
Abstract
Objectives
: To investigate the willingness of the general Hong Kong population to use teleconsultation in primary care and the factors affecting their decisions and to ascertain the medical problems for which people will consider using teleconsultation in primary care. The study was a cross-sectional territory-wide random population survey on adults recruited through a computer-assisted telephone interview system.
Outcome Measures
: Outcomes were the proportion of the general Hong Kong population indicating their willingness to use teleconsultation in primary care; the drivers and barriers affecting their willingness; and the medical problems in primary care for which people would consider using teleconsultation.
Results
: After applying population weighting, 51.6% of the study respondents were found to be willing to use teleconsultation in primary care. The main drivers were possessing the perception that teleconsultation would serve the majority of their health problems (odds ratio [OR] = 3.693, p < 0.001), provision of government subsidy (OR = 3.567, p < 0.001), and ownership of a computer/tablet (OR = 2.116, p < 0.001). A major barrier for people’s reluctance to use teleconsultation in primary care was having an education level of primary or below (OR = 0.388, p = 0.002). The majority of people had reasonable expectations on which medical conditions teleconsultation could be helpful but misunderstandings did exist.
Conclusion
: Our survey estimated that more than half of the general Hong Kong population was willing to use teleconsultation in primary care. Health care service providers and the government should address the drivers and barriers and clarify any misconceptions if teleconsultation is to be further developed in the Hong Kong primary care system.
Introduction
Telemedicine is defined by the World Health Organization as “the delivery of health care services where distance is a critical factor, by all health-care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment, and prevention of disease and injuries all in the interests of advancing the health of individuals and their communities.” 1 Teleconsultation, provision of remote clinical services to clients/patients, is one of the ways how telemedicine is being conducted. 1 Teleconsultations are most commonly conducted via telephone or video. 2 Due to the constraint in physical examination, teleconsultation plays only a minor role in most health care systems. 3,4
In Hong Kong, the development in teleconsultation was not a priority in the past due to the easy accessibility of health care services in this compact city. Few people had used teleconsultation, and the majority of the studies related to teleconsultation in Hong Kong mainly focused on its application in different clinical settings together with the health care provider’s perceptions and specific patient’s acceptance or experience. 5,6
Among the few local studies, Hui and Woo 5 published a paper in 2002 on the feasibility, acceptability, and cost-effectiveness of using telemedicine (videoconferencing) in the public health care system to provide geriatric services to residents of nursing homes. In 2016, Kung et al. 6 conducted an exploratory qualitative study of 30 patient’s views on medical e-consultation in a public primary care setting to assess perceived advantages and concerns of e-consultation. The most notable advantages of e-consultation expressed by the participants of that study were convenience, expected shorter waiting time, and removal of geographic barriers.
However, participants also expressed concerns such as technical difficulties with computer or internet access, lack of personal interaction leading to possibility of inaccuracy in doctor’s diagnoses, pitfalls in cyber security and safety, and issues of getting medications after the e-consultation. Nonetheless, people did express that they would consider using e-consultation if it was simple to use or help from family members or friends was available, especially when their presenting condition was mild or if the consultation only involved a simple follow-up. Participants also suggested that the government could play a role to enhance patient’s trust in e-consultation by setting up relevant operational regulations. The study provided us with insights toward the patients’ needs and concerns toward teleconsultation.
The COVID-19 pandemic changed the world drastically and prompted everyone to turn to teleconsultation service provision and research. During the pandemic, the number of teleconsultation visits in the United States increased by 50% in the first quarter of 2020 compared with the same period in 2019. 7
When the pandemic hit Hong Kong in 2020, custom-made teleconsultation platforms first emerged in the private health care sector and attracted the younger generation to try this alternative mode of consultation. 8 Two years later in July 2022, teleconsultation service exclusive for COVID-19 patient management was also available in the public sector. 9
After 3 years of fighting against the pandemic, in May 2023, the World Health Organization declared COVID-19 was no longer a public health emergency of international concern but should be regarded as an established and ongoing health issue. 10 Governments around the world began to review their public health policies and health care systems’ sustainability. Further developing teleconsultation seemed to be a solution to prepare for future epidemiological crises and to enhance health care accessibility. As primary health care researchers in Hong Kong, our question was “How ready is our general population to accept teleconsultation?”
During the pandemic, Hong Kong population’s smart phone coverage and people’s information technology literacy increased, as around 20,000 smart phones were provided to citizens of the lower socioeconomic class by charity bodies. 11 An online survey conducted by Lingnan University in Hong Kong in May 2020 during the pandemic revealed that among the 638 respondents aged 55 years or more, 61.3% were willing to use teleconsultation “when the relevant technology is fully developed.” 12 The fairly high receptiveness of teleconsultation among the senior citizens in this pilot survey suggested that teleconsultation might be a viable alternative to face-to-face consultations in our locality. However, how “mature” the technology would it then be considered by the public to be “fully developed” remained unanswered.
Another small-scale survey involving 109 participants conducted in Hong Kong in late 2020 among the elderly relatives (age ≥60 years) of a group of medical students revealed that provision of government subsidies for telemedicine services would be the strongest driver, and the only positive independent predictor toward the use of telemedicine both during a severe outbreak, as well as after the COVID-19 pandemic. 13
Our study was the first large-scale population-wide survey to examine the knowledge, attitude, and main concerns of the Hong Kong general public toward using teleconsultation in primary care. We aimed to ascertain the population’s willingness to use teleconsultation and identify the drivers, barriers, and misconceptions behind. We hoped our study could provide insights to inform policy and guide further service development in the field.
Methods
STUDY DESIGN AND SETTING
Data were derived from a cross-sectional, territory-wide random population survey conducted via telephone interviews from October to November 2023. All Hong Kong residents of ≥18 years old with an ability to communicate through telephone by either Cantonese (the most common dialect used in the locality) or English were eligible to participate in the survey. Subjects were recruited through computer-assisted telephone interview system by a local professional public opinion survey center: the Center for Communication and Public Opinion Survey (CCPOS) 14 of The Chinese University of Hong Kong. Participants were recruited through a mixed mode of fixed line telephones and mobile phones in order to obtain a random sample. Verbal consent was obtained from all participants included in the study.
The latest census statistics (July 2022) of Hong Kong 15 was adopted in this study for weighting purposes to project the results to the general Hong Kong population. Since the target respondents in this survey were people aged 18 years or above (instead of aged 15 years or above in the report published by Census and Statistics Department 15 ), the CCPOS had requested the Census and Statistics Department to provide this study with the corresponding data of age 18 or above to produce the weighted data appropriate for our study’s analyses. A similar weighting mechanism had been used by Bedford et al. in their study on the sleep quality of the general Hong Kong population. 16
OUTCOME VARIABLES
The primary outcome in this study was the percentage of the general Hong Kong population indicating their willingness to use teleconsultation in primary care. The secondary outcomes were the demographical factors, people’s knowledge and attitudes toward teleconsultation as the drivers and barriers affecting their willingness, and the ascertainment of medical problems for which patients would seek help with teleconsultation in primary care.
DATA COLLECTION
Pilot testing on the flow of the study was conducted by the CCPOS with 22 subjects using the sampling method mentioned above. The questionnaire was generally well received. The final questionnaire used in the study proper was shown as “Supplementary Data S1.” The key question (Q7), “If teleconsultation is available with your family doctor or the general outpatient clinic, would you consider trying this mode?” was used to address the primary outcome of this study. Major demographical, health-service utilization, and clinical characteristics of the participants were also obtained together with their knowledge and attitudes toward teleconsultation. The participant’s opinions on whether they would use teleconsultation under different clinical scenarios were also collected.
STATISTICAL ANALYSES
For the sample size calculation, we took the conservative estimate of 61.3% from the online survey conducted by the Lingnan University in May 2020 among senior citizens who indicated their interests in using teleconsultation during the COVID-19 outbreak. 12 A sample size of 1,496 was required to construct a two-sided 95% exact Clopper–Pearson confidence interval for the proportion of population indicating their preference in using teleconsultation such that the width of the interval was no wider than 0.05.
Descriptive statistics namely frequencies and percentages of categorical variables were reported for the participant’s demographic and clinical characteristics and their knowledge and attitudes toward the various aspects of teleconsultation. In addition to the analysis at the original sample level, weighted sample data provided by the CCPOS as mentioned previously using random iterative method (RIM method) 17 to project the result in general population level were also analyzed. Multivariable binary logistic regressions were used to assess the single and adjusted effects of sociodemographic factors, knowledge, attitudes, and clinical factors toward the likelihood of people’s willingness to use teleconsultation. Multicollinearity between predictor variables was examined by both correlation matrix and variance inflation factor (VIF). VIF <10 indicated the complete absence of multicollinearity. All tests of significance were two-tailed, and p < 0.05 was considered as statistically significant. Statistical analyses were performed using the Statistical Product and Service Solutions (SPSS).
Results
SUBJECT CHARACTERISTICS
Our study successfully recruited 1,507 subjects to complete the telephone interviews. Fig. 1 illustrates the subject recruitment flow. The overall response rate was 39%, which was similar to previous surveys conducted by the CCPOS.
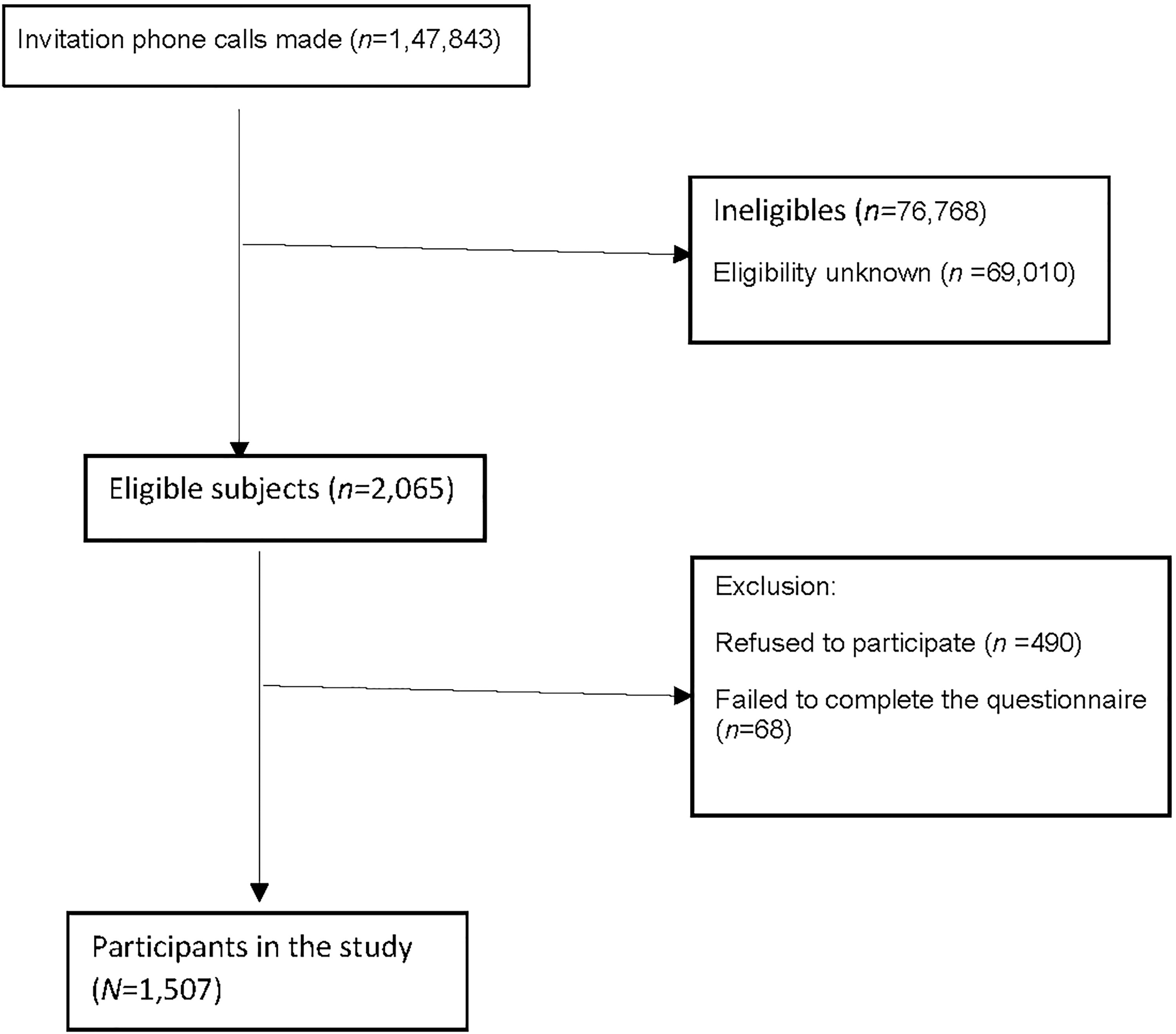
Subject Flowchart.
Results of all demographic variables of the unweighted (original) and the weighted samples as provided by the CCPOS are listed in Table 1. In the weighted sample, most people reported to possess a smartphone (90.3%) or a computer/tablet (72.2%) with internet access. The majority (67.4%) of them did not require chronic follow-up in primary care. Table 2 describes the clinical characteristics of the minority of participants who required chronic follow-up.
Demographic Characteristics of the Participants (N = 1,507)
Clinical Characteristics of the Participants (n = 1,507)
Table 3 illustrates the health care utilization characteristics of the participants. Most people (81.5%) could have access to their primary care service providers in less than 30 min in terms of physical distance. A small proportion of the participants (6.6%) required assistance to attend a primary care service point. Only 11.5% of the participants had prior experience in using teleconsultation as a patient. When we asked the key question, “If teleconsultation is available with your family doctor or the general outpatient clinic, would you consider trying this mode?” 51.6% of the participants replied “Yes”. Among those who are willing to try teleconsultation in primary care, >90% considered a charge of lower than or equal to face-to-face consultation as reasonable. Only 6.5% of these respondents accepted a higher charge.
Health Care Utilization Characteristics of the Participants (N = 1507)
Table 4 lists out the participant’s decisions as to whether they would choose teleconsultation under various medical conditions. More than half of the participants in the weighted sample stated that they would consider using teleconsultation when they suffered from mild respiratory tract (60.6%) or gastrointestinal symptoms (53.2%) or for stable known chronic illnesses follow-up (65.9%). On the other hand, although being the minorities, significant proportions of the participants would consider using teleconsultations in medical emergencies such as acute chest pain (20.9%), shortness of breath (27.2%), suspected stroke (16.5%), or if they had thoughts of self-harm or harming others (32.8%).
Proportion of Participants Who Would or Would Not Consider Using Teleconsultation Service in Primary Care Under Different Clinical Scenarios (N = 1,507)
Less than one-third (30.5%) of the participants in the weighted sample knew that paid teleconsultation service was available in the private primary care sector in Hong Kong, and only 28.4% knew that drugs and documents such as sick leave certificate delivery was inclusive in the service. Only 20% of the weighted sample knew that patients must be physically present in Hong Kong when they receive teleconsultation services provided by doctors practicing in Hong Kong. Only 10.7% of the weighted sample knew that the Hong Kong Medical Council had issued Ethical Guidelines on the practice of telemedicine in Hong Kong 18 to govern doctors’ practice.
The vast majority (74.3%) of the weighted sample agreed that government subsidy would attract them to use teleconsultation in primary care. Many of them (71.7%) agreed that teleconsultation could reduce their risks of getting cross infections in the clinic.
As for the concerns, 78.0% of the weighted sample worried about the accuracy of the doctor’s diagnosis in the absence of onsite physical examination. Half (50.7%) of the participants worried about patient information and health care record confidentiality issues. More than half (56.2%) of the participants worried about post-teleconsultation logistics such as drug and document delivery.
PREDICTORS ON THE WILLINGNESS OF TELECONSULTATION
Results of 13 (0.9%) and another 226 (15.0%) participants were excluded from this part of the analysis due to missing answers either to the key question on their willingness to use teleconsultation in primary care or to the predictor variables, respectively.
The results of multivariable logistic regression based on the unweighted samples are presented in Table 5. A statistically significant positive relationship was shown with a perception that teleconsultation would serve the majority of his/her health problems (OR = 3.693, p < 0.001), availability of government subsidy (OR = 3.567, p < 0.001), perception of teleconsultation could reduce one’s infection risk (OR = 1.831, p < 0.001), ownership of a computer/tablet with internet connection (OR = 2.116, p < 0.001), and in those who need assistance for accessing primary care services (OR = 1.838, p = 0.046). Statistically significant negative associations were shown with an educational level of primary or below (OR = 0.388, p = 0.002), not knowing that prescription and document delivery was inclusive in the teleconsultation services provided in Hong Kong (OR = 0.651, p = 0.014), and foreseeing problems in diagnosis accuracy (OR = 0.675, p = 0.040) or post-teleconsultation logistics (OR = 0.505, p < 0.001). Remarkably, those who knew that paid teleconsultation was available in the private sector tended not to use this mode of service (OR = 0.667, p = 0.013). From the responses of our participants to the open question on whether there were any other factors that would affect their willingness to use teleconsultation in primary care, we were satisfied that we had covered all the major domains of interest among the respondents.
The Association Between Willingness to Use Teleconsultation in Primary Care and the Participants’ Demographic Factors, Knowledge, and Attitudes by Multivariable Logistic Regression Model Based on the Unweighted Sample (n = 1,268)
Tertiary education or above included participants who were nondegree bearers and those with a Bachelor degree or above.
significant at 5% level by multivariable logistic regression.
Thirteen respondents were excluded due to their missing answers for the question on their willingness to use teleconsultation in primary care.
226 respondents were excluded due to their missing answers in any of the predictor variables.
White collars were defined as participants who worked as employers, professionals, associate professionals, and clerical workers.
Blue collars were defined as participants who worked as service providers and manual workers.
Primary level or below included the participants with primary and pre-primary education levels.
Discussion
This was the first cross-sectional population survey on the topic of teleconsultation in primary care in Hong Kong. From the projection of our weighted sample, it was encouraging to see over half (51.6%) of the general Hong Kong population indicated their willingness to use teleconsultation in primary care.
Due to the easy accessibility of health care services in Hong Kong, the time to reach a primary care clinic did not associate with the willingness to use teleconsultation among Hong Kong citizens. However, the need of assistance to attend a primary care clinic in some people was clearly a strong pull-factor. “Convenience” was also a major driver to use teleconsultation, especially for those who thought teleconsultation could address most of their health problems. This was consistent with the results from the qualitative studies by Powell et al. for primary care patients in the United States. 19 Moreover, avoiding getting infections from clinic attendance was also a strong reason for Hong Kong people to choose teleconsultation. This aligned with the findings in the study conducted by Baudier et al. among respondents from Europe and Asia. 20 Previous local studies and the current study all echoed that provision of government subsidy would be a significant facilitator to attract people to use teleconsultation. As the COVID-19 pandemic greatly increased the coverage of electronic device ownership among our local citizens, it might be a good time to consider further developing teleconsultation in primary care.
Barriers identified from our study toward choosing teleconsultation in primary care were low education level, having worries on the post-teleconsultation logistics (drug and document deliveries), and the accuracy of the doctor’s diagnosis in the absence of onsite physical examination. It is noteworthy that people who knew that teleconsultation was available in the private sector tended not to use the service. This shall be an area requiring further exploration in future.
In terms of expectations toward teleconsultation in primary care, most people were very reasonable and would consider using teleconsultations if they suffered from common mild illnesses or for follow-up of stable chronic diseases. However, it was alarming to see that although not many, some people did indicate that they would use teleconsultation if they had medical emergencies such as acute chest pain, and shortness of breath. We suspect that might be due to people’s assumption that teleconsultations implied a shorter waiting time to see the doctor. Anyhow, misunderstanding did exist in the population toward what were the suitable conditions to be handled by teleconsultation. More education to the general public regarding the proper use and limitations of teleconsultation is definitely needed (especially toward the less educated population, which was also proposed by Alboraie et al. in their study in Egypt 21 ) to avoid delays in treatment and patients’ disappointments.
STRENGTHS
This was the first territory-wide cross-sectional survey to holistically examine the population’s willingness, knowledge, attitudes, and main concerns toward the use of teleconsultation in primary care in Hong Kong. The data were derived from a large representative sample with high data completion rate. As the survey was done by random telephone interviews, we believed it entailed a high generalizability across the population.
LIMITATIONS
As teleconsultation is only beginning to take hold in Hong Kong’s primary care system, and the majority (88.5%) of the respondents had no experience with the use of teleconsultation, most of the respondents’ replies were based on their hypothetical assumptions toward teleconsultation.
Moreover, as most of the teleconsultation services available in Hong Kong were offered through video instead of pure audio phone calls, the participants’ considerations were likely to be based on the video type of teleconsultation and hence the results may not be suitable for direct application in other parts of the world, especially if the use of audio phone calls is predominant.
IMPLICATION FOR FUTURE RESEARCHES
Although our study showed acceptability among Hong Kong people to use teleconsultation in primary care, we noted people who knew about the service being available in the private sector tended not to use it. It would be good to conduct further in-depth qualitative studies among those Hong Kong citizens who have used teleconsultation services in primary care to obtain their feedbacks in order to identify the underlying obstacles.
Conclusions
Our survey estimated that more than half of the general Hong Kong population were willing to use teleconsultation in primary care, and hence this modality of care should be further resourced. Facilitators and barriers to choose teleconsultations when receiving primary care services were clearly identified. The government and health care providers should address these factors to meet the public expectation while safeguarding the quality of the services provided. More resources should also be invested in public education regarding the proper use and the limitations of teleconsultations in primary care.
Footnotes
Acknowledgments
The authors thank Mr. Chan Kok Yin Eugene, our project’s research assistant, who made a significant contribution to the statistical analysis, results interpretation, and article drafting. Appreciation also goes to Dr Tang Ho Man Eric, senior research assistant, for his contribution and guidance in our statistical analysis.
Authors’ Contributions
E.T.Y.T., C.K.H.W., J.Y.C., D.D.W., and T.P.L. contributed to the study design. E.T.Y.T. coordinated the acquisition of data. E.T.Y.T. and C.K.H.W. contributed to data analysis, interpretation of results and writing of the article. J.Y.C., D.D.W., and T.P.L. contributed to interpretation of results and review of the article. All authors read and approved the final article.
Ethical Approval
Institutional Review Board of The University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB) (Reference number UW 22-743).
Availability of Data and Materials
Our research data are available upon reasonable requests.
Disclosure Statement
No competing financial interests exist.
Funding Information
Health and Medical Research Fund, the Health Bureau, The Government of the Hong Kong Special Administrative Region (Project reference: 20212351). Kerry Group Kuok Foundation (Hong Kong) Limited supported the publication as an open access journal article.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.