
Abstract
Introduction:
Telemedicine has the potential to improve abortion access disparities in Canada. We aimed to explore the provision of telemedicine for first-trimester medical abortion and related barriers in 2019.
Methods:
We conducted a national, cross-sectional, anonymized, web-based survey of clinicians who provided abortion care in 2019 in Canada. We distributed our survey through professional health organizations to maximize identification of possible eligible respondents and used a modified Dillman technique to foster responses. Questions elicited provider demographics, clinical characteristics, including telemedicine first-trimester medical abortion and perceived related barriers. Descriptive statistics were analyzed using R software.
Results:
Among 465 respondents, 388 reported providing first-trimester medical abortion across Canada; 44.0% reported experience using telemedicine for some components of care: 49.3% of primary care clinicians and 28.7% of specialists. Telemedicine was used for initial consultation (86.0%), prescription (82.2%), or follow-up (92.2%). The median percentage of telemedicine providers' patients who underwent a dating ultrasound was 90.0. The majority usually followed up with patients through quantitative human chorionic gonadotropin (hCG) (84.2%). Seventy-eight percent perceived barriers to telemedicine; the most common being inability to confirm gestational age with ultrasound (43.0%), and lack of provincial telemedicine abortion fee code to pay practitioners (30.2%), timely access to serum hCG testing (24.6%), and nearby emergency services (23.3%).
Discussion:
In 2019, fewer than half of respondents reported providing some aspects of first-trimester medical abortion through telemedicine and the majority perceived barriers. Our results can inform knowledge translation activities to reduce barriers and increase telemedicine abortion care in Canada.
Introduction
Abortion care is an essential health care service in Canada, with ∼84,000 abortions provided annually. 1 The United Nations Human Rights Commissioner expressed concern over inequitable access to abortion across the country. 2 Rural–urban abortion access disparities, with services lacking in the vast rural areas, were also highlighted in our first iteration of the Canadian Abortion Provider Survey (CAPS) in 2012. 3
A mifepristone–misoprostol regimen, the gold standard for first-trimester medical abortion, became available in Canada in 2017. 4 Shortly thereafter, Canada removed restrictive regulations, thus permitting mifepristone prescribing and dispensing as for other prescription medications, facilitating medical abortion care. 5 Although federal regulations required an ultrasound before prescribing mifepristone until April 2019, 6 the Society of Obstetricians and Gynaecologists of Canada 2016 medical abortion clinical practice guidelines included support for pregnancy dating options in the absence of ultrasound availability and telemedicine for follow-up care. 7
Telemedicine uses information and communication technologies to improve patient outcomes by increasing access to care and medical information compared with in-person care. 8 Emerging data suggest that there has been a substantial increase in the proportion of first-trimester medical abortion among all abortions from 3.6% in 2012 to 27.7% in 2019 in Canada and to 31.4% in 2020 in Ontario. 9 –11 The introduction of the mifepristone–misoprostol regimen and removal of restrictive prescribing and dispensing regulations in Canada has enabled telemedicine medical abortion.
Emerging evidence supports telemedicine provision of medical abortion as safe, effective, and acceptable. 12,13 Telemedicine medical abortion, especially low-/no-test protocols that do not rely on ultrasound availability, has the potential to improve accessibility of abortion services, especially for rural and remote patients. Eligibility for low-/no-test protocols usually includes certainty of last menstrual period by which the gestational age is <70 days and the absence of risk factors for or symptoms of an ectopic pregnancy. 14 –16
Canadian data on the use of telemedicine for first-trimester medical abortion, the number of abortion providers, and barriers to providing this care are limited. A retrospective Canadian study compared telemedicine medical abortion with in-person medical abortion obtained between 2017 and 2019 at a single clinic. 17 Physicians provided care virtually, and only obtained dating ultrasounds when clinically indicated. Follow-up included serum human chorionic gonadotropin (hCG) testing for all participants.
Efficacy and safety were similar in both groups, but remote patients more often initiated unscheduled communications. 17 Respondents to a survey of first-trimester medical abortion providers in Canada during COVID-19 reported some adoption of the low-/no-test protocol. 14,18 The majority ordered ultrasound only as indicated (81.2%), but still always ordered serum hCG or hemoglobin (59.6% and 55.6%, respectively). 18 The survey, however, did not explore details of the care the respondents provided nor barriers to telemedicine, which continue to be understudied in Canada.
Our objective was to study the first-trimester medical abortion Canadian workforce in 2019, their provision of telemedicine abortion care, and their perception of barriers. These data can inform knowledge translation activities to remove barriers and improve equitable access to abortion care.
Methods
We conducted a pan-Canadian survey of physicians and nurse practitioners who reported abortion services provided in 2019. We collected data between July and December 2020.
SURVEY INSTRUMENT
Our team created the CAPS by updating and adapting previous instruments 3,9,19 to account for the recent availability of mifepristone, and updated clinical care guidelines. 7 We conducted a national, cross-sectional, web-based survey, available in English and French. 19 The survey started with a consent statement, followed by sections exploring respondent demographics and their reported clinical characteristics of abortion care. We included questions on use of telemedicine for first-trimester medical abortion and related barriers, which we report on in this article. We reminded respondents throughout the survey that the questions pertained to care provided in the calendar year of 2019 and thus pertained to pre-COVID-19 care.
CAPS was hosted by the British Columbia Children's Hospital Research Institute's Research Electronic Data Capture platform. 20 The University of British Columbia Research Ethics Board approved this survey (H18-03313).
RECRUITMENT
Physicians and nurse practitioners were eligible to participate if they provided abortion services in 2019. Canada does not systematically record the number of abortion providers. Therefore, we were unable to identify a comprehensive list of abortion providers to invite to the survey. To reach as many eligible clinicians as possible, we distributed a generic survey link through multiple collaborating health care professional organizations and networks such as the College of Family Physicians and the Society of Obstetricians and Gynaecologists, and the Canadian Nurses Association, which are home to all possible respondents. We employed a modified Dillman 21 technique sending email reminders through our partnering organizations 1, 2, and 4–6 weeks after the initial invitation to optimize our response rate. Respondents could request remuneration (CA $50 gift certificate).
DATA CLEANING AND STATISTICAL ANALYSIS
We conducted an anonymized, web-based survey with a generic link invitation and offered remuneration. We, therefore, screened incoming responses for fraud to exclude those submitting nonsensical answer combinations. To exclude fraudulent responses, we adapted and combined multiple validated fraud detection approaches into a fraud detection algorithm, which we describe in detail elsewhere. 22 During data cleaning, we removed noneligible and fraudulent respondents. 22 Figure 1 depicts the respondent flow chart informed by the supplementary data checklist. We used R statistical software to generate descriptive statistics, and where appropriate present proportions or medians with interquartile ranges (IQRs). 23
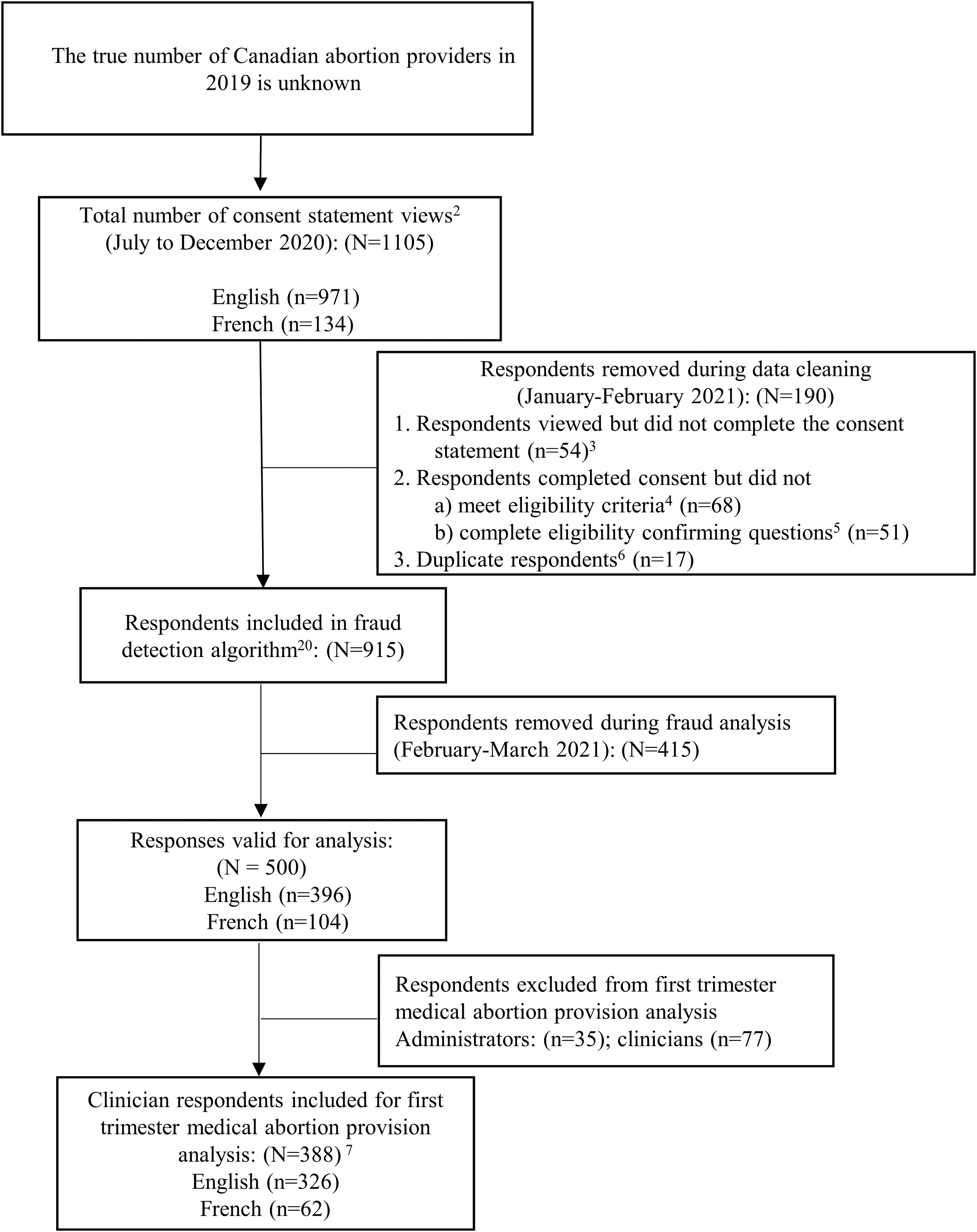
CAPS respondent flow chart for telemedicine first-trimester medical abortion care.1 1This flow chart is informed by the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).35 2Consent statement view recorded on Research Electronic Data Capture (REDCap) platform. 3 The participation rate was 95.1%. 4 The initial mandatory survey questions verified respondents' eligibility. If responses did not match the eligibility criteria, respondents were automatically exited from the survey. This included a question confirming that they had not taken the survey before. 5 Manual removal of respondents who exited the survey before completing mandatory eligibility questions. 6 Duplicate analysis was conducted using R Statistical software, flagging matching demographics, followed by manual review of all flagged respondents. We did not collect IP addresses or use cookies, per our research ethics board (REB) request, to maintain respondents' anonymity. 7 Completed the survey (n = 346), defined as completing the first-trimester medical abortion survey section. Completing the entire survey took between 30 and 80 min depending on the range of abortion services respondents provided, programmed using skip pattern logic based mostly on mandatory questions. Respondents could change answers on their current screen, but not go back to prior screens. The completion rate for the first-trimester medical abortion survey section was 89.2%. The survey contained mandatory and nonmandatory questions (to increase survey completion rate). We included questions with missing responses in the analysis. CAPS, Canadian Abortion Provider Survey; MA, medical abortion.
Results
SAMPLE DESCRIPTION AND WORKFORCE
We included 465 clinician respondents for final analysis, of whom 388 reported providing first-trimester medical abortion. Forty-four percent of these provided some components of first-trimester medical abortion care by telemedicine in 2019; 49.3% of primary care clinicians and 28.7% of specialists. Table 1 shows first-trimester medical abortion respondent demographics broken down by providers and nonproviders of telemedicine.
Canadian Abortion Provider Survey Providers and Nonproviders of Telemedicine First-Trimester Medical Abortion Care
Percentages were calculated based on the total number of respondents for the individual variable (based on skip pattern logic and nonmandatory questions).
Did not report totals to maintain respondents' anonymity.
Primary care physicians include FPs and EMs who have family medicine certification.
Specialists included obstetricians and gynecologists as well as maternal-fetal medicine subspecialists.
Prairies include Alberta, Manitoba, and Saskatchewan.
Atlantic Provinces include New Brunswick, Nova Scotia, Newfoundland & Labrador, and Prince Edward Island.
Territories include North West Territories, Yukon, and Nunavut.
We defined urban providers and facilities as those located within Statistics Canada's defined CMA. All other providers and facilities were classified as rural. To maintain respondent anonymity, we reported geographic results by regions (British Columbia, the Prairies, Ontario, Quebec, the Atlantic Provinces, and the Territories), combining some low respondent number provinces. For the same reason, we grouped FPs, EMs into a “primary care physician” category when reporting results by specialty in this table.
CAPS, Canadian Abortion Provider Survey; CMA, census metropolitan areas; EM, emergency medicine physician; FP, family physician; MA, medical abortion.
British Columbia had the highest proportion of telemedicine providers (63.8%), while Quebec had the lowest (10.7%). Telemedicine providers were more common among nonhospital-based respondents (55.3%) than hospital based (26.3%), and among those with <5 years' abortion care experience (50.9%) than those with more experience (30.4%). Nonhospital-based respondents provided abortion services in a range of facilities, including freestanding dedicated abortion clinics, reproductive health clinics, or in their private practice.
CLINICAL CARE OF TELEMEDICINE PROVIDERS
Table 2 shows characteristics of telemedicine abortion services, including which components of care (initial consultation, medication, and follow-up) respondents provided through telemedicine. Seventy-six percent provided all three components of care for some patients. We asked clinicians to estimate the percentage of patients for whom they obtained a dating ultrasound. The median reported percentage was higher in rural (100%; IQR 78.8–100.0) than in urban (80%; IQR 20.0–100.0) respondents.
Clinical Characteristics of Canadian Abortion Provider Survey Telemedicine Abortion Care
Percentages were calculated based on the total number of respondents for the individual variable (based on skip pattern logic and nonmandatory questions).
Respondents could select >1 answer option.
hCG, human chorionic gonadotropin; IQR, interquartile range; Rh, rhesus.
The majority of telemedicine providers (81.6%) reported requesting a dating ultrasound for their telemedicine and in-person care patients. The majority of those (80.9%) accessed ultrasound through a diagnostic imaging department in their health region or hospital. The remainder accessed ultrasound in the clinic they worked at. Reported percentage of patients who underwent preabortion urine hCG testing was higher in urban (70.0%; IQR 0.0–100.0) than in rural (0.0%; IQR 0.0–100.0) respondents, while urban and rural respondents did not differ in serum quantitative hCG, rhesus (Rh), and hemoglobin testing.
The majority of respondents usually followed up with patients through quantitative serum hCG testing (84.2%) and/or telephone appointment (56.4%). Rural respondents reported less use of ultrasound for follow-up (10.5%) and more quantitative serum hCG testing (94.7%) compared with urban respondents (14.9% and 77.0%, respectively). First-trimester medical abortion respondents estimated that patients infrequently required a uterine evacuation after a mifepristone–misoprostol medical abortion (median 2%; IQR 0.0–5.0); most often for an ongoing viable pregnancy (85.9%) followed by symptomatic retained products of conception (81.5%). Some respondents offered first-trimester medical abortion in person or through telemedicine to patients who lived >2 h from emergency uterine evacuation (31.9%) and from an emergency department (16.3%), respectively.
BARRIERS TO PROVIDING TELEMEDICINE MEDICAL ABORTION
The majority of all first-trimester medical abortion respondents (77.7%) perceived barriers to telemedicine; 92.5% among nonproviders of telemedicine. Table 3 shows barriers perceived by telemedicine providers versus nonproviders. The largest difference in reported barriers between nonproviders and providers was regarding lack of ability to confirm gestational age with ultrasound where the patients live, lack of ability to order serum hCG testing, and lack of telemedicine equipment. Rural respondents did not report more barriers than their urban counterparts.
Perceived Barriers Among Canadian Abortion Provider Survey Providers and Nonproviders of Telemedicine First-Trimester Medical Abortion Care
Respondents could select >1 answer option; percentages were calculated based on the total number of respondents for the individual variable.
Did not report totals to maintain respondents' anonymity.
CAPS, Canadian Abortion Provider Survey; GA, gestational age; hCG, human chorionic gonadotropin; MA, medical abortion.
Among all first-trimester medical abortion providers, respondents in the Prairies (47.2%) and Ontario (40.4%) more commonly reported lack of a telemedicine medical abortion fee code. Hospital-based respondents more commonly reported an inability to access mifepristone (23.0%) than nonhospital-based respondents (10.7%). Access to dating ultrasound was more commonly a barrier for those hospital based (61.0%) as well as those in Quebec (64.3%) and in the Territories (63.6%). Lack of access to serum quantitative hCG testing was the highest in the Territories (63.6%) and in hospital-based respondents (39.0%).
Lack of access to emergency services was highest in the Territories (81.8%) but was only slightly higher in rural (26.2%) than in urban (20.4%) respondents. Quebecois respondents were most likely to report provincial regulations being a barrier (16.1%). Multiple respondents (16.1%) listed other barriers in a free-text field. Recurring themes of these were personal preference or comfort level, lack of guidelines/guidance, and not having enough time in their schedule. Others said they felt it was difficult to assess patients' mental state or abuse exposure, and worried about not performing a physical examination, lack of effective communication over the phone, and patient confidentiality.
Discussion
Our results show that in 2019, before the COVID-19 pandemic, adoption of telemedicine as a method to deliver medical abortion was modest, with 44% of 388 first-trimester medical abortion provider respondents having experience using telemedicine for some components of care. The adoption of telemedicine increased to 88.9% according to a survey of abortion providers in Canada during COVID-19. 18 Of those providing care through telemedicine, most had experience providing initial consultation, prescription, and follow-up care, though not all three components might have been provided for all patients via telemedicine by individual survey respondents.
We observed a high uptake in medical abortion provided in primary care and rural settings after mifepristone became available in Canada. 10 Among rural respondents, we reported that 44% of first-trimester abortions were provided medically compared with 25.6% in urban areas. 10 In our analysis, rural and urban respondents reported similar adoption of telemedicine and similar experience of barriers. Our survey did not determine whether urban telemedicine providers delivered care to patients in rural areas.
Canadian studies have documented rural patients seeking care among urban abortion providers for surgical abortion. 24,25 We hypothesize that telemedicine medical abortion provision for rural patients could have addressed some of the previously described access disparities. 3 An Australian qualitative study demonstrated that rural patients had severely limited access to in-person abortion care, which improved with telemedicine medical abortion. 26
CLINICAL CARE
Almost all telemedicine medical abortion providers still obtained preabortion ultrasound, quantitative serum hCG, Rh, and hemoglobin testing. This corresponds to the Society of Obstetricians and Gynaecologists of Canada 2016 medical abortion clinical guideline suggesting this testing for most patients, and to Health Canada regulations requiring a dating ultrasound until April 2019. 6,7 Scientific articles describing use of telemedicine for medical abortion before the COVID-19 pandemic also showed that telemedicine was mostly restricted to history taking, decisional process, and consent. 12,13
Since then, the COVID-19 pandemic has been a catalyst for developing telemedicine abortion protocols nationally and internationally. 14 –16,27 –30 In April 2020, the Society of Obstetricians and Gynaecologists of Canada recommended use of a low-/no-test medical abortion protocol through telemedicine. 14 Low-/no-test protocols primarily rely on telemedicine appointments and patient history for preabortion assessment, and to triage for the need of testing. 14 –16,27 –30 Mifepristone/misoprostol is either obtained by the patient through mail or at a local pharmacy. Follow-up usually includes a telemedicine encounter and a home urine pregnancy test 4 weeks after taking misoprostol with additional follow-up as needed. 14 –17,27 –29,31
A move from pre-COVID-19 in-person medical abortion to telemedicine medical abortion since the pandemic onset was observed in Canada, the United States, England, and Scotland. 15,16,18,27 –29 A wide range of ultrasound uses, either as indicated by protocol or due to patient or provider preference, were reported between studies, ranging from 28.3% to 85.0% of patients. 15,27,28 The ongoing need for access to testing has been highlighted in multiple studies. In an English study, 39% of patients did not meet clinical eligibility criteria for a no-test telemedicine medical abortion and had in-person appointments with ultrasound. 16 In a Hawaiian study on telemedicine medical abortion, a third of patients elected to receive in-person care, demonstrating that it is still important to offer in-person care for those who have limited technology access, require an ultrasound, or prefer a face-to-face interaction. 28
Evidence on outcomes of low-/no-test protocols is emerging. With triage for eligibility, low-/no-test medical abortion is as effective (95.0–98.8% required no surgical intervention), safe, and acceptable as traditional in-person care. 16,27 –29
BARRIERS
Over three-quarters of our respondents perceived barriers to providing abortion care through telemedicine in 2019. Common barriers described were related to pre- and postabortion testing. Our data indicate a lack of access to testing such as ultrasound, which most respondents reported they obtained at an imaging department rather than in their clinics. These barriers further suggest discomfort among most respondents in 2019 to forgo ultrasound, possibly related to the above-mentioned regulations and clinical practice guidelines. 6,7 In a qualitative study, physicians and stakeholders described that a need to access dating ultrasounds limited their ability to provide first-trimester medical abortion, especially when local availability of timely ultrasounds was challenging. 5
Similarly respondents were hesitant to forgo Rh testing despite the 2016 SOGC guideline offering this option for early pregnancies and to test hemoglobin as indicated. 7 Data are lacking as to whether abortion providers' experience of barriers to access testing changed during the pandemic, although barriers to health care access generally increased. 32 Updating SOGC guidelines to include a hybrid in-person and low-/no-test telemedicine approach to first-trimester medical abortion paired with easily accessible education opportunities during training and thereafter for nurse practitioners and physicians has the potential to decrease testing and improve abortion access. In addition, improved access to testing especially rurally is critical as some patients will not be eligible for low-/no-test protocols.
While some respondents offered first-trimester medical abortion to patients living >2 h from emergency uterine evacuation or emergency departments, some identified lack of access to emergency services as a barrier for provision of first-trimester medical abortion through telemedicine. This highlights the need for training providers in remote areas to perform manual uterine aspiration to provide emergency services for patients experiencing complications from an early pregnancy loss or first-trimester medical abortion alike. 33
In our survey, fewer hospital-based respondents provided telemedicine, and more of them experienced barriers. We do not know if these providers lacked access to resources at their hospital or in the community of their patients, or if their threshold to forgo testing was higher than among nonhospital respondents. It is possible that in 2019, some providers did not know mifepristone/misoprostol could be dispensed at community pharmacies, or had difficulties identifying an abortion-friendly community pharmacy. While Canadian abortion researchers and stakeholders focused on implementing first-trimester medical abortion in community settings, 5 our results identified a need to better enable hospital-based abortion providers to offer first-trimester medical abortion services through telemedicine.
A lack of fee code for telemedicine medical abortion from provincial health system practitioner payment mechanisms, especially in the Prairies and Ontario, was a prominent barrier identified by our respondents. Wiebe et al. discuss that some jurisdictions in Canada did not have billing codes for telemedicine, in a similar time frame to our study. 17 Physicians identified the bureaucratic process in general, including adding the billing code for medical abortion to their payment system, as a barrier to prescribing mifepristone. 5 Unfortunately, to this date, not all provinces have established a fee code for telemedicine medical abortion (per personal communication with practitioners in various provinces).
Quebec had the lowest proportion of telemedicine providers of any region. This is consistent with prior data highlighting how unique restrictive provincial and facility policies, perceived vested interests in preserving surgical care, general uncertainty about regulations, and lack of interprofessional support have inhibited implementation of first-trimester medical abortion and have promoted surgical services, which cannot be accessed through telemedicine. 34
LIMITATIONS AND STRENGTHS
The main limitation of our survey is the inability to determine the representativeness of our sample as the number of abortion providers in Canada is unknown. Therefore, we are unable to determine our response rate. We aimed to mitigate this with our extensive recruitment method. The rigor of our sampling strategy is supported by the appropriate interprovincial ratios of respondents: we found that the highest proportion of respondents were from the most populated Canadian provinces. We detected fraudulent respondents in our survey and applied a rigorous fraud detection algorithm. 22 The key strength of our study is our national sample, recruited by partnering with multiple national clinician organizations in Canada.
Conclusions
Despite Canada's unique federal regulations including decriminalized abortion and the availability of mifepristone as a normal prescription, barriers to access to telemedicine medical abortion remained before the COVID-19 pandemic and persist. Removal of restrictive regulations on medical abortion in the province of Quebec will be required to implement medical abortion. While the proportion of first-trimester medical abortion providers in Canada who reported adopting aspects of telemedicine provision has increased from less than half in 2019 to >80% during the COVID-19 pandemic, most reported still using at least some testing.
Refinement of the Canadian medical abortion guidelines to include a hybrid in-person and low-/no-test protocol for eligible patients, paired with widely available medical abortion training and advancing virtual care options, will decrease the need for testing and increase abortion access. However, as testing will always be required for some people, access to testing will need to increase to overcome this identified barrier and to improve equitable access to high-quality first-trimester medical abortion.
Footnotes
Authors' Contributions
We guarantee that all authors have substantially contributed to this research project and article. R.M.R. is the PI on the CIHR grant funding this research and led article preparation. M.E. contributed to recruitment and article preparation, and led the data analysis. A.K. assisted with data analysis and article preparation. R.M.R., W.V.N., S.D., H.P., and E.G. conceived and designed the study with elements and revisions contributed by all authors. R.M.R. and M.E. drafted the first article, and all authors contributed to revisions and accepted the final article.
Acknowledgments
The authors thank the Women's Health Research Institute of the British Columbia Women's Hospital, the British Columbia Women's Hospital, the Society of Obstetricians and Gynaecologists of Canada, and the Canadian Nurses Association for their in-kind support.
Data-Sharing Statement
Our ethics approval has specified that none of the primary data are available to persons or agencies outside of our research team, and, therefore, cannot be accessed through anyone.
Disclosure Statement
W.V.N. was supported during this research by grants from the Canadian Institutes of Health Research and as a Scholar of the Michael Smith Foundation for Health Research, and served as a member of the board of directors of the Society of Family Planning. All authors declare we have no conflict of interest with respect to this research.
Funding Information
This work was supported by the Canadian Institutes of Health Research (PJT-162201), with Dr. Regina Renner as the Principal investigator. Drs. Dunn, Pymar, Norman, and Guilbert are coinvestigators on this grant. Dr. Norman is supported by a CIHR and Public Health Agency of Canada Chair in Applied Public Health Research (2014–2024, CPP-329455-107837) and as a Scholar of the Michael Smith Foundation for Health Research (2012-5139 [HSR]). The other authors have no additional funding to report that is relevant to this study.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.