
Abstract
The COVID-19 pandemic created critical challenges for hospitals and health care providers. Suddenly clinics were forced to close; elective procedures were delayed; scheduled visits were canceled; emergency rooms were overcrowded; hospital beds, equipment, and personal protective equipment (PPE) were in short supply; and staff were faced with rapidly changing circumstances, care protocols, trauma, and personal risk. To better address challenges of the ongoing COVID-19 pandemic and prepare for future pandemics, the National Telemedicine Technology Assessment Resource Center (TTAC) was asked to develop a Pandemic Response Action Plan that would allow its users to address critical issues with available telemedicine and related technologies. The project was constructed in 3 phases. Phase 1-Develop a Pandemic Response Action Plan and a Pandemic Response Action Plan Policy and Regulatory Summary, which identifies the regulatory challenges as well as policy recommendations. Phase 2-Publish the Action Plan and the Policy and Regulatory Summary. Phase 3-Look at health care providers who used the approaches, tools, and technology in the Pandemic Action Plan and document the results. This document represents Phase 3.
This document is Phase 3. In this report we look back at health care providers who used the approaches in the Phase 1
Methods:
The same multidisciplinary team that constructed Phase 1 and Phase 2 were engaged to develop this Phase 3 report. The members of the team represent leadership expertise and key stakeholders in health care delivery during a pandemic (administration, infection control, physicians, nurses, public health, contingency planning, disaster response, and information technology) as well as a facilitator. For Phase 3, the group used structured brainstorming to define the findings, issues, and results of their own organizations’ digital health response to the pandemic. In addition, eight health care providers (hospitals) identified by the Telemedicine Resource Centers’ (TRCs) organizations, who used the Pandemic response Plan (created in Phases 1 and 2), were interviewed. All interviews were conducted by the same facilitator with leaders (CEO, and leaders of the telemedicine programs) in each of the eight programs, using a standard questionnaire created by the team. Current literature references are included in this report to illustrate when findings are known to have broader applicability.
Conclusions:
The impact of the COVID-19 Pandemic was severe and identified multiple critical challenges and weaknesses. Applying the approaches, tools, and technology outlined in the
Introduction
Most weaknesses that COVID-19 exacerbated already existed before the pandemic. They were already well known but most have not been addressed. They include staff shortages, antiquated and inefficient workflows/service delivery strategies, failure to adopt new technologies, and poor coordination of information. The research and team discussion established serious questions, including: Why doesn’t health care have virtual encounters while almost every other industry does? Why does health care depend on in-person registration? Why do health care providers still use physical waiting rooms? Why does health care often fail to share resources and expertise and fail to offer services close to the patient? Why are patients required to travel to get care, examination, and follow-up (especially when the patients are sick and travel challenging in both urban and rural environments) when this can be done remotely?
The team concluded that, in general, before the pandemic, many health care processes were similar to other industry processes of the 1970s (i.e., manual, not using modern process tools, requiring face to face where not needed, etc.). resulting in higher cost, patient dissatisfaction, worse outcomes, and often exposing patients and consumers to increased risk of infection. Postpandemic, there is a risk of bouncing back to these workflows. The pandemic gives us a unique opportunity to use the experiences of the pandemic to improve care, improve access to care, and reduce costs. (See detailed Recommendations-Next steps at the end of this document).
This document builds on the previously reported work. 1,2 It can be used as a guide to the application of these technologies in the current and future pandemics, including lessons learned from the team participants (Table 1) and the health care providers interviewed.
List of Subject Matter Experts
The critical issues created by the demands of the COVID-19 pandemic (Identified in the Phase 1 Pandemic Response Action Plan) are as follows: Keeping care protocols up to date. Keeping the hospital open (operations, care delivery, quality, revenue) Diverting the potentially infected before they arrive at the hospital. Providing for critical staff needs – temporarily or permanently replace infected staff or staff due to infection or personal or family medical leave COVID-19 containment in the hospital/clinic Providing access to urgent care, ongoing care/follow-up care for current patients (hospital, private practitioners, rehabilitation, etc.) Providing care at home, create ability to rotate patients out of the hospital to make room for monitoring more critical cases, (monitoring, RPM, CDM, address technical issues, care support, monitoring, deal with issues of isolation and quarantine/patient safety) Supporting remote work for staff Supporting behavioral health needs (support for patients, community; and addressing needs and fears of staff) Transportation (replacement of current options that may no longer exist or be practical for people, patients, supplies, treatment equipment, critical pharmaceuticals) Public health (providing support for community communications, accurate information, training to the community)
Summary Findings-What Did We Learn?
GENERAL OBSERVATIONS
The availability and use of telemedicine rose radically in response to the COVID-19 pandemic. This leveled off during June and July of 2020 at about 38 times the volume before the beginning of the pandemic. 3 This rapid growth was driven by 4 factors: (1) Necessity and patient demand; (2) Centers for Medicare & Medicaid Services (CMS) waivers; (3) Providers rapidly making the services available; and (4) State reimbursement policies encouraging the use of telemedicine. An excellent example is Medicare providers’ rapid increase in offering telehealth services to Medicare beneficiaries:
As per the interviews and task force experiences as well as research by others, including the Kaiser Family Foundation, a large majority of providers used telemedicine during the pandemic (See Fig. 1). The majority converted almost the majority of encounters to virtual (audio or video) early in the pandemic out of necessity addressing a variety of needs/situations.
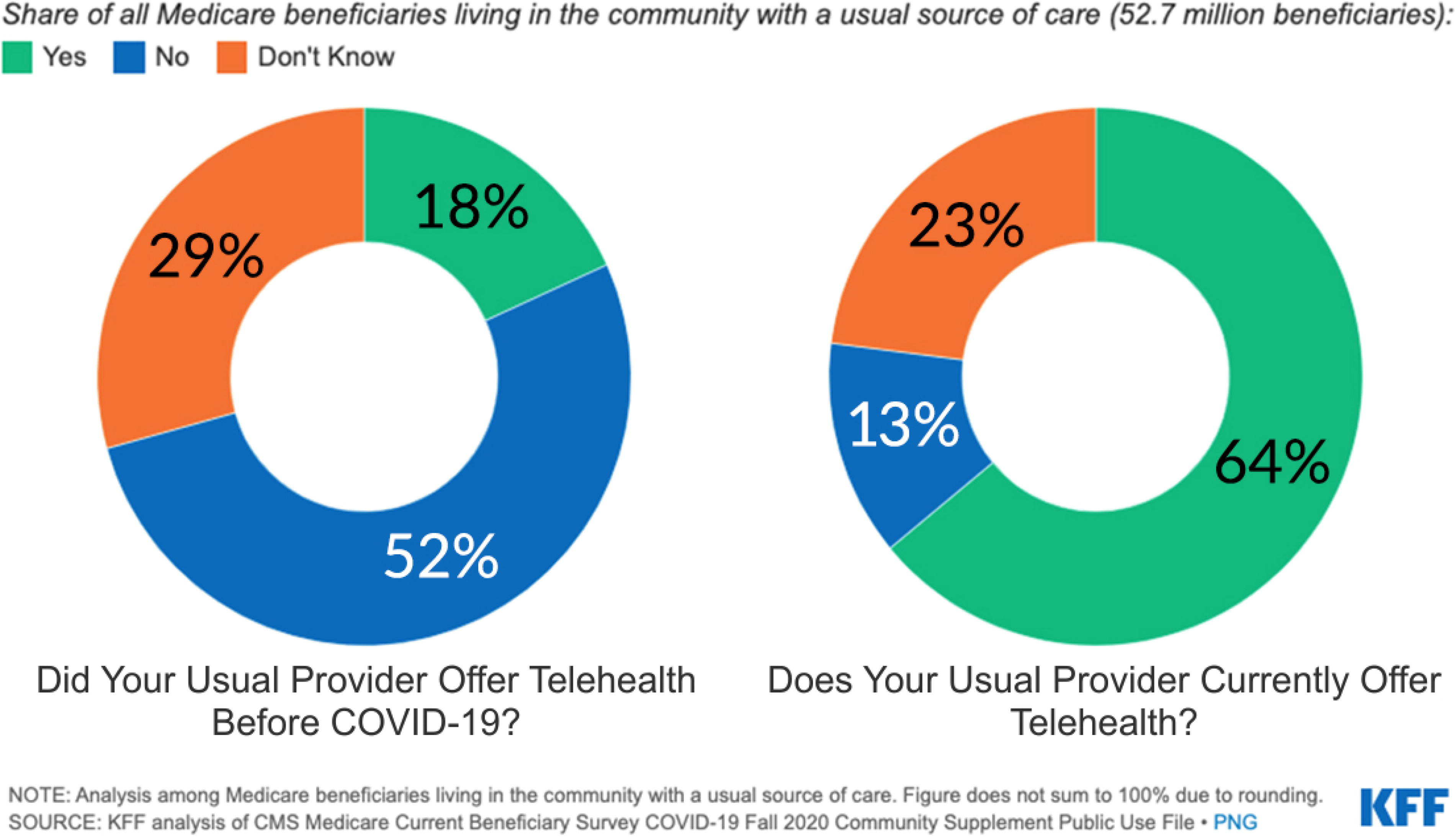
Share of all Medicare Beneficiates living in the community with a usual source of care. 4
CMS’s waiver of coding/billing restrictions and implementation of payment parity with in-person encounters was very successful and represents timely, sound decision making early in the pandemic by CMS and others.
During the COVID-19 pandemic Telehealth was used broadly, nationally and in high volume for the first time. This creates an exceptional opportunity for health care providers, CMS and state Medicaid programs to gather data and make future decisions based on true cost and true value.
Gaps remained
In-person procedural encounters were stopped or sharply curtailed.
A minority of providers were unable, or chose not, to use telemedicine. 5
A minority of patents were unable, or chose not, to use telemedicine or faced disparities in accessing telemedicine services. 6
Disruptions in the continuum of care resulted in increase rates of health decline and/or death in populations with chronic diseases (example: congestive heart failure). 7 Telemedicine and related technologies should have been applied more broadly to identify and mitigate the indirect health effects of epidemics. This requires more study (see Fig. 2).
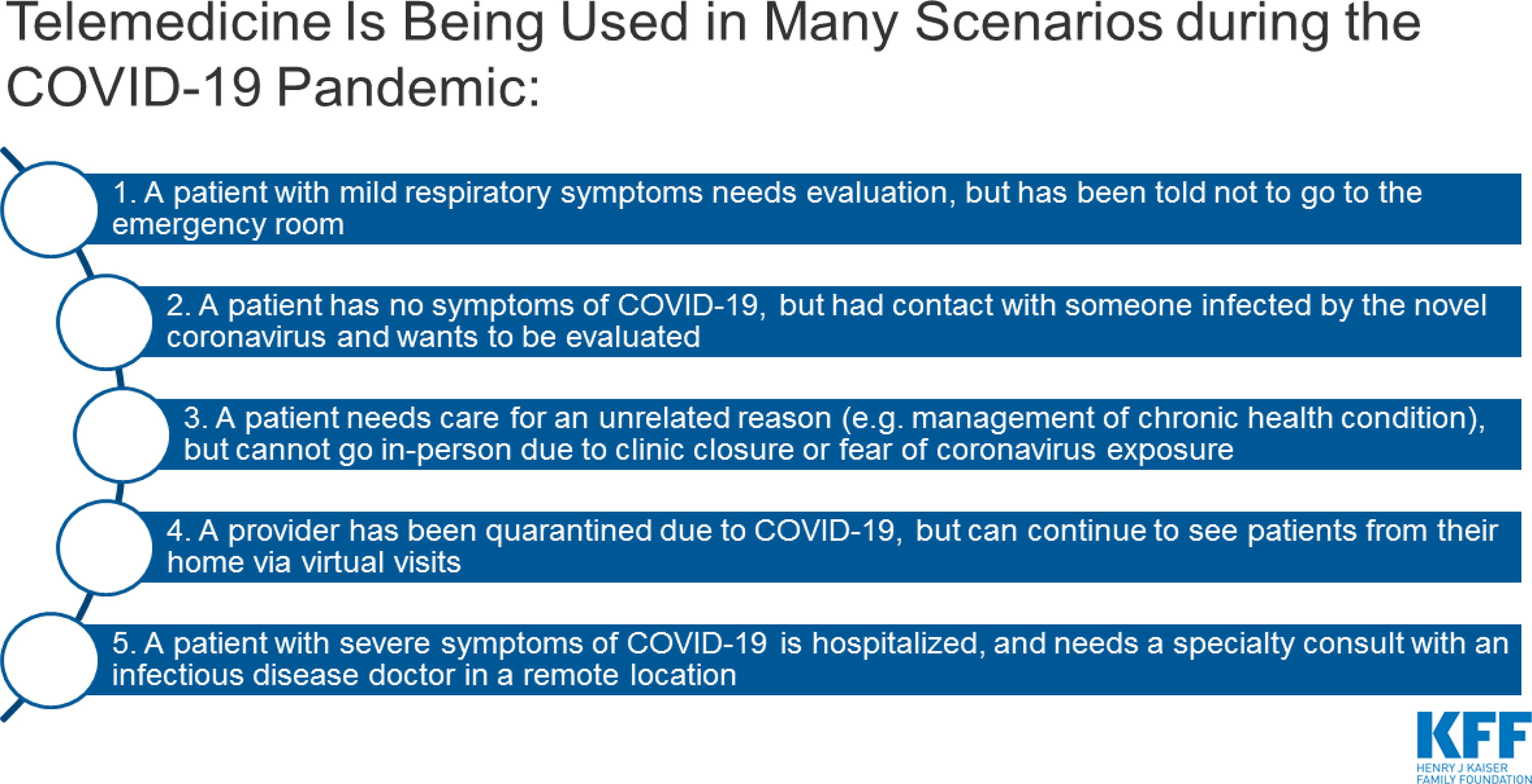
Telemedicine use in various scenarios during the COVID-19 pandemic. 5
The experience of the COVID-19 pandemic put exceptional stress and trauma on providers. The intense time demands, increased exposure to death, and fear for their own safety and the safety of their families and coworkers resulted in low morale, burnout, and post-traumatic stress disorder (PTSD). Anxiety about the system (“the experts did not listen”) and their jobs further complicated behavioral health issues. It appears that very little of this situation has been resolved. The impact, including increased resignations, may be just in its early stages. Up to 1/3 of health care workers are now considering leaving health care. This is extensively supported by current literature. 8 –10
Public health’s efforts to educate the community and encourage vaccination were severely disrupted by political conflicts and false messaging. Low vaccination rates have created an environment for the pandemic to linger and COVID-19 to mutate, creating variants that are more infectious and more easily transmissible, even in some vaccinated individuals.
What Were the Top Barriers or Challenges?
Identified during the Pandemic Response Action Plan development and from the actual COVID-19 experiences of those responding to the interviews and questionnaires
Keeping up with and communicating constantly changing care protocols and establishing a source of “truth.”
Delivering patient care services especially for chronic disease patients, resulting in higher fatality rates.
Mental health support for patients, staff, and families.
Reducing infection exposure for patients, staff, and families.
Transportation of patients, staff, and supplies became difficult or unavailable due to COVID-19 pandemic restrictions.
Cost, availability, and inventory control of PPE and competition within the community for limited supplies.
Cost and availability of replacement staff. Small and nonprofit providers had little access to replacement staff or locum tenens, as they were out-bid by larger institutions.
Historic restrictions on Medicare reimbursement for telehealth before the pandemic had constrained the adoption and use of telehealth. This lack of experience hurt the ability to transition to telehealth during an emergency.
Decreased revenues due to reduced utilization and suspension of elective procedures made it harder for facilities to make potentially expensive changes in patient intake and conversions to telehealth.
Rapid implementation of virtual care to scale was challenged by: Lack of experience. Lack of standard or established telehealth workflows. Lack of standard and/or established video platforms leading providers to use whatever was available (transitioning to a shared platform remains a challenge).
The need for rapid dissemination of training and support across entire organizations.
Challenges to increasing patient access to telehealth included: Informing patients that telehealth services are available. Broadband, internet access connectivity to the home, especially in rural areas or underserved urban areas. This was complicated by competition within the home for internet access for health care, education, and work especially during the height of the pandemic. Access to technology, especially among underserved populations (rural and urban). Technical or “digital literacy” especially among the elderly. Informing and educating the general public regarding the dangers of COVID-19 and the importance of vaccine and safety methods (e.g., wearing masks, cleaning hands, etc.) in the face of disinformation, established fears, ignorance, and the public perception of pharmaceutical companies (suspicions of big business).
What Are the Top Lessons Learned?
Experience with and/or existing telemedicine services provided substantial advantages when the pandemic struck. None of the health care providers interviewed had a truly comprehensive, broad, scalable telehealth model in place before the COVID-19 pandemic. However, organizations that had some level of telemedicine in place before the pandemic had a significant advantage over those organizations who had little to no experience with telemedicine. This argues that to give providers more resilience during a pandemic telehealth must be part of providers’ daily care operations as well as every public health operation. It should also be part of every facility’s and region’s strategic and disaster recovery plans as part of the toolkit “response fabric” in disaster recovery planning and action. The COVID-19 experience showed us that this is a national necessity and funding, guidelines, and support should be provided accordingly.
Assumptions that providers or patients would not do or accept virtual visits were proven largely wrong. It was found that a majority of patients engaged and liked the convenience and safety of receiving health care visits in their home (e.g., reduced travel, reduced risk of exposure to COVID-19).
Admitting to the scale of the problems early and assembling productive cross-functional teams proved essential. Prepandemic contingency or disaster recovery plans were not effective in this type of an emergency. Assembling highly functional rapid implementation teams was required to address this new challenge. Also, drawing on critical resources outside the hospitals proved essential. For example: early engagement of your community’s broadband providers is critical and productive. Where this was done, the broadband providers responded positively.
DETAILED OBSERVATIONS
COVID-19 forced organizations to innovate and expand service delivery methods.
Telemedicine in place gave organizations considerably greater resilience in the crisis.
Telehealth offered a way to maintain continuity of care, 11 revenues, and viability.
Providing virtual rounding and visits to inpatients using simple tablet technology delivered multiple benefits at a relatively low cost: Reduced infection exposure. Radically reduced the consumption/cost of PPE. Reduced patient isolation from family and caregivers.
Disparities in accessing telehealth care driven by varied access to broadband and devices, financial capacity, and digital literacy (or lack of…especially among older patients and new immigrant populations) remain.
If we treat the use of telehealth as a fire alarm (e.g., use only in case of emergencies), then the good ground gained will be lost as care reverts back to traditional workflows. However, if we look at telehealth as a sea change in how care should be delivered, then we can leverage the gains made.
In addition, it is the observation of the project team that:
The impact of COVID-19 on hospital staff remains largely unresolved and cannot be overestimated. These need to be addressed or a significant turnover of labor may result.
Public health is underfunded and often under supported by political leaders.
The current local and regional approach to disaster response is not effective in dealing with a pandemic.
There is a lack of consistency and efficient data collecting and sharing systems in public health and this hindered response.
What Are the Top Activities That Will Continue after COVID-19?
Both provider and consumer perceptions of telehealth are changing, creating significant opportunities. 12
There will be no complete return to the “Old Normal.”
Patients are rethinking how to access the services they need without leaving home—consumer expectations for telehealth are increasing.
Health care organizations are more rapidly moving toward virtual care, redesigning care models and incorporating telemedicine.
Progressive health care organizations and academia are training providers, fellows, residents, and students in how to use telehealth and interact with the patient in virtual consults. This has become essential.
Health care providers and other organizations are marketing virtual services to the community to generate greater community engagement. As health care entities offer more virtual services, old geographic barriers/boundaries will begin to fade, consumers will have more options and, therefore, competition for market share will increase and virtual care is an important, competitive tool.
What Are the Top Factors for Success?
Necessity drove innovation—The ability to innovate drove success.
CMS waivers and expansion of coverage were critical and successful:
Payment parity with in-person care reimbursement was a critical decision by CMS, state and private insurance was essential for most providers, especially independent practitioners, to remain solvent during the early part of the crisis. It also was a significant behavioral motivation.
This was an example of good and responsive policymaking.
Executive commitment and support as well as committed champions and informal leaders.
Effective state and local public policy that supports telemedicine.
Having some telemedicine in place before the pandemic increased the organization’s resilience and made rapid conversion to virtual care much more viable.
Effective cooperation between health providers, Public Health, and political leaders.
SUMMARY OBSERVATIONS
The “assumption” of provider resistance identified as a barrier to the use of telemedicine, turned out to be a false assumption. Most providers pivoted quickly to telemedicine.
Providers started with whatever communication technology they had (Skype, FaceTime, Zoom, etc.) and as time went on, the systems worked to bring then back to using standard systems
Needs a closer look—What are patients and providers most comfortable with? Is there an opportunity here?
Patient Intake forms should include: What devices do they have or prefer? Will they do telemedicine? Do they have an internet connection? These are now essential parts of demographic information.
It is important that the incentives for at-risk plans be addressed and virtual visits be counted, recognized, accepted, and risk scored (and contribute to STAR rating)
Rounding virtually with pads-on-a-pole was valuable in multiple ways (see lessons learned above)
Tele-ICU was valuable to expand/sustain capacity and compensate for staff shortages. This was especially true if a Tele-ICU was implemented before the pandemic. It is difficult to set up in a crisis.
There is a challenge keeping staff during the pandemic; this applies to all clinical and nonclinical staff and it appears that shortages will continue.
This needs deeper analysis. How can telemedicine help in resolving burn-out/PTSD (too many staff have seen a lot of death; have the feeling that they are languishing; needing to overcome fear and needing protection):
Alternative work settings to provide care/expertise without exposure (e.g., remote work, Tele-ICU, remote monitoring, etc.)
Mental health demand from patients, health care workers, and the general public have seen sudden increases while a shortage of providers is worsening. Telemental health appears to be a solution.
Mental health providers rapidly moved to virtual. Established telemedicine providers (example: AmWell, Teledoc, SOC) have seen substantial increase in demand for mental health consultations. Additional specialized mental health telemedicine providers have emerged or are growing rapidly.
More attention to this is critical. This needs deeper analysis. Are these services a solution for this demand? What are the advantages and limitations? If yes, how can they be applied, made available? What incentives are needed for their use and their provision?
Voice only was valuable and necessary during the pandemic and should be accepted in select circumstances.
Current innovation curve steps/factors for telemedicine appear to be:
Implementation (forced by the pandemic) into normal workflows.
Proved to be a tool that works.
Increased interest in innovation in health care especially for digital technologies to improve logistics and provision of care.
Patient demand and expectations are changing and expected to drive more innovation.
Policy is lagging behind both needs and what is already going on. Broader action and benefits are waiting for policy.
Conclusions
The impact of the COVID-19 Pandemic was severe and identified multiple critical challenges and weaknesses. Applying the approaches, tools, and technology outlined in the
Most weaknesses that COVID-19 exacerbated already existed before the pandemic. Most were already well known but had not been addressed. Few of these core issues have been resolved as a result of the pandemic. These include: staff shortages as well as antiquated and inefficient workflows/service delivery strategies. This was complicated by the failure to adopt new technologies, and poor coordination of information.
Postpandemic, there is a risk of bouncing back to old workflows. The pandemic gives us a unique opportunity to use the experiences of the pandemic to improve care, improve access to care, and reduce costs.
EXAMPLES
Replace In-Person visits when “In-Person” is not necessary—much of Primary, Urgent Care, and Mental Health transitioned from In-person to virtual out of necessity during the pandemic. This was very productive. Unfortunately, some specialty clinics appear to remain locked into ‘In-person”.
Physical waiting rooms persist even though they have long been known to expose patients and staff to infection. In addition, items in waiting rooms directly and negatively impact patient satisfaction and provider’s scores. 14 In response to the pandemic, many practices transitioned to virtual waiting rooms (virtual cueing). Using these systems, patients completed registration online, checked in through text and were called into the office when the clinic notified them. This also eliminated the need for a waiting room and related expenses.
“The clipboard” persists—Almost every visit to a provider has required that the patient be handed a clipboard for decades. The patient then fills out paper forms manually. This is despite well-established evidence that online registration is more convenient for both the patient and practice, improves patient engagement, and is more accurate and complete. Implementing on-line registration cuts the staffing requirements as well as the cost of manual data entry and resulting data error correction. Even during the pandemic, many specialty encounters still appeared to require this paper process.
Consumer preference—Most patients prefer less complex more convenient access to care, yet United States (U.S.) health care has generally failed to respond accordingly.
Incentives drive the system. The revenue models before the pandemic focused on incentives that kept things the way they were. They did not incentivize implementing telemedicine or digital health or exploring greater efficiency or improvement of work process or staff use. They directly incentivized in-person encounters whenever possible.
There was no source of medical “truth'' for patients, providers, or the general public, which fed the misinformation campaigns of others.
Example: “HHS Protect” was well intentioned, but it exposed conflict even from the same sources of information.
The team observed that our federalist system of public health and public health information is fractured and counterproductive. 15
A single source for lessons learned and proven solutions is badly needed.
Inefficient care workflows and narrow work rules often cause excess demand on limited “high-expertise” resources by forcing them to do work that could be done by lower skilled personnel. This inflexibility proved damaging to expert staff and exacerbated the impact of staff shortages in critical areas. Work rules and decision making need to be reexamined with the specific objective of shifting appropriate decision making to more available, and often lower cost, appropriately trained staff.
The assumption that the only staff and expertise that is available is “within the facility” limited options. The use of technology to share staff and expertise from a larger pool through telemedicine solutions is critical.
Our care models are incentivized to care for patients in higher cost “facilities.” However:
Establishing technology-based patient management services, such as Remote Patient Monitoring (RPM) and Chronic Care Management (CCM) and now Hospital to Home (H2H) have proven the ability to:
improve management of patients in their home.
improve care and reduce hospitalization and cost.
Reduce “high-expertise” resource demands.
These programs greatly increased flexibility and assured an improved continuum of care both in and outside of a pandemic. They also reduce cost.
Home-based care should be the first choice when appropriate. Financial incentives should support this.
Hospitals that had telemedicine and digital health programs before the pandemic showed greater flexibility and capacity to adapt workflows to the challenges of the pandemic.
Challenges of technical literacy and availability remain.
Incentives should reward overcoming these challenges and creating a more consumer-friendly process.
The cost, complexity, patient dissatisfaction of health care plus changing demographics and expectations (driven to some degree by expectations set in other industries) make health care ripe for disruption. Health care is the largest business sector in the United States, which makes it a worthy target for disruptors. If the current U.S. health care system fails to adapt, fails to control its costs, fails to deliver on the expectations of consumers, then disruption will most likely come from outside the current health care systems. This requires additional study.
RECOMMENDATIONS: NEXT STEPS
Preserve the advancements achieved during COVID-19—Maintain the incentives to motivate and sustain behavior. To CMS, State Medicaid, and Private payers: Maintain reimbursement at the same rate for virtual and in-person for at least 2 years beyond COVID-19. Encourage the continued use of telehealth and digital health tools through incentives, policy, and messaging. Use this experience as a valuable opportunity to gather and examine the data of this first and only broad utilization of telehealth. Standardize telehealth data collection. For the first time, we now are in a position to collect the largest body of telehealth data that we have had to date from both breadth and volume of use. Look at this experience not just from a perspective of utilization (significant increase in telehealth visits) but the clinical and economic impact of those visits. Determine what went poorly, where telemedicine failed or fell short, what are new recognized limitations, etc. Use this opportunity to determine the true value and costs of telemedicine and set policy, reimbursement, and other incentives accordingly. Call for robust research into the impact of telehealth during COVID and what” best practice” might look like in the future. We know we spent less during COVID-19. Did telehealth contribute to that? We know non-COVID-19 patients used the emergency room less frequently. Did telehealth contribute to that? We know that fewer specialists were seen “in-person” and fewer elective procedures done. Did telehealth fill in the gaps and preserve or improve health? Where else can telemedicine and the application of digital health tools be applied to address issues of access, equity, efficiency, quality, and cost? Make implementation of telemedicine and virtual workflows an essential part of contingency preparation and planning. Make surge capacity an essential measure of resilience as well. (HHS, American Hospital Association (AHA), Joint Commission, etc.). Examine current workflows with the specific objective of increasing efficacy, including the appropriate/efficient use of staff and technology. Encourage a more expansive relationship with patients to improve care and reduce the need for in-person visits. Integrate Remote Patient Monitoring, Chronic Care Management, and Care Coordination into care wherever appropriate. Integrate mental health into care practice. Integrate Social Determinants of Health into care planning. Examine and assess a ‘virtual first” strategy. Apply in-person only to the patients that need it. Ask which patients really need care in a care facility. Eliminate barriers: Expand telemedicine beyond just video encounters. Meet the patient where they are. Encourage the use of store and forward, voice and cell phone video applications, etc. where appropriate. Assure that “expansion of broadband” meets the specific requirements of health care Remove geographic restrictions for telemedicine acknowledging that underserved communities are just as likely to be urban as rural. Set reimbursement policy to motivate service reinvention. Fund research of the potential consumer-oriented disruptors to health care delivery. Identify and examine these new or proposed business designs. Learn from them and create incentives that drive innovation. Prepare and plan for disruption. Create a central national source of truth for medical/public health information during a pandemic to give a basis of public discourse and to assure up-to-date care. Continue postpandemic to help providers adjust and to address long-term conditions (Example: Long COVID). Align the messaging of the CDC, National Institutes of Health (NIH), Health and Human Services (HHS), Public Health, and provide a reliable “single source of science-based truth.” Encourage potentially helpful legislation (some is already in process). Create and implement a single consistent system for gathering and measuring Public Health information and fund accordingly. Set training standards to include new technologies and workflows to deliver care in every health care profession.
Traditional workflows result in higher cost, lower patient satisfaction, lower outcomes, and often expose patients and consumers to increased risk of infection. As reflected in this study, telemedicine and other digital health solutions can reduce demand on critical resources; reduce health care inequities; improve outcomes 16 and quality as well; and improve patient compliance, satisfaction, and loyalty. They should be implemented into the daily workflow and business of health care.
Footnotes
Disclaimer
This document does not represent the opinion of Health Resources and Services Administration (HRSA), Federal Office of Rural Health Policy (FORHP), Office for the Advancement of Telemedicine (OAT), Alaska Native Tribal Health Consortium (ANTHC), the Telemedicine Resource Centers (TRCs), or any other grant-funded entity. It comprises suggestions and opinions of experts in the fields of telehealth, epidemiology, public health, nursing, hospital administration, and policy/regulatory who worked together to create this documentation of “lessons learned.” For more information regarding this publication, or to learn more about Telehealth, please contact TTAC at www.telehealthtechnology.org, or your regional TRC or the National Policy Telehealth Resource Center. The 12 regional and 2 national telehealth resource centers (TRCs) that provide assistance, education, and information to organizations and individuals are actively providing or interested in providing health care at a distance. You can find your regional or national telehealth resource center through the national consortium of telehealth resource centers (NCTRC), which comprises all 14 telehealth resource centers. The NCTRC website is ![]() .
.
Disclosure Statement
No competing financial interests exist.
Funding Information
This publication (report, briefing article, document, etc.) was made possible by grant number