
Abstract
Introduction:
Robot-assisted visits, as part of telemedicine, can offer doctors the opportunity to take care of patients. Due to the COVID-19 pandemic, there has been an increase in telemedicine. The use of teleconsultations, for example, has found its way into the German health care system. However, the practicability and the benefit of robot-assisted postoperative visits have not been systematically investigated in any study worldwide.
Methods:
Patients were enrolled in a prospective randomized study comparing the standard postoperative visit with the doctor on call and the digital visit through the Double robot between December 2019 and April 2022. All patients and doctors completed a survey after the visit. The primary outcome was patient satisfaction. Secondary outcomes included patients’ pain, hospitalization time, and patients’ opinions about the usefulness of the robot. Likert scales of arithmetic mean, standard deviation, and subgroup analyses with the Mann–Whitney U test and the Fisher’s exact test were used to compare outcomes.
Results:
We enrolled a total of 106 patients: 54 (50.9%) of them underwent the robot visit and 52 (49.1%) underwent the conventional visit. Baseline demographic and clinical characteristics were similar between groups. Our primary outcome was the same in both arms. Similar results were obtained for the secondary endpoints.
Conclusion:
Robot-televisits were comparable with standard visits including satisfaction, usefulness, and time of hospitalization. Digitalization in medicine is an irreversible process, especially after the COVID-19 pandemic. We hope that our study will provide concrete help to encourage the allocation of funds for telemedicine in Germany’s health care system.
Introduction
Robot-assisted visits, as part of telemedicine, can offer doctors the opportunity to take care of patients even from a distance. Telemedicine is defined as “the delivery of health care where distance is a critical factor, by all health-care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries all in the interests of advancing the health of individuals and their communities.” 1 Even though technological innovations have eased the expansion of the supply of telemedicine services in recent years, 2 demand has not been as strong as expected.
In 2020, the COVID-19 pandemic led many governments to impose lockdowns and social‐distancing policies, which induced patients around the world to experience telemedicine for the first time. 3 The rapid spread of cases made the utilization of telemedicine essential to minimize contact and mitigate the transmission of cases as well as cutting down costs and decreasing the time consumed during in-person visits. 4 Therefore, there has been a promotion and an increase in telemedicine, especially in video consultations, because it promotes social distancing measures and helps medical centers manage prolonged waiting times and risk of disease progression. 5
However, the use of telemedicine was not homogeneous across the various countries hit by the pandemic. Teleconsultations, for example, have found their way into the German health care system. Recently, Germany has introduced a separate billing code for resident doctors. For the first time, you can bill teleconsultations. The patient no longer has to come to the doctor’s office but can meet the doctor digitally and discuss therapy options. Teleconsultations are particularly advantageous for patients who have difficulty accessing medical care structures. Extensive studies have been conducted on their use, and they have proven valuable in these situations. The demonstrated benefits of telemedicine include reducing unnecessary clinical visits, providing more timely care and expanding access to underserved communities. 1 Although telemedicine offers opportunities to expand enhanced access to health services, its implementation must be guided by careful reflection of regulatory and strategic frameworks to mitigate potential risks and harms and to maximize its sustainability within the health sector. 1
In every medical sector, telemedicine could find a lot of applications with numerous time and cost advantages. 6,7
Telecommunication can also be an important asset in improving patient care in hospitals. As medical teams are not available 24 h a day, transfers between them are necessary, and the flow of information between doctors and patients is sometimes not firsthand but through third, even fourth parties. Furthermore, introducing teleconsultations means facilitating handover. For example, in recent years, telemedicine has been adopted in several domains of surgical care, including preoperative and postoperative care. 8,9
Recently, postoperative robotic telerounding, introduced as service robotic technology, has evolved for human−robot interaction with vision and sound information. Robotic telerounding increases accessibility, reduces inconvenience, and improves cost-effectiveness by reducing labor cost. 10
However, the practicability and benefits of robot-assisted postoperative visits for patients have not been systematically investigated in any study worldwide. Most reported postoperative telemedicine studies, which were conducted in subspecialties such as general surgery, urology, plastic surgery, neurosurgery, and obstetrics and gynecology, 8,11 –15 were performed from the surgeon’s office to another medical facility (e.g., clinics or hospitals) with the nurse’s presence to aid the patient 16 or directly to the patient’s home. 17
Until today, the feasibility and the benefits of a robot-assisted visit have not been analyzed in any study.
Ours is a prospective randomized study, the only one of its kind in the field of gynecology, aiming to report the results of telemedicine consultations for postoperative care via robot and compare them with in-person visits after gynecological surgery.
The study began on December 12, 2019, and we conducted it in two phases because of the COVID-19 pandemic. The pre-coronavirus period spans from December 2019 to February 2020, and the post-coronavirus period is from March 2020 to April 2022. In the initial era of the pandemic, we had to suspend patient recruitment from March 2020 to January 2022 for safety reasons and because of a lack of human resources in our gynecological department.
Our hypothesis is that telemedicine consultations could be associated with greater patient satisfaction, potentially leading to reduced pain and so shorter hospitalizations.
Methods
Patients were enrolled in a prospective randomized study comparing the standard postoperative visit and the digital visit through a robot during a period from December 2019 to April 2022. During the preparatory visit, patients were randomized with an application called “Roundom” after signing the informed consent. This research was approved by the Ethics Committee of the Medical Association Berlin (DRKS-ID of study: DRKS00032896).
INCLUSION AND EXCLUSION CRITERIA
The inclusion criteria for the study consisted of being treated in the gynecological surgery department for a benign disease without severe complications (defined as complications greater than or equal to grade 2 according to Clavien–Dindo), having an age between 18 and 80 years, and providing clarification and written consent.
The exclusion criteria were refusal to participate, carcinoma diseases, and serious illnesses that result in restricted participation, with a Karnofsky Index of <80 and an ECOG ≥2.
Patients who met these criteria were offered the opportunity to enroll in the study by the surgeon in charge during their preoperative consultation. If they agreed, they provided informed consent, and on the day of the surgery, they were assigned sequentially to the corresponding group. The allocation was performed using a computerized block randomization program with an allocation ratio 1:1.
INTERVENTION
The robot-assisted visit was performed with the “Double robot.” It offers the possibility to be moved through the clinic from the outside and can be connected to a screen. As a physician, this autonomous movement creates a sense of being part of the scene and enables effective interaction with the patients.
Data protection was ensured through the robot system used, and its implementation in the pilot project was conducted in close consultation with Mr. Koeppe, the Head of Data Protection at Vivantes.
The teleconferencing circuit utilized in the study was secure and developed in the United States specifically for the teleconferencing industry. To prevent industrial espionage, the system used end-to-end encryption and had a pronounced firewall. The manufacturer data emphasized secure communication: Double uses the WebRTC standard for video and audio, ensuring encryption and constant security. The encryption used utilizes AES cipher with 128-bit keys for encrypting audio and video, along with HMAC-SHA1 to verify data integrity. Video and audio connections are end-to-end encrypted and peer-to-peer whenever possible.
The gynecological surgeons carried out their daily operations, and the postoperative consultations were performed in two ways based on randomization.
For the standard postoperative visit, the workflow was as follows: Day 1: Operation Day 1: Afternoon or evening postoperative consultation with the doctor on call Day 2: Fill out the questionnaire in the morning Day 2: Clinical round/discussion with the surgeon
For the robot-assisted visit, the workflow was as follows: Day 1: Operation Day 1: Afternoon or evening consultation with the surgeon through the “Double robot” Day 2: Fill out the questionnaire in the morning Day 2: Clinical round
The questionnaires for the surgeons and the patients were developed by the Institute for Patient Satisfaction at Hannover Medical School and were used as the standard for patient surveys. Some of the questions were developed at the Department of Medical Psychology and Psychotherapy, University of Graz (Figs. 1–2).
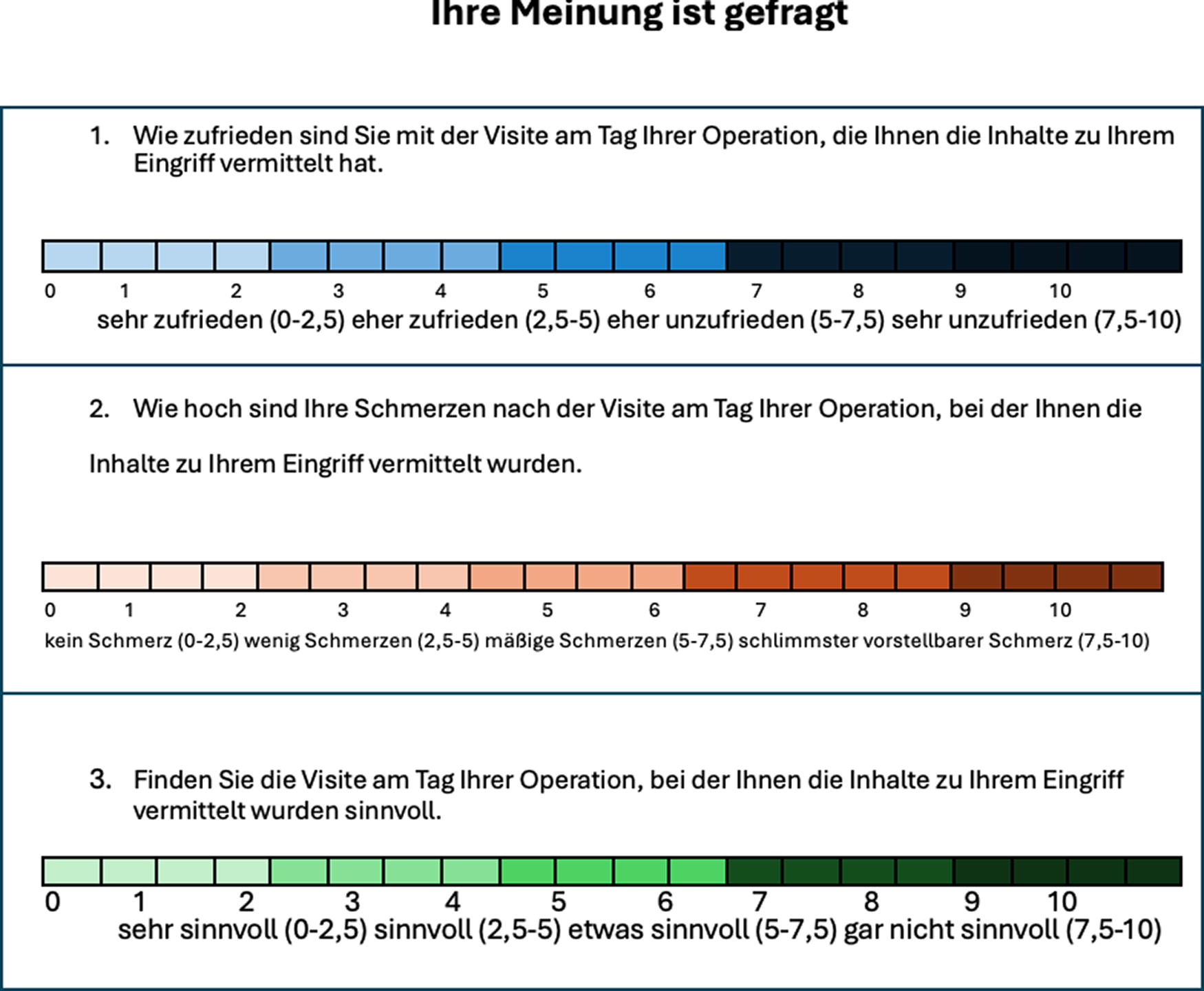
Patient’s questionnaire.
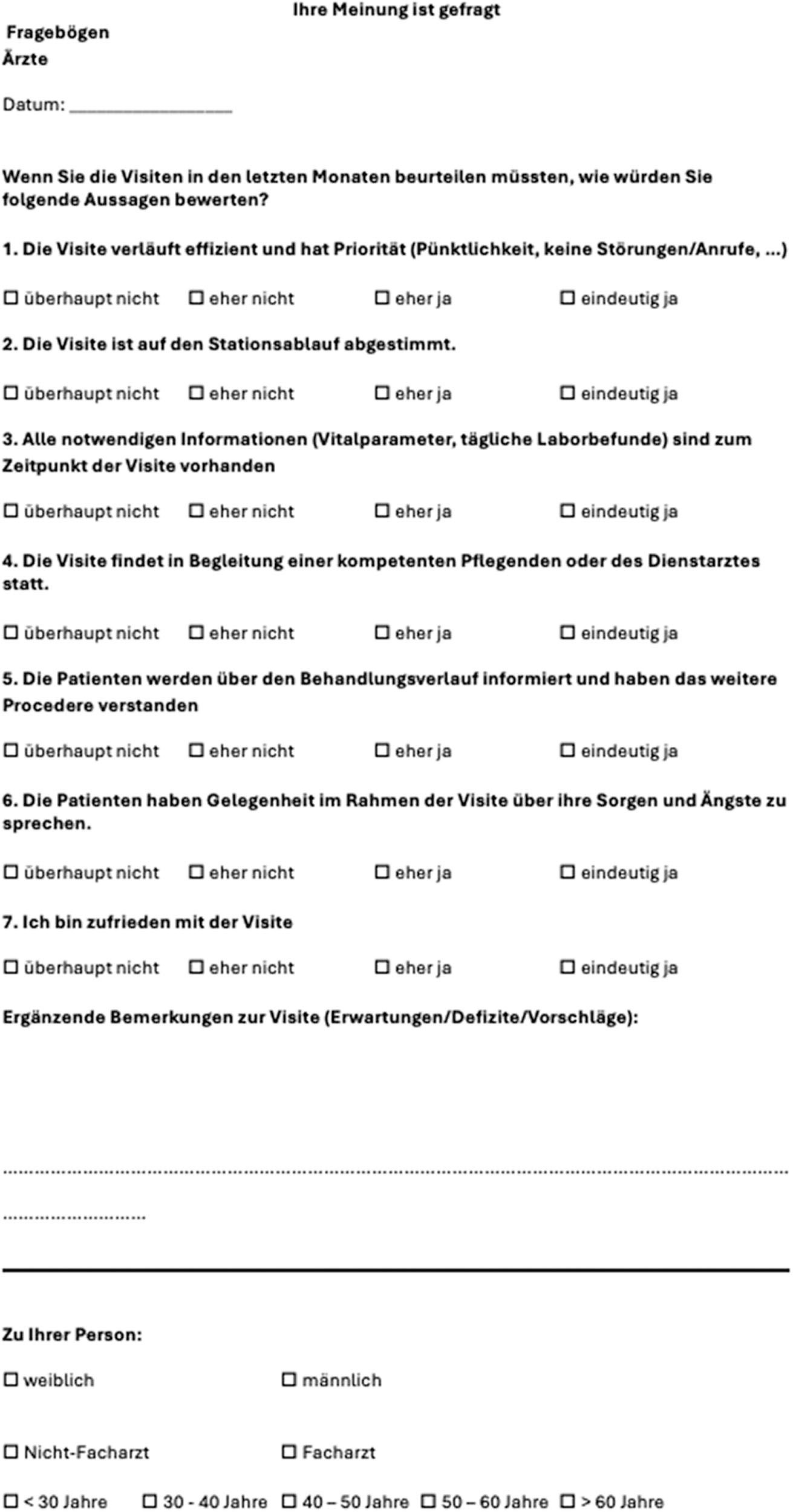
Doctor’s questionnaire.
STUDY OUTCOMES
The primary outcome measure was patient satisfaction, assessed on a Visual Analog Scale (VAS) ranging from 0 to 10, comparing patients who received additional robot visits to standard patients (see Fig. 1).
The secondary outcomes included patients’ pain levels, measured on a VAS ranging from 0 to 10, hospitalization duration in hours, and patients’ opinions regarding the usefulness of the robot visit, measured on a VAS from 0 to 10 (Fig. 1).
In addition, we assessed various parameters, such as information flow. We hypothesized that there could be changes in the information flow, which could lead to clinical changes, such as an accelerated recovery phase. We also expected changes in the process, potentially resulting in shortened hospitalization periods or improvements in clinical parameters, such as pain reduction. Transaction flow, including the costs incurred not only in financial or personal terms but also in terms of time resources, was also taken into account.
The questionnaires served for evaluation and the analysis of the parameters. The involved doctors also received and completed a questionnaire regarding their visits and related satisfaction (Fig. 2).
STATISTICAL EVALUATION PLAN
A total of 106 patients, 54 in the robot-assisted visit group and 52 in the standard postoperative group, were included in the study. Data evaluation was conducted descriptively using the statistical program IBM® SPSS® Statistics 24, which was also utilized for data recording and management.
The demographic data, intentionally kept concise to preserve anonymity, were initially presented as simple frequency distributions (absolute and relative frequencies).
Each item in the survey instrument was coded numerically, and assuming an equidistance of the levels on the Likert scales used, arithmetic mean and standard deviation were calculated. Subgroup analyses were performed based on demographic variables such as age and diagnosis.
For subgroup comparisons, the Mann–Whitney U test was used as a nonparametric test method, and for groups with low sample sizes, the Fisher’s exact test was used for comparisons.
For all mentioned methods, a significance level of p < 0.05 was considered statistically significant, without applying Bonferroni correction.
Results
PATIENT POPULATION
We enrolled a total of 106 patients between December 2019 and April 2022. Out of these, 54 (50.9%) underwent the robot visit, whereas 52 (49.1%) underwent the conventional visit (see Fig. 1). During the pre-coronavirus period, 25 patients were enrolled in the robot visit group and 13 in the standard visit group. In the post-coronavirus period, 29 patients were enrolled in the robot visit group and 39 in the conventional visit group (Fig. 3).
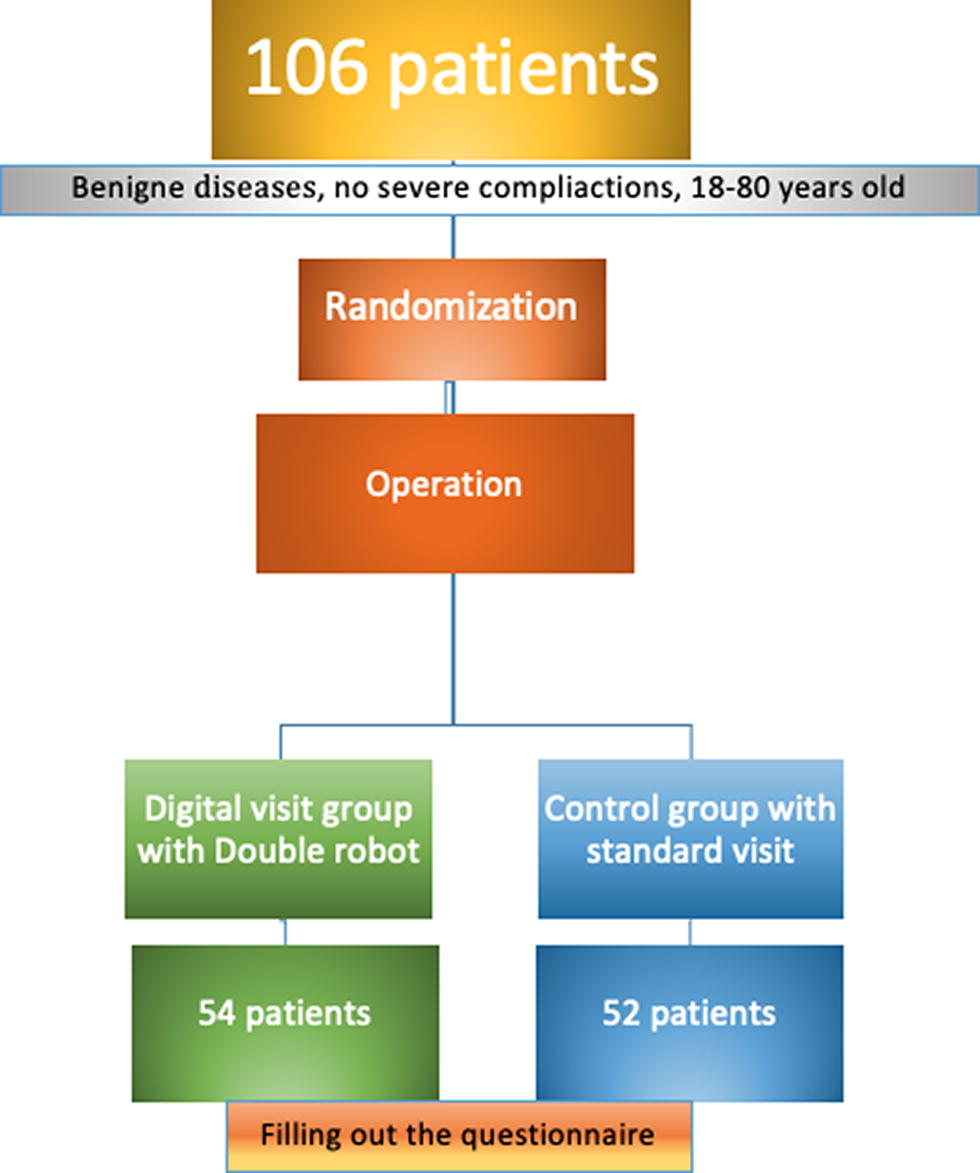
Study design.
In the robot visit group, there were technical problems that prevented the visit from being performed in six cases (11.1%), whereas in the conventional visit group, the visit was not performed in only one case because of the doctor’s lack of availability (1.9%).
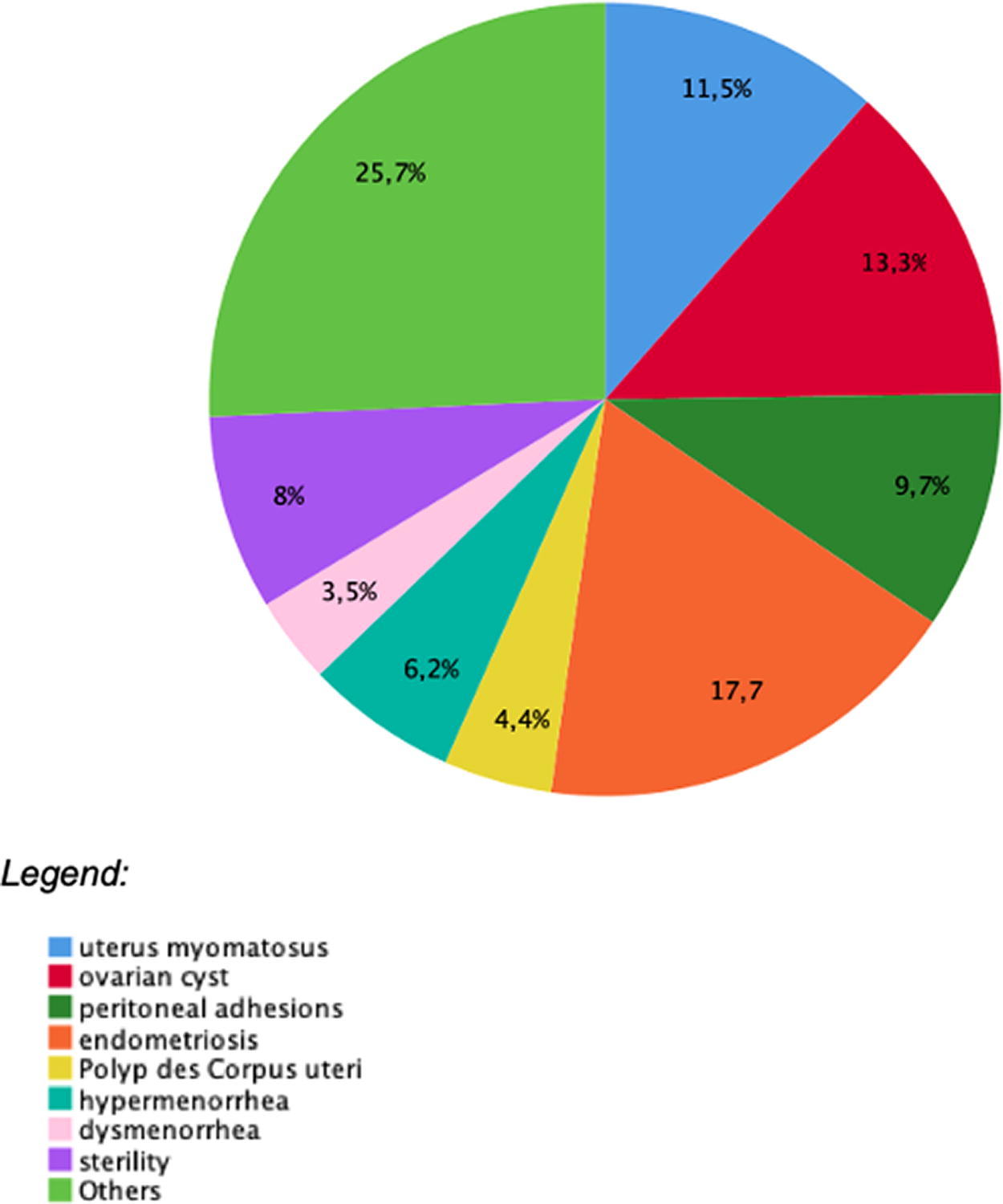
Baseline demographic and clinical characteristics were generally similar between groups (Figs. 4–7). The overall mean age ranged from 30 to 40 years in both the robot visit group (31.5%) and the conventional visit group (28.8%) (Figs. 4 and 5).
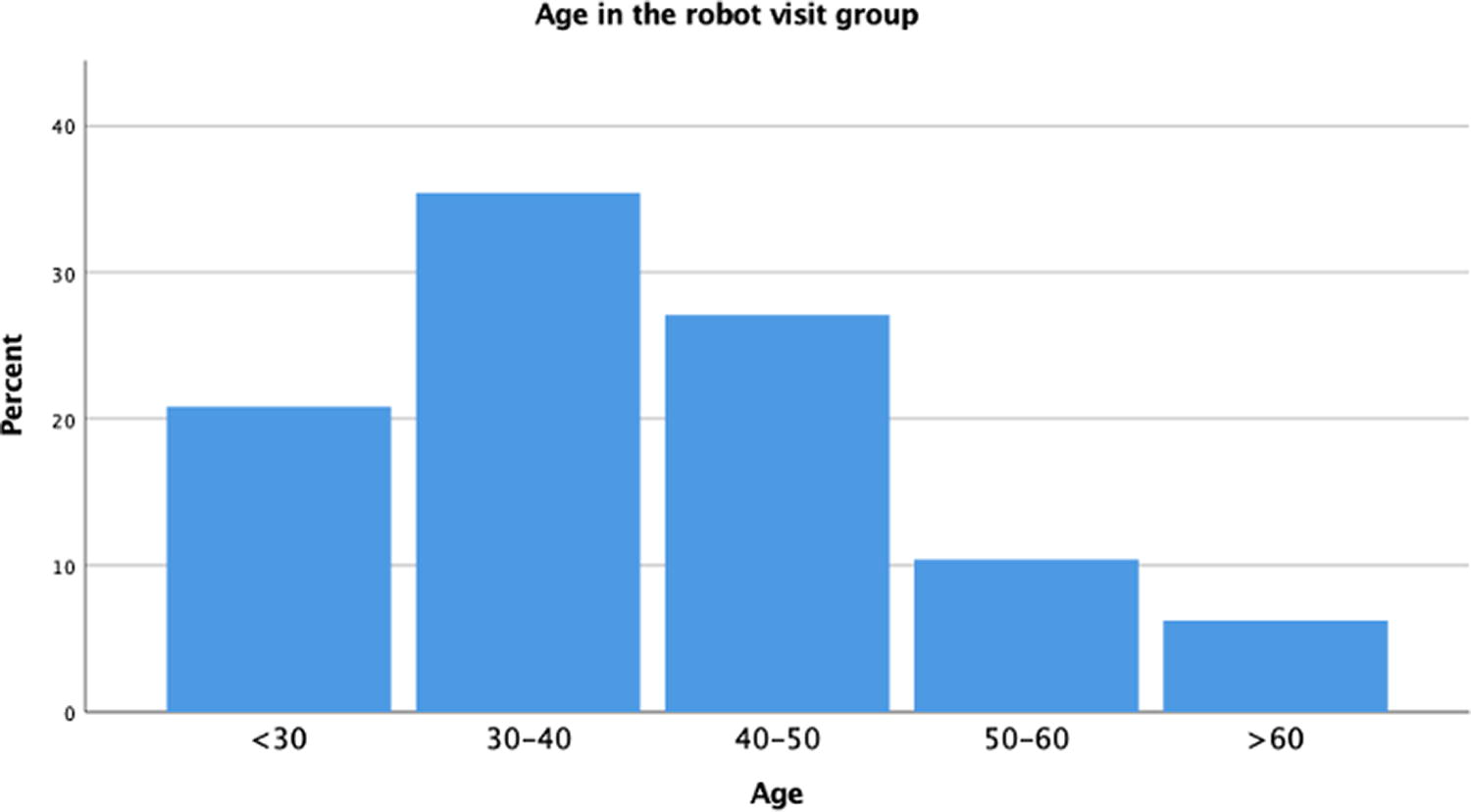
Frequencies of the patients’ age in the robot visit group.
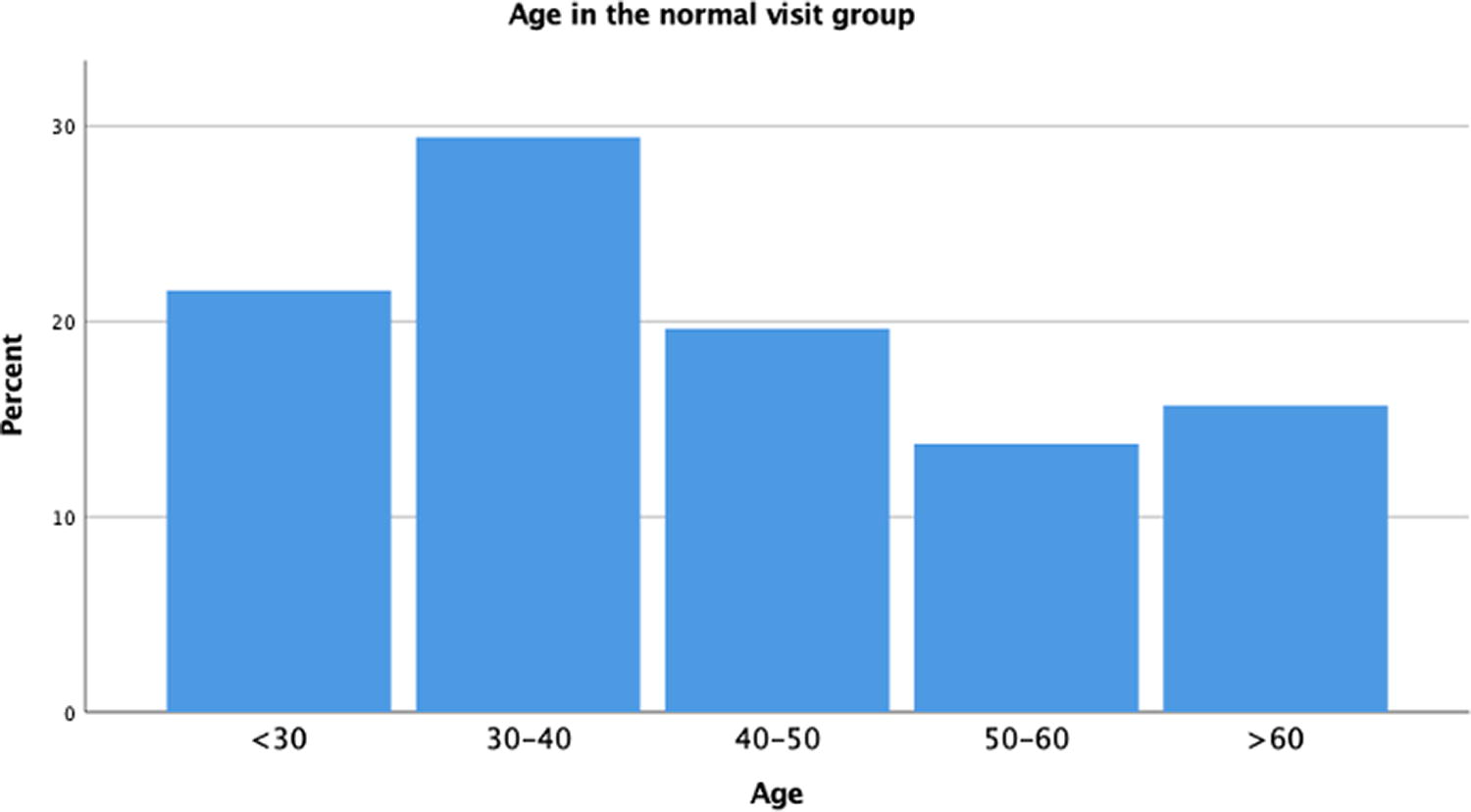
Frequencies of the patients’ age in the normal visit group.
Frequencies of diagnosis in the robot visit group.
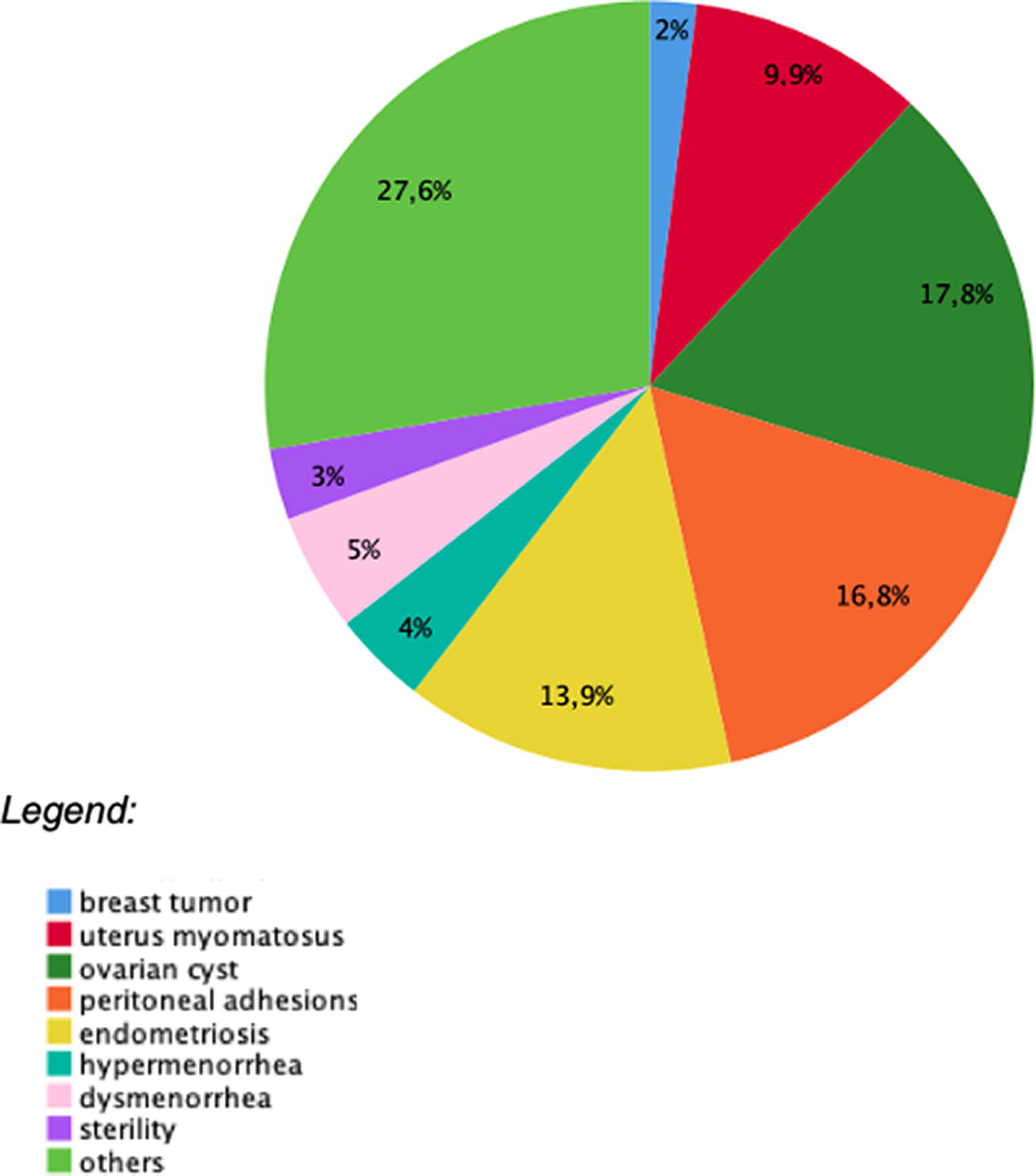
Frequencies of diagnosis in the normal visit group.
DOCTOR POPULATION
In both groups, the majority of doctors were female (80% in the robot visit group and 96% in the conventional visit group), and most of them were medical specialists (78% in the robot visit group and 90% in the conventional visit group). However, the mean age differed between the two groups, with the robot visit group having a mean age of 40–50 years (42%) and the conventional visit group having a mean age of 30–40 years. The reason is that most operations are conducted by experienced specialist doctors and postoperative visits are normally conducted by the doctor on duty.
PATIENT SATISFACTION WITH TELEMEDICINE
The primary outcome measure was patient satisfaction among those who received additional robot visits, assessed on VAS ranging from 0 to 10 (Fig. 1), compared with patients who had standard visits. No differences were observed between the two groups (Table 1).
Primary and secondary outcomes
Patients’ number.
Satisfaction scale: very satisfied (0–2.5), rather satisfied (2.5–5), rather unsatisfied (5–7.5), very unsatisfied.
Postoperative pain: no pain (0–2.5), little pain (2.5–5), moderate pain (5–7.5), worst pain immaginable (7.5–10).
Usefulness of the visit: very useful (0–2.5), useful (2.5–5), something useful (5–7.5), not at all useful (7.5–10).
Patients were also asked to express their confidence in the visit and the quality of treatment: in the pre-coronavirus era, 60% of patients had “rather great trust” in the robot visit, and 60% rated the quality of treatment as “rather high.” In the post-coronavirus era, the confidence level increased to “great” in 58.6% of patients, and the quality of treatment was rated as “very high” by 57.1%. The overall experience with the visits was found to be identical in both groups, both in the pre-coronavirus era (p = 0.346) and the post-coronavirus era (p = 0.752) (Table 1).
SECONDARY OUTCOMES
We anticipated that the robot visit group would show improvement in clinical parameters, such as a reduction in pain, because of better satisfaction with the visit. However, the patients reported a similar moderate level of pain in both groups. The pre- and post-coronavirus p-values were not statistically significant (n.s.).
Furthermore, the hospitalization time in hours was also very similar between the two groups. This indicates that our assumption of an accelerated recovery and shortened hospitalization period in the robot visit group was not confirmed by our results.
Regarding the usefulness of postoperative consultations, measured in VAS ranging from 0 to 10 (Fig. 1), patients in both groups reported similar results. The p-value was not statistically significant in both the pre- and post-coronavirus periods (p = 0.744 in the pre-coronavirus era and p = 0.690 in the post-coronavirus era).
The distribution of satisfaction among doctors with the visits was identical in both groups. There were no statistically significant differences between the two groups in both the pre- and the post-coronavirus periods (Table 1).
Discussion
The evolution of surgical care should continue to focus on providing the highest quality patient care with a high degree of patient and provider satisfaction, meanwhile allowing the greatest access to surgical care. Telemedicine in postoperative care appears to attain these goals and should be considered as a viable option for health care centers. 18
Nowadays, and even more so in the post-coronavirus period, the hospital system needs digitalization. Teleconsultation is a crucial component of this process, serving as a substitute for or an integration to face-to-face visits.
Our study stands as the only prospective randomized study that evaluates patient and doctor satisfaction and the usefulness of postoperative consultations in a gynecological cohort. The results are highly interesting and carry significant implications for clinical practice. We have demonstrated the effectiveness of robot-assisted visits in clinical settings, considering that both patient and doctor satisfaction levels were equal in both groups.
In addition, we hypothesized that satisfaction with televisits would be higher in the post-coronavirus era because of increased need and improved confidence in the utilization of digital health. However, our results revealed no significant differences between the pre- and the post-coronavirus periods in terms of satisfaction levels.
The results pertaining to the significant comparability between robot-assisted postoperative visits and standard visits are particularly valuable, as they offer an alternative system to address challenges within the national health care system. These challenges include staff and time constraints, as well as the increasing number of patients in need of treatment.
Regarding the secondary outcomes, we hypothesized that there would be an accelerated progression into the next phase of healing and consequently a shorter hospitalization time. However, this did not occur as the satisfaction with the visits was equal in both groups.
Furthermore, through this study, we aim to promote the digitalization process in German hospitals. The implementation of robot-assisted visits with the “Double robot” does not require specific training and is user-friendly for everyone, regardless of their location.
LIMITATIONS
Technical problems with the robot visit, such as internet connection issues, occurred in only 6 out of 106 cases. In such situations, we recommend exploring alternative solutions, such as a simple video phone call and this would also tie up less staff. In addition, it is important to note that teleconsultation may not be suitable for every type of conversation or interaction.
Conclusion
In conclusion, robot-televisits were found to be comparable with standard visits in terms of satisfaction, usefulness, and hospitalization time. The digitalization of medicine has become an irreversible process, particularly accelerated by the COVID-19 pandemic. The German health care system is actively supporting this transition, and we anticipate that our study will provide tangible support in advocating for the allocation of funds toward telemedicine initiatives.
Footnotes
Acknowledgments
The authors greatly thank all the participants involved in this trial and really appreciate the contribution of their colleagues of the Department of Obstetrics and Gynecology of Vivantes Auguste-Viktoria-Klinikum for their skilled assistance in enrolling patients and collecting clinical data.
Authors’ Contributions
G.P.: Conceptualization, data curation, formal analysis, investigation, methodology, visualization, and writing original draft. T.H.: Software, supervision, validation, writing, reviewing, and editing. J.S.: Visualization, investigation, and supervision. F.J.: Investigation and validation. V.P.: Investigation and validation. M.G.: Investigation and validation. M.M.: Conceptualization, investigation, methodology, project administration, writing, reviewing, and editing.
Data Sharing Statement
Raw data are not publicly available to preserve individuals’ privacy under the European General Data Protection Regulation.
Disclosure Statement
The authors have no conflicts of interest or financial conflicts to disclose.
Funding Information
Authors state no funding involved.