
Abstract
Background:
Although depression is one of the most common mental health disorders outpacing other diseases and conditions, poor access to care and limited resources leave many untreated. Secure messaging (SM) offers patients an online means to bridge this gap by communicating nonurgent medical questions. We focused on self-care health management behaviors and delved into SM initiation as the initial act of engagement and SM exchanges as continuous engagement patterns. This study examined whether those with depression might be using SM more than those without depression.
Methods:
Patient portal data were obtained from a large academic medical center’s electronic health records spanning 5 years, from January 2018 to December 2022. We organized and analyzed SM initiations and exchanges using the linear mixed-effects modeling technique.
Results:
Our predictors correlated with SM initiations, accounting for 25.1% of variance explained. In parallel, 24.9% of SM exchanges were attributable to these predictors. Overall, our predictors demonstrate stronger associations with SM exchanges.
Discussion:
We examined patients with and without depression across 2,629 zip codes over five years. Our findings reveal that the predictors affecting SM initiations and exchanges are multifaceted, with certain predictors enhancing its utilization and others impeding it.
Conclusions:
SM telehealth service provided support to patients with mental health needs to a greater extent than those without. By increasing access, fostering better communication, and efficiently allocating resources, telehealth services not only encourage patients to begin using SM but also promote sustained interaction through ongoing SM exchanges.
Introduction
Mental health affects nearly half of Americans 1 and is the leading cause of disability around the world. 2 Depression is one of the most common mental health disorders outpacing other diseases and conditions. 3 Despite this, many affected individuals go untreated due to poor access to care and limited resources. 4 The problem is exacerbated by various barriers such as geographic isolation, financial limitations, and social stigma. 5 With the advancements in health information technologies, telehealth services, which include video visits, e-visits, and secure messaging (SM), have emerged as a promising solution that can bridge this gap. SM offers patients an online means to communicate discreetly, privately, and asynchronously a wide range of nonurgent medical questions with their health care teams in anticipation of more timely and personalized care plans. This is nontrivial given that 82.3% of American adults visit providers each year 6 and telehealth usage has seen a significant rise partly attributed to the COVID-19 pandemic, with 68% of patients now engaging with such services, up from 45% 2 years ago. 7 During the same period, the number of secure messages doubled. 8,9
This study seeks to delve into the SM utilization patterns among individuals with depression. While the significant growth in the use of SM has been associated with improved health care access and outcomes, 10 –12 the specific ways in which people with depression are using SM remain unclear. Individuals with depression might be using SM services more for several reasons. The level of anonymity and privacy associated with SM enables individuals with depression to more easily express their thoughts and feelings in writing who otherwise may hesitate to ask for advice openly or fear judgment. 13 Depression can sometimes manifest as difficulty in verbal expression, so SM serves to communicate feelings and experiences more clearly and accurately in a pace and manner when individuals feel ready. 14 Therefore, we seek to shed light on whether patients with depression use SM more frequently and to understand the broader implications of their self-care health management behaviors. We delve into SM initiation as the initial act of engagement and SM exchanges, akin to e-mail threads or conversations, as continuous engagement patterns. This differentiation may provide deeper insights into telehealth’s role in supporting patients with mental health needs, highlighting areas for improving accessibility, communication strategies, and resource allocation to enhance patient health care and outcomes. The insights gleaned from this study could inform the enhancement of SM services, including the use of mobile technologies to facilitate greater patient–provider communication. 15 Given the ongoing digital divide challenge, this study also underscores the importance of addressing health equity and disparities in technology access and usage to ensure that the benefits of telehealth, and more specifically SM, reach all segments of the population. 16
OBJECTIVE
We aim to examine whether those with mental health issues might be using SM more. More specifically, we focus on the interplay among demographic, racial, geographic dimensions, and technology use among individuals with depression that explains the extent to which individuals with depression engage in SM initiations and exchanges.
Methods
This retrospective analysis was approved by the Institutional Review Board at the University of Cincinnati (IRB20230600).
Our longitudinal analysis assessed telehealth SM use among patients with depression due to increasing depression rates. We used patient demographic and portal use data from a large academic medical center’s (AMC) electronic health records (EHR) spanning from January 2018 to December 2022. The dataset comprised patients with portal accounts, representing approximately 60% of the AMC’s patient population. Patients diagnosed with depression were identified using ICD-10 (International Classification of Diseases, Tenth Revision) codes F32 and F33, whereas others were categorized as nondepressed patients.
In primary care settings, depression is routinely screened, diagnosed, and monitored using the established Patient Health Questionnaire. Unlike chronic conditions characterized by physical symptoms such as elevated HbA1c or blood pressure, mental illnesses such as depression manifest through nonphysical symptoms such as feelings, mood, and thoughts that are often accompanied by stigma and judgment. Our focus was on self-care health management behaviors, where patients take charge of maintaining their good health, managing conditions, and coping with illness and disability. Thus, we set out to examine potential differences in self-management practices between patients with and without depression by analyzing SM initiated by each patient and exchanges that continued. Overall, we posit that patients with depression will engage in SM use to a greater extent than patients without depression.
MEASURES
Table 1 depicts a partial structure of the SM table. When a patient uses the SM telehealth service, the EHR generates unique message IDs and encounter IDs. Each response also gets a unique message ID and a parent message ID but maintains the encounter ID for continuity in the conversation. The first patient–encounter pair signifies one Secure Messages Initiated [SM_INIT], whereas the total number of messages sent and received represents Secure Messages Exchanged [SM_EXCHG]. We aggregated SM_INIT and SM_EXCHG yearly due to missing data in monthly aggregation.
Secure Messaging Exchanges by One Patient
aMessage identification number.
bParent message identification number.
cEncounter identification number.
Zip code [Zip]. A five-digit zip code representing a patient’s residential mailing address, reflecting socioeconomic status and geographical location potentially impacting patients’ SM use.
Year [Year]. Our dataset spanned from 2018 to 2022.
Age [Age]. The patient’s age was determined as of March 2023 (date of data extraction), with our study focusing on adults, excluding those younger than 18. In addition, ages over 89 were grouped into a single category of 90 or older to adhere to Health Insurance Portability and Accountability Act (HIPAA) regulations.
Gender [Female]. Biological sex at birth was coded as 1 for females and 0 for males.
Underrepresented minority [URM]. Race was self-reported, with Black coded as 1 (representing 21% of the dataset) and White as 0 (representing 72.4% of the dataset). Other races (e.g., Asian, Hispanic, Pacific Islander, Mixed, and Others) were not coded as they collectively represented <7%.
Marital status [Married]. Marital status was self-reported from the most recent encounter, with married coded as 1 and others as 0 (e.g., separated, widow, divorced, significant other).
Low income [Low_Income]. Patients with low income were determined using Medicaid eligibility. We coded Low_Income = 1 for patients whose 2022 insurance plan was “Medicaid” (operating on a fee-for-service) or “Managed Medicaid” (administered by Managed Care Organizations). Other insurance plans, including Commercial and Medicare, were coded as 0.
Patient portal use [PP_Time]. Our dataset included patients with a patient portal account, necessary for accessing telehealth services. Patient portal activities were time stamped per session, capturing active time from log on to log out. The total annual active time spent on the patient portal, PP_TIME, was recorded in hours. The EHR could discriminate between “active” and “inactive” time (e.g., forgot to log out).
Diagnosed with depression [Depr_Diag]. Our study assessed SM telehealth’s differing effects on patients, tracking those with ongoing depression (ICD-10 codes F32 or F33) 17 annually and excluding those whose diagnoses were not present in subsequent years. We coded DEPR_DIAG = 1 for diagnosed patients and DEPR_DIAG = 0 for others each year.
STATISTICAL ANALYSIS
We analyzed adult patients with telehealth access, categorizing them based on depression status. We used linear mixed-effects models (LMEM) for statistical analysis, which are adept at handling fixed and random effects as predictor variables. 18 Fixed effects are explanatory variables akin to those in standard linear regression models, while random effects act as categorical control variables often used for grouping predictors. In our study, we controlled for the impact of sociodemographic predictors such as zip code-based location and changing conditions year-to-year such as pre- and post-COVID-19 pandemic effects, on patients’ SM use.
Results
SM initiations and exchanges are illustrated in Fig. 1, and the characteristics of study measures are provided in Summary Statistics in Table 2. Our baseline models (Table 3) allowed our intercepts—that is, Zip and Year means—to randomly vary for SM initiations and exchanges; these models tested for whether there were significant variations in Zip and Year means. In other words, the variance that arose within each zip code and the variance that occurred between zip codes contributed to the overall variance. Similarly, the variances within and between years also contributed to the overall variance. LMEM has the advantage of capturing uncertainty resulting from heterogeneity among zip codes and years. Although our main interest was not in inter-Zip or inter-Year variations, they needed to be controlled. The “Intercept” for both models A (β = 1.315, p < 0.01) and B (β = 3.722, p < 0.01) was positive and significant suggesting that Zip and Year vary significantly. There was a total of 430,315 observations accounting for a total of 6.3% and 6.0% variations in SM initiations and exchanges, respectively, that can be explained by the Zip and Year random variables.
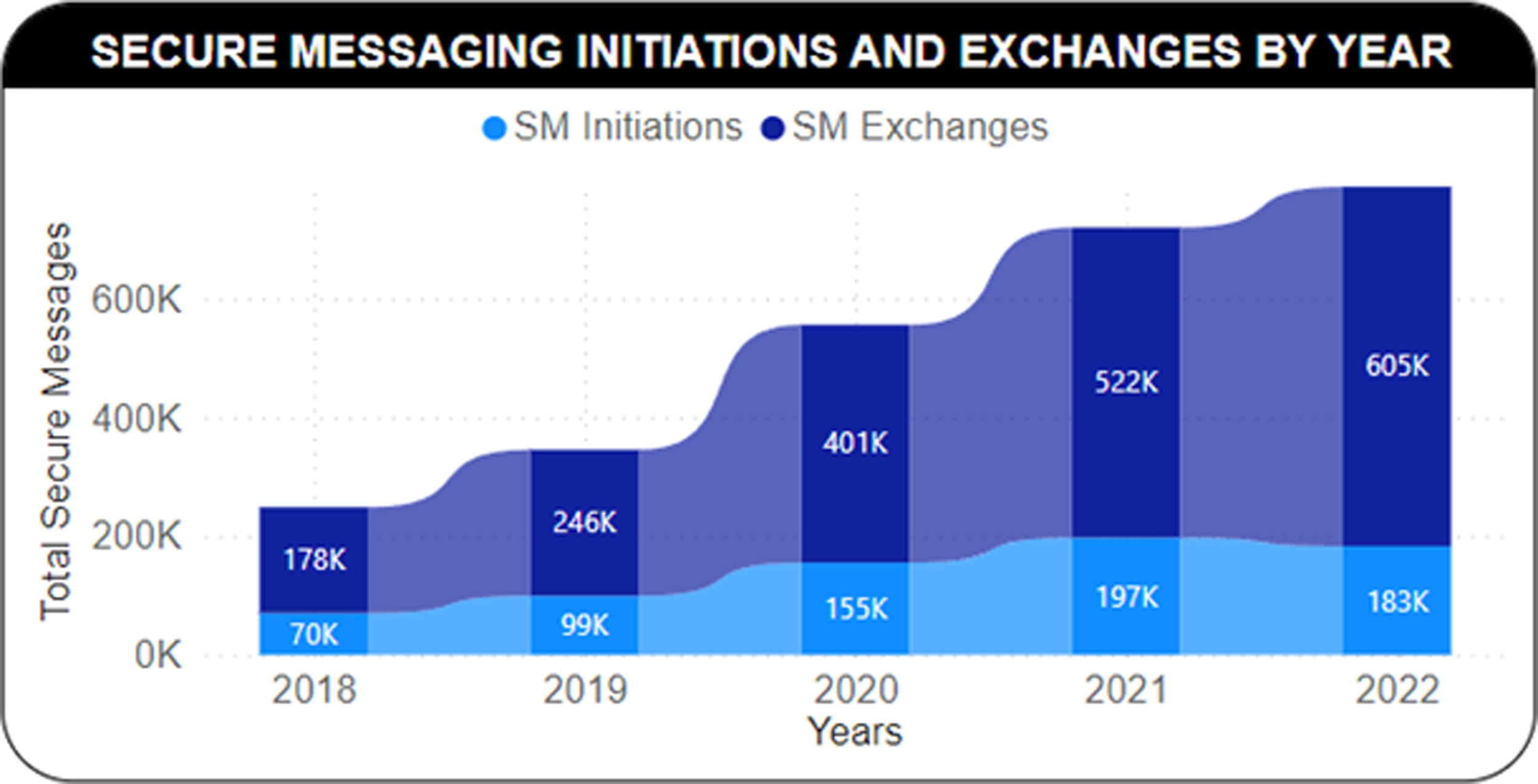
Total number of secure messaging initiations (lighter shade) and exchanges (darker shade) highlighting the increasing growth in the use of secure messaging telehealth service.
Summary Statistics
Linear Mixed-Effects Model Statistics—Baseline Models
p < 0.05.
p < 0.01.
p < 0.001
aSecure messaging.
The fixed-effect results are shown in Table 4. We controlled for Zip and Year captured as the “Intercept” (explained above in the baseline models). The fixed-effect variables explained 22.5% of variations in SM initiations and 22.9% in SM exchanges. Our primary interest was to determine whether patients with depression were more likely to use SM relative to patients without depression. Our results showed a positive and significant relationship with SM initiations ([7]: β = 1.628, p < 0.001) as well as continued SM exchanges ([7]: β = 4.914, p < 0.001) indicating that patients with depression were more likely to use SM.
Linear Mixed-Effects Model Statistics—Full Models
p < 0.05.
p < 0.01.
p < 0.001.
aFixed effect.
Prior literature suggests that in the primary care context, older adult patients sent secure messages to a greater extent to communicate with their providers. 19 In our dataset, we observed no significant differences in SM initiations ([1]: β = −0.001, n.s.) for our population; however, older patients exchanged messages significantly less than their younger counterparts ([1]: β = −0.011, p < 0.001). For patients with depression, the older patients initiated ([8]: β = −0.010, p < 0.001) and exchanged ([8]: β = −0.041, p < 0.001) secure messages significantly less than patients without depression.
The population in our dataset was 61.5% females. We found statistical significance with female patients in our overall sample population who initiated ([2]: β = 0.204, p < 0.001) and exchanged ([2]: β = 0.610, p < 0.001) secure messages. The results were consistent among female patients with depression who initiated ([9]: β = 0.147, p < 0.01) and exchanged ([9]: β = 0.628, p < 0.001) messages.
The population in our dataset was 72.4% White and 21% Black, which differed from AMC’s greater metropolitan area representation of 78.4% White and 11.8% Black. We speculate that we may have observed the digital divide phenomenon that disadvantaged the adoption and use of SM among Black adults. The URM in our sample population (i.e., Black adult patients) was significantly and negatively associated with SM initiations ([3]: β = −0.191, p < 0.001) and exchanges ([3]: β = −0.569, p < 0.001). The associations were also significant among URM patients who suffered from depression ([10]: β = −0.340, p < 0.001 and β = −0.884, p < 0.001).
Approximately half of our sample population was married. Our results showed significant and positive associations between married patients and SM initiations ([4]: β = 0.098, p < 0.001) and exchanges ([4]: β = 0.271, p < 0.001), suggesting they engaged in messaging activities to a greater extent than those who were not married. Our results also showed that married patients with depression actively sought medical advice ([11]: β = 0.180, p < 0.001) and continued their exchanges ([11]: β = 0.614, p < 0.001) compared with those without depression.
Approximately a quarter of our sample population was characterized as low-income patients. Low-income patients in our sample population were significantly and negatively associated with SM initiations ([5]: β = −0.234, p < 0.001) and exchanges ([5]: β = −0.661, p < 0.001). The relationships remained significant and negative among low-income patients with depression ([12]: β = −0.185, p < 0.001 and β = −0.384, p < 0.05) when compared with patients without depression.
Patients in our sample spent zero to 1,632 h annually using the patient portal, with an average of 3.86 h. The more time they spent using the patient portal, the more they engaged in SM initiations ([6]: β = 0.227, p < 0.001) and exchanges ([6]: β = 0.660, p < 0.001). However, when patients with depression spent more time using the patient portal, the less they initiated SM ([13]: β = −0.003, p < 0.05). Time spent using the patient portal did not affect SM exchanges ([13]: β = 0.006, n.s.).
Discussion
We examined patients with and without depression across 2,629 zip codes over five years. The random-effect baseline models indicate where patients live did influence their SM use. Zip codes are used in health research using publicly available data to characterize sociodemographics such as income, education, and accessibility to food, parks, employment, and the internet. Our results show that patients’ SM use did vary from year-to-year; however, the variance was significantly less when compared with zip codes. The widespread growth in SM use over the years examined in this study is evident; however, we speculate that the COVID-19 pandemic may have contributed to some of the variations observed in our study—an increase in 57% and 63% of SM initiations and exchanges, respectively, from 2019 to 2020 (see Fig. 1, Table 3). Overall, the results provide empirical support that variations in SM use were influenced by residence (zip code) and time (years).
We set out to examine whether those with mental health issues might be using SM more. We offer empirical support that patients with depression engaged in SM initiations and exchanges more than those without depression. Our findings demonstrate a consistent utilization pattern of SM that aligns with the advancements in the telehealth ecosystem, with depression health information requests expanding at a more rapid pace than other medical conditions. Should this pattern continue, health care teams can expect to encounter more secure messages from patients with depression in the coming years.
In our sample population, age did not play a role in initiating SM; however, older adults did significantly exchange fewer messages. One plausible explanation is that it is more difficult for older adults with declining vision and hearing to use the internet or mobile apps, thus hindering their enthusiasm to engage in SM initiations and exchanges. 20 For patients with depression, older adults initiated and exchanged messages significantly less compared with those without depression. This finding is consistent with a recent study suggesting that high utilization of communication technologies among older people with depression was associated with decreases in communication frequency. 21 It could also be that older people may have different depressive symptoms than younger people. Sadness may not be their main symptom; rather, they could be feeling numbness or a lack of interest in activities leading to less willingness to communicate their feelings. 22
Our results indicate that females engaged in SM use more than males. Males feel stigmatized and are far less likely to seek mental health treatment than women. 23 Research has shown that males who suffer from depression are at greater risk of harm, including suicide 24 and substance abuse, 25 yet our results show that males were not as actively engaged in self-care management. To combat this dilemma, telehealth can target males and “push” messages to improve communication, engagement, relationships, and health outcomes.
Demographics and race affected SM utilization among individuals with depression. In general, low-income patients did not engage in SM use relative to their counterparts. Prior literature suggests that key barriers among low-income patients such as low health literacy, complications with health insurance, a distrust of health care providers, and holding multiple jobs make it difficult to prioritize SM use and are associated with increased depression. 26 –29 URM patients also did not use SM relative to Whites. Although the digital gap regarding the use of patient portals is shrinking especially through mobile devices 15 and SM is one of the most frequently used features, our results suggest that mistrust among Blacks 30 and patient–physician racial concordance on clinical care 31 may be contributing to what we were observing. The effects were more pronounced among patients with depression. Married individuals with depression used SM significantly more. This is consistent with prior research that being married is associated with receiving treatment. 32
Technology also affected SM utilization among individuals with depression—the positive association between more time spent using the patient portal and SM use is consistent with prior literature. With SM being one of the most frequently used features in patient portals, there was more opportunity to engage in SM initiation and exchange activities. Probing deeper, our results revealed that patients with depression who spent more time using patient portals were initiating significantly less secure messages when compared with patients without depression. The cognitive model of depression suggests that patients suffering from depression may have developed self-referential schemas that influence information processing through negative biases 33 leading them to engage in questionable decision-making. 34 The perceived negative information about themselves in the patient portal and poor concentration that often accompany those with depression 35 combined with their information and decision-making processes may deter them from initiating secure messages. There was no significant difference concerning SM exchanges.
This study is not without limitations. First, we were limited in the data provided to us; our data were from a single-site health system using a binary classification of having been diagnosed with depression or not. Therefore, caution should be exercised when interpreting the results of our findings. Second, we aggregated and analyzed annual data. The granularity of monthly data has the potential to provide additional insights; however, we opted for a large sample in place of a significantly smaller sample due to missing data. Nevertheless, the breadth and depth of our longitudinal data provide a glimpse into the behaviors of our patient population, which we believe can generalize to other health systems and populations. Third, our data were limited to patients with portal access. The digital divide gap precluded the inclusion of patients who did not have portal access; consequently, our results may not adequately represent the socioeconomically disadvantaged and URM populations.
Conclusions
Our objective was to examine whether individuals with depression might be using SM more. The results of our study show that individuals with depression used SM telehealth services to a greater extent than those without depression and there were stronger associations with SM exchanges. Our findings also revealed that the predictors affecting SM use are multifaceted, with certain predictors enhancing its utilization and others impeding it. Additional research is needed to disentangle these complex relationships. Future research can examine the relationship between SM telehealth service usage and health outcomes or patient satisfaction. As communication technology and generative artificial intelligence advance, SM telehealth service can be a powerful asset to inform, educate, and engage with patients who have the greatest need—those suffering from depression and the broader mental health population.
Data Sharing
The proprietary nature of HIPAA data used in this study prevents data sharing.
Footnotes
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the AMC or the University of Cincinnati.
Authors’ Contributions
SAK made a substantial contribution to the conception of the study; she conducted a literature review; she performed data preprocessing and preliminary/descriptive statistical analysis instrumental in the selection of linear mixed-effects modeling technique; and she prepared the draft of the article and continued to make revisions. EJW made a substantial contribution to the interpretation and implications of findings; and he reviewed and guided the overall article critically. DPS made a substantial contribution to the interpretation of data analysis and results. DGK made a significant contribution to the conception and design of the study; he coordinated all aspects of research activities; he acquired the data; he performed the final statistical analysis; and he prepared the draft of the article and continued to make revisions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.