
Abstract
Background:
Musculoskeletal (MSK) pain is the leading cause of disability worldwide. Telemedicine is of growing importance, yet impacts on treatment efficacy remain unclear.
Objective:
This umbrella review (CRD42022298047) examined the effectiveness of telemedicine interventions on pain intensity, disability, psychological function, quality of life, self-efficacy, and adverse events in MSK pain.
Methods:
PubMed, SPORTDiscus, Cochrane Library, EMBASE, and CINAHL were searched from inception to August 9, 2022, for systematic reviews with meta-analysis, including telemedicine-delivered exercise, education, and psychological interventions, in randomized controlled trials (RCTs). AMSTAR-2 was implemented. Standardized mean differences (SMDs; negative favors telemedicine) were extracted as effect estimates.
Results:
Of 1,135 records, 20 reviews (RCTs: n = 97, participants: n = 15,872) were included. Pain intensity SMDs were −0.66 to 0.10 for mixed pain (estimates: n = 16), −0.64 to −0.01 for low-back pain (n = 9), −0.31 to −0.15 for osteoarthritis (n = 7), −0.29 for knee pain (n = 1), −0.66 to −0.58 for fibromyalgia (n = 2), −0.16 for back pain (n = 1), and −0.09 for rheumatic disorders (n = 1). Disability SMDs were −0.50 to 0.10 for mixed pain (n = 14), −0.39 to 0.00 for low-back pain (n = 8), −0.41 to −0.04 for osteoarthritis (n = 7), −0.22 for knee pain (n = 1), and −0.56 for fibromyalgia (n = 1). Methodological quality was “critically low” for 17 reviews. Effectiveness tended to favor telemedicine for all secondary outcomes.
Conclusions:
Primary RCTs are required that compare telemedicine interventions with in-person delivery of the intervention (noninferiority trials), consider safety, assess videoconferencing, and combine different treatment approaches.
Introduction
Musculoskeletal (MSK) pain is the most common reason for disability worldwide and affects 1.7 billion people. 1 Subsequently, MSK pain incurs a financial burden of 1,387,200 USD (0.417% of the GDP) in the United States. 2 Therefore, identifying treatments capable of reducing the global burden of MSK pain is critical.
Treatment approaches for MSK pain are most commonly provided through in-person delivery (e.g., by physical therapist, physiotherapist or exercise physiologist). However, circumstances, such as insufficient infrastructure in rural and remote regions, the recent COVID-19 pandemic, consumer preference or convenience, or other challenges to consumer access, have stressed the need for alternatives to in-person rehabilitation. 3,4 A burgeoning option is telemedicine, 5,6 which offers several benefits to patients, such as reduced travel, 7 increased self-management, 8 and time flexibility, 9,10 and is commonly accepted by patients with MSK pain. 11 The term telemedicine describes different kinds of diagnostics and interventions, which are delivered digitally either synchronously or asyncronously. 4 Telemedicine can be defined as “the use of advanced telecommunication technologies to exchange health information and provide health care services across geographic, time, social, and cultural barriers.” 12 However, there is still much uncertainty regarding several aspects of telemedicine.
Recent umbrella reviews concluded that telemedicine treatments can reduce disability in patients with MSK pain. 13 –15 However, prior reviews only considered patients with MSK pain collectively, rather than by diagnostic subgroups, which overlooks that specific MSK pain conditions may manifest through differing mechanisms. 16 Specific MSK pain conditions may also respond differently to the same treatment and thus impact recovery trajectories. 17 Furthermore, prior umbrella reviews focused on single interventions, rather than the range of treatments commonly employed for MSK pain. Finally, previous reviews tend to omit key clinical outcomes, such as pain intensity, psychological functioning, 18 health-related quality of life (HrQoL), self-efficacy, and adverse events, which preclude a broader understanding of treatment efficacy.
This umbrella review primarily aimed to examine the effectiveness of telemedicine interventions on pain intensity and disability among diagnostic subgroups of patients with MSK pain. Secondary aims examined the effectiveness of telemedicine interventions on psychological functioning, health related quality of life (HrQoL), and self-efficacy, as well as safety (adverse events). In addition, another goal was to identify evidence gaps in primary studies.
Methods
Protocol and registration
We prospectively registered this umbrella review using PROSPERO (CRD42022298047) and followed PRISMA2020 19 and PRIOR 20 guidelines in the conduct and reporting of this review. Deviations from the protocol are displayed in Supplementary Data S1, S12–S14.
Ethical Approval
No ethical approval was needed because we used data from previously published studies in which informed consent was obtained by the respective primary investigators.
Eligibility criteria
Eligibility criteria were based on the participant, intervention, comparator, outcome, and study design (PICOS) framework. 21 Telemedicine definitions relevant to eligibility criteria are provided in Supplementary Data S2.
Population
Adults (≥18 years of age) of any sex with MSK pain considered subacute (6–12 weeks 22 ) or chronic (>12 weeks 22 ). MSK pain was defined as pain referring to the MSK system (e.g., muscles, tendons, ligaments, cartilage) of a specific or nonspecific origin. Reviews including secondary pain without MSK origin (e.g., asthma, Morbus Crohn's or heart diseases) and specific to post-surgical/post-traumatic pain were excluded.
Intervention
Any synchronous or asynchronous telemedicine intervention delivered using a digital pathway (e.g., website, mail, app, messaging, telephone) in isolation or conjunction with other treatments. Education, exercise/physical training, and psychological therapies were considered eligible as treatments. Reviews that focused solely on interventions that need specific equipment, additional to that used for telemedicine such as virtual reality devices or requiring participation from a specific geographical location, were excluded.
Comparator
Usual care, any in-person intervention, waiting list, and no intervention. Studies in which comparator interventions were linked to telemedicine were excluded.
Outcomes
Reviews had to evaluate pain intensity or disability. Secondary outcomes were HrQoL, psychological functioning, self-efficacy, and adverse events, yet the absence of these outcomes did not preclude inclusion.
Study type
Systematic reviews with meta-analyses in English and German language, including randomized and nonrandomized controlled trials (RCTs), were eligible for inclusion.
Information sources and search strategy
The following databases were searched: PubMed, SPORTDiscus, Cochrane Library (Cochrane Database of Systematic Reviews), EMBASE, and CINAHL. The full search strategy is available in Supplementary Data S3. We also manually searched the reference lists of included reviews and conducted forward citation tracking using Google Scholar. Covidence (
Study selection
Title/abstract and full-text screening were conducted by two independent reviewers (S.K. and C.L.S.) using Covidence. Conflicts were resolved by a third independent reviewer (N.L.M.). Title/abstract and full-text screening were piloted (S.K. and C.L.S.) on 60 and 10 articles, respectively. Potential discrepancies were discussed among the entire authorship team. For quality control, an independent reviewer (R.D.) randomly cross-checked title/abstract (articles: n = 66) and full-text screening (n = 6).
Data extraction: Included systematic reviews
Data extraction was conducted by two independent reviewers (S.K. and M.T.) using a custom-designed Google spreadsheet. Extraction was piloted with two reviews and compared using a custom-written code in the R statistical environment (version 4.02). Conflicts were resolved by a third independent reviewer (N.L.M.).
We extracted the following parameters: Author name, year of publication, number of trials included in the review/meta-analysis, number of participants, diagnostic subgroup, pain stage (subacute/chronic), mean age, percentage of females, details on intervention and control group, assessed outcomes with the corresponding effect size and confidence interval, adherence rate, and adverse events. Missing outcomes were classified as not reported. If details of outcome measures were missing, the corresponding author of the review was contacted three times in a timeframe of 8 weeks. If no answer was obtained, the study was not integrated in the quantitative summary. For quality control, an independent reviewer (R.D.) cross-checked extraction of two articles selected at random.
Data extraction: primary studies
In addition to the extraction of study details at the review level, the following data were extracted at the primary study level: Details of intervention and control group, delivery pathway, mode of delivery, and number of randomized participants. In case of missing data and/or discrepant data between included reviews, the data were extracted directly from the primary studies.
Assessment of methodological quality: Included systematic reviews
The methodological quality of included reviews was assessed using the AMSTAR 2 tool. 23 To account for the specifications of this umbrella review and that methodological advances have occurred since AMSTAR 2 was developed, we implemented the tool as described in Supplementary Data S4. Assessment of methodological quality was piloted on two studies, conducted by two independent reviewers (S.K. and M.T.), and discrepancies were adjudicated by a third independent reviewer (N.L.M.).
Data synthesis
We conducted a narrative synthesis by grouping meta-analyses from the included reviews per outcome and diagnostic subgroup, and presented the standardized mean differences (SMD = difference in mean outcome between groups/standard deviation of outcome among participants 24 [negative values favor telemedicine]), 95% confidence intervals (CI), sample size, number of studies, intervention and comparator details, and certainty of evidence (GRADE) together in forest plots without pooling the data. Where different measures of spread were reported, the SMD and CI with Hartung–Knapp correction 25 were calculated manually in the R statistical environment using the package “meta”. 26 Subgroup analyses conducted in the included reviews were presented in additional forest plots. Clinical meaningfulness was defined as an SMD of at least 0.5. 27
The amount of overlap of included primary studies was quantified by calculating the corrected covered area 28 (CCA) for each primary outcome and presented in tabulated form to estimate the independency of each effect estimate. If reviews included subgroup meta-analyses that did not meet our eligibility criteria, the primary studies from those meta-analyses were not included in the calculation of the CCA.
To identify evidence gaps on the primary study level, intervention content details and delivery pathways were synthesized in a heat map, where darker colors represent a larger sample size.
Results
The search strategy yielded 1,135 records (Fig. 1). Full-text screening involved 73 records and 19 reviews were ultimately included. Manual search identified one additional included review 29 for a total of 20 included reviews. Studies excluded at full-text screening are detailed in Supplementary Data S5.
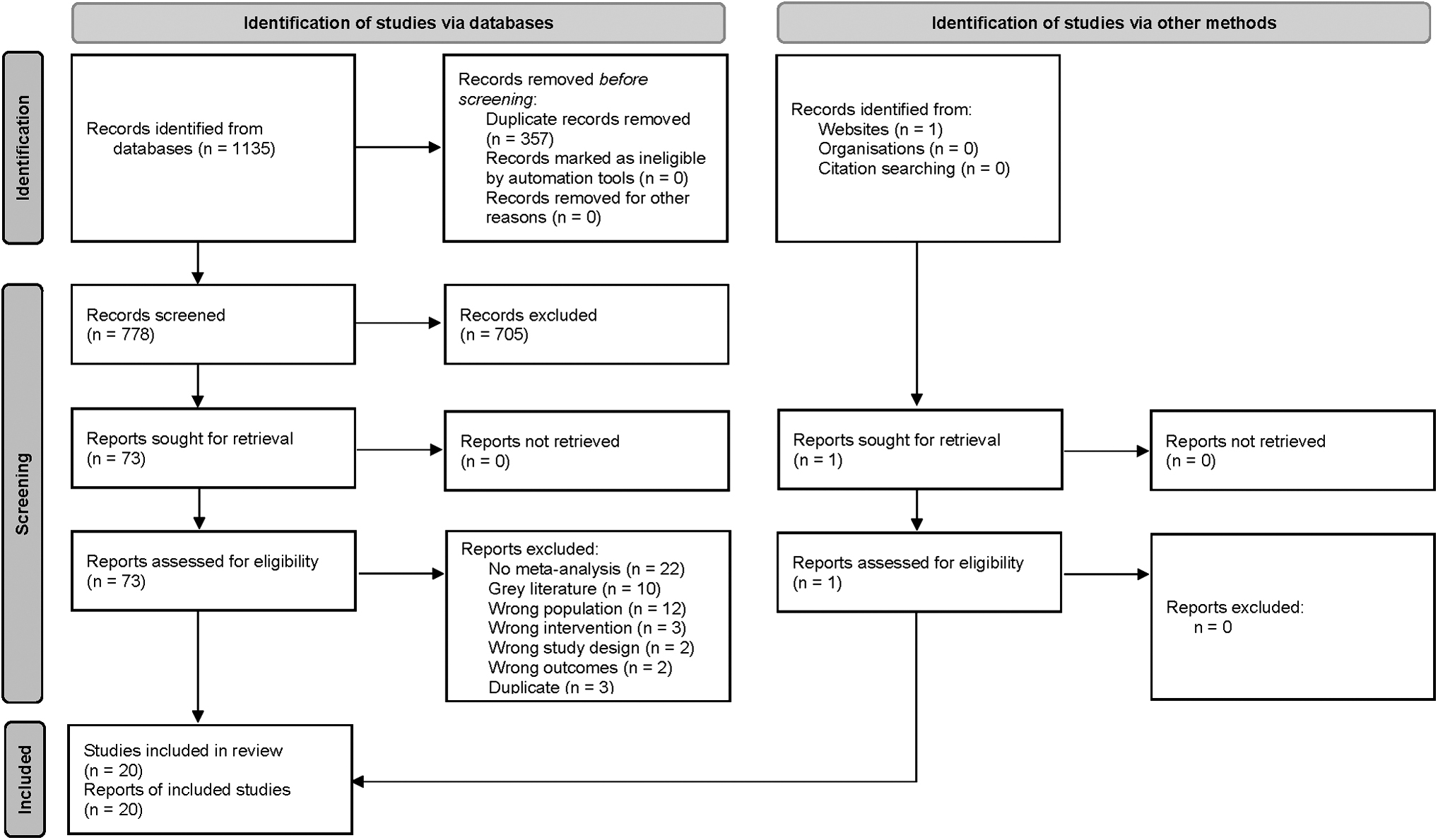
PRISMA search flow diagram.
Data handling
An overview of data handling is shown in Supplementary Data S6.
Study characteristics
Included reviews (N = 20; Table 1) were published between 2014 and 2022 and investigated the effectiveness of telemedicine on mixed MSK pain populations (N = 5), 30 –34 low-back pain (N = 5), 29,35 –38 knee pain (N = 1), 39 osteoarthritis (N = 4), 40 –43 fibromyalgia (N = 1), 44 and mixed chronic conditions, including subgroup analyses for MSK pain (N = 4). 45 –48 Twelve reviews included RCTs investigating participants with chronic pain 15,29,30,37 –40,43,44,46 –48 and eight investigated mixed pain stages. 31 –33,35,36,41,42,45 Interventions examined were as follows: exercise (N = 3), 30,39,45 psychological (N = 4), 34,44,46,47 exercise/education (N = 2), 35,41 education/psychological (N = 3), 36 –38 and exercise/education/psychological (N = 8). 29,31 –33,40,42,43,48
Details of Included Reviews
SR, systematic review; MA, meta-analysis; NR, not reported; HrQoL, health-related quality of life.
One review included usual care as comparator group, 35 while the remaining included different kinds of comparator groups in combination. The majority (N = 19) examined pain intensity and disability, yet one only included outcomes of pain intensity. 34 Seven reviews examined self-efficacy, 31 –34,44,47,48 six examined psychological functioning, 32,33,44,46 –48 eight examined HrQoL, 30,31,39,41,43 –46 and five examined adverse events. 32,33,38,44,46 Follow-up time points ranged from 2 weeks to 30 months.
Reviews included 97 primary RCTs (N = 15,872) for the primary outcomes pain and disability. While eligible, no non-RCT was included in any included review. For pain intensity, 160 publications (including double counting) were included in meta-analyses, which represented 84 unique RCTs (CCA: 8.43, moderate overlap). 28 For disability, 113 publications (including double counting) were included in meta-analyses, representing 71 unique RCTs (CCA: 6.64, merely moderate overlap). A citation matrix is available in Supplementary Data S7.
An overview of interventions by delivery pathway and sample size of the primary studies is provided in a heat map (Fig. 2). Heat maps for each diagnostic subgroup are available in Supplementary Data S8 and a tabulated summary is included in Supplementary Data S9.

Heat map of intervention content (y-axis) and delivery pathway (x-axis) of primary RCTs included in the systematic reviews; colors indicating N participants per combination of intervention content and delivery pathway. RCT, randomized controlled trial.
Methodological quality
The methodological quality was rated “critically low” in 16 reviews, 29 –32,35 –43,46 –48 “low” in three reviews, 33,34,45 and “moderate” in one review. 44 The detailed ratings for each component of AMSTAR 2 are shown in Table 2.
AMSTAR 2 Results
Primary outcomes
Mixed MSK pain conditions
Eight reviews, 16 effect estimates for pain intensity, and 15 effect estimates for disability were identified for mixed MSK pain conditions ( Figs. 3, 4 and Supplementary Data S10 and S11). One review provided no effect estimate. 47 For exercise interventions, 30,45 SMD (95% CI) ranged −0.22 to 0.10 (−0.45 to 0.40; 4 estimates; GRADE: low to high) for pain intensity and −0.20 to 0.10 (−0.66 to 0.65; 5 estimates; GRADE: low to high) for disability. For psychological interventions, 46 SMD (95% CI) ranged −0.48 to −0.37 (−1.18 to 0.22; 2 estimates; GRADE: not reported) for pain intensity and −0.50 to −0.15 (−0.80 to -0.01; 2 estimates; GRADE: not reported) for disability. For exercise/education/psychological interventions, 31 –33,48 SMD (95% CI) ranged −0.66 to −0.07 (−1.60 to 0.62; 10 estimates; GRADE: very low to moderate) for pain intensity and −0.45 to −0.06 (−0.70 to 0.31; 7 estimates; GRADE: low to moderate) for disability.
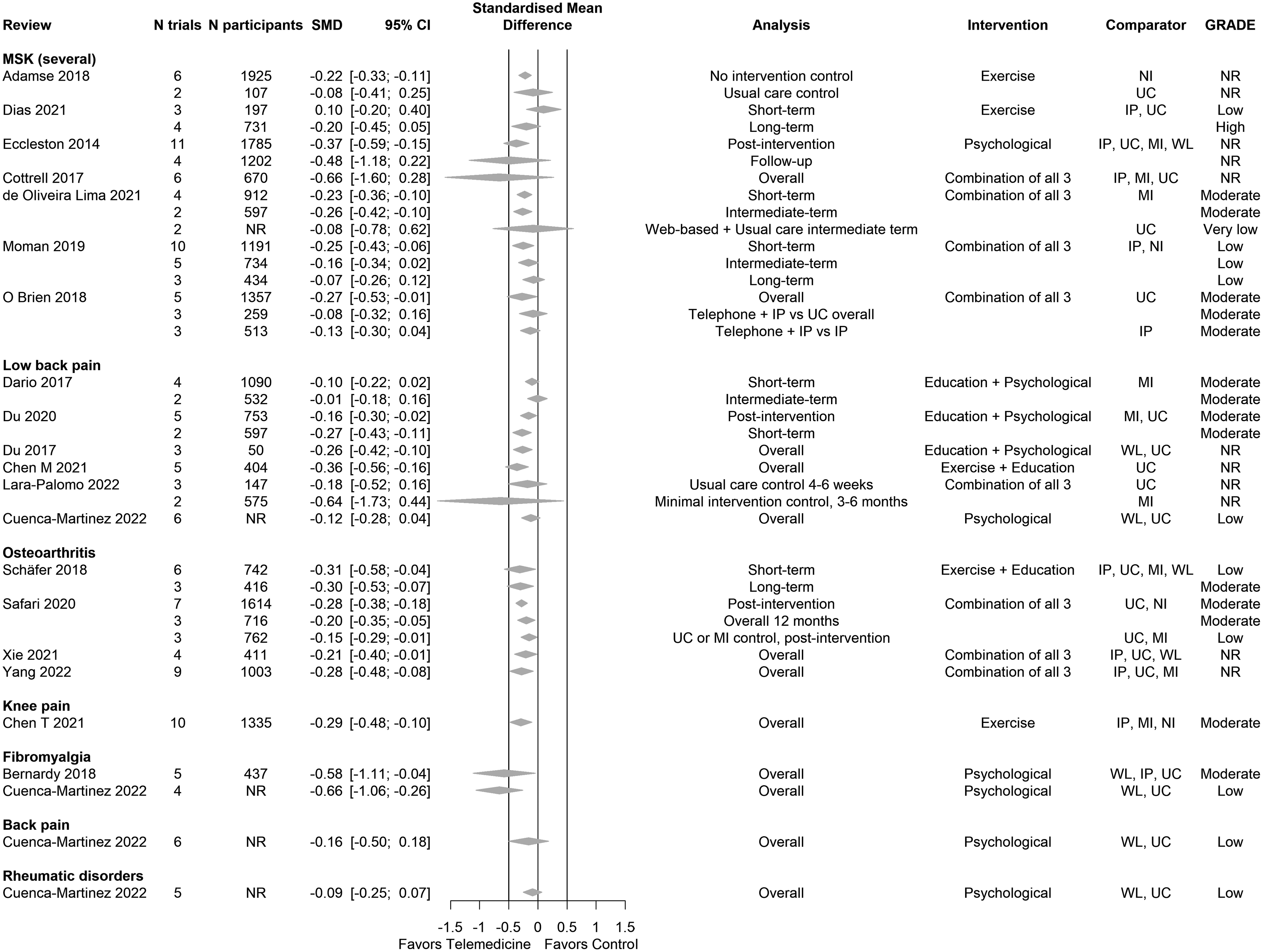
Forest plot for the outcome pain intensity of main analyses. A negative value represents an effect in favor of telemedicine. Effect sizes and 95% confidence intervals from meta-analyses are represented by a diamond. Bold lines of equivalence represent borders of clinical meaningfulness (−0.5; 0.5 SMD). NI, no intervention; MI, minimal intervention; WL, waiting list; UC, usual care; IP, in-person; SMD, Standardized mean difference.

Forest plot for the outcome disability of main analyses. A negative value represents an effect in favor of telemedicine. Effect sizes and 95% confidence intervals from meta-analyses are represented by a diamond. Bold lines of equivalence represent borders of clinical meaningfulness (−0.5; 0.5 SMD).
Low-back pain
Six reviews, nine effect estimates for pain intensity, and eight effect estimates for disability were identified for low-back pain ( Figs. 3, 4 and Supplementary Data S10 and S11). For exercise/education interventions, 35 SMD (95% CI) was −0.36 (−0.56 to −0.16; 1 estimate; GRADE: not reported) for pain intensity and −0.31 (−0.46 to −0.16; 1 estimate; GRADE: not reported) for disability. For psychological interventions, 34 SMD (95% CI) was −0.12 (−0.28 to 0.04; 1 estimate; GRADE: low) for pain intensity. For education/psychological interventions, 36 –38 SMD (95% CI) ranged −0.27 to −0.01 (−0.43, 0.16; 5 estimates; GRADE: moderate) for pain intensity and −0.34 to 0.00 (−0.52 to 0.18; 5 estimates; GRADE: low to moderate) for disability.
For exercise/education/psychological interventions, 29 SMD (95% CI) ranged −0.64 to −0.18 (−1.73 to 0.44; 2 estimates; GRADE: not reported) for pain intensity and −0.39 to −0.20 (−0.87 to 0.41; 2 estimates; GRADE: not reported) for disability.
Osteoarthritis
Four reviews and 7 effect estimates for both pain intensity and disability were identified for osteoarthritis ( Figs. 3, 4 and Supplementary Data S10 and S11). For exercise/education interventions, 41 SMD (95% CI) ranged −0.31 to −0.30 (−0.58 to −0.04; 2 estimates; GRADE: low to moderate) for pain intensity and −0.41 to −0.30 (−0.76 to 0.16; 2 estimates; GRADE: low to high) for disability. For exercise/education/psychological interventions, 40,42,43 SMD (95% CI) ranged −0.28 to −0.15 (-0.48 to −0.01; 5 estimates; GRADE: low to moderate) for pain intensity and −0.26 to −0.04 (-0.42 to 0.12; 5 estimates; GRADE: low to moderate) for disability.
Knee Pain
One review and one effect estimate for both pain intensity and disability were identified for knee pain ( Figs. 3, 4 and Supplementary Data S10 and S11). For exercise interventions, 39 SMD (95% CI) was −0.29 (−0.48 to −0.10; 1 estimate; GRADE: moderate) for pain intensity and −0.22 (−0.43 to −0.00; 1 estimate; GRADE: moderate) for disability.
Fibromyalgia
Two reviews, 2 effect estimates for pain intensity, and one effect estimate for disability were identified for fibromyalgia ( Figs. 3, 4 and Supplementary Data S10 and S11). For psychological interventions, 34,44 SMD (95% CI) ranged −0.66 to −0.58 (−1.11 to −0.04; 2 estimates; GRADE: low to moderate) for pain intensity and was −0.56 (−1.00, −0.13; 1 estimate; GRADE: moderate) for disability.
Back pain
One review and one effect estimate for pain intensity were identified for back pain (Fig. 3 and Supplementary Data S11). For psychological interventions, 34 SMD was −0.16 (−0.50, 0.18; 1 estimate; GRADE: low).
Rheumatic disorders
One review and one effect estimate for pain intensity were identified for rheumatic disorders (Fig. 3 and Supplementary Data S11). For psychological interventions, 34 SMD was −0.09 (−0.25, 0.07; 1 estimate; GRADE: low).
Secondary outcomes
Mixed MSK pain conditions
Three reviews and 3 effect estimates for HrQoL were identified for mixed MSK pain conditions (Fig. 5 and Supplementary Data S11). SMD (95% CI) ranged −0.03 to 0.30 (−0.50 to 1.10; 2 estimates; GRADE: high) for exercise interventions, 30,45 and was −0.27 (−0.54 to 0.00; 1 estimate; GRADE: not reported) for psychological interventions. 46

Forest plot for the outcome health-related quality of life of all analyses. A negative value represents an effect in favor of telemedicine. Effect sizes and 95% confidence intervals from meta-analyses are represented by a diamond. Bold lines of equivalence represent borders of clinical meaningfulness (−0.5; 0.5 SMD).
Four reviews and 15 effect estimates for psychological functioning were identified for mixed MSK pain conditions (Fig. 6 and Supplementary Data S11). For psychological interventions, 46 SMD (95% CI) ranged −0.53 to −0.19 (−1.84 to 0.78; 4 estimates; GRADE: not reported). For exercise/education/psychological interventions, 32,33,48 SMD (95% CI) ranged −0.45 to 0.11 (-3.02 to 2.56; 11 estimates; GRADE: very low to moderate).

Forest plot for the outcome psychological functioning of all analyses. A negative value represents an effect in favor of telemedicine. Effect sizes and 95% confidence intervals from meta-analyses are represented by a diamond. Bold lines of equivalence represent borders of clinical meaningfulness (−0.5; 0.5 SMD).
Three reviews and four effect estimates for self-efficacy were identified for mixed MSK pain conditions (Fig. 7 and Supplementary Data S11). For exercise/education/psychological interventions, 32,33,48 SMD (95% CI) ranged −0.46 to −0.19 (−0.78 to −0.02; 4 estimates; GRADE: very low to high).

Forest plot for the outcome self-efficacy of all analyses. A negative value represents an effect in favor of telemedicine. Effect sizes and 95% confidence intervals from meta-analyses are represented by a diamond. Bold lines of equivalence represent borders of clinical meaningfulness (−0.5; 0.5 SMD).
Three reviews 32,46,48 reported on adverse events. One review on exercise/education/psychological interventions 32 stated the primary studies did not report the outcome, while adverse events were synthesized only narratively in one review on exercise/education/psychological interventions 33 where either no intervention-related adverse event occurred or adverse events were balanced between intervention and control group. The remaining review on psychological interventions 46 reported on the adverse events in one primary study (11.9%) and stated that the other primary studies did not report on adverse events.
Low-back pain
One review and one effect estimate for self-efficacy were identified for low-back pain (Fig. 7 and Supplementary Data S11). For psychological interventions, 34 SMD (95% CI) was −0.52 (−1.58, 0.54; 1 estimate; GRADE: low).
One review on education/psychological interventions 36 in LBP patients stated that zero adverse events were reported in the primary studies.
Osteoarthritis
Two reviews and 6 effect estimates for HrQoL were identified for osteoarthritis (Fig. 5 and Supplementary Data S11). SMD (95% CI) ranged −0.27 to −0.13 (-0.61 to 0.35; 5 estimates; GRADE: moderate to high) for exercise/education interventions 41 and was 0.00 (−0.26 to 0.26; 1 estimate; GRADE: not reported) for exercise/education/psychological interventions. 43
Knee pain
One review and two effect estimates for HrQoL were identified for knee pain (Fig. 5 and Supplementary Data S11). For exercise, SMD (95% CI) ranged −0.18 to −0.25 (−0.46 to 0.05; 2 estimates; GRADE: high). 39
Fibromyalgia
One review and 2 effect estimates for HrQoL were identified for fibromyalgia (Fig. 5 and Supplementary Data S11). For psychological interventions, 44 SMD (95% CI) ranged −0.58 to −0.58 (−1.06 to −0.09; 2 estimates; GRADE: moderate).
One review and 3 effect estimates for psychological functioning were identified for fibromyalgia (Fig. 6 and Supplementary Data S11). For psychological interventions, 44 SMD (95% CI) ranged −0.77 to −0.12 (−1.10 to 0.16; 3 estimates; GRADE: moderate).
Two reviews and three effect estimates for self-efficacy were identified for fibromyalgia (Fig. 7 and Supplementary Data S11). For psychological interventions, 34,44 SMD (95% CI) ranged −0.65 to -0.24 (−1.02 to 0.06; 3 estimates; GRADE: low to moderate).
One review on psychological interventions 44 concluded that no adverse event was reported in the primary studies.
Back pain
One review and one effect estimate for self-efficacy were identified for back pain (Fig. 7). For psychological interventions, 34 SMD (95% CI) was −0.63 (−1.98 to 0.71; 1 estimate; GRADE: low).
Rheumatic disorders
One review and one effect estimate for self-efficacy were identified for rheumatic disorders (Fig. 7 and Supplementary Data S11). For psychological interventions, 34 SMD (95% CI) was −0.24 (−0.70 to 0.22; 1 estimate; GRADE: low).
Discussion
This umbrella review showed that reductions in pain intensity and disability across a range of MSK pain conditions tended to favor telemedicine interventions when compared to control. However, few estimates were greater than the threshold considered clinically meaningful (i.e., SMD: −0.5). In the limited studies that examined HrQoL, psychological functioning, and self-efficacy across a range of MSK pain conditions, improvements tended to favor telemedicine, yet the majority of estimates were not clinically meaningful. Notably, overall study quality was considered “critically low” in 16 studies and five robustly reported adverse events.
Psychological interventions tended to demonstrate clinical meaningful effects for pain compared to active and passive comparators in patients with fibromyalgia. 34,44 Our observations align with Cuenca-Martínez et al., 15 yet we also observed a clinically meaningful effect for exercise/education/psychological interventions in patients with general back pain compared to usual care. 34 Previous umbrella reviews found no difference between the effect of exercise/education/psychological interventions delivered through telemedicine and in-person/usual care for disability in patients with MSK pain. 13,14 This is supported by our findings, while our review adds similar results for pain intensity, 33 patients in the osteoarthritis subgroup 33 and for exercise alone. 45
A clinically meaningful effect to improve psychological functioning, HrQoL, and self-efficacy 44 was found for psychological interventions in patients with fibromyalgia compared to active and passive comparators. These findings are in line with those from Cuenca-Martínez et al., 15 except for HrQoL and self-efficacy, which is a new finding from our review. For several MSK pain conditions combined, exercise/education/psychological interventions delivered through telephone alone or in adjunction to in-person delivery are probably not less effective than in-person delivery and usual care to improve psychological functioning and HrQoL. 33
Furthermore, self-efficacy was slightly improved compared to usual care. 33 Those clinical outcomes have not been investigated by prior umbrella reviews. None of the prior umbrella reviews included analyses about other diagnostic subgroups that have been investigated in our review. Psychological interventions may have little to no effect on self-efficacy for patients with rheumatic disorders and general back pain compared to active and passive controls. 15 All three interventions delivered through telephone showed similar effects compared to in-person delivery and usual care for HrQoL in patients with osteoarthritis. 33
Several evidence gaps were identified during the conduct of this umbrella review. On the review level, it is evident that only four reviews with relatively small sample sizes included self-efficacy in their analysis, despite self-efficacy being an important outcome in the context of telemedicine. Lower self-efficacy is associated with a reduced likelihood of clinical improvement in internet-based interventions. 49
On the RCT level, web based (39/97 [40.2%]), telephone (24/97 [24.7%]), and mHealth (15/97 [15.5%]) were most frequently investigated, while videoconferencing was only evaluated to a small amount (5/97 [5.2%]). This finding reflects an important evidence gap, since the use of videoconferencing in practice has increased during the COVID-19 pandemic. 50
Furthermore, it is apparent that education was only investigated in 10/97 (10.3%) RCTs and never in combination with mHealth. A combination of exercise, education, and psychological treatments was only used in 3/97 (3.1%) trials. Regarding the control group, the minority of trials used in-person interventions as comparator group (15/97 [15.5%]), while most trials compared to usual care (43/97 [44.3%]), no or minimal intervention (23/97 [23.7%]) or waiting list (16/97 [16.5%]).
Some limitations of this umbrella review must be considered. On the level of systematic reviews, it is important to note that many reviews included several different comparison groups and pooled them all together in meta-analyses. RCTs with true controls tend to have higher effect sizes than those with waiting list and placebo intervention. 51 Furthermore, many reviews did not account for the risk of bias of primary studies in their meta-analyses and failed to conduct sensitivity analyses, which lead to an increased risk of nonrobust results. Overall, the quality of included reviews was poor in AMSTAR 2. Although it has to be kept in mind that floor effects of AMSTAR 2 can occur due to relatively strict items, the quality is most often decreased due to an insufficient preregistered protocol (9/20 [45%]) and inadequate statistical methods (8/20 [40%]), which are key factors for reliable evidence.
The methodology of this umbrella review also demonstrates some limitations. First, the lack of secondary outcomes reported in the reviews might be the consequence of including only reviews that investigated either pain or disability. Second, we did not re-extract all data from primary RCTs, but, unless any discrepancy between reviews was present, relied on the reporting of reviews. Last, we excluded systematic reviews without meta-analyses, which might lead to missing information, but increased the consistency of our summary of results.
The findings of this study have several implications. When excluding studies with critically low levels of evidence, 29 –32,35 –43,46 –48 telemedicine-based interventions seem to be comparably effective to usual care or in-person delivery and could be sought as an alternative or adjunction to in-person care. Those implications are applicable across different types of interventions. However, regarding the implementation of telemedicine in practice, it has to be kept in mind that the safety of telemedicine-based interventions is not completely clear, given few studies reported adverse events in detail.
In particular, asynchronous telemedicine interventions have the potential to address waiting times commonly experienced by patients with MSK pain. Longer waiting times have a negative effect on clinical outcomes, 52,53 and show a negative association with patient satisfaction with therapy, 54 which likely contributes to the overall burden of MSK pain. Furthermore, since longer waiting times lead to higher health care utilization and higher costs for patients, 52 health insurance providers should consider funding telemedicine-based interventions like standard in-person interventions.
Future research should examine self-efficacy and safety outcomes of telemedicine-based interventions. Furthermore, future RCTs should use evidence-based, in-person interventions compared to the same intervention delivered through telemedicine modalities to draw more accurate conclusions on the effectiveness of telemedicine. Researchers conducting meta-analyses should account for the large heterogeneity across RCTs by conducting appropriate subgroup analyses and having clear and meaningful inclusion criteria.
Conclusion
This body of evidence tends to slightly favor telemedicine compared to traditional treatment delivery approaches for pain intensity, disability, psychological functioning, HrQoL, and self-efficacy in patients with MSK pain across a range of diagnostic subgroups, yet effect sizes were mostly not clinically meaningful and focused on comparisons to no intervention. Furthermore, results should be interpreted with caution owing to the poor methodological quality of included reviews. Current evidence gaps include primary RCTs that compare telemedicine interventions with in-person delivery of similar intervention approaches (noninferiority trials), RCTs for videoconferencing, and investigations combining different treatment approaches. Further research is needed on safety and factors influencing adherence.
Authors' Contribution
S.K., D.L.B., P.J.O., and N.L.M.: Conceptualization: Ideas; formulation or evolution of overarching research goals and aims; S.K., T.S., D.L.B., and P.J.O.: Methodology: Development or design of methodology and creation of models; D.L.B., T.S., and S.K.: Software: Programming, software development; designing computer programs; implementation of the computer code and supporting algorithms; and testing of existing code components; R.D.: Validation: Verification, whether as a part of the activity or separate, of the overall replication/reproducibility of results/experiments and other research outputs; S.K. and T.S.: Formal analysis: Application of statistical, mathematical, computational, or other formal techniques to analyze or synthesize study data; S.K., M.T., and C.L.S.: Investigation: Conducting a research and investigation process, specifically performing the experiments, or data/evidence collection; Not Applicable: Resources: Provision of study materials, reagents, materials, patients, laboratory samples, animals, instrumentation, computing resources, or other analysis tools; S.K. and D.L.B.: Data Curation: Management activities to annotate (produce metadata), scrub data, and maintain research data (including software code, where it is necessary for interpreting the data itself) for initial use and later reuse; S.K.: Writing - original draft: Preparation, creation, and/or presentation of the published work, specifically writing the initial draft (including substantive translation); All: Writing - review and editing: Preparation, creation, and/or presentation of the published work by those from the original research group, specifically critical review, commentary or revision – including pre-publication or post-publication stages; S.K.: Visualization: Preparation, creation, and/or presentation of the published work, specifically visualization/data presentation; D.L.B., L.D., P.J.O., and N.L.M.: Supervision: Oversight and leadership responsibility for the research activity planning and execution, including mentorship external to the core team; S.K.: Project administration: Management and coordination responsibility for the research activity planning and execution; Not Applicable: Funding acquisition: Acquisition of the financial support for the project leading to this publication.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6
Supplementary Data S7
Supplementary Data S8
Supplementary Data S9
Supplementary Data S10
Supplementary Data S11
Supplementary Data S12
Supplementary Data S13
Supplementary Data S14
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.