
Abstract
Introduction:
Beginning in 2019, the Department of Veterans Affairs (VA) prioritized improving access to care nationally to deliver virtual care and implemented 18 regionally based Clinical Resource Hubs (CRHs) to meet this priority. This observational study describes the quantity and types of care delivered by CRH Mental Health teams, and the professions of those hired to deliver it.
Methods:
A retrospective cohort study, based on national VA CRH mental health care utilization data and CRH staffing data for CRH's first 3 years, was conducted.
Results:
CRH Mental Health teams primarily used Telemental Health (TMH) to provide care (98.1% of all CRH MH encounters). The most common disorders treated included depression, post-traumatic stress disorder, and anxiety disorders. The amount of care delivered overtime steadily increased as did the racial and ethnic diversity of Veterans served. Psychologists accounted for the largest share of CRH staffing, followed by psychiatrists.
Conclusions:
CRH TMH delivered from a regional hub appears to be a feasible and acceptable visit modality, based on the continuously increasing CRH TMH visit rates. Our results showed that CRH TMH was predominantly used to address common mental health diagnoses, rather than serious mental illnesses. Traditionally marginalized patient populations increased over the 3-year window, suggesting that CRH TMH resources were accessible to many of these patients. Future research should assess barriers and facilitators for accessing CRH TMH, especially for difficult-to-service patient populations, and should consider whether similar results to ours occur when regional TMH is delivered to non-VA patient populations.
Introduction
Telemental Health (TMH) programs are rapidly developing across many health care systems, yet little is known about the feasibility, accessibility, and equitability with which these programs are implemented within large healthcare systems. TMH is commonly defined as using telecommunication technologies to provide mental health assessment and treatment at a distance. 1,2 The Department of Veterans Affairs (VA) has been a leader in developing and implementing TMH services for Veterans, and has long prioritized improving access to care. 3 –6 In response to concerns related to long travel times and wait times, Title IV of the (Health Care in Underserved Areas), section 402 of the 2018 MISSION Act funded the VA Clinical Resource Hubs (CRHs) to provide primarily primary care and mental health care. 7
There are 18 CRHs affiliated with all the 18 regional Veterans Integrated Service Networks (VISNs). 3,8 The CRH Mental Health (CRH-MH) teams primarily offer TMH care to Veterans enrolled underserved VA medical centers (defined as those with long appointment wait times), and Community-Based Outpatient Clinics (CBOCs). Inclusion versus exclusion criteria for establishing TMH care to these sites follow enrollment criteria used by VA for other non-CRH TMH care delivery.
Mental health providers who offer care through these CRH-MH teams are required to undergo VA-mandated training. In addition, they are expected to provide the same treatment guideline level care as other mental health providers in the VA, regardless of whether they are providing in-person or general TMH care. CRH-MH teams follow all national VA guidelines related to quality management and safety, and expectations for CRH-MH are not different than for routine VA care.
Within the VA, the MISSION Act (Title 1 Subtitle B, Section 151) allows those providers approved to offer telehealth services the ability to provide telehealth care across state lines with a single state license. 7 As providers work across state lines and time zones, care is based on where the Veteran is located. The majority of these appointments are scheduled routinely, with a small number of acute care interventions for mental health emergencies. Each CRH-MH team has a supervisor who oversees all providers on the team. Supervision expectations and services across state lines are completed in the same manner as within-state service delivery.
The early implementation period for CRH-MH teams studied here (FY20–FY22) was characterized by relatively naturalistic implementation of mental health services guided by broad CRH program goals, such as responding to the needs of rural clinics. During this period, the overall CRH program focused on developing mandated regional organizational elements, including recruitment of staff, and on responding to site requests for support. 8 –10 Early CRH-MH implementation was strongly influenced by the national emergency created by the onset of the COVID-19 pandemic, which emerged during the first year of CRH-MH implementation.
The pandemic forced rapid expansion of virtual services, including those for providing mental health care through CRH. 10 Previously shown determinants of utilization of VA virtual care included reduced uptake among rural Veterans, 11 ethnic minorities, and those with negative social determinants of health including socioeconomic status and homelessness. 12 –15 Without detailed national mandates or guidance regarding what types of mental health providers to hire, regional leaders collaborated with national program leaders to decide how best to meet pressing, unmet mental health needs among Veterans in their regions through virtual care.
Given that regional CRH-MH leaders had significant latitude in how they implemented staffing for MH services, staffing choices were made based on regional staffing resources and leadership perceptions about what types of staff would best meet patient needs. By observing staffing trends over 3 years, we aimed to provide a basis for future work on the relationships between staffing composition and the quantity, quality and accessibility of the mental health care provided.
The objective of this article is to describe the early stage of the CRH-MH services in terms of the demographics of those Veterans who received care, the types of diagnoses being treated, and the types of providers who offered this care. This information might be useful to other mental health professionals, patients, and health care system leaders as they consider implementing or evaluating provision of regional MH used as a means of addressing in-patient access deficits due to insufficient mental health staffing. To accomplish this, we assessed changes over time in utilization and staffing during the first 3 years of CRH-MH implementation (FY20–FY22).
Methods
Overview and ethics
We extracted national VA utilization data between October 1, 2019, and September 30, 2022 (FY20–FY22) from the VA's Corporate Data Warehouse (CDW) to evaluate early implementation of CRH-MH. This study is designated as quality improvement by the VA Office of Primary Care. This study is a component of the overall evaluation of the CRH program. 8 The study uses only deidentified VA administrative data and does not directly involve human subjects. This article adheres to STROBE reporting guidelines for observational studies. 16
TMH intervention
The CRH program nationally implemented regional TMH across all 18 VA administrative regions (VISNs). Each region supports a CRH “Hub” that aims to fulfill requests from any clinic in the region that is experiencing a staffing deficit. Clinics whose requests for CRH support are granted are considered CRH “Spoke” sites. As noted, for purposes of this report, TMH is defined as providing mental health care using video to clinic, video to home, or telephone-based care.
TMH evaluation
Sample
To assess the proportion of all VA-enrolled patients who had mental health encounters during the study period, we identified all Veterans enrolled in VA care nationally who had received at least one outpatient mental health visit during the study period as “mental health patients.” To assess the proportion of these who received CRH-MH care, we identified the subset of mental health patients who had completed at least one CRH-MH encounter during the study period and identified them as the cross-sectional cohort for each of the three study years. To assess CRH-MH staffing, we used operational staffing reports from the VHA CRH Dashboard.
Data collection
We extracted clinical encounters from VA's national CDW. For our longitudinal CRH-MH cohort, we attributed each included encounter to each patient's VA-assigned local clinic, using the VA Primary Care Management Module. Finally, we identified any encounters that were attributed to a CRH provider's Hub site when the Hub site was not the patient's most frequently visited mental health site. We attributed these encounters to the patient's assigned Spoke clinic instead, often by eliminating a duplicate encounter attributed to the Spoke site.
Measures
For each CRH-MH encounter and each study year, modality of care was determined based on primary and secondary stop codes. We extracted the Veteran's demographic information, which included age (years), sex (male/female), race (self-reported as White, Black, Asian, Multi-Race, Other), ethnicity (Hispanic/non-Hispanic), marital status (married/other), copay status (copay required/copay not required due to means/copay not required due to disability/unassigned), comorbid condition count, enrollment in primary and community care, and homeless status from the CDW. We linked in data from the Planning Systems Support Group Files for each year to assess Veteran drive distance to the nearest VHA primary care site and the rurality of the patient's home address (urban, rural, highly rural/insular islands).
Analysis
We aggregated each measure by fiscal year. Descriptive statistics were calculated using independent t-tests for continuous variables and Fisher's exact or Chi-square tests for categorical variables to evaluate differences. Missing data values for all covariate measures were included in the analysis. All statistical analyses were performed using SAS Enterprise Guide Version 7.1. p-values of 0.05 were used to assess statistical significance across FY to assess changes in the type of Veterans engaging in CRH-MH services over time.
Results
A total of 165,942 (of 2,741,677) Veterans (6.1%) engaged in any VA mental health services during the study period. There were 779,908 encounters among these 165,945 Veterans over a 3-year period. Of these encounters, only 1.9% were presumed to be in-person encounters. The average age of the CRH-MH cohort was 52.0 years (standard deviation = 16.1); 18.8% (n = 31,175) were female, and 76.5% were White.
The majority of the cohort (93.0%) did not require a copay to use VA services due to either disability or means, and 83.7% of the cohort had two or more chronic conditions. Approximately 42.0% of Veterans reside in rural or highly rural designated areas, and the majority of Veterans were receiving primary care services through the VA (94.9%). Although there were two VISNs that were responsible for ∼30% of overall CRH-MH utilization during this time period, these VISNs contained pilot sites that were early adopters of the program with infrastructure already in place.
Between FY20 and FY22, the mean age of Veterans enrolled in CRH-MH services decreased from 53.16 in FY20 to 51.39 in FY22. Racial and ethnic diversity increased over time, with Black (12.93% in FY20 to 19.75% in FY22), Asian (0.64% in FY20 to 1.37% in FY22), and Hispanic Veterans (7.87% in FY20 to 10.19% in FY22) representing an increasing volume of CRH-MH patients engaging in services. The percentage of Veterans who were female increased from 16.39 in FY20 to 19.86 in FY22, as did those who were unmarried (48.91% in FY20 to 50.96% in FY22) and living in urban areas (48.93% in FY20 to 62.4% in FY22).
In addition, the percentage of Veterans enrolled who required a copay due to means decreased (7.43% in FY20 to 6.69% in FY22), as did the percentage of Veterans enrolled in primary care (96.3% in FY20 to 93.46% in FY22). Driving distance to the closest VA primary care site decreased from FY20 to FY22, while the percentage of Veterans enrolled in community care increased from FY20 to FY22 (4.52–6.21% in FY22).
Mental health providers
In VA, a 1.0 “Full-Time Equivalent Employee (FTEE)” included a single full-time (40 h/week) employee or multiple part-time employees whose paid time sums to 40 h/week. Total CRH TMH FTEEs grew 433% from 95.6 FTEE in FY20 to 411.4 FTEE by FY20. There was an increase in full-time MH providers for CRHs between FY20 and FY22, with 37.9% of providers at 1.0 FTEE in FY20 and 63.1% in FY22.
The most common types of providers hired across all study years were psychologists (35.4 FTEE in FY20 to 122.1 FTEE in FY22), psychiatrists (22.5 FTEE in FY20 to 80.8 FTEE in FY22), and mental health social workers (17 FTEE in FY20 to 52.6 FTEE in FY22). Registered nurses, nurse practitioners, and peer specialists accounted for the remaining FTEEs. Notably, within each type of MH provider there was an expansion in the types of providers in CRH from year to year, and an increase in FTEE among all occupation types (Fig. 1).
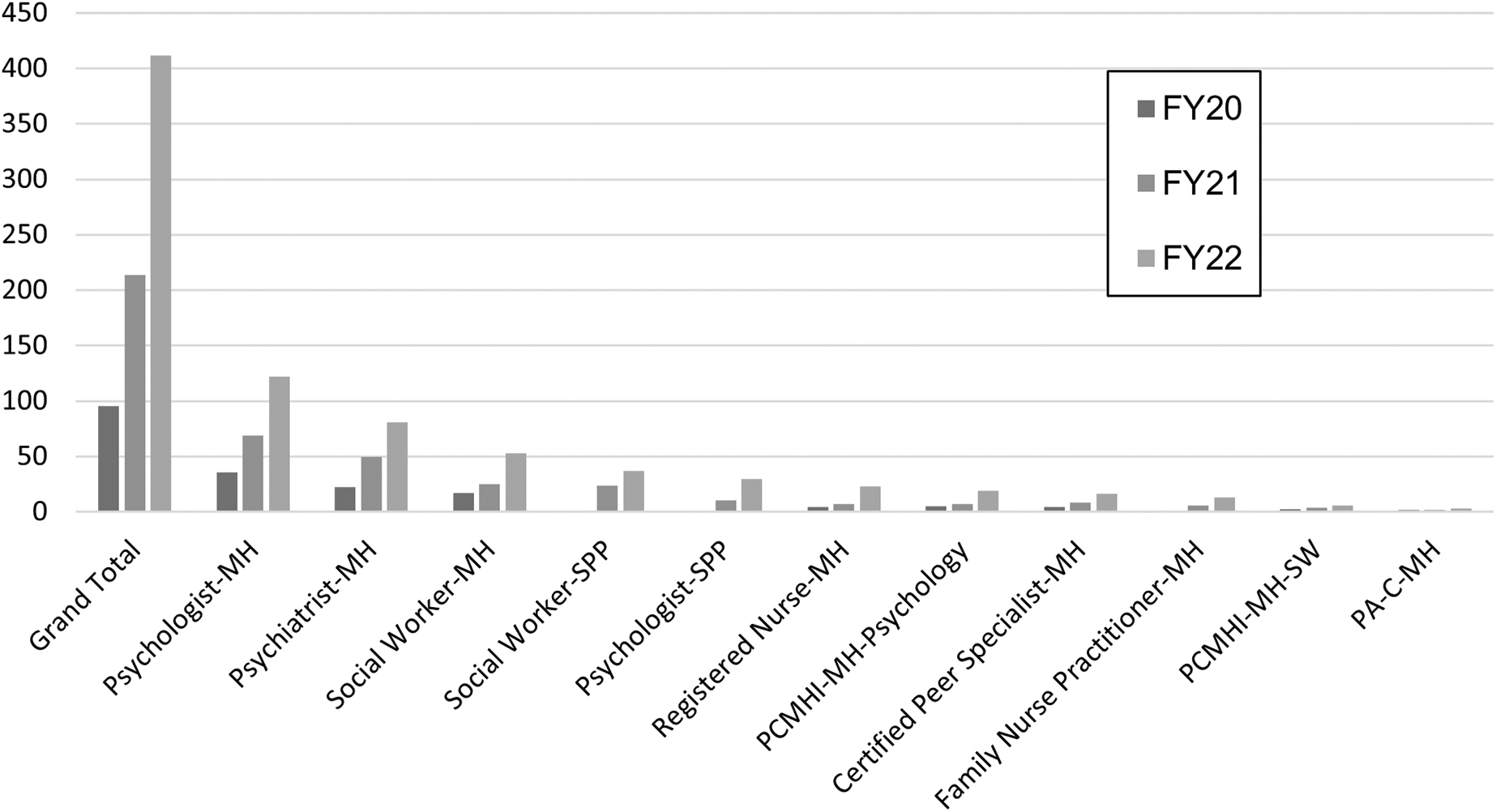
MH Providers FTE by type, fiscal year 2020–2022. FTE, full-time equivalent; MH, mental health; PCMHI, primary care mental health integration; SPP, service provider in psychology.
Mental health diagnoses
The most common comorbidities of patients utilizing CRH-MH services were depression (68.48% of mental health patients in FY20 to 65.03% of mental health patients in FY22), post-traumatic stress disorder (PTSD; 52.71% of mental health patients in FY20 to 52.35% of mental health patients in FY22), and anxiety (52.25% of mental health patients in FY20 to 56.34% of mental health patients in FY22). The distribution of mental health diagnoses remained approximately stable over the study period (Fig. 2).
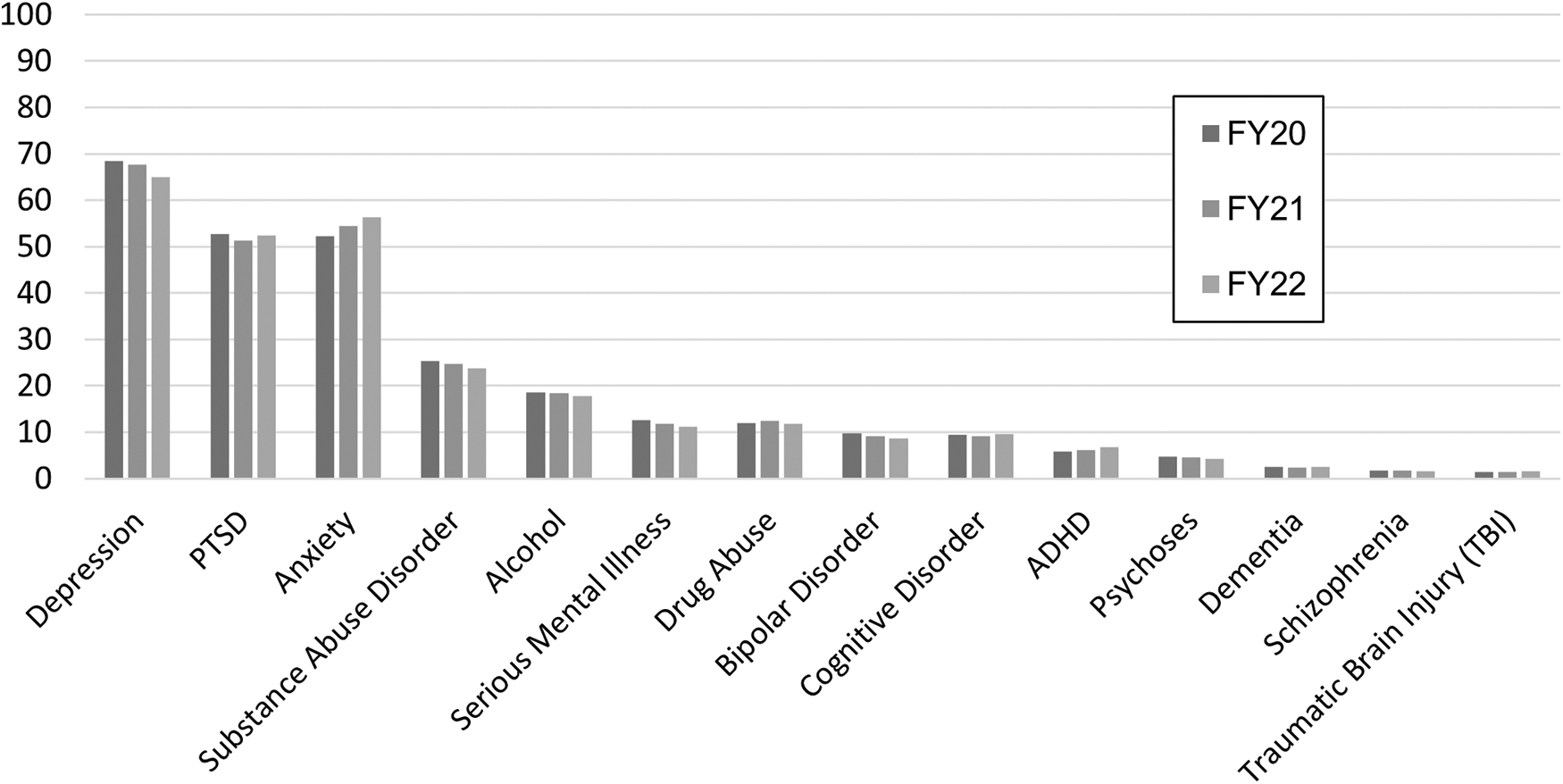
MH Diagnoses by FY, CRH Unique Mental Health Patients. ADHD, attention-deficit/hyperactivity disorder; CRH, community resource hub; FY, fiscal year; PTSD, post-traumatic stress disorder.
Urban versus rural
During the study period, the proportion of CRH-MH encounters that supported patients assigned to urban clinic sites versus rural sites increased with urban site patients accounting for 49% of encounters in FY20, and 62% in FY22 and from 45% in FY20, to 33% in FY22 for patients from rural sites. There was a 4-fold increase in CRH-MH utilization for Veterans at urban sites. CRH-MH encounters increased by 2.5-fold at rural sites, and 2-fold at highly rural or insular island sites. Although utilization expanded across all sites, after FY20 there was a more rapid expansion of CRH-MH services to urban sites when compared with rural or highly rural sites (Fig. 3).
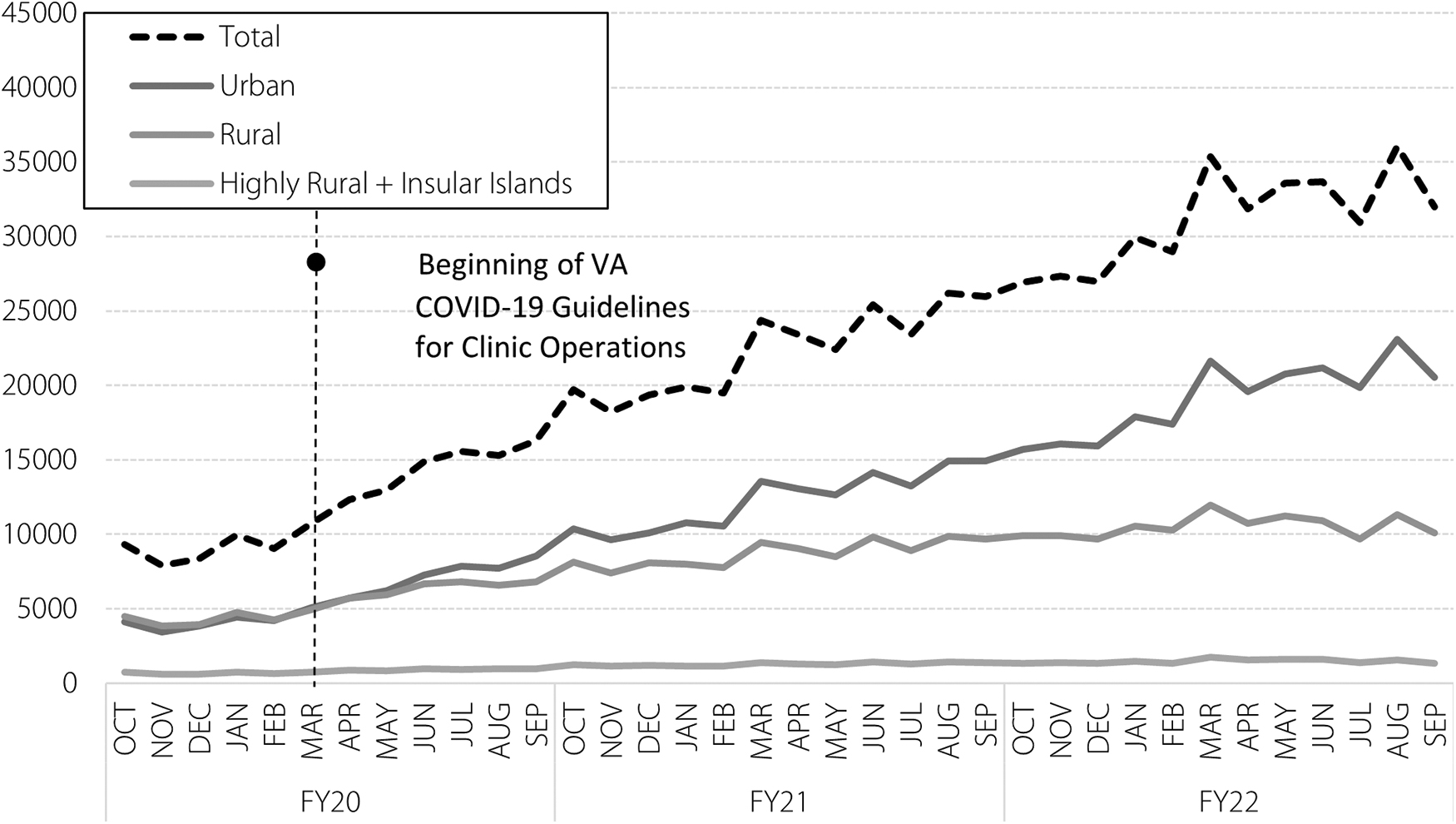
CRH-MH encounters by urban/rural, FY2020–2022.
Race and ethnicity
CRH-MH care increased among all races between FY20 and FY22. The proportion of Veterans utilizing CRH-MH decreased among Veterans identifying as White (79% in FY20 to 70% in FY22), remained stable among those identifying as Multi-Race (2.1% in FY20 and FY22), and increased among Veterans identifying as Black (13% in FY20 to 20% in FY22), Asian (0.6% in FY20 to 1.4% in FY22), and Other (3.1% in FY20 to 3.7 in FY22; Table 1). CRH-MH use increased among both Hispanics and non-Hispanics between FY20 and FY22. The proportion of Veterans identifying as Hispanics increased (7.9% in FY20 to 10.2 in FY22), while there was a decrease in the proportion of non-Hispanic Veterans (89% in FY20 to 83% in FY22; Table 1).
Demographics of Clinical Resource Hub-Telemental Health Patients, Fiscal Years 2020–2022
Statistically significant at the 0.05 level across FY.
FY, fiscal year; SD, standard deviation.
Care modality
The modality of care at CRHs underwent a shift between FY20 and FY22. Telephone encounters increased during the onset of COVID-19, but largely plateaued after FY20. There was a decline in Clinical Video Telehealth (CVT) to site encounters after March 2020, while VA Video Connect (VVC) encounters to patients home increased from FY20 to FY22, to become the predominant modality of care (Fig. 4).
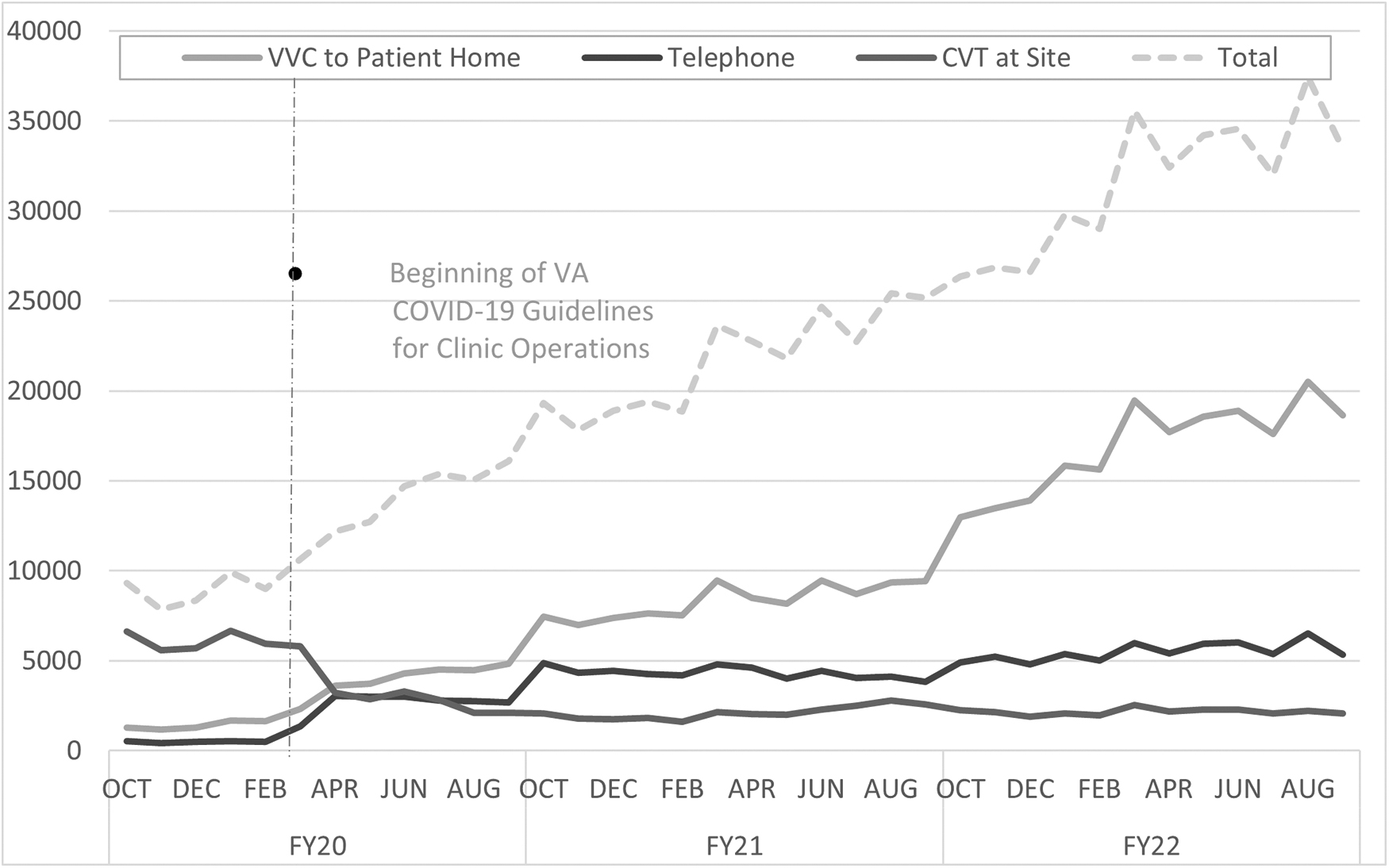
CRH-MH encounters by modality of care, FY2020–22. CVT, clinical video telehealth; VVC, VA video connect.
Discussion
This descriptive evaluation of the first 3 years of CRH-MH services suggests that virtual mental health care reached a diverse patient population and was adopted by a steadily increasing number of VA clinics, at both VA medical centers and at clinics based in the surrounding communities. While CRH-MH providers were able to deliver in-person care, the vast majority of care (98.1%) was delivered using TMH modalities, including video to clinic (CVT), video to home (VVC), and telephone-based care. With the onset of COVID, there was a shift away from CVT at site encounters and toward VVC to patient home encounters. This trend continued as the CRH-MH program expanded, and parallels the overall expansion of TMH services provided throughout the VA during this period. 17 –19
When looking at the number of unique Veterans receiving MH services, this care steadily increased as did the number of MH encounters between FY20 and FY22. However, there was variability between the clinics where MH services were delivered over time. The percentage of MH appointments at VA Medical Centers steadily increased, while the percentage of MH appointments at CBOCs steadily decreased between FY20 and FY22.
In terms of rurality status, care to urban clinics increased by 4-fold, while care to rural and highly rural sites increased by 2-fold over the same 3-year period. It is not clear why there was greater increase in the medical centers than in rural clinics. However, greater increase in urban versus rural VA clinics is consistent with prior research. Veterans in rural areas have been reported to access mental health care at lower rates for a variety of reasons that might also be related to Veteran perception of care. 19
CRH-MH services treat the same diagnoses and use the same MH staffing as traditional MH services in the VA, and the CRH-MH leadership team is not aware of any adverse outcomes specifically related to CRH-MH. When looking at unique patients engaged in CRH-MH services between FY20 and FY22, the top three diagnoses for each year were depression, anxiety, and PTSD, while the least commonly treated diagnoses were schizophrenia and dementia. These diagnoses are known to be highly prevalent in VA primary care clinics and are typically treated by primary care mental health integration (PCMHI) teams in combination with mental health specialty consultants. 20 –22
The number of mental health providers offering care through the CRH-MH teams continued to grow during this time, with a shift toward hiring more full-time providers. The most common providers were as follows: psychologists followed by psychiatrists, then MH social workers. Other mental health providers working in these clinics would include those specialized in PCMHI and providing suicide prevention. That psychologists followed by psychiatrists are the most common mental health providers providing TMH in CRHs parallels what is reported in overall VA TMH care delivery. 10
CRH-MH saw an expansion of services during our 3-year time period. This expansion was seen across patient groups that are traditionally marginalized in accessing MH services, including racial-ethnic minorities and patients from a lower socioeconomic status. Between FY20 and FY22, there was a higher percentage of Veterans who were non-White (Black and Hispanic), female, and living in urban areas. While those who self-identified as White or Multi-Race saw a 3-fold increase in utilization, those who identified as Black or Other saw a 5-fold increase, and those who identified as Asian saw a fourteen and half fold increase in CRH-MH utilization.
Similarly, CRH-MH use increased among both Hispanics and non-Hispanics between FY20 and FY22. Hispanics saw a 5.4-fold increase in care utilization, whereas non-Hispanic Veterans saw a 3.25-fold increase in CRH-MH care utilization. These increased rates of TMH use in Veterans who identify as non-White are consistent with other reports, stating that racially and ethnically diverse samples of Veterans report positive views of TMH and would recommend it to others. 23
For Veterans accessing telehealth, it has been reported that there have been minor differences in use of virtual care by race or ethnicity, while another recent report with a small sample size and effect sizes suggests that during COVID most ethnic groups defined as Black, Indigenous, and People of Color remained the same or increased except for American Indian or Alaska Native Veterans for whom TMH utilization rated decreased during COVID. 23,24 Similarly, we found CRH-MH service use to increase during COVID across racially and ethnically diverse groups, with increased utilization among these groups from year to year when compared with White or non-Hispanic Veterans.
Limitations
In terms of limitations, there are several that need to be highlighted. First, this report relied on administrative data sets. Future research using survey or qualitative investigation is needed to understand what the barriers and facilitators to receiving CRH-MH care are. Second, this report provides initial descriptive data on the implementation of the CRHs, and cannot comment on the quality of care or other processes used to implement these TMH services.
Third, while we can describe the makeup of CRH-MH teams, we cannot assess staff attrition across the national CRH network due to limitations in available human resources data, although this is a possible area of future research. Despite this shortcoming, the overwhelming trend observed is a consistent growth in CRH staffing for mental health services since the inception of the program, as depicted in Figure 1. While there were regional differences in the adoption of this program, some of the variation was due to program history in terms of participation in a prior pilot study, limiting conclusions about regional variation.
Finally, it is important to remember that the CRHs only provide a small fraction of the TMH services delivered through the VA system, so conclusions drawn from these administrative data on the implementation of the CRH-MH teams cannot be extrapolated to comment on overall TMH provided by VA.
Conclusions
This report summarized descriptive quantitative administrative data collected in the first 3 years of CRH-MH implementation. Based on these data, CRH-MH teams were implemented using predominantly TMH rather than in-person care, provided care for common mental health diagnoses throughout the VA on a national level, and provided care to traditionally marginalized patient populations. Care to rural populations increased, but not as much as care for urban or medical center-based clinics.
Future work will focus on the impact of CRH-MH care at the local clinic level and the clinical effectiveness of the CRH-MH teams. While our study utilizes VA data and focuses on the context of CRH programs within the VA, the systematic approach to TMH, the infrastructure for remote care provision, and the strategies for addressing staffing challenges could be relevant to other settings, especially those serving dispersed or underserved populations.
Footnotes
Acknowledgment
The authors thank Emily Ashmore for her assistance with data visualization.
Disclaimer
The views expressed are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded by the Department of Veterans Affairs Veterans Health Administration, through the VA Office of Rural Health and the VA Office of Primary Care.