
Abstract
Introduction:
To examine telehealth use in chronic care management and disparity reduction among the aging population.
Methods:
This longitudinal cohort study compared the changes in chronic care quality measures among patients with and without telehealth visits during the COVID-19 pandemic relative to patients in the previous years and by patient sociodemographic subgroup. Participants were Medicare fee-for-service beneficiaries 65 years or older from an Accountable Care Organization in the Midwest United States. Three utilization-based measures included having 2+ A1C tests, breast cancer screening, and depression screening. Three outcome-based measures included A1C control, blood pressure control, and depression diagnosis.
Results:
During the study period, the pandemic cohort experienced 5–17 percentage points' decrease in utilization-based measures (e.g., 2+ A1C tests 63.9% vs. 51.1%; OR [95% confidence intervals] = 0.35 [0.34–0.36]) from baseline relative to the control cohort. The outcome-based measures also significantly decreased but at smaller magnitudes (3–5 percentage points). About 51.5% patients had at least one telehealth visit. The utilization-based measures for these patients were significantly higher than those without any telehealth visit (e.g., 2+ A1C 57.1% vs. 51.1%, p < 0.01). However, the outcome-based measures were comparable. Patients from historically underserved groups had a larger decline in health care outcomes than their counterparts. Among patient with at least one telehealth visit, these disparities were no longer significant.
Discussions:
Telehealth was associated with less negative impact of the pandemic and better performance in chronic care management, but more for utilization-based measures and less for outcome-based measures. Telehealth was also associated with less disparities in care outcomes.
Introduction
Almost a third of U.S. adults live with multiple chronic conditions (MCC). Among this group, disadvantaged or historically underserved populations such as the low-income, disabled, racial/ethnic minorities, and rural residents are disproportionately affected, with significant disparities in health and care quality. 1 –3 Primary care has a critical role in optimizing management for these patients with MCC. 4 However, during the COVID-19 pandemic, non-COVID-related care utilization significantly decreased. 5 –8 Preventive care and chronic care management in primary care settings experienced the largest decline among all care service categories. 9,10 The missed or delayed care and the related results in worse-care outcomes were found to be more severe among disadvantaged subpopulations. 11,12
Telehealth use has rapidly increased in primary care since the outbreak of the COVID-19 pandemic. Chronic care management programs within health systems increased their use of telehealth to provide timely care and prevent exposure to COVID-19. 13 It is unclear if telehealth could improve chronic care management and reduce disparities in real-world conditions. 14 Telehealth use can potentially mitigate or exacerbate disparities in care quality; it can reach beyond the office to more diverse patients, yet disadvantaged patients are least likely to have the technology required. 15 With the expansion of telehealth use and its potential to overcome barriers to care access, 16 –19 health systems and patients must have real-world evidence of the benefits of telehealth use on health outcomes and disparity reduction to optimize telehealth use in MCC management. 20
Incorporating telehealth into MCC management should mitigate, not exacerbate, the existing documented health disparities among vulnerable populations. 21 –24 While there existed some evidence on telehealth use disparity, the evidence regarding telehealth's effect on care outcomes and the disparities in the benefits of telehealth is still limited. Existing studies have shown that males, the advanced aged (86 years or older), high-risk (with MCC), low-income patients, and patients living in rural areas were all less likely to use telehealth. 12,25,26 What is still unclear is to what extent telehealth could help improve or maintain care quality in MCC management, and whether these telehealth benefits are the same among different subpopulations. 20,21,25,27,28
The objective of this study is to examine the association of telehealth use with chronic care management and disparity reduction in care outcomes for disadvantaged patients 1 –3 with chronic conditions among the aging population. In March 2020, the Centers for Medicare & Medicaid Services (CMS) implemented waivers to allow telehealth to be reimbursed for Medicare fee-for-service (FFS) beneficiaries with few restrictions. 12,17,29 Telehealth utilization increased more than 10-fold within the first few months of this policy change. 12,17,20 This study uses telehealth expansion during the COVID-19 pandemic as an opportunity to examine the extent to which telehealth is associated with care outcomes for patients with chronic conditions and the disparities in these outcomes among historically underserved populations.
Findings from this study will support health system decisions on incorporating telehealth for chronic care management in primary care settings. Findings will also support public and private payers to make informed decisions on telehealth reimbursement policy, for example, to end, extend, or make permanent the waivers for telehealth delivery. 30,31
Methods
STUDY DESIGN, DATA, AND SAMPLE
This longitudinal cohort study compared the changes in completion rates of a series of care performance metrics for chronic care management between Medicare FFS beneficiaries during the COVID-19 pandemic (treatment) when telehealth became reimbursable for the first time by CMS and those before the pandemic (comparison) when telehealth was rarely used by these beneficiaries. The baseline information for the treatment and comparison groups was used to adjust the time-invariant differences between the two groups. The patient-month level longitudinal data were used to adjust the variations at the patient level. To quantify the role of telehealth in maintaining chronic care management under the general background of the pandemic, beneficiaries in the treatment group were categorized into groups with no telehealth or in-person visit, with at least one telehealth visit, and/or with at least one in-person visit.
To quantify the role of telehealth in reducing disparities, comparisons of care metric changes were also made by patient subgroup. The subgroups included beneficiaries who had Medicare and Medicaid dual coverage or disability entitlement, were racial/ethnic minorities, living in town/rural areas, having a hierarchical condition category (HCC) score two or more (high risk), or aged 86 years or older.
The data used in this study were from electronic health records (EHRs) and claims data from a Medicare Accountable Care Organization (ACO) in the Midwest of the United States. Medicare FFS beneficiaries 65 years or older who were continuously enrolled in Medicare Part A and Part B and were served by primary care physicians from the ACO provider list at the beginning of the study period were included in the study sample. The study period for the pandemic cohort (treatment group) was from April 2020 to December 2020. The same 9 months in the previous year (April–December 2019) was the study period for the comparison cohort (comparison group). The baseline period was defined as the previous 12 months of the study period for each cohort (Supplementary Fig. S1).
To differentiate beneficiaries with different chronic care management concerns, the sample was further categorized into health care concern-specific cohorts: diabetes, blood pressure monitoring, breast cancer screening, and depression monitoring. Eligible patients for each health care concern were identified using existing methods. 32,33 The diabetes cohort included beneficiaries who were ever diagnosed with diabetes as of the beginning of the study period. The blood pressure control cohort included those beneficiaries with diabetes, hypertension, or cardiac conditions. The breast cancer screening cohort included all female beneficiaries between 65 and 75 years old. The depression monitoring cohort included all beneficiaries 65 years or older with at least one mental health-related visit in the baseline period. For all cohorts, eligible patients only included those who were not in hospice or any other institutional living settings. The final data set was organized as longitudinal data with patient-month as the unit of observation.
The University of Wisconsin-Madison Institutional Review Board approved for an exemption of this study. Report of the study results followed the STROBE guidelines.
OUTCOMES
Two groups of validated care performance metrics from chronic care management guidelines were used as outcomes in the study. 34 –36 The utlization-based measures included having two or more A1C tests, breast cancer screening, and depression screening (complete Patient Health Questionnaire [PHQ]-2 or PHQ-9). The outcome-based measures included having A1C control (<8% for the most recent test score), 37 blood pressure control (<140/90 mmHg for diabetic patients and <150/90 mmHg for hypertensive patients), 38 and a depression diagnosis. These measurements were calculated for each eligible patient in each month using a 12-month look back rolling period except breast cancer screening, which used a 24-month look back instead. 39,40
For each patient-month record, a care performance metric had a value of 1 if the patient completed the recommended laboratory tests (laboratory or screening), achieved the care maintanence goal (A1C or blood pressure control), or was diagnosed within the past 12 (depression) or 24 months (breast cancer) according to the guideline, and 0 otherwise.
MAJOR EXPLANATORY VARIABLES
The major explanatory variables included indicators of the pandemic cohort (vs. the comparison cohort), the study period (vs. the baseline), and whether there was at least one telehealth visit for each patient-month record within the pandemic cohort during the study period. Two-way and three-way interaction terms were also included in the analytical models.
CONFOUNDERS AND RISK ADJUSTMENT
Variables used for risk adjustment included patients' sociodemographic variables and health conditions in the baseline, as well as the monthly care utilization in outpatient settings. The sociodemographic variables included a patient's age group (65–74 years old, 75–85 years old, or 86 years or older), sex, race/ethnicity (minority or nonminority white), having Medicare and Medicaid dual coverage (ever or not), having disability entitlement (ever or not), and the geographic category for living areas (urban, suburban, large town, or small town/remote rural). Health conditions in the baseline included a patient's HCC, indicators of an HCC score higher than two (deemed as high-risk population), and having three or more chronic conditions. 41
The monthly care utilization in outpatient settings included indicators of having at least one in-person visit in primary care settings, the total number of primary care visits (both in-person and telehealth), and the total number of specialty care visits (both in-person and telehealth).
STATISTICAL APPROACHES
For each of the six care performance metrics, logistic regression models were used to regress the value of a quality metric (1 if yes and 0 otherwise) at the patient-month level on indicators of cohort, time, the interaction of the two, and the three-way interaction of cohort, time and telehealth utilization (1 or 0) for the corresponding patient cohort (diabetes, blood pressure, breast cancer, or depression). The interaction term of cohort and time captured the changes in the completion rate of a care performance metric for the pandemic cohort during the study period from the baseline relative to the comparison cohort. The three-way interaction term of cohort, time, and telehealth utilization captured the changes in completion rates that could be explained by telehealth for the pandemic cohort in the study period.
It was hypothesized that (1) the completion/success rates for care metrics decreased during the pandemic relative to before; (2) the utilization-based metrics experienced a larger decrease in completion/success rates than the outcome-based metrics, since utilization-based metrics were more directly responsive to the systematic reduction in non-COVID care utilization during the pandemic, whereas outcome-based metrics would take longer time to show the changes; and (3) telehealth use was associated with lower decreases in these metrics (than no telehealth use), and further, the association was stronger for the utilization-based metrics and weaker for the outcome-based metrics.
To calculate the different changes in completion rates by telehealth use across subgroups in the pandemic cohort during the study period, six indicators of disadvantaged groups were used. These indicators included Medicare and Medicaid dual coverage, disability entitlement, racial/ethnic minorities, living in town/rural areas, having an HCC score of two or more (high-risk), and aged 86 years or older. These subgroups were evaluated one at a time. In the regression model, in addition to the major explanatory variables (cohort, time and telehealth utilization), the subgroup indicator, the three-way interaction of the subgroup indicator and cohort and time, and the two-way interaction of the subgroup indicator and telehealth utilization were added. We hypothesize that (1) the disadvantaged subgroups experienced a larger decrease in completion rates for the care metrics (as negative pandemic impacts) than their counterparts and (2) telehealth use was associated with less negative pandemic impacts for these disadvantaged subgroups.
To report the results, we calculated the odds ratios and 95% confidence intervals (CIs) for cohort, time, and the interaction of the two. We also predicted the average completion/success rates and their 95% CIs for each care quality metric by cohort, time, telehealth utilization, and patient subgroup. The analysis was conducted from March to December 2022 using STATA SE 16.0.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The University of Wisconsin-Madison Institutional Review Board approved for an exemption of this study because it involves secondary analysis of deidentified data. This article does not contain any studies with human or animal subjects. There are no human subjects in this article and informed consent is not applicable.
Results
SAMPLE CHARACTERISTICS
The study sample included 31,870 patients (16,222 in the pandemic cohort and 15,648 in the comparison cohort) and 675,348 patient-month records. Around 6,350 patients (19.9%) were identified to be eligible for diabetic care management, 21,706 patients (68.1%) for blood pressure monitoring, 8,077 patients (25.3%) eligible for breast cancer screening, and 20,042 patients (62.9%) under depression monitoring. The sample had an average age of 75 years old (standard deviation = 6), were 59.5% women, 96.4% nonminority white, 6% with Medicaid and Medicare dual coverage, 4.3% with disability entitlement, and 12.8% living in town or rural areas. About 48% of the patients had three or more chronic conditions and 43% had an HCC score higher than two (Table 1).
Sample Description in the Baseline
HCC, hierarchical condition category; SD, standard deviation.
Entries are percentages (0–100) unless otherwise noted.
The care utilization in the baseline period was also comparable between the pandemic and comparison cohorts for each chronic condition group. During the 10-month study period, care utilization for the pandemic cohort decreased in all categories, whereas care utilization for the comparison cohort stayed almost the same as the baseline (Table 2).
Care Utilization per Patient in the Baseline and the Study Period
Entries are averages with SDs in parentheses.
CARE PERFORMANCE METRICS DURING THE PANDEMIC
The completion rates for utilization-based metrics significantly decreased for the pandemic cohort during the study period relative to the comparison cohort (OR [95% CI] = 0.35 [0.34–0.36], 0.54 [0.51–0.56], and 0.45 [0.45–0.46], respectively, for having two or more A1C tests within the past 12-month period, having breast cancer screening, and having depression screening). For A1C tests, the risk-adjusted completion rate was 63.9% (95% CI = [63.6–64.3%]) for the pandemic cohort in the baseline. Yet the rate decreased to 51.1% (50.6–51.6%) among patients with no telehealth visit in the study period, which represented a 12.8% absolute decrease and 20% relative decrease. In comparison, the completion rate for patients with at least one telehealth visit during the study period was 57.1% (55.7–58.5%), suggesting that telehealth was associated with less negative impacts of the pandemic on chronic care quality metrics by almost 50%.
Furthermore, the completion rate for patients with at least one in-person visit in the pandemic cohort during the study period was 57.1% (56.3–58%), suggesting that telehealth is comparable with in-person visits in maintaining chronic care management. Similar results were found for depression screening. For breast cancer screening, although the completion rate decreased for the pandemic cohort during the study period relative to the baseline (72.5% vs. 76.6%), the rate was not significantly different among patients with telehealth visits, in-person visits, or without (72.7%, 73.4%, 72.5%, respectively) (Table 3).
Risk-Adjusted Quality Measures
The symbols ***, and * represent 99%, 95%, and 90% significance level.
CI, confidence intervals.
The success rates for outcome-based quality metrics such as A1C control and blood pressure control were significantly lower for the pandemic cohort in the study period relative to the baseline (OR [95% CI] = 0.71 [0.67–0.75] and 0.68 [0.66–0.70]). The depression diagnosis rate was higher during the study period than the baseline (1.23 [1.12–1.34]). These results suggested a negative effect of the pandemic on chronic care management and mental health outcomes for patients, which was consistent with the general literature. 10,11,42 However, the success rates of these measures (or diagnosis rates for depression) were not significantly different among patients with telehealth visits, in-person visits, or without (Table 3).
DISPARITIES IN CARE PERFORMANCE METRICS
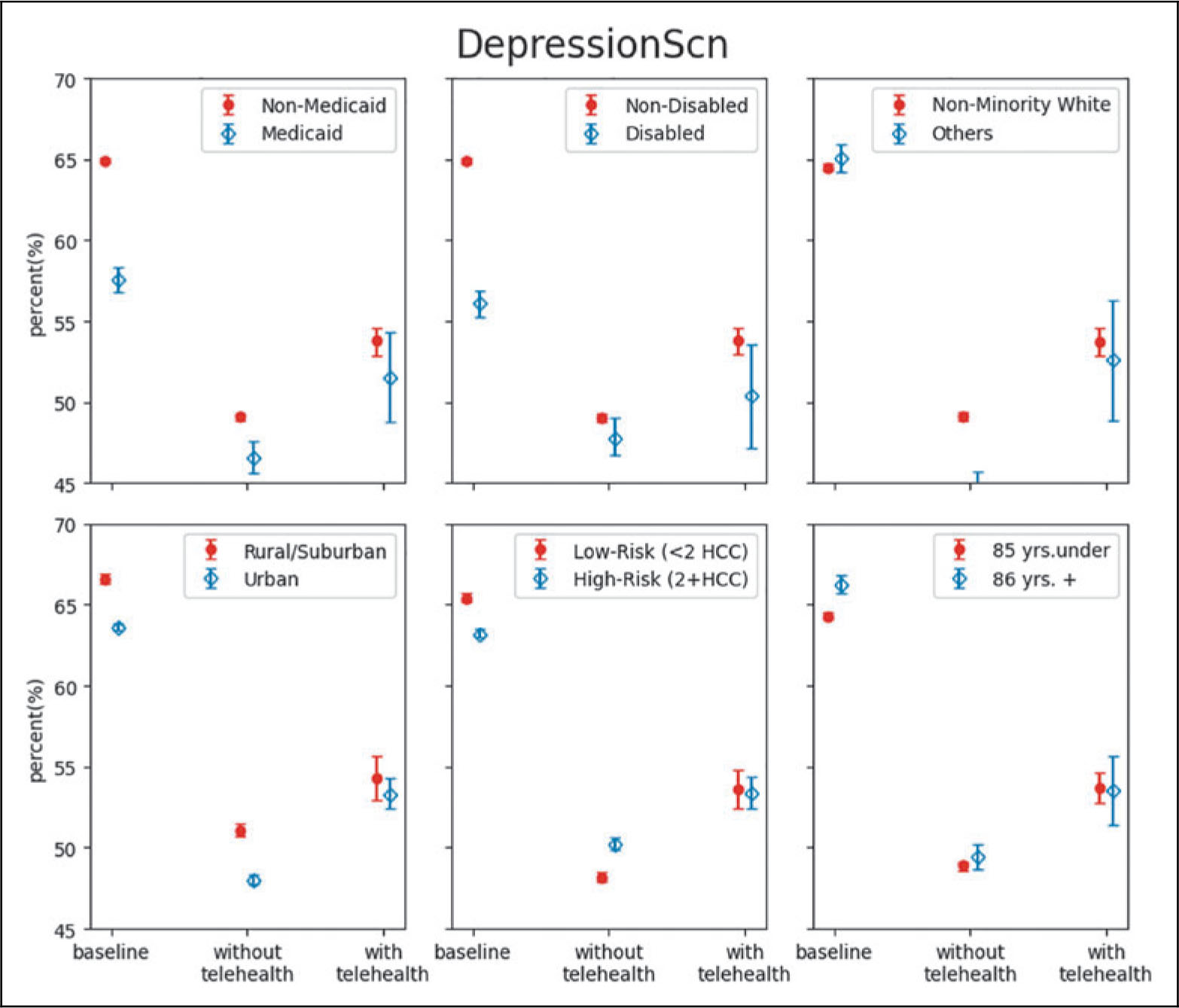
Telehealth was also associated with disparity reduction in care metrics during the pandemic for some subpopulations. For utilization-based measures, during the pandemic, patients with Medicare and Medicaid dual coverage experienced a larger decrease in the completion rate of having two or more A1C tests, yielding a significantly lower rate than patients without dual coverage. However, among patients with at least one telehealth visit in the study period, this difference was no longer significant. Similar disparity reduction patterns of telehealth were also found among disabled, urban, or high-risk patients for breast cancer screening, and among dual coverage, racial/ethnic minorities, or low-risk patients in depression screening rates (Fig. 1 and Supplementary Table S1).
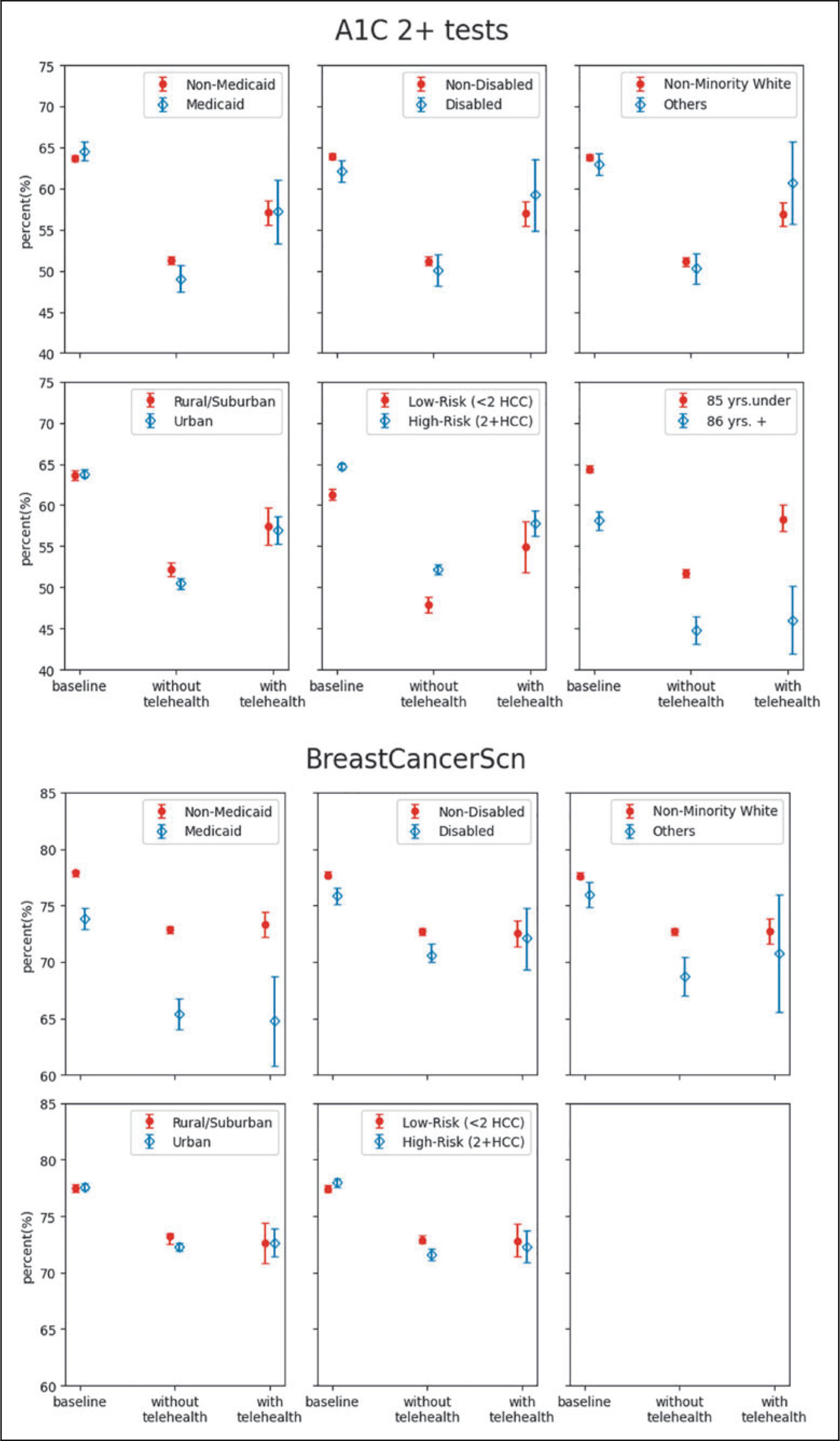
Risk-adjusted care metrics by subgroup—A1C 2+ tests, breast cancer screening, and depression screening.
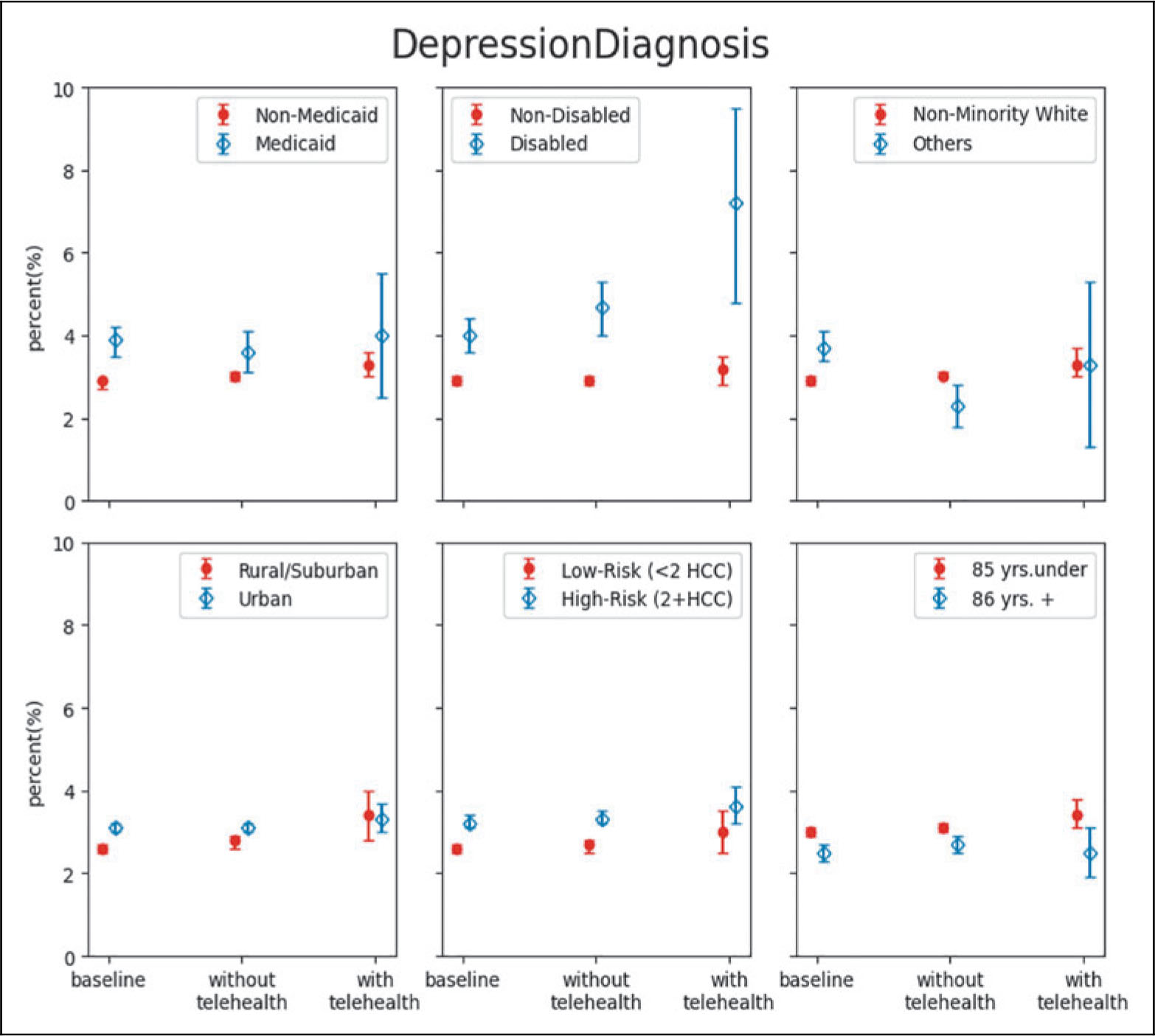
For outcome-based measures, dual coverage, rural/suburban, or high-risk patients had significantly lower success rates in A1C control than their counterparts when they did not have any telehealth during the pandemic. Yet, with at least one telehealth visit, the differences in A1C control rates were no longer significant between subgroups. Similar patterns were also found for racial/ethnic minorities, urban or high-risk patients in blood pressure control rates, and for dual coverage, racial/ethnic minorities, rural/suburban patients, or low-risk patients in depression diagnosis rates (Fig. 2 and Supplementary Table S1).
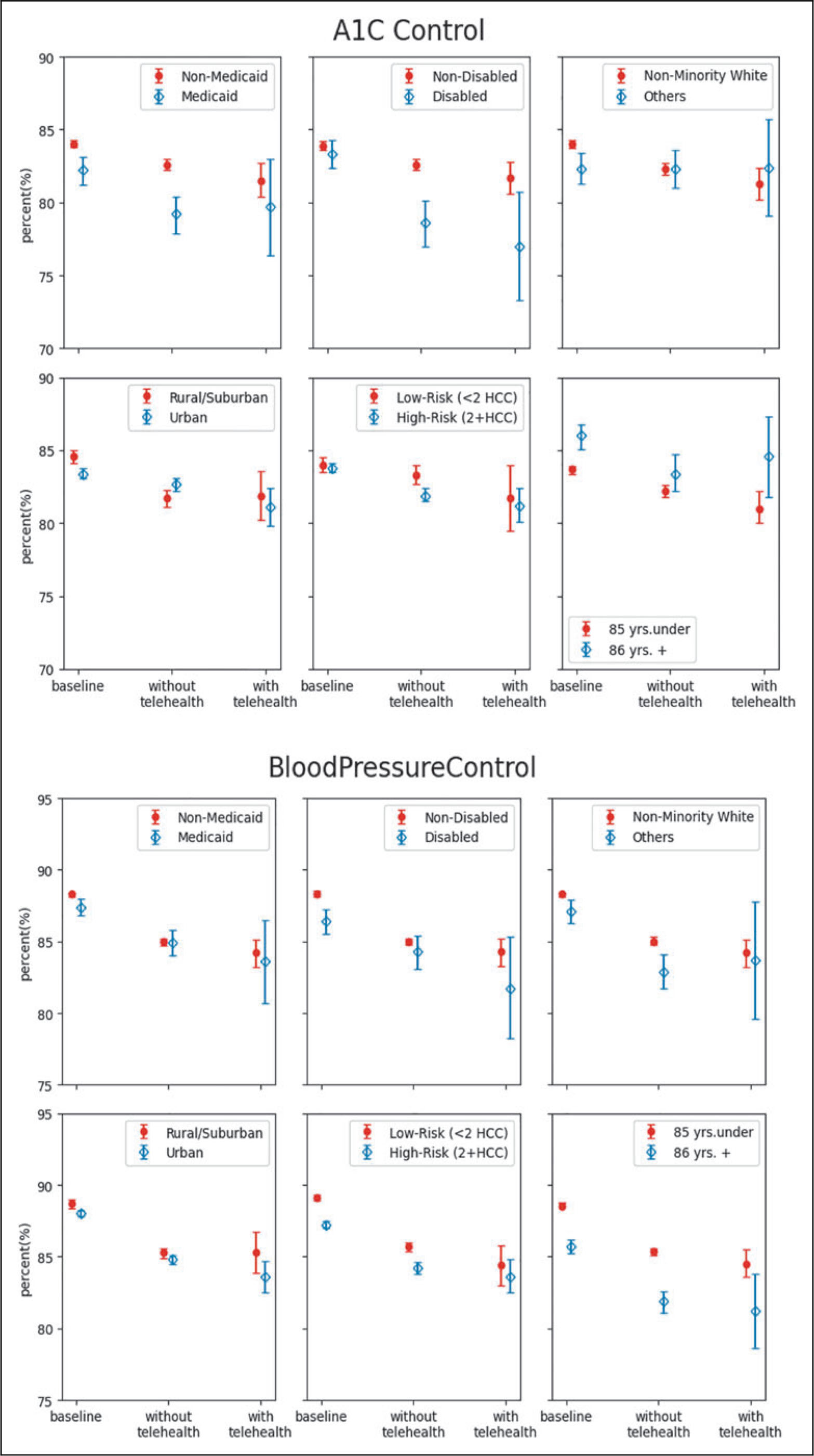
Risk-adjusted care metrics by subgroup—A1C control, blood pressure control, and depression diagnosis.
Discussion
Using the rapid expansion of telehealth among clinics and patients during the COVID-19 pandemic, this study examined the use of telehealth in chronic care management and disparity reduction among the aging population. Our results suggest that telehealth use was associated with better chronic care monitoring and care performance metrics. Telehealth use was also associated with less negative effects of the pandemic and less disparities in chronic care outcomes.
Our results generated the following implications. First, in the general background of missed or delayed care due to the pandemic, telehealth acted as an alternative to in-person care services to help make up for missed or delayed care and maintain completion rates of chronic care management. Existing research showed that patients with chronic care management needs were less likely to keep up with health condition monitoring such as laboratory tests and screening during the pandemic. 43 –46 Our results showed consistent findings. In addition, we found that telehealth was associated with less negative pandemic effects by almost 50%. Furthermore, the association of telehealth with better completion rates of chronic care management was found to be very comparable with in-person services (Table 3).
Second, our study separated care performance metrics by utilization-based and outcome-based measures and found that outcome-based measures were less negatively affected by the pandemic than utilization-based measures. Moreover, telehealth was also associated with higher completion rates of outcome-based measures such as A1C and blood pressure control and better identification of depression cases.
Third, this study generated evidence on the association of telehealth with disparity reduction for care outcomes among vulnerable populations. 9,47 –50 These findings support the long-lasting policy initiatives, which recommended telehealth as a key strategy to reduce disparities in chronic care management in primary care settings. 9,51 These findings also highlight the need to reduce barriers to accessing telehealth for those from historically underserved groups. 47,48 During the COVID-19 pandemic, telehealth utilization was consistently lower among racial/ethnic minorities, the low-income population, the advanced aged, and those from remote rural areas. 12,49 These vulnerable populations were also found to be more likely to use office-visits or emergency department visits, 20,50 and less likely to complete a scheduled telehealth visit or maintain glucose or blood pressure control. 11,52 Given the evidence of telehealth's positive association in care management and disparity reduction, equitable access to telehealth is a key action to improve care quality in the long run.
LIMITATIONS
This study has a few limitations. First, the study sample is from one health care system, and hence, the sample and the study results may not be fully representative to the general population. The study sample also included only patients whose primary care providers were affiliated with the care system (to obtain accurate measures of chronic care management over time), and hence, results may not be generalizable to those who lack primary care coverage. Yet, limiting the scope to one health care system and patients who were medically homed within the system allowed us to leverage the rich information in the EHR to compile the monthly care quality metrics based on a full 12- or 24-month rolling look back period and patients' care history. Second, findings in this study about telehealth implied only association but not causal relationship with the care performance metrics.
For example, the changes of depression screening rates before and during the pandemic are likely confounded with the increase in depression or anxiety caused by the pandemic. Using some instruments such as the pandemic severity by time and location, or interventions (of telehealth) adopted at the care system or clinic level to create exogenous variations in telehealth utilization might help. Third, the data did not include information on patients' information technology (IT) literacy, receptiveness, or accessibility. Neither did it include information on IT education, technical support, and the variation of IT education and support offered by the health system. As a result, the observed telehealth utilization was conditional on availability and accessibility. Research on barriers and barrier removal efforts from both patient and provider sides is needed for the next steps.
Last, the analysis in this study was conducted based on care management needs rather than chronic care conditions. For example, the blood pressure monitoring sample included patients with diabetes, hypertension, cardiac conditions, and others. Extra caution is needed to interpret the results for any specific chronic care condition.
Conclusions
This study leveraged the telehealth expansion during the COVID-19 pandemic to examine telehealth use in chronic care management in primary care settings. Findings suggested that telehealth is associated with less negative effects of missed or delayed care due to care access barriers and better maintenance of the completion rates for utilization-based metrics. These associations stayed the same for outcome-based metrics but were not as strong for utilization-based metrics. Telehealth is also associated with disparity reduction in these care metrics for vulnerable subpopulations. Yet, the existence and magnitude of the disparity reduction depend on the specific metrics and/or patient subgroups.
Availability of Data and Materials
The data that support the findings of this study are available from the CMS, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with the permission of CMS.
Footnotes
Authors' Contributions
Study concept and design: Y.C. and M.S. Acquisition of data: M.S. and Y.C. Analysis and interpretation of data: all authors. Drafting of the article: Y.C. and D.C. Critical revision of the article for important intellectual content: all authors.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study is supported by the Patient-Centered Outcomes Research Institute (HSD-1603-35039) and the Wisconsin Alumni Research Foundation (AAI2989).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.