
Abstract
Objective:
To compare telemedicine versus office visit use at two Medicaid-focused pediatric primary care clinics.
Methods:
Retrospective cohort study from March 15, 2020 - March 15, 2021 at two Medicaid-focused pediatric primary care clinics. Site A and Site B care for different populations (Site B care for mostly immigrant families with preferred language Spanish). Outcomes included the percent of visits conducted through telemedicine and reason for visit. Descriptive statistics, univariable and multivariable mixed multilevel logistic regression, were used to assess relationship between patient demographics and telemedicine use.
Results:
Out of 17,142 total visits, 13% of encounters at Site A (n = 987) and 25% of encounters at Site B (n = 2,421) were conducted using telemedicine. Around 13.8% of well-child care (n = 1,515/10,997), 36.2% of mental health care (n = 572/1,581), and 25.0% of acute care/follow-up (n = 1,893/7,562) were telemedicine visits. After adjustment for covariates, there was no difference in odds of a patient having any telemedicine use by preferred language, sex, or payor. Patients 1–4 years of age had the lowest odds of telemedicine use. At Site A, patients who identified as Non-Hispanic Black (odds ratio [OR] = 0.33, 95% confidence interval [CI] = 0.24–0.45), Hispanic/Latinx (OR = 0.40, 95% CI = 0.24–0.66), or other race/ethnicity (OR = 0.35, 95% CI = 0.23–0.55) had lower odds of telemedicine use in comparison to Non-Hispanic White.
Conclusions:
Telemedicine was successfully accessed by Medicaid enrollees for different types of pediatric primary care. There was no difference in telemedicine use by preferred language and payor. However, differences existed by age at both sites and by race/ethnicity at one site. Future research should explore operational factors that improve telemedicine access for marginalized groups.
Introduction
Medicaid-enrolled children, comprising approximately half of the nation’s pediatric population, 1 have been shown to have decreased access to primary care and preventative services. 2 These families experience significant barriers to care, including limited transportation and access to child care. 3 Specifically for Medicaid-enrolled children, telemedicine has significant potential to improve access to pediatric care, as recognized by the American Academy of Pediatrics (AAP). 4 This population can benefit from the increased convenience of telemedicine, but may also face barriers to accessing digital technologies. Understanding telemedicine utilization specifically for Medicaid-enrolled populations is important to ensure equitable telemedicine implementation.
Before the pandemic, pediatric telemedicine was shown to be feasible in specific settings, including specialty care, 3,5 –8 mental health care, 9 acute-care visits at day care centers, 10 pretransport assessment and stabilization of critically ill children at community hospitals, 11 remote monitoring of patients in their homes, school-based health, 12 –14 and rural pediatric populations. 8,15,16 Logistical and regulatory barriers prevented broad adoption, especially among Medicaid enrollees, and pediatric telemedicine programs were primarily funded by institutional direct investments and/or grants. 5 Medicaid reimbursement for most states was limited to synchronous video telemedicine to patients located at specific health sites only, such as school and school-based health centers, local health departments, federally qualified health centers, private practices, and hospital facilities. Few states had coverage for telemedicine visits for patients when they were located at home. 17
With the COVID-19 pandemic, drastic changes in policy, regulation, and reimbursement supported telemedicine use in pediatric primary care where Medicaid enrollees could complete visits from home.
In line with recent AAP guidance, 4 it is important then to understand telemedicine use patterns and evaluate for disparities in access to care in pediatric primary care to guide future policy and reimbursement strategies.
Literature since the COVID-19 pandemic have demonstrated disparities in pediatric telemedicine access, primarily in subspecialty settings, 3,15,18 –22 and limited evidence has been generated in pediatric primary care settings. Early studies in pediatric primary care 23 –28 have shown that Latinx patients, those requiring interpreter services, and those with reduced broadband and public insurance were less likely to complete telemedicine visits for subspecialty use, in comparison to those who are non-Hispanic/Latinx, English-speaking, and with high income and access to broadband and private insurance, respectively.
The few studies that have examined telemedicine use among pediatric patients who are predominantly Medicaid enrolled mirror the disparities previously mentioned, but have a few key limitations. Primarily, most of these studies had limited proportion of patients with preferred language other than English (PLOE). As families with PLOE represent a growing proportion of the United States (U.S.) population and historically face more challenges in access to care compared to those speaking English, it is imperative that telehealth use among this population is studied more closely to prevent exacerbating these disparities. 29 In addition, studies focused on Medicaid enrollees (1) were conducted for short periods early in the volatile phases of the pandemic, (2) emphasize on Medicaid claims data, 30,31 which may not provide adequate operational and clinical context behind the disparities, or (3) varied in degrees to which well-child and mental health care was conducted using telemedicine, in addition to acute care visits. Our institution offered a unique way to evaluate telemedicine use patterns because we have two Medicaid-focused clinics, but the populations served by these clinics differ by race/ethnicity and preferred language: one site serves predominantly non-Hispanic/Latinx Black patients, whereas the other serves predominantly Latino children of immigrant parents with Spanish as preferred language. In addition, we have now been able to observe telemedicine use over longer time frame than prior studies to understand steady-state patterns.
Our study aim was to compare telemedicine versus office visits during the COVID-19 pandemic (March 15, 2020 – March 15, 2021) in terms of overall trends in use, reason for visit, and patient characteristics at two diverse Medicaid-focused pediatric primary care clinics with a substantial subset of patients with Spanish as the preferred language.
Methods
DESIGN AND SETTING
This retrospective cohort study compared trends in telemedicine versus office visits during the first year of the COVID-19 pandemic in pediatric primary care clinics serving Medicaid-enrolled patients. This study was approved by the Johns Hopkins Institutional Review Board.
Patients in two academic-based practices in Baltimore City were included. Site A cares for approximately 7,300 patients from birth to 21 years of age, who predominantly identify as non-Hispanic/Latinx Black. Site B cares for approximately 6,500 patients from birth to 21 years of age and serves predominantly Latino children of immigrant parents with Spanish as the preferred language. The predominant payor at both clinics is Maryland Medicaid (including Medicaid managed care organizations). Both clinics are Johns Hopkins Medicine ambulatory sites. They use the same electronic health record (EHR), Epic (Epic Systems, Verona, WI), and have similar policies, procedures, and infrastructures. Telemedicine visits could be launched from the EHR and accessed by patients through the patient portal. Both clinics had access to alternative telemedicine platforms if the patient could not access the EHR-embedded platform. Both clinics initially implemented restrictions related to whether patients with COVID-19 symptoms could be seen for in-person appointments. Site A had the capability to see symptomatic patients in person as of November 2020, whereas site B did not have the ability to evaluate and test symptomatic patients in person during the study period.
Inclusion criteria for this analysis were as follows: all new or follow-up telemedicine or in-person office encounters at the two pediatric primary care clinic sites from March 15, 2020 - March 15, 2021; patients 0–21 years of age at the time of their visit. Telephone (audio only) visits comprised <5% of all telemedicine visits. Given this small proportion (<5%), we did not differentiate between video-based and telephone-based visits in our analysis. Encounters were excluded if they were the following visit types: ancillary, procedural, imaging, infusion, research, nurse only, or influenza vaccine.
MEASURES
We examined several demographic characteristics. For each patient in the study, we obtained child’s age (categorized as <1, 1–4, 5–13, 14–17, and 18–21 years), sex, race/ethnicity (coded from independently reported race and ethnicity variables, as recorded in the EHR as four distinct groups: non-Hispanic/Latinx Black, non-Hispanic/Latinx White, Hispanic/Latinx, and Other), preferred language (English, Spanish, or Other), need for interpretation (yes or no), and payor (public, private, or self-pay/other/unknown). Rapidly changing registration processes during the pandemic led to a higher percentage of patients with unknown insurance status at the time of encounter. As a result, we categorized these patients as self-pay/other/unknown.
For our visits, we categorized based on visit type and reason for visit. Visit type was classified as either telemedicine or office visit. Reason for visit was classified as well-child care (WCC, defined by EHR visit type, including key words “New Patient,” “Physical,” or “Newborn”), mental health care (MHC, defined by having mental and/or behavioral health as encounter diagnoses), and acute/follow-up care (AC/FU, defined by EHR visit type, including key word “Follow,” “Same Day,” “Video New,” “Video Return,” and did not have an encounter diagnosis for MHC, WCC, or need for vaccination). An encounter may be categorized as having more than one purpose for visit based on these definitions.
DATA ANALYSIS
Using services of the Johns Hopkins Biostatistics, Epidemiology, and Data Management Core and the Johns Hopkins Center for Clinical Data Analysis, data were obtained from Epic data field extraction. Data contained limited personal identifiers in compliance with rules and regulations regarding protected health information.
Descriptive statistics were reported for each site as follows: (1) differences in demographic characteristics by visit type and (2) differences in reason for visit by visit type. Chi-square test analysis was used to assess differences between proportions, and a value of p < 0.05 was deemed statistically significant. We additionally evaluated monthly telemedicine utilization changes over the course of the study period for both clinics collectively, overall and stratified by reason for the visit.
Univariable and multivariable mixed multilevel logistic regression was used to assess odds ratios of any telemedicine use for the primary outcome mentioned above. A forward stepwise approach was utilized in building the multivariable models, including clinically important demographic factors (patient age, sex, race/ethnicity, payor, and preferred language), as well as a significance cutoff of p < 0.05 for other potential confounders. All analyses were performed using Stata 17.0 (College Park, TX).
Results
The sample included 17,142 total completed visits for 8,375 patients: 7,447 encounters from Site A and 9,695 encounters from Site B. At both sites, most patients were publicly insured (Site A: 77%, Site B:75%). At Site A, 78% identified as non-Hispanic/Latinx Black and had 94% with English as the preferred language, whereas at Site B, 81% identified as Hispanic/Latinx and had 78% with Spanish as the preferred language (Table 1).
Characteristics of Telemedicine and Office Visits by Preferred Language (n = 17,142)
Around 13% of encounters at Site A (n = 987) and 25% of encounters at Site B (n = 2,421) were conducted using telemedicine. At both sites, those who identified as non-Hispanic/Latinx White had English as the preferred language and no interpretation needed had the highest proportion of telemedicine visits, in comparison to encounters for patients of other race/ethnicities, Spanish or other as the preferred language, and needed interpretation, respectively (Table 1).
There was variation in the extent to which telemedicine was used as a proportion of total visits and for each reason. Overall, 64.2% of encounters were for WCC (n = 10,997/17,142), 9.2% were for MHC (n = 1,581/17,142), and 44.1% were for AC/FU (n = 7,562/17,142). At both clinics, encounters for MHC had the highest proportion of telemedicine visits, followed by AC/FU and then WCC (Table 2).
Purpose of the Visit by Encounter Type (n = 17,142 Encounters)
Note: Categories are not mutually exclusive. A visit can be represented more than once. See Methods.
In addition, there was variation in the extent to which telemedicine use was sustained throughout the study period. For all types of visits, telemedicine use reached a peak at approximately April 16–May 15, 2020 (45% overall, 28% WCC, 77% MHC, and 55% AC/FU visits), reaching a stable rate by January–March 2021 (17% overall, 10% WCC, 34% MHC, and 24% AC/FU visits) (Fig. 1).
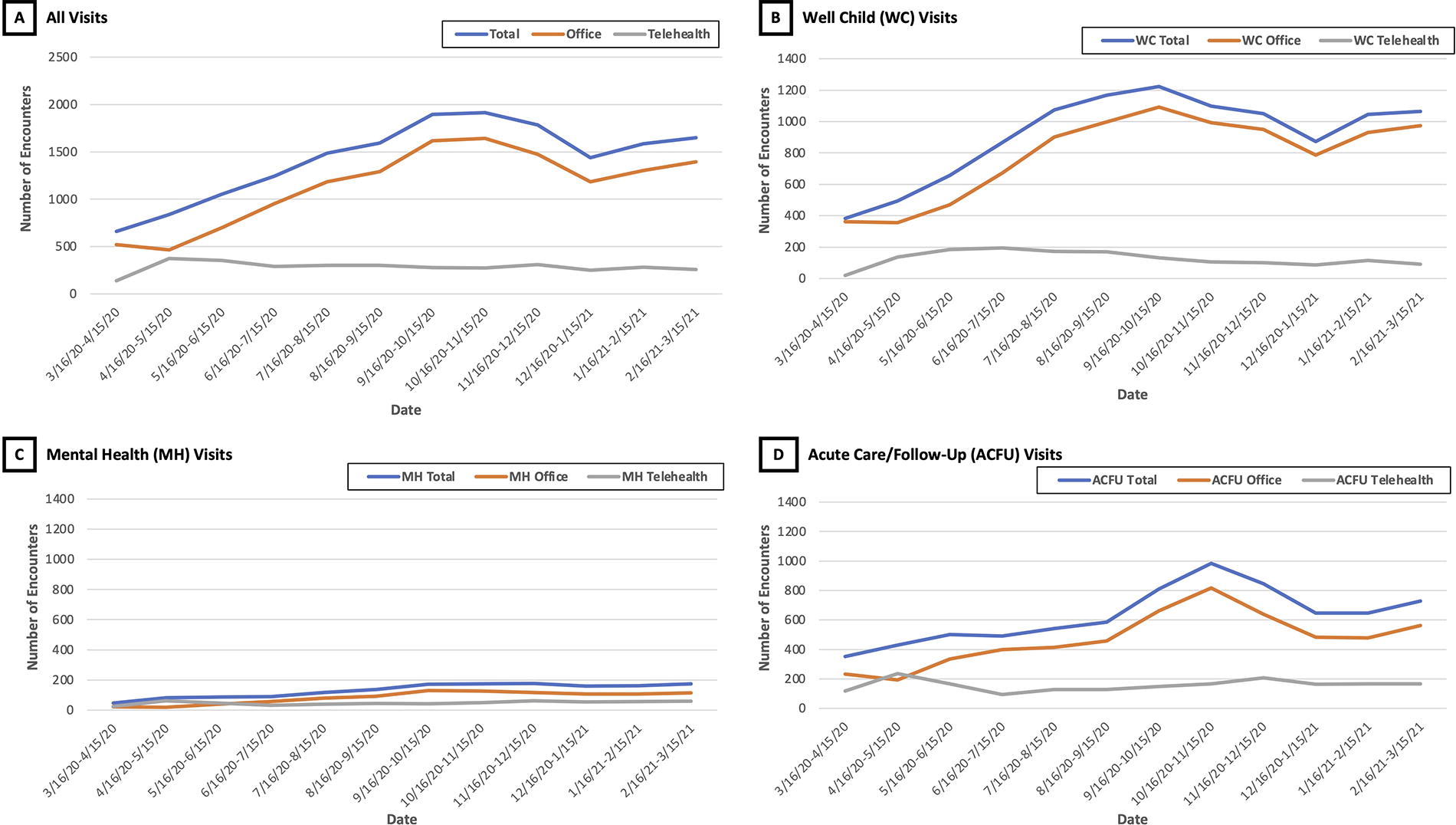
Distribution of encounters over time by encounter type for all encounters and by visit purpose (well-child, mental health, and acute care/follow-up). *Note: Visits were not mutually exclusively categorized into these areas. See Methods.
Table 3 summarizes patient-level analysis of odds of a patient having at least one telemedicine encounter by patient characteristics. After adjustment for covariates, at both sites, there was no statistically significant difference in odds of telemedicine use by preferred language, sex, and payor. At both sites, patients of different age groups had different odds of telemedicine use in comparison to patients < 1 year old, with the 1–4-year age group having the lowest odds of completing at least one telemedicine visit. While at Site A, patients who identified as NH Black, Hispanic/Latinx, or other race/ethnicity had lower odds of telemedicine use in comparison to NH White, at Site B, there was no statistically significant difference in odds of telemedicine use by race/ethnicity.
Odds of Telemedicine Use by Patient Characteristics (n = 8,375 Patients)
Multivariable adjustments were as follows:
Preferred language—adjusted for age, sex, race/ethnicity, and payor; age—adjusted for sex, race/ethnicity, payor, and preferred language; sex—adjusted for age, race/ethnicity, payor, and preferred language; race/ethnicity—adjusted for age, sex, payor, and preferred language; payor—adjusted for age, sex, race/ethnicity, and preferred language.
Discussion
In this study, we examined telemedicine use in two pediatric primary care settings serving predominantly Medicaid-enrolled patients, but with distinct populations in the same city (Site A serving predominantly non-Hispanic/Latinx Black versus Site B serving predominantly Hispanic/Latinx Spanish-speaking communities). We found that telemedicine was successfully accessed during the first year of the COVID-19 pandemic regardless of preferred language and payor. Both patient populations were able to complete telemedicine visits for a variety of visit purposes, including well-child care, mental health care, and acute care/follow-up. The highest proportion of visits conducted using telemedicine was for the purpose of mental health care. Both clinics rapidly transitioned to providing a large proportion of pediatric primary care visits through telemedicine and sustained these offerings 1 year into the pandemic.
These findings are consistent with recent studies showing similar patterns of rapid telemedicine operationalization in adult primary care, pediatric subspecialty utilization during the COVID-19 pandemic, 24 –26,32,33 and specifically, studies in pediatric primary care in underserved populations. 23 –28 Given that the majority of prior studies did not evaluate a variety of populations in a single study and did not have representation of populations with PLOE, our study results showing telemedicine operationalization in distinct Medicaid-focused populations offers valuable insights into how we can achieve equitable telemedicine access.
In contrast to prior studies in pediatric primary care showing lower telemedicine use by patients with PLOE, our study showed that there was no difference in odds of telemedicine use by preferred language. 24,25,33 This may be because, as previously mentioned, Site B is a medical home that primarily supports patients who identify as Hispanic/Latinx and has providers who are directly able to communicate in Spanish with their patients. Although Site A has a smaller proportion of patients who are Hispanic/Latinx and/or Spanish speaking than Site B, Site A did offer significant language support for telemedicine visits through remote video and telephone interpreters. Overall, by offering telemedicine with interpretation support (either in person or through video or telephone), we were able to provide access to telemedicine for patients with non-English preferred language. These findings highlight that telehealth can be operationalized for children in families with PLOE and the need for future Medicaid reimbursement to sustain telemedicine infrastructures equitably in pediatric primary care settings. 29
One interesting finding in our study was that we only saw differences in telemedicine use by race/ethnicity at Site A, but not site B, and by age at both sites. It is unclear whether these differences were related to patient-based (e.g., preference for telemedicine or in person) or clinic-based factors (e.g., availability of in-person versus telemedicine visits for patients with respiratory symptoms). Site B had two notable operational differences from Site A. In addition to having providers able to conduct visits in Spanish, Site B offered significantly more community resources specifically for Hispanic/Latinx families with Spanish as preferred language. In addition, Site B clinic policies also required all patients with respiratory symptoms to be seen by telemedicine first, potentially eliminating patient choice in choosing in-person care modalities. These differences in disparities by race/ethnicity between the two clinics may be highlighting the differential impact of overall clinic operational procedures in outpatient clinics. As a result, knowledge of how operational procedures can mitigate or exacerbate disparities in telemedicine use can help inform the creation and maintenance of future telemedicine implementation within health systems and be successful across all populations.
LIMITATIONS
There are a few limitations to consider when interpreting our study findings. First, because our study focused on EHR data, we cannot account for patient or parent preferences for telemedicine use. Second, because the two clinics varied significantly in resources, we were unable to further investigate variation in operational factors that contributed or mitigated disparities we saw during a turbulent time in the pandemic. Third, our study focused on two pediatric primary care clinics, with both sites affiliated with one institution, which may impact generalizability. Fourth, we did not have data available to examine the effect of health literacy and access to devices on telehealth use in our study sample. Fifth, the study period overlapped with the COVID-19 pandemic, which significantly impacted operationalization of telemedicine over time. However, our study does overcome other previous study limitations, which did not have study populations with majority being on public insurance and those with significant proportion of patients with Spanish as the preferred language. Therefore, our study contributes to the overall need for literature around achieving equitable telemedicine access for diverse Medicaid-focused pediatric populations.
Conclusions
Telemedicine was found to be feasible in pediatric primary care settings for Medicaid-enrolled patients and for variety of types of care, including well-child, mental health, and acute care/follow-up. This was consistent for families who had the preferred language as Spanish in comparison to English and those who had Medicaid insurance in comparison to private insurance. Disparities continued to exist by race/ethnicity at one site and may be attributable to operational differences and resource support for telemedicine between two clinic sites. Despite the end of the pandemic, telehealth continues to be an important part of health care delivery and to understand the nuances to how it can be done equitably continues to be a key need, especially among pediatric patients for primary care. Medicaid programs should consider investment in device access, access to interpreter services, digital health access and addressing digital health literacy as a social determinant to promote equitable digital health use among marginalized pediatric populations.
Footnotes
Authors’ Contributions
N.C.: Conceptualization, methodology, formal analysis, writing—original draft, and project administration; A.R.L.: Methodology, formal analysis, writing—review and editing, and project administration; L.P.: Software, validation, formal analysis, data curation, and writing—review and editing; M.T.: Funding acquisition, writing—review and editing, and supervision; N.S.: Funding acquisition, writing—review and editing, and supervision; S.P.: Funding acquisition, writing—review and editing, and supervision; E.M.P.: writing—review and editing and supervision; H.K.H.: Conceptualization, methodology, writing—review and editing, funding acquisition, and supervision.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded by the Robert Wood Johnson Foundation (Grant # 78238).