.004). 26
MLHFQ scores in our study were higher than those of other studies in Vietnam and around the world. Schulz et al.’s 29 study reported MLHFQ in their telemedicine group and control groups were 50.4 ± 14.0 and 47.1 ± 14.6, respectively. A study in China investigating the effect of home-based telehealth exercise training in Chinese patients with HF showed a baseline MLHFQ score of 49.43 ± 12.25. 30 There are many potential reasons for this phenomenon. First, our patients with HF have lower left ventricle ejection fractions (33.2 ± 5.8) compared with other studies. The Pharmacy-based interdisciplinary program for patients with Chronic Heart Failure (PHARM-CHF) study reported a mean LVEF of 50.4 ± 14.0 in the pharmacy care group and 47.1 ± 14.6 in the usual care group, while in Peng’s study, these numbers were 34.03 ± 6.64 and 34.07 ± 6.66, respectively. 29,30 Lower LVEF correlates with higher MLHFQ scores (lower HRQoL). Second, despite the comprehensive management of VNHI’s outpatient HF program, including educating patients on how to inform doctors whenever alert signs occur to make timely treatment adjustments, adherence remains unstable among patients, depending on various factors, including patients’ views and attributes, social contexts, patient–physician discordance, access, and service issues. 31 –33 Third, the notable increase in Vietnamese patients, especially in central hospitals, adds to the crowded atmosphere in the OPD, leading to shorter consultations between patients and doctors, adversely affecting their satisfaction levels, which contributes to higher MLHFQ score. 34,35
High MLHFQ scores in question 15 ([Is heart failure] causing you to spend more money on medical care?) leading to differences in patients’ QoL can be explained by socioeconomic levels and insurance policy differences of our patients, particularly when our outpatients’ medications were not covered by insurance. In our study, patients scored high on question 10 (Does it make it more difficult for you to have sex?), suggesting that sexual activity is markedly affected by a diagnosis of HF among Vietnamese patients. This is a worldwide issue and has been mentioned in previous HF studies. In a cross-sectional study of 77 stable ambulatory HF patients in Belgium, more than half (58.5%) of the patients indicated an important need for information on how to cope with symptoms associated with HF during sexual activity, and 43.1% of patients experienced an important overall need for counseling concerning sexual activity. 36 Remarkably, Schwarz et al. reported that 75% of females and 60% of men stated that no physicians had ever asked about potential sexual problems. 37 These results highlight the potential value of telemedicine in meeting patients’ information needs of sexual problems.
Depression is frequent in HF and associated with adverse clinical outcomes. 38,39 Mental health disorders may lead to an overall decreased HRQoL due to noncompliance with medical therapy and follow-up clinic appointments. 40 A positive correlation between mental health disorders and low levels of education, poor socioeconomic status, and financial stress in LMIC was demonstrated in several studies. 41,42 In our study, emotional scores in the telemedicine arm improved significantly. The results of prior studies in this area are inconsistent. For instance, Chen et al. reported that there was no significant improvement in anxiety or depression following telehealth exercise training or at 4 months after the program in patients with HF. 43 In contrast, Kulcu et al. reported that an 8-week aerobic exercise program showed a significant reduction in anxiety and depression among patients with HF. 44 In our study, anxiety and depression scores at baseline were high, so there was room for improvement when patients had more interaction with doctors.
Most of the patients in our study claimed that they were satisfied with how they had more time to interact with doctors and share their thoughts and anxiety without the rush that comes from time pressure during a clinic visit. Many of their existing concerns were easily managed and explained by the dedicated telemonitoring doctors. This suggests the importance of telemedicine and collaborative management by a multidisciplinary heart team that includes psychologists, psychiatrists, and cardiologists.
LIMITATIONS
Our study has several limitations. First, although it demonstrated significant improvements in QoL and reductions in HF-related hospitalizations, it was not specifically powered to detect statistically significant differences in mortality outcomes. Second, as a single-center study, the findings may have limited generalizability to other patient populations, given potential variations in geography, ethnicity, culture, and patient management models. Additionally, QoL data were not available for all patients after 6 months due to loss to follow-up and mortality. However, the rates of missing MLHFQ values were similar between the two groups, and the number of deaths was not significantly different.
Conclusions
In this study, our findings provide evidence that telemedicine significantly improves the QoL of patients with chronic HFrEF compared with usual care among patients in an LMIC.
Footnotes
Acknowledgments
The authors are thankful to the Department of Science and Technology of Hanoi City’s People Committee, the University of Medicine and Pharmacy-Hanoi National University, and the Vietnam National Heart Institute, Bach Mai Hospital, for providing them with the opportunity to conduct this study.
Authors’ Contributions
H.T.T.N., D.V.N., P.M.T., J.N.K., and C.M.R. conceived the study design and are responsible for the overall content. P.M.T., H.B.T., H.T.T.N., and D.V.N. collected the data. D.V.N., H.T.T.N., H.B.T., H.M.P., and H.Q.N. analyzed and interpreted the data. P.M.T., D.V.N., and H.T.T.N. prepared the article in collaboration with H.B.T., H.M.P., H.Q.N., L.D.D., J.N.K., R.J., and C.M.R. J.N.K., R.J., and C.M.R. reviewed and edited the article. H.T.T.N. revised and submitted the article. All authors approved the submitted and final versions.
Ethics Approval
This study was approved by the Ethics Committee of Bach Mai Hospital (Number: 1973/BM-HĐĐĐ). To take part in this study, the patients/participants gave their written, informed consent.
Consent for Publication
All participants in the study provided consent for publication.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This research was funded by the