
Abstract
Introduction:
Despite advances in treatment of children with critical heart disease, cardiac arrest (CA) remains a common occurrence. We provided virtual support to bedside teams (BTs) from a tele-critical care (TCC) unit in a pediatric cardiac intensive care unit (CICU) and focused on early detection of concerning trends (CT) and avoidance of CA. Virtual surveillance workflows included a review of remote monitoring, video feed from patient room cameras, medical records, and artificial intelligence tools. We present our initial experience with a focus on critical communications (CCs) to BTs.
Methods:
A retrospective, descriptive review of TCC activities was conducted from January 2019 to December 2022, involving electronic databases and electronic medical records of patients in the CICU, including related CCs to BTs, responses from BTs, and related CA.
Results:
We conducted 18,171 TCC activities, including 2,678 non-CCs and 248 CCs. Over time, there was a significant increase in the proportion of CCs related with CT (p = 0.002), respiratory concerns (<0.001), and abnormalities in cardiac rhythm (p = 0.04). Among a sample of 244 CCs, subsequent interventions by BTs resulted in adjustment of medical treatment (127), respiratory support (68), surgery or intervention (19), cardiac rhythm control (17), imaging study (14), early resuscitation (9), and others (10).
Conclusions:
CCs from a TCC unit in a pediatric CICU changed over time with an increased focus on CT and resulted in early interventions, potentially contributing to avoiding CA. This model of care in pediatric cardiac critical care has the potential to improve patient safety.
Introduction
The potential occurrence of cardiac arrest remains an important concern in the critical care environment, including pediatric intensive care units (PICU) and pediatric cardiovascular intensive care units (CICU). 1 Even after the implementation of well-established quality and safety interventions and the use of traditional tools (such as incident reports, databases, chart review, regular or continuous monitoring, adjustments in personnel workflows, specialized personnel, and simulation training), as well as improvements in perioperative care, the prevalence of CA in children, after an initial increase in survival, has shown a relative lack of improvement in the past 10 years. 2 In hospitalized children with acquired and congenital heart disease, CA occurs at a rate of more than 10-fold than the one in children without cardiovascular disease, 3 with reported CA rates of 4.8 CA/1,000 CICU days and a corresponding hospital survival of 53.2%. 1,4 Hence, additional solutions are needed to decrease the occurrence of this serious complication.
Tele-critical care (TCC) has emerged as an additional tool during the past decades, leveraging clinical expertise, virtual technology, and artificial intelligence (AI) tools to support bedside teams in remote locations, and in adult patients, it has been associated with improved patient outcomes. 5,6 During the COVID-19 pandemic, it became an integral part of a national pandemic response with the development of the Tele-Critical Care Network (NETCCN). 7 In addition, the use of telemedicine in the pediatric critical care environment can improve resource utilization due to a decrease of transfer to PICUs in tertiary and quaternary care centers, allowing some patients to receive high-quality care near home. 8
Starting in 2019, we developed a TCC model aiming to provide an additional layer of safety over patient care by providing virtual support to bedside teams taking care of patients in our CICU. This model of care is focused on avoidance of cardiac arrest by early detection of abnormal trends and targeted communications with the clinical providers. We share here our experience from January 2019 to December 2022, with a focus on critical communications (CCs) with bedside teams.
Methods
DEVELOPMENT OF TELE-CRITICAL CARE OPERATIONS
Overall strategic goals for our TCC model are to provide an additional virtual layer of safety over patient care in support of bedside providers, aiming to minimize cardiac arrest, ensure clear and effective communication, support escalation of care when appropriate, and at the same time be minimally disruptive to the workflow of bedside teams.
In 2018, a physical space was identified and adapted in a provisional TCC unit and dry runs were conducted, with formal operations starting on January 2019. Our initial virtual surveillance workflows have been previously described 9 and were developed based on a continuous care model. 10 Briefly, they include a systematic review of remote monitors, video feed from patient room cameras (Ocularis VMS, Kintronics), a dashboard with an AI tool trained to detect low systemic venous oxygen saturation (Etiometry®, Inc., Boston, MA, USA), 11 a clinical critical care dashboard and an electronic medical record (EMR) (iAware®, Cerner®), as well as relevant imaging studies. At the end of this process, a decision was made on whether to communicate with bedside teams based on clinical analysis of the findings for each surveillance activity (Supplementary Fig. S1). Prioritization of virtual surveillance is based on patient acuity, alarms, and data from remote monitors and AI dashboards, as well as staffing considerations. Communications with the clinical providers were conducted by text or direct call using a Health Insurance Portability and Accountability Act (HIPAA) compliant app (Connect Messenger, Cerner®) and were categorized as non-CCs vs. CCs (Supplementary Table S1), providing the BTs with the reason for concern with relevant supporting information. Authority over patient care was always maintained by the bedside teams. Initial coverage included working hours during regular weekdays (7:00–17:00 h).
Our initial staffing consisted of one telemedicine fellow (replaced by a research faculty physician in 2020) conducting the virtual surveillance workflows and two CICU attendings. Two experienced CICU nurses were recruited in 2021, and a new TCC unit—embedded in our CICU—started operations in February 2022, with current staffing covering 54 h per week. A neurologist member of our neurocardiac critical care program and a noninvasive imaging cardiologist were incorporated to improve and expedite interdisciplinary communication. Finally, specific workflows for TCC nurses were developed, including specific communications and activities supporting bedside nurses, and are described in a separate report. 9
DATA COLLECTION
A waiver of consent was obtained from our IRB to conduct this study (IRB number: Pro00013086; approved: 01/09/2020). This is a descriptive review of EMR and an electronic TCC database (REDCap®), 12 from patients admitted to our CICU and supported with surveillance from our TCC unit between January 1, 2019, and December 31, 2022.
Patients with incomplete data or still in the hospital during data review were excluded from analysis. Collected information included age, gender, weight, primary cardiovascular and other diagnoses, index cardiovascular surgery, hospital survival, information related to virtual surveillance activities, concerns related to CC, and the response from the BTs. Additionally, the occurrence of cardiopulmonary arrest during the first 24 h after CCs was documented.
Depending on the interaction with the bedside teams, virtual surveillance activities were designated as remote monitoring, non-CCs, and CCs. Detailed information related to TCC nurse communications and activities with bedside nurses are described in a separate report. 9
Reasons for communications were divided into 13 categories (Supplementary Table S2), and responses from bedside teams were classified as in agreement, partial agreement, or different approach from suggested interventions. The presence of cardiac arrest during the 24 h following CC was verified in the patients’ EMR.
STATISTICAL ANALYSIS
Demographic and clinical characteristics of CICU patients supported by CCs and virtual surveillance activities were analyzed by descriptive statistics. Continuous variables are expressed as mean ± standard deviation or median and interquartile range as applicable. Categorical variables are reported as frequencies and percentages. All categorical variables were assessed by χ 2 or Fischer’s exact test as appropriate, while all the continuous variables were evaluated using t test or Kruskal–Wallis test as appropriate. The significance level for these analyses was set to α = 5%. All statistical analyses were done on the statistical analytical software (SAS).
Results
Between 2019 and 2022, we conducted a total of 18,171 virtual surveillance activities, and of these, 2,678 were associated with non-CCs, and there were 269 CCs during the care of 150 patients. After excluding 21 CCs with incomplete data, 248 CCs related to 145 patients were included for subsequent analysis (Fig. 1, Supplementary Table S3). Among the patients related with CCs, the more common cardiovascular diagnoses included hypoplastic left heart syndrome (n = 28, 19%), coarctation of the aorta or hypoplastic aortic arch (n = 17, 12%), and Tetralogy of Fallot with pulmonary atresia (n = 17, 12%), among others (Table 1), and most of them were in the postoperative period (n = 115, 79.3%). About one-half of the patients had STAT category ≥4. In addition, the most common surgical procedures included pulmonary artery bands (n = 16, 13.9%), Norwood operation (n = 15, 13.1%), and systemic to pulmonary shunt (n = 10, 8.6%) (Table 2).
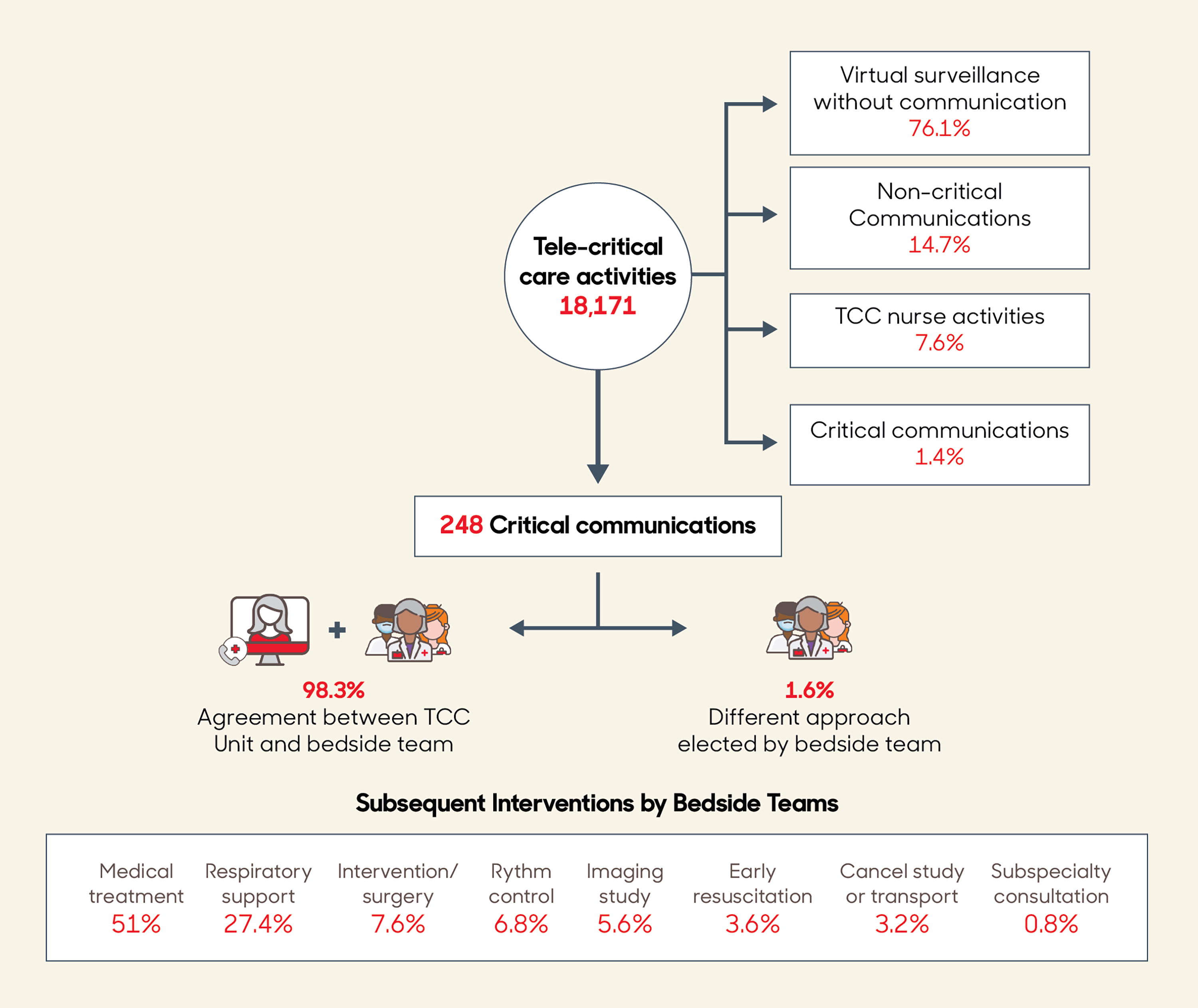
Virtual surveillance activities and interventions after critical communications.
Patients Related with Critical Communications, with Cardiovascular Diagnosis
HLHS, hypoplastic left heart syndrome; TGA, transposition of great arteries; Tetralogy of Fallot/pulmonary stenosis TOF/PA; VSD, ventricular septal defect; ASD, atrial septal defect; CoA, coarctation of the aorta; DILV, double inlet left ventricle; DORV, double outlet right ventricle; CAVC/AVSD, common atrioventricular canal/atrioventricular septal defect; HCM, hypertrophic cardiomyopathy; PV, pulmonary valve; DCM, dilated cardiomyopathy; AS, aortic stenosis; AR, aortic regurgitation; ALCAPA, anomalous left coronary from the pulmonary artery; IAA, interrupted aortic arch; TAPVC, total anomalous pulmonary venous connection.
Postoperative Patients Related with Critical Communications, with STAT Categories Procedures
PA, pulmonary artery; ASO, arterial switch operation; BDG, bidirectional Glenn; RV-PA, right ventricle to pulmonary artery; VSD, ventricular septal defect; CAVC, complete atrioventricular canal; MPA, main pulmonary artery; OHT, orthotopic heart transplantation; DORV, double outlet right ventricle; TOF, Tetralogy of Fallot; VAD, ventricular assist device; PAB, pulmonary artery band; STAT, The Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery; NA, not applicable.
CHANGES IN COMMUNICATION PATTERN OVER TIME
From 2019 to 2022, there was a threefold increase in CCs in the last year of study, and there was a significant decrease in the proportion of non-CCs. Virtual surveillance activities without communication with the bedside teams also showed a significant decline. Over the last two years, there was a significant increase in the proportion of TCC nursing activities (Fig. 2).
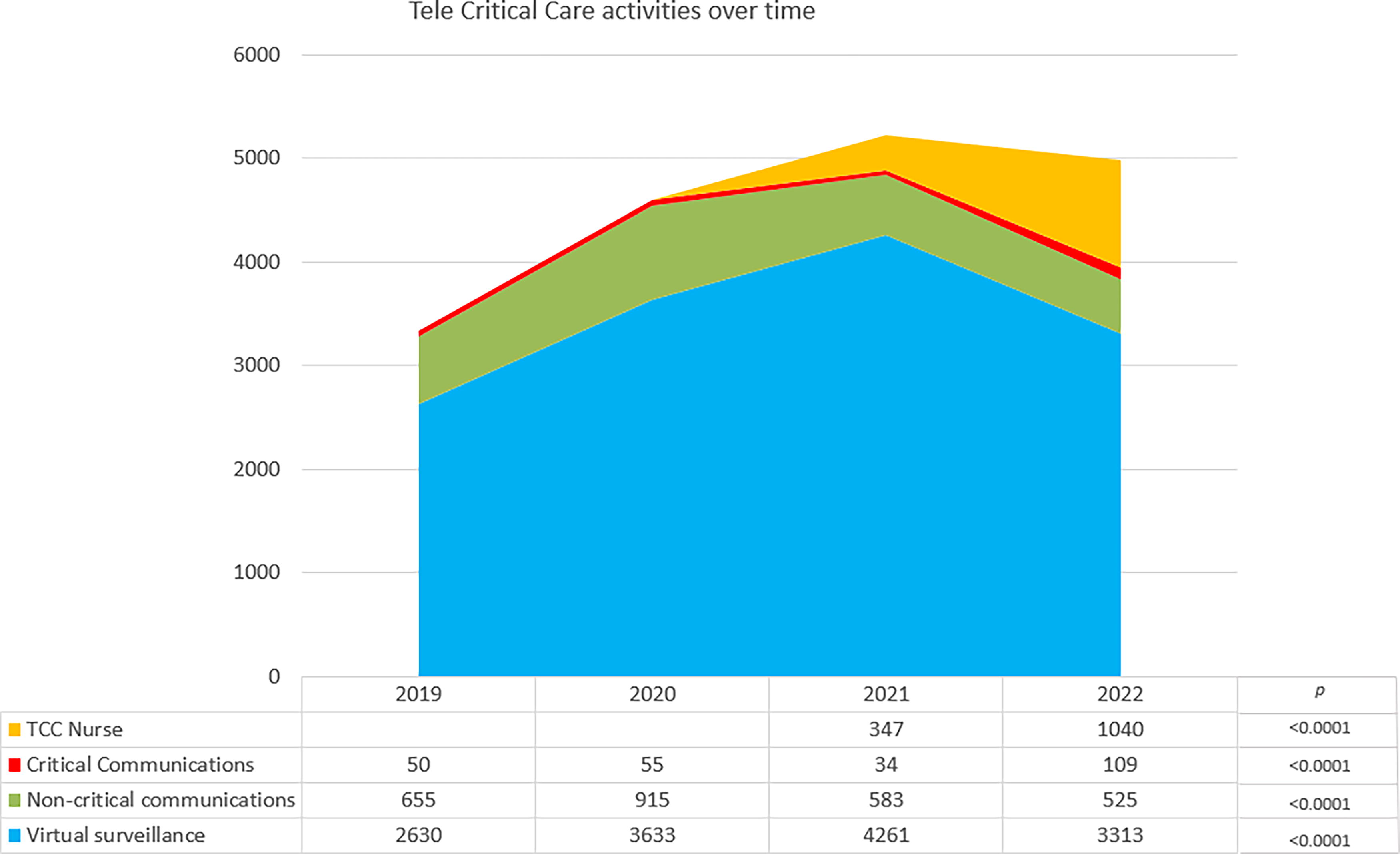
Trends in tele-critical care activities over time.
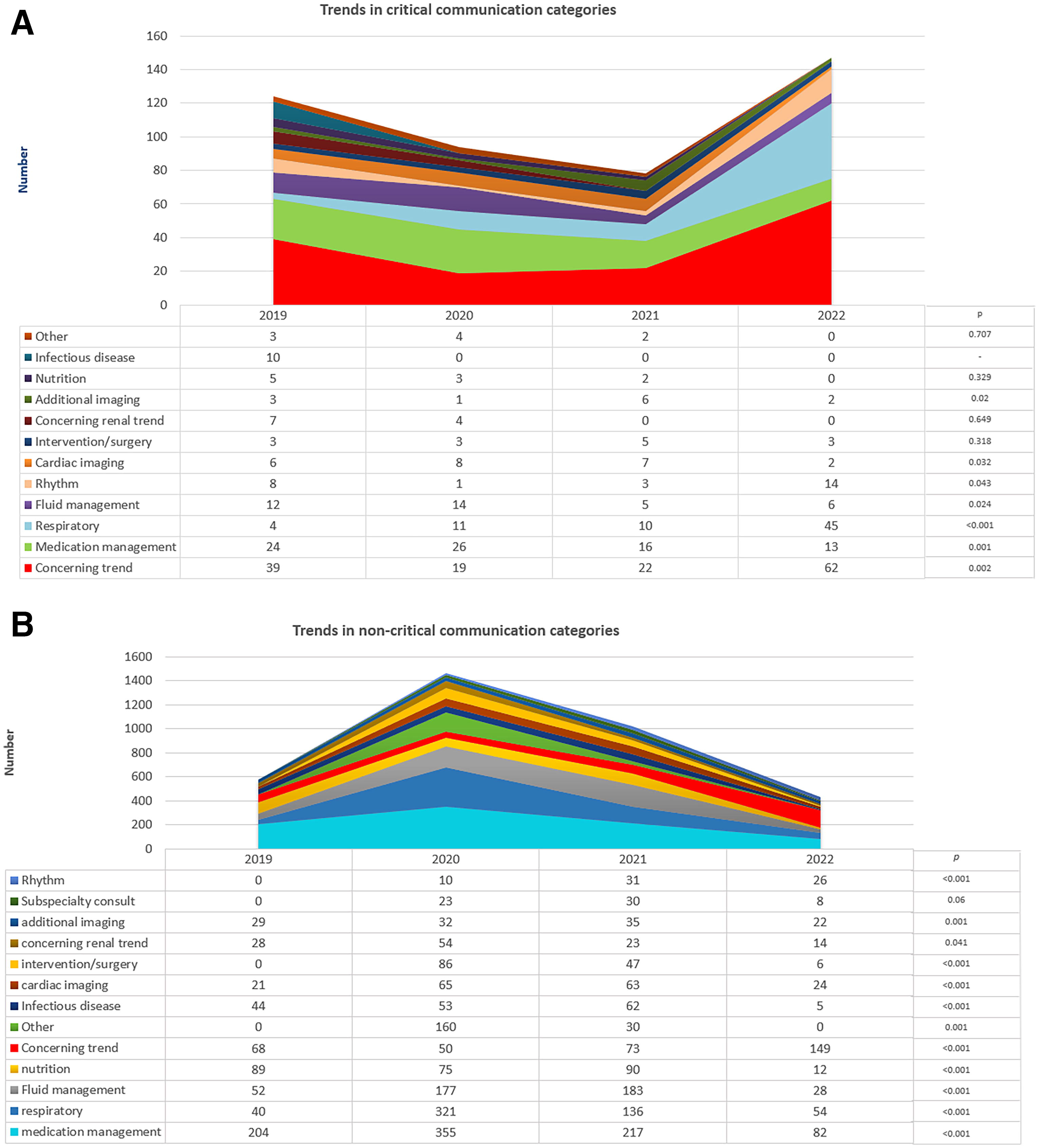
Comparing the distribution of communicated categories between CC and non-CC related with a concerning trend (CT), respiratory and rhythm concerns were more frequent in CCs. Conversely, non-CCs related with nutrition and other issues were more frequently communicated (Fig. 3, Supplementary Table S3). Interestingly, for CCs, over time there was a significant increase in the proportion of communications related with CTs, respiratory concerns, and abnormal cardiac rhythm, and a decrease in those related to cardiac imaging issues, medication, and fluid management, as well as additional imaging (Fig. 4A). For non-CCs, over time there was also an increase in the proportion of communications related to CTs and a decrease in those related to respiratory concerns, medication management, fluid management, nutrition, and other issues (Figure 4b).
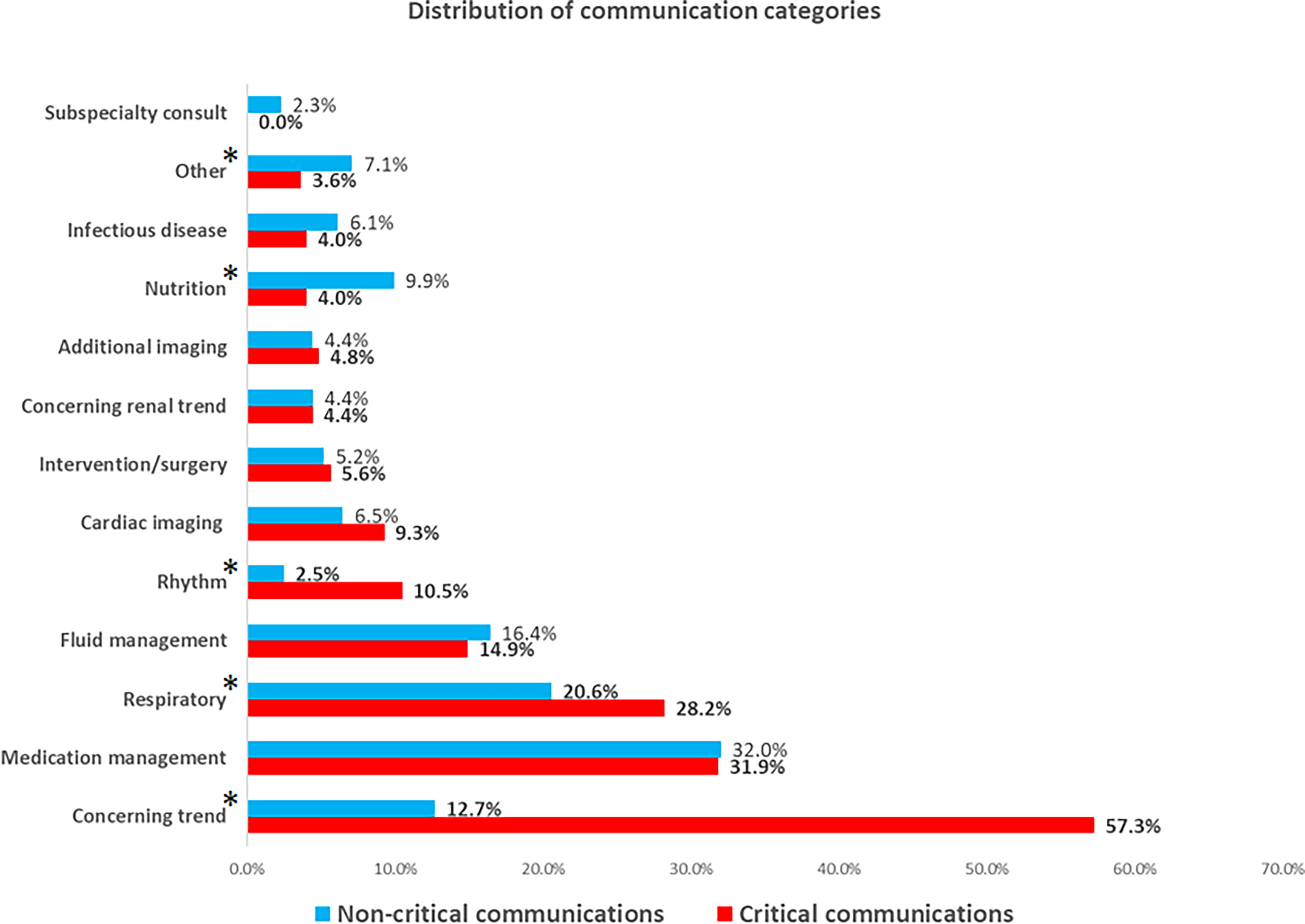
Distribution of communication categories, comparing critical vs. noncritical communications. *p < 0.05.
OUTCOME OF CRITICAL COMMUNICATIONS
In most CCs, there was agreement between the TCC unit staff and the clinical provider about the patient condition and potential response (244, 98.39%), and in four of them, the bedside team elected a different approach. After CCs, interventions by bedside teams resulted in adjustment of medical treatment (127, 51%) or respiratory support (68, 27.4%), additional surgery or intervention (19, 7.6%), and early resuscitation (9, 3.6%), among others (Fig. 1, Supplementary Table S4).
Four patients presented cardiac arrest within 24 h following a CC (range 2–92 min after CC) and in all of them, CC resulted in early resuscitation interventions, allowing for return of spontaneous circulation, earlier preparations for ECMO cannulation, or surgical intervention (Table 3). For patients related with CCs, hospital survival was 73.1% (Table 1).
Patients with Cardiac Arrest following Critical Communication
BAS, balloon atrial septostomy; BDG, bidirectional Glenn; CA, cardiac arrest; CC, critical communication; CoA, coarctation of the aorta; CPR, cardiopulmonary resuscitation; DKS, Damus–Kaye–Stansel procedure; Dx, diagnoses; ECMO, extracorporeal membrane oxygenator; E-CPR, ECMO cardiopulmonary resuscitation; GT, gastric tube; LCOS, low cardiac output syndrome; mBTTS, modified Blalock–Taussig–Thomas shunt; MPA, main pulmonary artery; NEC, necrotizing enterocolitis; PAB, pulmonary artery banding; TCC, Tele-critical care nurse; TGA, transposition of great arteries; TV, tricuspid valve; ROSC, return of spontaneous circulation; VSD, ventricular septal defect.
Discussion
Our findings show that the use of virtual surveillance of multiple clinical data points from children with critical heart disease, assisted with AI tools, can find and communicate valuable information that otherwise may have been missed by the bedside teams. Among the CC categories, the most common communications were related to a CT, medication management issues, a need for increased respiratory support, cardiac rhythm, and fluid management. This distribution seems appropriate for unstable clinical conditions requiring a rapid clinical response. These communications led to numerous interventions from the clinical providers, and these resulted in the avoidance of cardiac arrest or an earlier resuscitation. At the same time, we aimed to be the least disruptive to our bedside providers, as demonstrated by 76.1% of all our virtual surveillance activities with no communication with bedside teams. Over time, there have been numerous iterations of virtual surveillance and communication workflows aimed to improving the detection of potentially CTs and ensure closed-loop communication and buying-in by bedside teams. Additionally, there were significant changes in communication patterns across time that warrant further analysis. We speculate that they may be related with a number of contributing factors like the mentioned changes in workflows as part of our learning process, as well as adaptation to pandemic and postpandemic environments, resulting in an increased focus in communications related with CTs (a threefold increase during the last year), and a decrease in the proportion of those related with less acute medical management issues that may be perceived as “virtual micromanaging” by the bedside providers.
Several features of our TCC model are worth mentioning. First, even when a TCC model is common in the adult setting with up to 28% of ICU beds in the USA covered by a tele-ICU service, 13 to the best of our knowledge, this is the first report of a TCC with a continuous care model in support of a pediatric CICU to prevent cardiac arrest in children with critical heart disease. Recently, Berrens et al. reported the implementation of a telemedicine system with rapid-response and code-response teams at a satellite facility supported via telemedicine by a pediatric intensivist, 14 but most reports in children have described a consultative model with physician-to-physician communication to rural and isolated populations, 8 or in the international setting. 15,16
LIMITATIONS
While this is an encouraging initial experience, there are important limitations pointing toward the need for further work to bring this model to its full potential. The retrospective and descriptive nature of this report precludes us from establishing a relationship between our communications and patient outcomes. Also, we have not yet established 24/7 operations, and consequently, uncovered times may impair any sustained protective effect. We plan to expand our TCC coverage during night shifts, where this model of care has been reported to be more effective. 17 Additionally, we are unable to fully differentiate the proportion of communications where the bedside teams received additional and new information from those in which they were already aware about the communicated data. We specifically chose not to track this information to optimize the perception and acceptance of our service by the bedside providers. Four patients presented CA shortly after a CC, and this finding points toward the need to improve our virtual surveillance workflows and our AI tools to allow for earlier detection, communication, and intervention. Response from bedside teams to non-CCs is not available, and we are unable to establish their impact on interventions by the clinical providers. Finally, our workflows still rely on clinical judgment and memory to conduct virtual surveillance, and the final decision to communicate depends on the personal assessment of a physician or nurse at the TCC unit. Virtual surveillance and communications prompted by automated triggers, assisted with additional AI tools may allow for earlier detection and more efficient interventions.
CONCLUSION
A TCC unit within a pediatric CICU detected clinically relevant information, resulting in communications with bedside teams and numerous interventions that may have prevented or decreased cardiac arrest. Over time, CC patterns changed with an increased focus on CTs, respiratory concerns, and abnormalities in cardiac rhythm. Further refinements of this model of care in staffing, financial model, and virtual surveillance and communication workflows are needed to establish the most effective virtual interventions to prevent cardiac arrest, improve survival and quality of life of patients, and improve satisfaction, resilience, and collaboration with BTs.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
Funding for our BOV Telehealth Command Center was awarded by the Founders Auxiliary Board (formerly Board of Visitors) at Children's National Hospital.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.