
Abstract
Objective:
One potential solution to limited health care in rural and remote regions is remote presence robotic tele-presentation to allow health care providers to care for patients in their home community via a robotic interface. We synthesized evidence regarding the use of remote presence robotic tele-presentation in rural and/or remote Canadian health settings.
Methods:
Medline, PubMed, and Embase were searched up to August 2023. Remote presence robotic tele-presentation refers to any robotic device used for the purpose of presenting and/or collecting patient information. Primary research was included if the patient was located in remote and/or rural Canada, featured remote presence robotic tele-presentation, and assessed patient, family, or clinician satisfaction, patient transport to nearby regional or urban center, health care costs, clinical outcomes, infrastructure outcomes, adverse events, or telementoring.
Results
: Six studies were included. Patients, nurses, and physicians all reported high levels of satisfaction when using the remote presence robotic tele-presentation. Fifty to sixty-three percent of patients were managed in their home community and did not require transfer to another center. Remote presence robotic sonography resulted in adequate imaging in 81% of first trimester ultrasound limited exams but was less useful for second trimester complete obstetric ultrasounds (20% adequate imaging). Two of eight laparoscopic colorectal surgeries had to be converted to open surgeries. Telerobotic ultrasound clinics resulted in a diagnosis in 70% of cases.
Conclusions:
Evidence suggests remote presence robotic tele-presentation is a safe and cost-effective approach to providing care in distant communities and can prevent some transfers and evacuations to tertiary hospitals.
Introduction
Disparities in health care access and services in remote and rural Canada are well documented, particularly in northern communities. Only 21% of Nunavut residents live within 100 km of a hospital and 20% of Nunavut’s health costs are spent on medical travel 1 (∼26% of its gross national product is spent on health expenditures). 2 Projected 2019 per-person health care spending is greatest in northern territories ($16,090 CAD compared with the Canadian average of $7,068 CAD). 2
Access to health care within home communities is a key social determinant of health, 3 and lack of locally available health care is one contributor to poorer health outcomes. Telehealth is defined as digital health care including phone and/or online/virtual platforms used for medical care, provider and patient education, health information services, and remote patient monitoring. 4 It can improve access to care and has similar health outcomes compared with in-person care for several conditions. 5 Telehealth can reduce patient hardships associated with leaving their community for health care, decrease costs associated with transfers or air evacuations, and help mitigate health care staffing challenges in rural and remote locations. 6,7 The Canadian Medical Association’s 2022 report on virtual care recommended to “make equity a fundamental principle underpinning the delivery of virtual care in Canada.” 8 It is imperative to consider the usefulness, effectiveness, and suitability of various forms of telehealth to meet patient and family needs.
Telehealth is typically conducted using video and/or audio technology. Telehealth use increased during the COVID-19 pandemic. 9,10 A frequently cited limitation of telehealth is the health care provider’s limited ability to perform a physical exam. 11 –14 Recent technological advancements include the use of remote presence robotic tele-presentation (referred to herein as a “robot”) to provide real-time clinical care. The robot is physically located at a rural or remote health center and features can include high-definition cameras, microphones, speakers, stethoscopes, dermatoscopes, otoscopes, and printers. With the assistance of a trained health care provider who is located physically elsewhere (e.g., urban center), the robot can partially address the physical exam. The health care provider can perform functions like driving the robot to the patient's bedside, adjusting camera positioning to facilitate conversation or assessments (e.g., visualization, auscultation), and print patient education materials or prescriptions. Adequate bandwidth is required at both sites to facilitate bidirectional video communication. Robots have successfully provided prenatal sonography 15 and pediatric urgent and primary care in rural and remote Canada. 16
There is growing evidence supporting the utility, feasibility, and potential cost-effectiveness of remote presence robotic tele-presentation in Canada. Our objective was to synthesize the available evidence regarding the use of remote presence robotic tele-presentation in health care settings in rural and/or remote Canada to determine safety, acceptability, and effectiveness in managing medical conditions.
Methods
LITERATURE SEARCH
Pubmed, Medline, and Embase were searched for potentially relevant articles from inception to August 2023. Clinicaltrials.gov was searched in July 2024 to confirm no unpublished or ongoing trials. Search strategies were adapted for each database but included derivations of the following terms: robot, robotic, robotic technology, telehealth, telerobotic, telementoring, remote presence, Indigenous health, rural, remote, and Canada (Table 1). The electronic search output was downloaded into Rayyan 17 and duplicate references were removed. The reference lists of included studies were reviewed to ensure that no relevant studies were missed. The protocol was not registered for reasons outlined by Tawfik et al. including that registration is not mandatory, unclear benefits of registration, time-consuming process, and fear of idea theft. 18 There were no methodological changes once data extraction began.
Search Strategy
INCLUSION CRITERIA
To be included, studies must (1) include individuals of any ages living in rural or remote areas (defined by the author) in Canada whose clinical appointment included the use of a robot with the health care provider in an urban center; (2) measure patient, family, or clinician satisfaction or acceptability, patient transport to the nearby regional or urban center or avoided transfers, health care costs, success in telementoring, clinical (e.g., diagnostic accuracy, initiating treatment) or infrastructure (e.g., sufficient internet, feasibility) outcomes, or adverse event (e.g., missed diagnosis); (3) be a randomized or controlled clinical trial, prospective or retrospective cohorts study, case-control study, case-series, or case cross-over study; and (4) be published in English or French. All medical conditions were included. Other countries were excluded due to the unique challenge of accessing health care in Canadian rural or remote communities (e.g., fly-in communities or roads only available during winter months) in addition to a universal health care system. Studies examining robotic assistance for image guidance during surgeries or ultrasonic-guided procedures at only one physical site were excluded. Robots were defined as any technological system able to be controlled or accessed by a remote health care provider.
STUDY IDENTIFICATION
Titles and, when available, abstracts of the potentially relevant studies were independently screened by two reviewers. Reviewers manually screened the studies into “potentially include” or “exclude.” Full texts of “potentially include” studies were obtained. A priori inclusion criteria were applied independently by two reviewers. Disagreements were discussed and resolved by a third reviewer as needed.
DATA EXTRACTION
Data extracted from each study included: study characteristics (author, year, funding), remote or rural site using the robot and the urban site controlling the robot (location, distance between sites), technology and infrastructure to operate the robot (robot model, capabilities, internet network), health care provider characteristics at both sites (training, specialties), patient characteristics (age, sex, medical condition/concern), and outcomes.
One reviewer extracted the data into an electronic form. A second reviewer checked the data for accuracy and completeness. Disagreements were resolved through discussion.
METHODOLOGICAL QUALITY ASSESSMENT
Methodological quality assessment was completed using the National Institutes of Health’s suite of study quality assessment tools. 19 This method assesses the study’s methodological quality by answering several study design-specific questions as “yes,” “no,” or “n/a.” The appropriate quality assessment tool was selected based on the study design (case–series, case–control, or cross-sectional or cohort study). All three tools included questions about the methodological quality, details of the objective, population, patient selection, exposure and outcome definition, and appropriateness of the statistics, sample size, or presentation of results. Tools for the case–control, cross-sectional, or cohort studies also assessed biases specific to the study design. Tools for the case–series and cross-sectional or cohort studies examined the length of follow-up. Methodological quality was independently assessed by two reviewers. All discrepancies were resolved through discussion or a third reviewer.
DATA ANALYSIS
The lack of consistent selection and reporting of outcomes across the studies precluded a meta-analysis. The data are presented narratively and in tables.
Results
STUDY IDENTIFICATION
Electronic searches identified 3,378 articles and 335 duplicates were removed. In total, 3,043 articles were screened and 124 articles were identified as being potentially relevant. The full text of the 124 articles was reviewed using the a priori inclusion criteria. Reasons for exclusion were: (1) the clinical exam was not conducted in rural or remote Canada, (2) did not use or refer to a tele-presenting robot, and (3) not primary research. Six studies were included (Fig. 1). One study found tele-presentation to be useful during pharmacist-led medicine reviews at discharge; however, it was excluded because the pharmacist’s location was not specified. 20
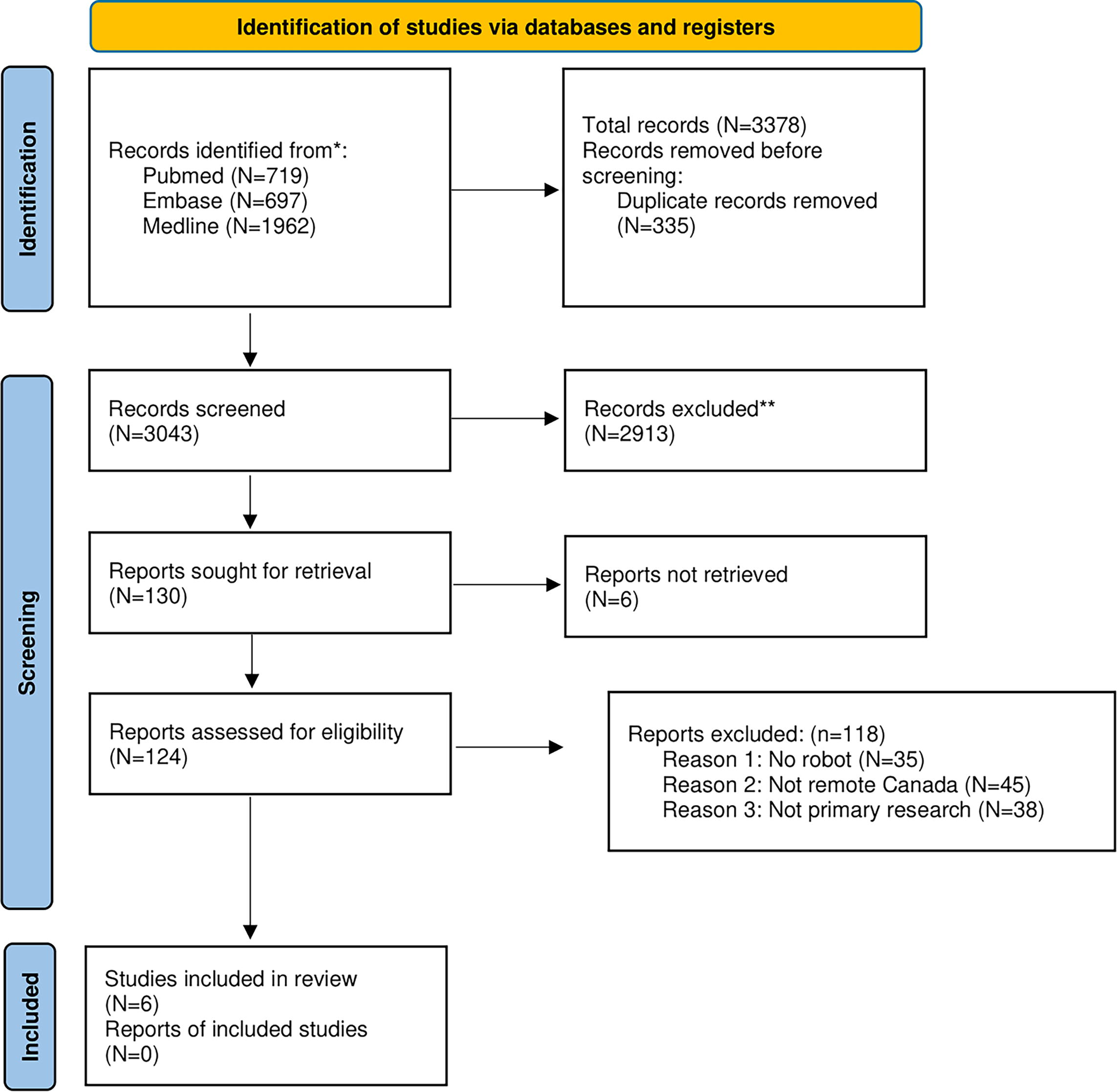
PRISMA diagram of the study identification process. 40 The process of identification of studies to be included in the systematic review. N, number of articles.
STUDY CHARACTERISTICS
The six studies were published between 2006 and 2022 and conducted in Saskatchewan, Ontario, Quebec, and Newfoundland and Labrador (Table 2). Four studies were case–series, 15,21 –23 one cross-sectional, 24 and one case–control. 16 In five studies, the health care provider and the robot site were within the same province. 15,16,21,23,24 In four studies, a physician operated the robot. 16,21,22,24 In two studies, a sonographer operated the ultrasound. 15,23 The clinical conditions included acute pediatric conditions, pregnancy ultrasounds, cancer, colorectal surgery, and diagnostic imaging for pelvic, abdominal, and renal conditions. Four different robots were used. Two studies used versions of the RP-7 Remote Presence Robot (Food and Drug Administration’s Class II medical device) that included a camera, microphone, speakers, and peripheral digital devices. 16,21 In two studies, the MELODY robot was used, which has ultrasound- and sonography-specific capabilities. 15,23 One study used both a telementoring system where a surgical mentor could remotely view a surgery and video output from the laparoscope from the remote operating room and provide demonstrations by drawing on the operating field screen and a Zeus TS microjoint telerobotics system where the mentor could see the remote operating room, operative view, and control a robotic arm remotely. 22 The final study included a digital stethoscope, fiberoptic scopes, and a high-resolution handheld camera; however, the individual pieces were not assembled as a one-piece robot. 24
Characteristics of Included Studies
FDA, Food and Drug Administration; LCS, laparoscopic colorectal surgery; PedCTAS, Pediatric Canadian Triage and Acuity Scale; QOS, quality of service; RPRT, remote presence robotic technology.
METHODOLOGICAL QUALITY OF INCLUDED STUDIES
Five articles were rated as “good” quality, 15,16,21,23,24 and one was rated as “fair” 22 using the quality assessment tool. Common methodological flaws were the lack of sample size justification 16,24 and the lack of follow-up. 21,23,24
OUTCOMES OF REMOTE PRESENCE ROBOTICS
Four outcomes were assessed: satisfaction, 15,22,24 transfers or patient evacuations, 16,21 costs, 21 and quality of the procedure 15,23 (Table 3).
Results and Conclusions of Included Studies
SATISFACTION
Four studies reported patient, nurse, physician, and mentor satisfaction. Brigden et al. surveyed 98 physicians about their experience: 86% were satisfied with the process and 61% believed teleoncology could result in sooner treatment initiation. 24 Half of physicians believed the teleoncology process could be further improved (suggestions not provided). Overall, 91% believed that their patients were satisfied; patient satisfaction was not directly assessed.
Mendez et al. assessed patient, nurse, and physician satisfaction: 95% of patients indicated they would use the robot in a subsequent appointment and 84% felt comfortable with the robot. 21 Approximately half the patients required an interpreter or assistance from a family member; 90% of caregivers believed the robot was helpful during the physician interaction. Most (84%) patients believed the nurse acting as a primary care provider at a rural nursing station improved patient management and diagnostics and 80% reported that the robot facilitated the patient–physician interaction. All nurses thought the robots could help offset nurse recruitment and retention challenges in northern Canada. All physicians surveyed believed the robot improved clinical collaboration, workflow, and reduced stress.
Adams et al. asked patients to identify the advantages and disadvantages of robotic sonography. 15 Advantages included not leaving their community, increased access to ultrasound, convenience, and a safe experience during the COVID-19 pandemic. The disadvantage was that some images were inadequate. Adams et al. found that 95% of patients were willing to have a future telerobotic exam. 23
MEDICAL TRANSPORTATION OUT OF HOME COMMUNITY
Two studies assessed the impact of robots on the need to transfer patients from their rural or remote community to an urban center for care. Mendez et al. reported that 7 of 14 (50%) patients assessed remotely were effectively managed in their home community and did not need to be transferred or evacuated to an urban center. 21 Holt et al. found that 24 of 38 (63%) children treated with robots did not require transfer, 6 (16%) were transferred to a regional hospital, and 8 (21%) to a tertiary center. 16 All 193 children whose management did not include the robot were transferred to a tertiary center. A secondary analysis was conducted where patients treated with a robot were matched based on propensity score to control patients in the Saskatchewan Pediatric Transport Database who required transfer. All control patients were transported to a tertiary center versus 43% of the children whose medical management included a robot. After propensity score matching, 44% of the robot-managed children were transported to a regional center compared with 0% of controls. Among transferred children, the length of stay was similar between children regardless of robot involvement (p = 0.89).
COST
Two studies reported costs associated with flights or projected cost savings by using robots. Mendez et al. reported providing health care to 50% of patients in their home community with robots resulted in a 60% reduction in the number of flights to referral sites. 21 At that time, a commercial flight was about $875 CAD round trip and a one-way medical evacuation flight cost ∼$1800 CAD. Holt et al. estimated a cost savings of $360,000 CAD because 24 of the 38 (63%) children did not need to leave their community compared with the ∼$100,000–300,000 USD cost of the robot (excluding local costs of health management). 16,21,25
QUALITY OF PROCEDURE
Adams et al. reported the success of first and second trimester pregnancy ultrasounds: 81% of first trimester ultrasound limited exams were adequate and 20% of second trimester complete obstetric ultrasounds were adequate. 15 The radiologist recommended repeat exams for 19% of first trimester exams and 70% of second trimester exams. Five of the 21 exams had technical difficulties due to time lags, but this did not impact the actual exam. Adams et al. 23 reported sonographers and radiologists at the urban site felt that 49% of exams were adequate for diagnosis, 24% were adequate with some reservations, and 28% were inadequate. Sebajang et al. assessed surgeon mentor and mentee satisfaction with the use of robotics for colorectal surgery and reported that all were satisfied with the surgery quality. 22 Two laparoscopic surgeries had to be converted to open surgery and the mentor could assist from afar using the robot.
Discussion
This study systematically assessed the evidence regarding the remote presence of robotic tele-presentation in rural and remote Canada. Collectively, the studies reported that it was relatively safe (no adverse events were reported), reduced medical transfers and evacuations to urban centers, allowed for medical care in the patient’s home community, and resulted in cost savings. Physicians, nurses, and patients reported satisfaction with their experience using robots.
Despite a universal health care system, access is not equally available to all Canadians. 26 People in remote and rural communities experience additional barriers to accessing health care (particularly specialist physicians and specialized equipment). 27 While timely health care is a pervasive problem for most Indigenous people, the challenges are most pronounced in rural, remote, and northern communities. 6 With sufficient bandwidth, robots can promote equitable access to health care by allowing patients to access specialized health care professionals and certain health services while remaining in their home community. This could supplement care delivery provided by locum specialists who travel to underserved communities. Robots can reduce the cost, fear, and anxiety associated with traveling to an unfamiliar city to access an often complex health care system that has a history of and continues to exhibit racism and cultural insensitivity. 3,28 However, robots require notable internet infrastructure and their widespread use and impact will require the Canadian government to follow through with commitments to decrease the “digital divide” by providing internet infrastructure throughout rural and remote Canada. 29,30 The Canadian government aims to connect all Canadians to high-speed internet by 2030 and access in rural communities has increased from <40% in 2017 to ∼60% in 2021. 31 Arguments can be made that access to broadband internet is a social determinant of health 32 and that reliance on the internet for health increased during the COVID-19 pandemic. 33 Canada’s promised investment to improve internet access would remove a barrier to broader robot use in rural and remote communities. 34
A limitation of telehealth is that it may be more difficult for the health care provider and patient to establish a trustful relationship. Patients prefer attending telemedicine appointments with a physician with whom they have an established relationship and prefer receiving specialist referrals from a trusted health care provider. 35 Patients and providers found that new relationships were difficult to establish using telehealth and described challenges in communication, rapport building, and alliance. 36 For interested communities, robots may serve as an intermediate between traditional telehealth and limited in-person care. It is important for future research to examine any changes in how people accept robots as part of their health care team.
Two studies found cost savings associated with robot use. Although the costs of purchasing robots are substantial ($100,000–300,000 USD at the time of writing, depending on the model), this cost could quickly be offset by avoided patient transport fees. The national cost for medical transportation of Indigenous patients was nearly $602.2 CAD million in 2022 37 and even partial reductions in travel and temporary living expenses would result in significant savings. Establishing the cost savings associated with robots in rural and remote settings would provide a persuasive argument for the government to increase their use while reducing inequities associated with access to health care and potentially improving health outcomes among those living in rural and remote Canada.
While this may take time to properly implement, we believe that the addition of more robots within Canada can improve timely access to quality health care in remote and rural communities. Preventing patients from being transported for initial assessments would be less burdensome for patients and their families. Robots are a promising tool within a multipronged approach to improving equitable health care access in the Canadian health care system. Decisions about its use will need to be made on a case-by-case basis, in partnership with communities.
LIMITATIONS
Several limitations should be noted. First, the included studies were heterogenous in terms of medical conditions assessed, outcomes measured, and capabilities of the specific robots. While this precluded a meta-analysis, the results of the individual studies largely favored the integration of robots into patient care to improve health care delivery.
The randomized controlled trial is the gold standard for establishing the effectiveness of an intervention or treatment. 38 No randomized controlled trials were identified. Therefore, there may be confounding bias in the observational studies. Although we only included studies published in English, it is unlikely we missed any relevant studies since English is one of two official languages in Canada. None of the included studies included references to French studies. We do not believe this biased our results. 39 While three studies commented on the cultural benefits of patients staying in their home community, 15,16,21 no study examined the cultural relevance or cultural safety of the robots. Qualitative methodology could be used to determine how patients and community members in rural and remote Canada perceive health care that includes robots.
Conclusions
Although only six studies examined the use of robots, the evidence suggests that robots can be successfully incorporated into clinical practice in rural and remote Canadian communities. Robots have the potential to support and increase the medical knowledge, skills, and capacity among people who live and work in rural and remote communities. While the initial cost of the robot is notable, the potential cost avoidance associated with emergency air transfers, food and accommodation stays in urban centers, and the cost of an escort for some patients will quickly offset the initial setup costs.
Footnotes
Author’s Contributions
K.R.: conceptualised the study, provided methodological expertise, and drafted and reviewed the manuscript; E.S.: assessed study inclusion, completed data extraction, assessed methodological quality, and drafted and reviewed the manuscript; H.N.: assessed study inclusion, completed data extraction, assessed methodological quality, and drafted and reviewed the manuscript; M.E.: conceptualised the study; A.D.: conceptualised the study, provided clinical expertise, and critically reviewed the manuscript; I.M.: conceptualised the study, provided clinical expertise, and critically reviewed the manuscript; R.J.: conceptualised the study, provided clinical expertise, and critically reviewed the manuscript; K.W.: conceptualised the study, provided clinical expertise, and critically reviewed the manuscript.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.