
Abstract
Introduction:
One of the challenges faced by the Colombian Health System is to improve access to health services for the dispersed and isolated rural population, particularly in the field of dermatology. This article examines the implementation of a teledermatology service using a PC and camera versus smartphone technology.
Methods:
A total of 542 teledermatology visits were conducted, involving 478 patients, in addition to 64 visits for clinical follow-up for patients as per the dermatologist's recommendation. Out of the 478 patients, 461 met the inclusion criteria and agreed to participate in the study. The data collection instrument from the general practitioner or referring provider covered three consultation moments: (1) sending an initial consultation, (2) providing a response to the patient, and (3) sending a follow-up consultation. Seven hundred forty-seven records were completed by the general practitioner for the three consultation moments. Furthermore, 372 consultations were documented by the dermatologist or referring provider for two moments: (1) response to the initial consultation by the dermatologist, and (2) response to the follow-up consultation by the dermatologist. After validating the information reported in the instruments, a descriptive analysis of the data was conducted, utilizing absolute frequencies and percentages for qualitative variables and measures of central tendency (mean, median, standard deviation, and interquartile range) for quantitative variables. The data were analyzed from 747 records of the referring provider instrument related to 461 patients, between 18 and 98 years of age, with a predominantly female representation.
Results:
The results indicated that for teleconsultations conducted using a mobile device, the average total duration of the teleconsultation was longer on the traditional platform compared with the mobile device (13.03 vs. 8.27 min). Additionally, it was observed that the time taken to store, send, and capture a single image (clinical or dermoscopic) using the mobile device was three times lower than that on the conventional platform (25 vs. 75 s). Similar findings were noted for teleconsultations carried out by the dermatologist, predominantly utilizing a mobile device. The average consultation time was shorter for the mobile device compared with the traditional platform (8.14 vs. 12 min).
Conclusions:
The cost reduction suggests that the operation of the service is more efficient with smartphone technology in comparison to the use of a PC and camera. Teledermatology with smartphones provides a streamlined, efficient, and technically sound process for obtaining clinical and dermoscopic images.
Introduction
Teledermatology has a long and effective history in providing remote and virtual treatment for patients with skin problems, enhancing access to health care in geographically remote areas. 1,2 Traditionally, teledermatology has been conducted using asynchronous communication (store-and-forward) with a desktop computer and a photographic camera (PC&C) to capture and send clinical data and images from a general practitioner to a dermatologist for evaluation and treatment recommendations. The dermatologist's response is then relayed back to the family doctor, who implements the recommended course of action. While this model offers cost savings for patients, it is not always economically viable for health care providers, 3 –5 as it requires significant resources for implementation and operation. As a result, teledermatology using PC&C, despite being accepted and validated, has not become widely adopted due to its lack of economic viability. 6
In contrast, the use of smartphones in dermatology, also known as mobile teledermatology, 7 has gained significant interest due to its enhanced portability, ease of use, and the convenience of having a single device with both camera and computer capabilities. 8 The current study compares the startup and delivery of teledermatology services using PC&C and smartphone technology through a Cost Minimization Analysis (CMA). Before conducting the research, a Cost-Effectiveness study was ruled out, as it was determined that the effectiveness of teledermatology is comparable when using both PC&C and smartphones. 9 –12 The CMA is a partial economic evaluation that quantifies the associated resources under the assumption of equivalent therapeutic effectiveness for the alternatives being evaluated.
Methods
Sample
This study conducted a CMA analysis from the perspective of a hospital institution, focusing on patients with dermatological conditions from three public primary care hospitals in the department of Caldas (Chinchiná, La Dorada, and Samaná) in Colombia. The informed consent form for teledermatology care SA-TLD-FO-001 was completed for each patient. The project was approved by the Scientific Committee and Research Ethics Committee of the Centro Dermatologico Federico Lleras Acosta in 2017.
Intervention
Teledermatology health care was provided using Smartphone technology (Huawei P30® with triple Leica 40 MP +16 MP +8 MP camera and DermLite® magnetic adapter) and compared with the use of PC&C technology (Lenovo IdeaPad Computer®, Intel Core i5 processor, 14” screen with 1366 × 768 pixel resolution, 8 GB DDR4 Sony DCS-W800® camera with dermatoscopy adapter). The dermatologist utilized the same DermLite DL200 Hybrid® dermatoscopy and a computer (iMAC®) to evaluate the consultations. The study incorporated direct costs associated with patient care using PC&C and Smartphone technology within a time horizon of less than one year, without any adjustments for discount rates.
Data collection
Data were collected through three direct cost instruments (fixed and variable) related to the medical personnel required for patient care, equipment, and general costs for the implementation and delivery of teledermatology services, using both PC&C and Smartphone.
The first instrument focused on medical personnel (#1 instrument), capturing time variables at three different stages of the consultation using PC&C and Smartphone technology. Moment 1 (m1) measured the time invested by the general practitioner in providing care, collecting data, capturing, storing, and delivering clinical and dermoscopic images. Moment 2 (m2) measured the time invested by the dermatologist in evaluating and responding to the consultation (case analysis, diagnosis, and treatment). Moment 3 (m3) measured the time spent by the attending physician in providing a response and treatment to the patient.
Communication between the general practitioner and dermatologist occurred asynchronously through two different software programs: XROL® for PC&C and Telederma® from the Hospital Universitario Centro Dermatológico Federico Lleras Acosta E.S.E (HUCDFLLA) for Smartphone use. The second instrument (#2) focused on equipment, including desktop and laptop computers, cameras, Smartphones, and dermatoscopes with adapters. The third instrument (#3) encompassed general costs such as legal framework, public services, physical space, security, cleanliness, maintenance, furniture, equipment installation and network configuration, training, server, teledermatology software, and administration.
Inclusion criteria
The study included patients of legal age with dermatological diseases who did not have a confirmed diagnosis by a specialist at the start of the study. These patients were referred from primary care services for dermatology evaluation. Additionally, patients had to provide informed consent for telemedicine care and agree to participate in the research. Patients who declined to participate were still offered clinical care but were not included in the study. Evaluations of patient satisfaction were conducted during m1 and m3 to ensure the quality of care. Attending physicians and participating dermatologists received training in the use of PC&C and Smartphone equipment and the teledermatology platform.
Statistical analysis
To estimate the approximate cost of using equipment and devices in each consultation, the concept of Equivalent Annual Cost was applied. This method, used for financial evaluation of investment projects, converts income and costs into an equivalent annual sum, considering discount rates when applicable. In equation 1, the variable K represents the initial disbursement, r represents the interest rate, and n represents the number of periods or years of useful life.
Finally, all calculations were conducted to determine the value of patient care using both PC&C and Smartphone, based on the investment and operating costs of the teledermatology service at CDFLLA University Hospital. For practical purposes, it was assumed that the institution utilized its maximum installed capacity, with a group of six teledermatology specialists, representing a capacity of 100%.
Results
A total of 461 patients participated in the study, with ages ranging from 18 to 98 years and an average age of 45.7 ± 17.6 years. The majority of participants were female (73.1% women and 26.9% men). Seventeen patients who did not meet the inclusion criteria were excluded. During the teleconsultations, 9% of the patients required a family member to accompany them.
Connectivity issues, software blocking, or manipulation of the dermatoscopy caused interruptions in 2% of the consultations. However, the duration of these interruptions was not included in the recorded times. Smartphones were used for 69.3% of the consultations, while PC&C was used for 30.7%.
Regarding
Instrument #1—Medical Staff
Also, during patient care in moment 1, the time taken to capture, store, and send clinical and dermoscopic images was measured precisely. It was found that using PC&C took an average of 1.2 min (75 s), which was three times longer than using a Smartphone, which averaged 0.4 min (25 s). Figure 1 illustrates the comparison of image capture, storage, and sending times based on the number of images and the platform used for the query. It can be observed that sending images was quicker when using Smartphones, thus explaining the difference in technology usage.
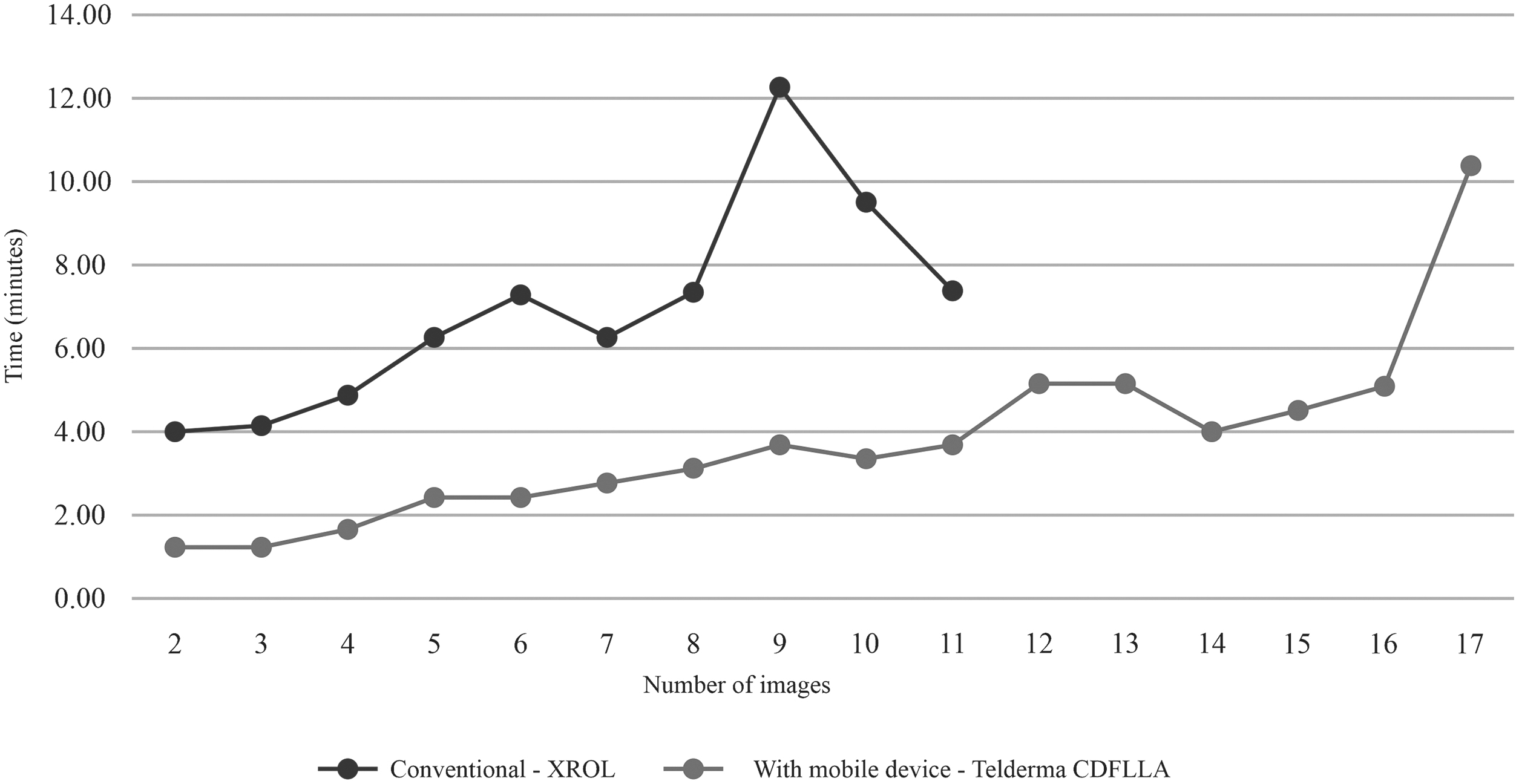
Image storage time according to number of images and platforms.
Tables 2 and 3 present the results of instrument #2, detailing the costs of the equipment used for teledermatology care, accounting for their useful life. The equipment cost for providing teledermatology care with PC&C technology amounted to $488, whereas with Smartphones, it was $296. The difference between the two is $192. It should be noted that although not all equipment is used throughout the entire consultation, such as the camera and dermatoscopy with adapter, their availability during the consultation is necessary.
Instrument # 2—Identification, Measurement, and Assessment of the Equipment
Law 1819 of 2016.
Instrument # 2—Equipment Costs According to the Time of Consultation, the CAE, the Proportion and the Time of Use and Availability
NA, not applicable.
Table 4 displays the overall investment and implementation costs of the teledermatology service. The general cost for providing teledermatology care with PC&C technology was $30 per patient, whereas it was $248 with Smartphones, resulting in a difference of $53. These calculations were estimated based on the assumption that the institution operated at its maximum installed capacity with a group of six teledermatology specialists, representing a yield of 100%. The general costs were differentiated according to the time invested by the dermatologist in addressing a query for each technology used (PC&C = 12 min, Smartphone = 8.1 min).
General Costs of Implementation and Operation of the Teledermatology Service
NA, not applicable.
Upon combining the costs from the three instruments (Table 5), it can be observed that a PC&C consultation costs $26,745, compared with $18,980 for a Smartphone consultation. The difference between the two technologies is $7,765. This difference is statistically significant (p-value: 0.000). It is evident that the primary cost of an asynchronous teledermatology consultation lies in the involvement of the primary care physician and dermatologist.
Summary of the Costs of Medical Personnel, Equipment, and General Costs
Finally, the patient satisfaction results are presented. A total of 581 responses were recorded, with 78.7% (457) corresponding to m1 and 21.3% (124) to m3. The survey did not reveal any differences in the evaluation between the two platforms. While some patients expressed concerns about the security and confidentiality of the images taken (9.4% for Smartphones and 2.8% for PC&C), they recognized that it is a vital tool for the treating physician to assist them with their problem (97.8% for Smartphones and 100% for PC&C). Additionally, they expressed their willingness to use teledermatology again (97.4% for Smartphones and 95.6% for PC&C), and they were satisfied with the quality of the service (96.2% for Smartphones and 97.8% for PC&C). The majority of patients reported that teledermatology saved them from traveling (94.9% for Smartphone and 97.8% for PC&C), and they also indicated that the time from their consultation with the general practitioner to receiving the diagnosis from the dermatologist was satisfactory (100% for Smartphone and 91.1% for PC&C).
Discussion
Within the 2015 Sustainable Development Goals outlined by the United Nations, the goal is for all people to have access to quality care when and where it is needed. 13 In the same way, the COVID-19 pandemic has marked a historical precedent challenging the health systems of the world 14 and placing virtuality on the agenda as a fundamental strategy to transcend and improve access to health services in vulnerable areas. Teledermatology, for its part, has become an effective and safe solution that allows responding to the previously mentioned demands and commitments to the extent that it is possible to guarantee an adequate implementation based on best practices, protocols, operating models, training of the health personnel, technology, and sustainability. The latter, essential for any health system or institution, has been affected by high costs reported by different studies. 15 However, with the advent and exponential development of mobile devices such as Smartphones, a new way of providing teledermatology 16 has been developed that is economically viable, as demonstrated by this study.
The first-of-its-kind research shows an opportunity cost with a Smartphone of $7,765 in each teledermatology consultation by PC&C when a general practitioner and a dermatologist carry out asynchronous communication. This opportunity cost ratio allows that for every five consultations by PC&C; two additional consultations are made through Smartphone.
The use of the Smartphone in teledermatology presents an essential advantage over the PC&C 17 as it allows filling out the patient's clinical information through text or voice and being able to immediately capture the images of the lesions using the equipment's camera and holding a dermatoscopy. Once this process is finished, the consultation can be sent directly to the dermatologist without having to carry out other processes. Of course, the described procedure requires an exclusive App or Web application for teledermatology. At this point lies the difference with the use of PC&C, since the use of this technology implies carrying out various processes, individual and serial (removing the card from the camera or connecting it to the PC, searching, viewing, storing, and sending images) that do not add value to patient care or may even create safety risks by transferring another patient's images or not deleting them from the camera.
For example, in the early stages of mobile device maturity and in which they were not yet sufficiently developed to support a teledermatology service fully, the Smartphone was used for camera purposes only, therefore, requiring the procedure of transferring the images from the cell phone to the PC with times ranging between 5 and 15 min, 18 –20 directly impacting the efficiency of the consultation, and therefore, its costs.
The quality of the images obtained from a Smartphone has been increasing for teledermatology, and its use compared with the conventional photographic camera is comparable, 21 even the American Telemedicine Association (ATA) has defined the technical characteristics that Smartphone cameras must meet to guarantee their quality. 22 As camera resolution improves, fewer studies cite it as a problem, and when they do, it is primarily due to the photographer's technique. 23 Because of all of this, the use of Smartphones for teledermatology has shown not only to meet the expected quality 24 but also to have a less complex, easy-to-use, and more affordable system, 25 which ultimately translates into cost reduction as evidenced in this study.
In our study, the costs of teledermatology are determined mainly by the time of the human resource, that is, by the operation and not by the implementation of the service as such. Logically, this analysis will be consistent because the teledermatology service has been planned to operate long-term and make the most of the installed capacity and infrastructure. Teledermatology is more or less economical to the extent that the number of steps and activities that the family doctor and the dermatologist must carry out to care for a patient decrease. The authors could demonstrate this last statement in m1 (PC&C 15.6′ vs. Smartphone 11.3′); however, for m2, it was a completely unexpected finding (PC&C 12′ vs. Smartphone 8.1′) since the same computer technology was being used to evaluate the cases by the dermatologist. A probable unproven explanation in the study is that differences have arisen in usability or handling on both platforms; that is, fewer clicks and steps to view information and images and respond to queries.
This study is the first to assess PC&C versus Smartphone technology costs for asynchronous teledermatology between a GP and dermatologist. For future research, it is important to incorporate indirect medical costs that evaluate the implications in terms of response time for the patient, an opportune diagnosis that allows them to access adequate treatment, and the possible savings in travel times through specialization of this type of health care.
These are images obtained by the Teledermatology application through Smartphone and dermatoscope (Figs. 2 and 3).

Image of the Telederma platform on smartphone.
Image of the Telederma platform on smartphone.
Conclusion
Teledermatology with Smartphone is a simplified, optimal, and technical quality process for acquiring clinical and dermoscopic images. The benefits are represented in the less time invested by the family doctor and dermatologist for the attention of a consultation. The minimization of costs suggests that the operation of the service is more efficient with Smartphone technology compared with PC and camera. However, it is essential to analyze each institution's local context to determine the barriers and facilitators that allow the implementation of this type of health service.
Footnotes
Acknowledgment
The authors appreciate the participation of the technical staff: Engineer Jeison Santa Restrepo, Dr. Natalia Zuleta Galvis, Dr. Ángel Omar Jaimes Ramírez, Dr. Victoria Eugenia Franco Correa, Dr. Luisa María Montoya Quesada, and Diana Isabel Osorio Cuevas.
Authors' Contributions
C.B.V.: specialist doctor, designer of the Telederma platform (Smartphone alternative) of the HUCDFLLA, principal investigator; in charge of coordinating the research activities, as well as supervising the technical, administrative, and financial execution in the established times and the correct and adequate execution of the resources according to the approved budget and coordination of the technological processes of the project.
E.X.P.F., coinvestigator, medical specialist, and employee of the HUCDFLLA with the functions of coordinator of conventional and mobile teleconsultations, articulation of the operating model proposed in the project and the Dermatological Center, support in the analysis of information, discussion of results, production of new knowledge.
Institutional Review Board Statement
The Ethics Committee approved this study, Hospital Universitario Centro Dermatológico Federico Lleras Acosta (HUCDFLLA) (State Social Enterprise/Ministry of Health and Social Protection, Colombia). Informed consent was obtained from all adult subjects before inclusion in the study (Study identifier code: 58249 Call 777-2017 Ministry of Science and Technology of Colombia. It considers the ethical standards in medical research according to the Declaration of Helsinki, where it is stipulated that it is a risk-free investigation.
The Superintendency of Industry and Commerce (SIC) of Colombia, through Resolution 79198 of December 3, 2021, granted an invention patent for “a method for a Dermatological Telemedicine consultation that allows the configuration of an image acquisition device automatically” IPC classification: A61B 5/00, G06F 19/00. Inventors (moral rights) are Drs. Camilo Alberto Barrera Valencia, Elin Xiomara Perea Flórez, and Claudia Marcela Rojas Daza and patrimonial rights belong to the Hospital Universitario Centro Dermatológico Federico Lleras Acosta E.S.E.
Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This research has been cofinanced by the Colombian Ministry of Science and Technology Registry Code: 58249. Title: Implementation and validation of a teledermatology model through mobile devices. Announcement 777-2017 for health science, technology, and innovation projects 2017.