
Abstract
Background:
Mobile health (mHealth) has an emerging potential for remote assessment of traumatic dental injuries (TDI) and support of emergency care. This study aimed to determine the diagnostic accuracy of TDI detection from smartphone-acquired photographs.
Methods:
The upper and lower anterior teeth of 153 individuals aged ≥ 6 years were photographed using a smartphone camera app. The photos of 148 eligible participants were reviewed independently by a dental specialist, two general dentists, and two dental therapists, using predetermined TDI classification and criteria. The sensitivity, specificity, accuracy, positive predictive value, negative predictive value, and inter-rater reliability were estimated to evaluate the diagnostic performance of the photographic method relative to the reference standard established by the dental specialist.
Results:
Of the 1,870 teeth screened, one-third showed TDI; and one-seventh of the participants had primary or mixed dentitions. Compared between the specialist’s reference standard and four dental professionals’ reviews, the diagnostic sensitivity and specificity for TDI versus non-TDI were 59–95% and 47–93%, respectively, with better performance for urgent types of TDI (78–89% and 99–100%, separately). The diagnostic consistency was also better for the primary/mixed dentitions than the permanent dentition.
Conclusion:
This study suggested a valid mHealth practice for remote assessment of TDI. A better diagnostic performance in the detection of urgent types of TDI and examination of the primary/mixed dentition was also reported. Future directions include professional development activities involving dental photography and photographic assessment, incorporation of a machine learning technology to aid photographic reviews, and randomized controlled trials in multiple clinical settings.
Introduction
Traumatic dental injuries (TDI) refer to sudden injuries to the dentition and supporting structures. TDI can lead to damage of the tooth structure, dental pulp, and periodontal tissues, and result in pain, tooth loss, and/or eruption disturbances. The prevalence of TDI remains high during childhood and adolescence, and global data show that approximately one-third of adults have sustained TDI to permanent teeth. 1 Although treatments for TDI are available, they are costly and require multiple visits 2,3 ; and untreated TDI can impact sleep, emotional well-being, and social interaction. 4
Many TDI cases occur outside of dental clinic office hours, 5,6 and many patients seek initial treatment at medical emergency departments that are not equipped and staffed to manage dental emergencies. 7 In addition, emergency physicians can provide symptomatic relief but may not necessarily be able to address the underlying cause. During the COVID-19 pandemic, emergency departments experienced a surge in patients, and consequently, many dental emergencies were left untreated or referred. 8 Moreover, inequity in access to dental care has become a driver of people using emergency departments to treat nonacute dental problems. 9 This further compromised their management capacity for TDI and other emergencies. Delays in adequate management can lead to worse outcomes; therefore, TDI must be managed within the first few hours of presentation 5 by competent dental professionals, 10 preferably in collaboration with a multidisciplinary team. 11 Teledentistry has been recognized as an approach to ensure timely care for TDI, where the visual clinical examination is of the essence. 7 Being a modality of teledentistry 12 and having a function of photography, the practice of mobile health (mHealth) could address the limitations of the traditional model of dental care.
The World Health Organization has defined mHealth as “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants, and other wireless devices.” 13 Recent generations of smartphone cameras permit the acquisition of high-resolution color photos. Submitting these images appended with patients’ symptoms to a dental practitioner could improve patient–provider communication in real time and facilitate patient-centered care. A previous study has validated the photographic detection of TDI from images captured with professional digital cameras. 14 A recent study has also shown the potential for the use of a specially developed mobile app on photographic identification of TDI in three simulated cases. 15 Moreover, an earlier article has reported the usability of images captured with a smartphone camera for TDI diagnosis, without involving a medical/dental app. 16 To the best of our knowledge, there has been a paucity of data on the use of mHealth technologies for remote evaluation of TDI.
Our previous research on the photographic assessment of dental caries by dental professionals has demonstrated that the mHealth model could offer practical and economical means for remote dental screening. 17,18 The application of a similar mHealth approach to oral cancer detection has also shown promising feasibility. 19 With the convenience of image acquisition and store-and-forward technologies, mHealth is becoming a relevant solution to assess oral conditions remotely and asynchronously. Having a purpose to facilitate remote assessments of patients with TDI and support emergency care with mHealth, this study aimed to determine the validity and reliability of photographic assessment of TDI by general dentists and dental therapists relative to the reference standard established by a dental specialist.
Methods
STUDY SETTING
This study adheres to the Standards for Reporting Diagnostic Accuracy Studies (STARD) 2015 guidelines. 20 Ethics approval was obtained from the Institutional Review Boards of the University of Minnesota (Study ID: STUDY00014736) and Khon Kaen University (Reference Number: HE651242). This cross-sectional study was conducted from August 2022 to July 2023 at multiple sites located in Minnesota (USA) and Khon Kaen (Thailand), including the University of Minnesota clinical site, Khon Kaen University clinical site, and Minnesota State Fair research facilities. A multicenter approach allowed the inclusion of dental images captured from various ethnicity backgrounds, with a potential to improve the diversity of the participant pool and minimize the impact from lower participation rates of ethnicity minority groups.
APP AND DATA MANAGEMENT SYSTEM
The data were collected using the mHealth system, as described previously, which has been tested and validated. 17,18 It had two components: (1) an image acquisition app “Teledental” (CSIRO, Canberra, Australia) to enter patient information and dental photos, and then to transfer the data to a password-protected server and (2) a web-based data management system “Remote-I” (CSIRO, Canberra, Australia), which allowed offsite dental professionals to review photos, chart dental findings, and submit recommendations (Fig. 1).

The mobile health (m-health) flowchart for remote assessment of traumatic dental injuries (TDI): people use a smartphone app and camera to enter patient information and dental photos, and then transfer the data to a secured cloud storage; dental professionals review the photos, chart dental findings, and provide recommendations through a reverse route.
PARTICIPANTS AND PHOTO CAPTURES
The dental photographers recruited for this study consisted of six dentists, a dental therapist, and four students from the University of Minnesota and Khon Kaen University. Each received a Samsung Galaxy S20 FE 5G Android smartphone (equipped with the “Teledental” app), which has a primary 12 MP wide-angle rear camera with a dual pixel autofocus feature and an f/1.8 aperture lens. 21 Before collecting data, dental photographers completed online training for image acquisition (PowerPoint presentation through Zoom meetings) and in-person calibration (through mutual photo-capture and immediate feedback).
Participants were enrolled through convenience sampling. At clinical facilities, participants were approached by the dental photographers when suspected TDI cases were seen or reported. At the State Fair research facilities, researchers carried a poster showing TDI photos and recruited participants (fairgoers) by asking them whether they had ever experienced injuries to their teeth. Only individuals aged ≥ 6 years and able to provide written informed consent, parental permission, and/or child assent were included in this study. To allow multiperspective photographic assessment, 22 three photos of the participant’s teeth were acquired, including frontal, upper occlusal, and lower occlusal views (Fig. 2). The images were taken using the preassigned smartphone under natural light (with the LED flashlight on) while the participant was seated on a chair, with the photographer standing in front of the participant. The captured images were transmitted by the “Teledental” app through a secured wireless network to a password-protected server and stored for later evaluation by reviewers.

Dental photos taken from a participant who consented to have their images presented in the publication:
IMAGE REVIEW
Dental photos were screened for diagnostic quality by the research team and then reviewed independently by five active USA-licensed dental professionals, including a dental specialist (an expert in pediatric dentistry and dental traumatology), two general dentists, and two dental therapists. They used the “Remote-I” system on their computers to access the images stockpiled in a secured cloud storage. The reviewers were trained and calibrated together by the research team to diagnose TDI from the photos stored in the cloud server, without access to dental history, injury cause, clinical examination data, and radiographs.
Before the COVID-19 pandemic, visual clinical examination was often used as the gold standard 14,16 –19 ; in this study, the dental specialist’s photographic review was used as the reference standard to evaluate the diagnostic accuracy of image assessments by four other dental professionals. Our rationale was to avoid inconsistency of clinical examinations among multiple sites and prevent the spread of COVID-19. Dental photos were reviewed for the type and tooth position of TDI. Only incisors and canines of both arches were assessed from the photos. The TDI types and criteria for their occurrence included uncomplicated and complicated crown fractures, intrinsic tooth discoloration, luxation, and avulsion. 23,24 Sound, missing, and partially erupted teeth were also recorded in the review process. Based on the TDI diagnoses made by the reviewers, three urgency levels for the care were generated, including urgent (complicated crown fractures, luxation, or avulsion), nonurgent (uncomplicated crown fractures or intrinsic tooth discoloration), and nontraumatic (sound, missing, or partially erupted teeth). 1 The urgency levels indicated different needs for emergency support because the treatments required are quite different. 23 For instance, a nonurgent uncomplicated crown fracture can be treated with edge-smoothing, fragment reattachment, or a simple resin restoration at a later time, whereas an urgent complicated crown fracture generally needs immediate and invasive pulp therapy. 23
DATA ANALYSIS
For an expected TDI prevalence of 30%, 3 a sample size of 91 participants would give an 80% power with a 5% type I error rate. Considering a 60% dropout rate, 146 participants from all sites were deemed sufficient. Data entry and statistical analyses were carried out with the IBM SPSS Statistics 29 (IBM, Chicago, IL, USA). Incomplete and missing data were excluded from analysis. The sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV), inter-rater reliability kappa value, and intrarater reliability kappa value of TDI diagnoses (using this mHealth model) were calculated on a tooth-by-tooth basis. To estimate the intrarater reliability, 20% of the records were selected, renamed, and randomly ordered by the research team, and reassessed by the five reviewers separately at least a week after completing the initial review. The strength of inter-rater and intrarater reliability was classified as described by Landis and Koch. 25 In addition, a 2 × 2 crosstab was created to separate the teeth based on the dentition (primary/mixed or permanent) and the consistency between each reviewer’s diagnoses and the dental specialist’s (consistent or inconsistent). A Pearson chi-square test was used to examine the differences in diagnostic consistency between the primary/mixed dentition and permanent dentition. The level of statistical significance was set at 5%.
Results
From 153 individuals who consented to participate, five were excluded because of incomplete photo captures. No adverse event was identified or reported. The final sample for remote assessment comprised 1,870 teeth of 148 individuals (Fig. 3), including 113 from Minnesota State Fair (USA), six from University of Minnesota clinical site (USA), and 29 from Khon Kaen University clinical site (Thailand). Sixty-seven (45.3%), 77 (52.0%), and 4 (2.7%) participants identified themselves as female, male, and other genders, respectively. Their age ranged from 6 to 76 years. Twenty-one (14.2%) participants were in the primary/mixed dentition.
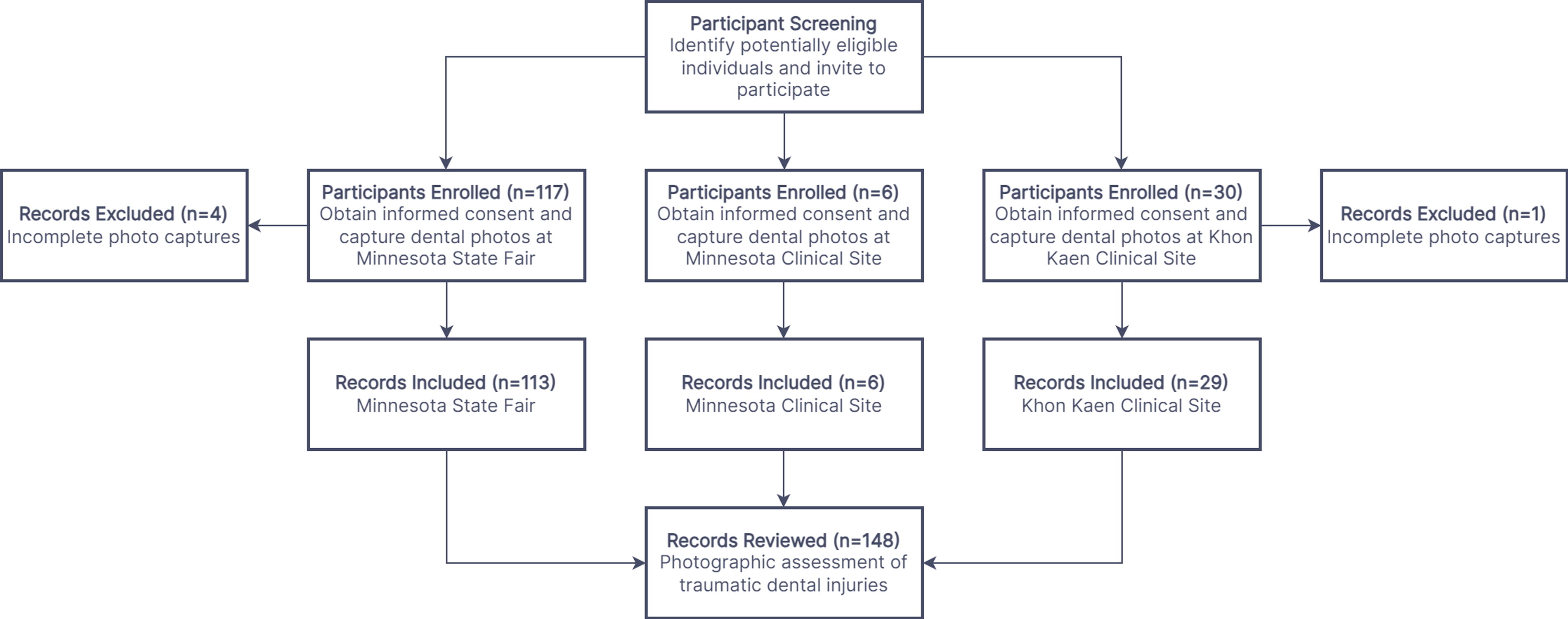
Flow diagram of the study participants.
Based on the dental specialist’s diagnoses, the tooth-by-tooth prevalence of TDI was 32.7% (95% confidence interval [CI]: 30.6–34.9%), and 109 participants (73.6%) had at least a tooth sustaining TDI. The teeth sustaining urgent TDI such as complicated crown fractures or avulsion represented 1.5% of all traumatized teeth. Table 1 presents the frequency distribution of TDI diagnoses.
Frequency Distribution of Traumatic Dental Injuries (n = 1,870)
Table 2 presents a cross tabulation of the reviewers’ results for differentiating TDI from nontrauma. When urgent and nonurgent TDI cases were pooled together, the diagnostic sensitivity of the mHealth model from the two general dentists and two dental therapists was 58.8% (95% CI: 54.8–62.8%) to 95.1% (95% CI: 93.1–96.7%). Their specificity varied from 46.9% (95% CI: 44.1–49.7%) to 93.0% (95% CI: 91.4–94.3%), and the accuracy varied between 62.7% (95% CI: 60.5–64.9%) and 81.8% (95% CI: 79.9–83.5%). The kappa values for inter-rater reliability ranged from 0.33 (95% CI: 0.30–0.36%) to 0.57 (95% CI: 0.53–0.61%), indicating a fair to moderate agreement. The intrarater reliability was moderate to substantial, with the kappa values ranging from 0.55 to 0.79.
Cross Tabulation of Traumatic Dental Injuries Diagnoses by the Four Reviewers versus the Dental Specialist
7 Teeth not rated by general dentist 1.
7 Teeth not rated by dental therapist 1.
4 Teeth not rated by dental therapist 2.
The chi-square test indicated that all the four reviewers’ diagnoses, regardless of the teeth with or without TDI, were more consistent with the reference standard when the dental photos contained a primary/mixed dentition (general dentist 1: p < 0.001, χ2 = 19.75, df = 1; general dentist 2: p < 0.001, χ2 = 39.93, df = 1; dental therapist 1: p < 0.001, χ2=48.94, df = 1; and dental therapist 2: p < 0.001, χ2 = 28.27, df = 1).
In addition, the diagnostic performance of the mHealth model in detecting urgent types of TDI showed sensitivity from 77.8% to 88.9% and specificity from 99.0% to 100.0%. The accuracy rate ranged between 98.9% and 100.0%. The kappa values for inter-rater reliability between the reviewers ranged from 0.44 to 0.94, indicating a moderate to almost perfect agreement. The intrarater reliability was estimated as substantial to almost perfect agreement, with the kappa values varying from 0.77 to 1.00. Table 3 presents the diagnostic performance of the mHealth model for differentiating urgent TDI from nontrauma and nonurgent TDI.
Diagnostic Performance of Urgent Traumatic Dental Injuries Using Photographic Assessments against the Reference Standard (Values within the Parentheses: 95% Confidence Intervals)
PPV, positive predictive value; NPV, negative predictive value.
Discussion
This study presents a valid mHealth model for remote assessment of TDI, demonstrating a moderate-to-high sensitivity and specificity. Our findings suggested that the diagnostic performance of TDI examination using a photographic method is acceptable. In the absence of dental history, injury cause, and clinical examination data, dental professionals could identify TDI manifestations, including uncomplicated and complicated crown fractures, intrinsic tooth discoloration, and avulsion, simply based on dental photos captured through the smartphone camera and app.
The practicability for photographic assessment of TDI demonstrated in this study was in agreement with previous articles. 14 –16 Compared to those studies, 14 –16 the strengths of our work are as follows: (i) the use of a store-and-forward technology composed of a smartphone app and a web-based data management system and (ii) the use of a larger sample size, including 148 participants and 1,870 teeth. On a more practical side, assessing and supporting TDI cases through teledentistry services are becoming common practice. The majority of teledental consultations provided by a Swiss telemedical center to TDI patients took place after dental clinic office hours. 6 A hospital in the United States has also reported that half of their teledentistry encounters were TDI related, even though TDI cases weighed only 5% of the total visits to the emergency department. 26 The disproportional use of teledentistry services for TDI disclosed the need for remote assessment and support to manage those cases. Being an easy-to-use modality of teledentistry 12 and having an acceptable diagnostic performance, mHealth can be incorporated in the remote management plan of trauma and emergency care.
Our sensitivity, specificity, accuracy, PPV, NPV, and inter-rater reliability for the detection of urgent TDI were better than those for the overall TDI. This indicates the usability of the mHealth model for individuals, such as emergency physicians, 27 school teachers, 28 athletic coaches, 29 and parents, 29 who often encounter urgent TDI cases, but are not fully trained to manage them. Their limited awareness, knowledge, and confidence can benefit from the remote support provided by dental professionals.
Two reviewers in this study were dental therapists, whose scope of practice included selected TDI management procedures such as pulp vitality testing, tooth restoration, tooth reimplantation and stabilization, pulp capping and pulpotomy, and extraction of primary teeth. 30 Although the dental therapist has a smaller scope of practice than the general dentist, 31 this did not limit their ability to assess and treatment-plan TDI cases. Our data confirmed that the diagnostic performance of the dental therapists was comparable to that of general dentists.
Our data showed a better diagnostic performance of the mHealth practice when assessing the primary/mixed dentition than the permanent dentition. This is in agreement with previous studies reporting a better diagnostic accuracy of photographic assessment when examining dental caries in primary teeth 32 or younger children. 17,33 Although AlShaya et al. implied that a larger number of primary teeth in their sample was a potential reason for a greater reliability observed 32 ; this reason is not applicable to our sample comprising six times more adults than children. Lower sensitivity and reliability of caries detection due to the morphological complexity of posterior permanent teeth have also been suggested by previous studies. 17,33 This is also not applicable to our study, which was limited to the assessment of anterior teeth only. Our observation of improved TDI assessment in primary/mixed dentitions is likely to have arisen from the diagnostic uncertainty between uncomplicated crown fracture and tooth wear (abrasion, attrition, and/or erosion) 34 on photographs. With the increasing prevalence of tooth wear among adults than in children, 35 a greater proportion of tooth wear in the permanent dentition could be possibly misidentified as uncomplicated crown fracture. As uncomplicated crown fracture and tooth wear do not require emergency care, the consequence of providing similar remote support to either condition is not alarming. Both conditions can be addressed when patients are referred for routine dental care.
The dominance of nonurgent and nontraumatic participants in the sample was a limitation of this study. Participant recruitment at the Minnesota State Fair was efficient and yielded valid data from 113 participants within a relatively short period of time. It is obvious that the majority of those fairgoers did not have urgent or severe TDI, or they would not have appeared at the joyful and exciting outdoor event. Although our clinical sites also recruited some participants showing urgent and severe TDI, the smaller number of urgent TDI led to wide variations (95% CIs) in some diagnostic performance parameters displayed in Table 3. Moreover, unavailability of clinical and radiographical data limited the reviewers’ ability to identify additional types of TDI, including root fractures, alveolar fractures, subluxation, and concussion. Their clinical competence for differential diagnosis of some oral conditions, such as tooth wear and uncomplicated crown fracture, was also compromised. More importantly, we relied on the dental specialist’s review as the reference standard and could not confirm the diagnosis on site.
Hence, data reported in this study should be interpreted with some caution.
Although all reviewers in this study were trained and calibrated before photographic assessment, the training focused on the charting operation of “Remote-I” and use of the TDI classification system. Thus, a detailed training session demonstrating the steps of photographic examination and diagnosis for each TDI type is indicated in future research. Moreover, our previous article has pointed out the relevance of image quality on diagnostic accuracy, 18 which was echoed by another study. 32 As training on dental photo acquisition could be a stronger determinant of image quality than the type of smartphone used, 36 additional photography training could enhance diagnostic performance. 33 To further improve the diagnostic performance of the mHealth model presented, these future directions are indicated: (1) professional development programs on dental photography and photographic assessment, (2) incorporation of a machine learning technology to aid in photographic review, and (3) randomized controlled trials at multiple clinical settings. Moreover, implementation of this mHealth model for remote assessment of other oral conditions should be fully explored, particularly in disadvantaged and vulnerable populations, as it holds promise to reduce oral health inequity.
Conclusions
This study suggests mHealth as a valid practice for remote assessment of TDI. The diagnostic performance of photographic assessment was acceptable, particularly appropriate for detection of urgent types of TDI. We also revealed a better diagnostic performance of the mHealth model in examining primary/mixed dentitions. To enhance the emergency support for TDI-related incidents, future research and professional development programs are required. Adequate training in dental photography and photographic assessment is also critical for successful implementation of mHealth in dentistry.
Footnotes
Acknowledgments
The authors acknowledge Minnesota Masonic Charities, International Association for Dental Research (IADR), the University of Minnesota Center for Global Health and Social Responsibility, and the University of Minnesota School of Dentistry for funding support. This study is also indebted to Dr. Sheila Riggs, Dr. Waranuch Pitiphat, and Mr. Janardhan Vignarajan for their support. Finally, we thank the participants, dental photographers, dental reviewers, and university staff who made this possible through their involvement. Part of this work was presented at the 101th General Session and Exhibition of the IADR (June 21–24, 2023; Bogotá, Colombia). Before the peer review and revision process, a draft of this article was available online as a preprint at ![]() .
.
Authors’ Contributions
Conceptualization and study design: B.H., M.E., P.P., K.Q., and S.R. Project administration: B.H., M.E., P.P., K.Q., S.R., and E.F. Data collection: B.H., P.P., A.A., J.W., F.D., M.S., D.S., and J.P.L. Data auditing: B.H., M.E., and E.F. Data analysis: B.H. and M.E. Resources: B.H., P.P., and J.P.L. Team lead and writing: B.H. All authors revised and approved the final article.
Disclaimer
The funders had no role in the conceptualization, study design, data collection, data analysis, and decision to submit results.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This study was supported with (1) a