
Abstract
Objective:
Optometrists are increasingly adopting teleoptometry as an approach to delivering eye care. The coronavirus disease 2019 (COVID-19) pandemic has created further opportunities for optometrists to utilize innovation in telehealth to deliver eye care to individuals who experience access barriers. A systematic literature review is presented detailing the evidence to support the use of teleoptometry.
Methods:
Databases of MEDLINE, Global Health, and Web of Science were searched, and articles were included if they reported any involvement of optometrists in the delivery of telehealth. Findings were reported according to the mode of telehealth used to deliver eye care, telehealth collaboration type, and the format and geographical areas where eye care via telehealth is being delivered.
Results:
Twenty-seven relevant studies were identified. Only 11 studies included the role of optometrists as a member of the telehealth team where the scope of practice extended beyond creating and receiving referrals, collecting clinical data at in-person services, and continuing in-person care following consultation with an ophthalmologist. Both synchronous and asynchronous telehealth services were commonly utilized. Optometrists were most commonly involved in ophthalmology-led telehealth collaborations (n = 19). Eight studies reported optometrists independently delivering primary eye care via telehealth, and commonly included videoconferencing.
Conclusion:
The application of teleoptometry to deliver eye care is rapidly emerging, and appears to be a viable adjunct to the delivery of in-person optometry services. The review highlighted the scarcity of evidence surrounding the clinical benefits, safety, and outcomes of teleoptometry. Further research is required in this area.
Introduction
In March 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) a pandemic. As a result, the capacity of health systems to continue to deliver optometry services in an office-based face-to-face experience has been restricted to ensure the safety of both the patient and the provider. In response to the need to maintain essential optometry services throughout the COVID-19 pandemic, there has been a dramatic rise in the utilization of telehealth services, and the profession has moved rapidly toward the adoption and delivery of teleoptometry. The increase in the uptake of telehealth to deliver optometry care during COVID-19 has caused the optometry profession to reimagine the role of telehealth.
Telehealth is a promising and well-received approach to connect practitioners and patients to deliver health care to individuals where access and resources may be limited. 1 The utilization of telehealth is becoming increasingly widespread in health care, with the many applications extending to numerous medical specialties. A recent systematic review highlighted the effectiveness of telemedicine in specialties, including telepsychiatry, teleradiology, and telecardiology. The review demonstrated the efficacy of consultations between primary and secondary level health care providers 2 and described the criticisms of the limited and inconsistent evidence surrounding efficacy and cost-effectiveness in telemedicine. 2,3
Other investigations that relate to the cost-effectiveness of telemedicine compared to conventional health care delivery has been found to be inconclusive at this time. 1,4,5 While there is evidence that showed telemedicine to be cost-effective when delivered in rural and remote areas, 6 conclusions shared in the systematic review by Ekeland et al. 2 called for more extensive studies to address the limited and inconsistent results regarding impact and cost in the literature.
The terms telehealth and telemedicine are at times used interchangeably. However, in an evaluation of peer-reviewed definitions of these terms, Sood et al. 7 demonstrated that these terms are not synonymous, and telemedicine is a subset of telehealth. Telemedicine is limited in scope to the delivery of the clinical service aspects of health care, whereas telehealth is more expansive and covers the preventive, promotive, and curative aspects of health care. 8 For the purposes of this review, the term “telehealth” will be used when referring to telehealth or telemedicine.
There are two primary forms of telehealth: synchronous and asynchronous telehealth. Synchronous telehealth refers to the delivery of consultations in real-time. 9 For example, video consultations commonly included prescribing medications, reassurance, or escalating the need for an in-person appointment. 10 In contrast, asynchronous telehealth involves transmitting health information in a store-and-forward approach that does not require real-time communication, 11 and applications include screening for diabetic retinopathy and retinopathy of prematurity. 12
The telehealth model has been applied across many health domains. Teleophthalmology is a well-researched discipline in telemedicine that is highly regarded by practitioners 13 and patients. 14 –16 Teleophthalmology is an evidence-based intervention where ophthalmologists deliver specialty care in hospital and outpatient settings to unserved or underserved populations. 14
Teleophthalmology is often dependent on optometrists and other skilled health workers to capture and transmit patient information. Applications of teleophthalmology are feasible for triage, screening, consultation, and remote supervision. 17 Screening for diabetic retinopathy is one such service commonly delivered by teleophthalmology, and in the United States, teleophthalmology screening services for diabetic retinopathy include optometrists. 18 Numerous systematic reviews support the use of teleophthalmology, 19 citing teleophthalmology to be cost-efficient, reliable, and valid. 20 Teleoptometry care models delivered during the COVID-19 pandemic include urgent care for acute eye health concerns, deterioration of chronic eye conditions, and other consultations, including contact lens follow-up.
In recent years, there has been increasing reports of optometry services being provided via telehealth. Teleoptometry can be defined as the application of optometrist-provided care via telehealth. The increasing utilization of teleoptometry is partly due to the emergence of novel and innovative approaches to eye care delivery supported by high-speed internet and continual software and equipment innovation in the eye care sector.
During the initial phases of the lockdown, only 5.54% of optometric services were delivered in optometry practices in Pakistan compared to prelockdown. 21 The impact of the COVID-19 pandemic disproportionately affected vulnerable populations such as those living in remote areas, elderly people, socially disadvantaged people, children, and people living with disabilities to access optometric care. The inability for these at-risk patients to present in-person contributed to an increase in inequity in accessing eye care services. Telehealth can increase access to health care to vulnerable groups by reducing barriers, including reduced travel time and cost. 22,23 The COVID-19 pandemic has further highlighted the need to create innovative approaches to provide primary eye care to vulnerable populations who experience barriers to access eye care. 24,25
RATIONALE
A number of studies detail the application of teleophthalmology programs in underserved areas and populations. 26 –28 However, despite growing interest in adopting teleoptometry during the pandemic, there is a paucity of published literature regarding the role of optometry in telehealth. Further, there is a lack of policies and protocols to guide the delivery of optometry services via telehealth platforms. The U.S. Department of Veterans Affairs (VA) is leading the expansion of optometry-facilitated telehealth services with the introduction of protocols and services, including low-vision rehabilitation, teleretinal screening services in primary care clinics, and Technology-based Eye Care Services (TECS). Globally, there is an urgent need to collate current evidence on the use of optometric care delivered by telehealth.
OBJECTIVES
The purpose of this report is to conduct a literature review to seek all of the peer-reviewed evidence surrounding the application of optometry services when delivered via telehealth models.
Methods
This review includes only peer-reviewed publications that were in English. Publications that were limited to a review of the literature were excluded. All peer-reviewed publications that included optometrists in the telehealth service were included in this review. Due to the scoping nature of the literature review, abstract presentations were included in the eligibility criteria.
SEARCH STRATEGY
A comprehensive database search was undertaken using MEDLINE, Global Health and Web of Science in October 2020. Reference lists were hand-searched for other relevant articles by the primary author. MEDLINE was searched using the following search string: “teleoptometry” OR “tele-optometry” OR “telemedicine” OR “telehealth” OR “teleophthalmology” OR “ehealth” OR “telecare” Or “video consultation” OR “electronic consultation” OR “e consultation” OR “virtual consultation” OR “remote consultation” OR “videoconferencing” OR “mhealth” AND “optom*”. Relevant MeSH terms were included in the search strategy. Analogous search terms were used for Global Health and Web of Science. No limits on study design or intervention were imposed. No restrictions were applied to publication date or location.
INCLUDED STUDIES
In total, 206 abstracts were identified via database searching. Nine additional studies were included that were identified through other sources. Following the removal of duplicates, 212 references were screened. Fifty-one full-text articles and four articles limited to abstracts only were accessed and included by the first author. Of the remaining articles, 27 met the inclusion criteria for analysis (Fig. 1).
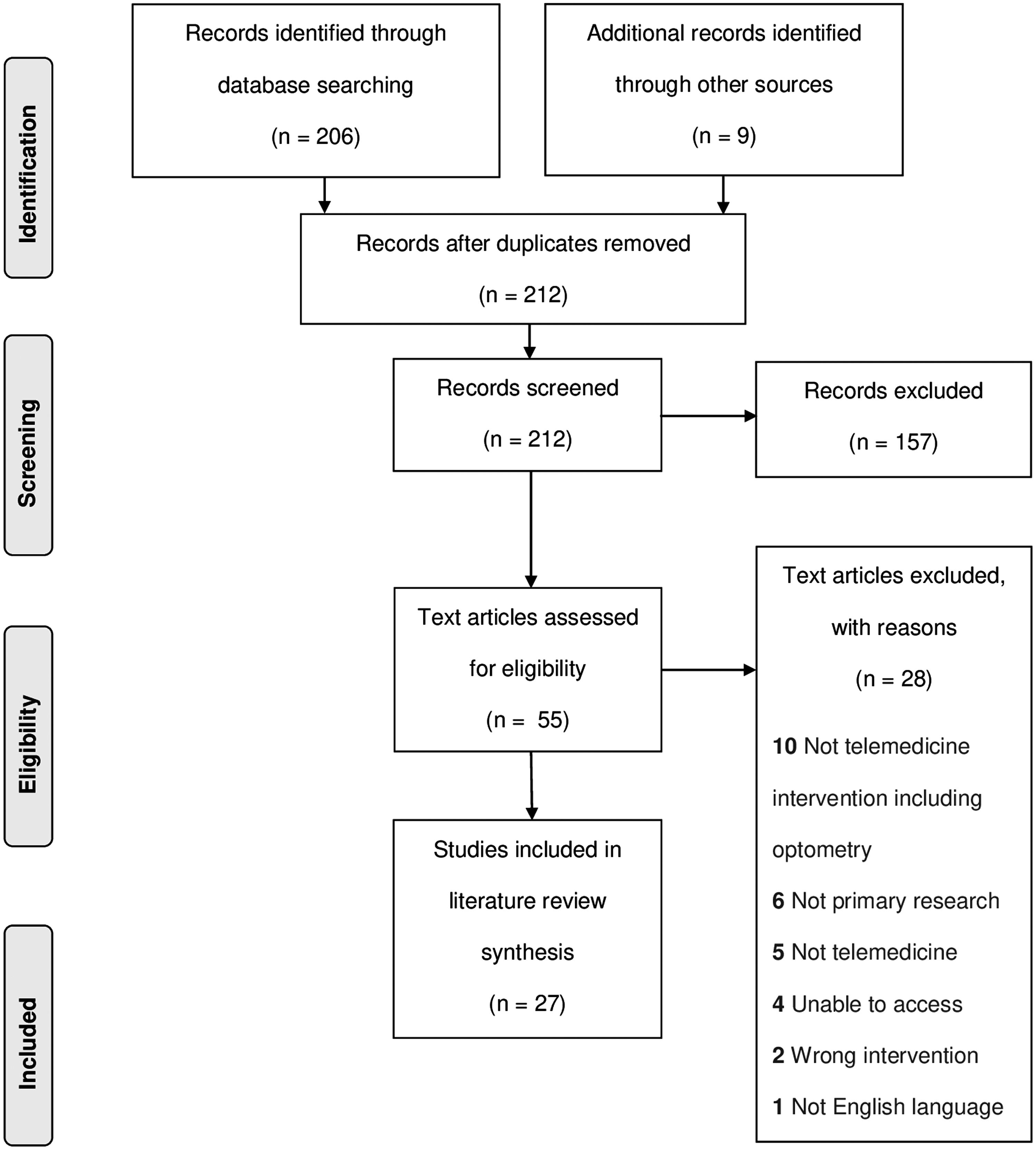
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram outlining the systematic literature review process.
DATA EXTRACTION AND SYNTHESIS
Following the review of full-text and abstract articles, a framework for data extraction and synthesis was developed, and the first author, (J.M.) independently extracted relevant data into Microsoft Excel. The framework listed the variables to be extracted from each article and included year, study design, country, study focus, mode of telehealth, population, collaboration type, and study summary.
Results
In total, 27 articles met the inclusion criteria for the review. The first published study in optometry-facilitated teleoptometry emerged in 1999, where Smythe 29 reported on a study exploring teleoptometry to facilitate contact lens fittings via asynchronous video. Since 1999, there has been a surge in studies examining optometry-facilitated telehealth in recent years, with most publications emerging between 2015 and 2021 (n = 20). Table 1 provides a summary of the 27 publications relating the optometric care in telehealth.
Overview of Included Studies
COVID-19, coronavirus disease 2019.
Publication dates of all studies included in this review ranged between 1999 and 2020. The location of the studies reviewed include seven studies conducted in Australia, 16,30 –35 seven in the United States, 29,36 –41 three in Canada, 42 –44 two in India, 45,46 two in The Netherlands, 47,48 three in the United Kingdom, 49 –51 one study was conducted in an undisclosed location, 52 and single studies were conducted in Ethiopia 53 and Spain. 54
STUDY CHARACTERISTICS
Prospective study designs represent the largest number of included studies, including four cohort studies 36,48,53,54 and four prospective audits. 31,33,34,49 Other frequently utilized study designs included retrospective audits (n = 4), 30,32,35,41 interobserver reliability studies (n = 2), 29,37 questionnaires (n = 3), 16,46,52 and mixed methods studies (n = 2). 47,51 Less frequently utilized study designs included retrospective cohorts (n = 2), 44,50 retrospective case series (n = 2), 43,45 one clinical protocol, 39 a prospective case series, 42 a clinical protocol for a pilot study, 40 and a cross-sectional pre–post study 38 (Table 1).
Of the 27 studies reporting the involvement of an optometrist to deliver telehealth, only 11 studies included the role of optometrists as a member of the telehealth team providing eye care services. 29,36 –42,44,46,52 That is, the optometrist had a role in the care of the patient beyond providing and receiving telehealth referrals, being present for the teleconsultation, collecting clinical data required for asynchronous teleophthalmology consultations, and providing the patient with continuing care following telehealth consultation with an ophthalmologist.
MODE OF TELEHEALTH USED TO DELIVER EYE CARE SERVICES
Table 1 outlines the inclusion of optometry in the delivery of eye care services via different models of telehealth. Of the 27 studies that included optometrists in the telehealth model of care, 12 studies utilized asynchronous telehealth, 29,35,36,38,43,44,47 –50,53,54 where the optometrist collected clinical data from the patient in an in-person consultation that usually accompanied a referral to a teleophthalmology service. Eleven studies used synchronous telehealth, 16,30,33,34,37,39 –42,51,52 where optometrists used video consultations to deliver primary care, including low-vision rehabilitation, consulted with general and subspecialty ophthalmologists to improve the efficiency of the referral process, and delivered comprehensive eye examinations with the assistance of an in-person technician.
The remaining four studies utilized both synchronous and asynchronous methods of delivering eye care via telehealth. 31,32,45,46 The role of optometrists in these hybrid telehealth services involved optometrists consulting with the patients to collect the clinical data required for the ophthalmologist to asynchronously review, followed by the optometrist supporting the video consultation between the patient and the ophthalmologist.
TELEHEALTH COLLABORATION TYPE
The most common form of collaboration involving optometrists is the delivery of eye care via teleophthalmology. In 19 studies, the optometrist facilitates the referral, communication, and management plans between the patient and the teleophthalmology service. 16,30 –36,38,43 –45,47 –51,53, 54 In this collaboration type, optometrists are often consulting in-person with the patient.
Eight studies described the independent application of teleoptometry between the patient and the optometrist. 29,37,39 –42,46,52 The scope of practice of independent teleoptometry included optometrists delivering comprehensive eye examinations assisted by a technician, 52 performing subjective refractions via a digital platform that included videoconferencing, 37 seeking advice from other optometry colleagues via teleoptometry, 29 supporting low-vision rehabilitation via teleconference (often supported by a technician who is present with the patient), 39 –42 and providing primary eye care during the COVID-19 pandemic. 46
The format and geographical areas where eye care via telehealth is being delivered
Single reports of other forms of collaborations were observed, including technicians working between the optometrist and ophthalmologist, 47 where the optometrist collected retinal photos to send to the ophthalmology clinic for interpretation by the hospital technician. In this study, the scope of practice of optometrists was limited to refraction care.
Optometry-facilitated telehealth was most frequently observed in general teleophthalmology services, and accounted for nine of the included studies. 16,30 –35,47,50 Optometrists have a role in other teleophthalmology subspecialties, including anterior and orbital disease, 45 and triaging for medical retina. 43,51,54 The role of optometrists in glaucoma management via telehealth was explored in six studies. 36,38,44,48,49,53 The scope of practice of optometrists reported in these publications included organizing referrals to teleophthalmology services, and facilitating videoconference calls between patients and specialists.
The role of optometrists in these comanagement arrangements also included initiating management plans made by ophthalmologists, booking patients for surgery during the consultation, and in asynchronous telehealth services, the optometrist communicated the ophthalmology findings to the patient.
Two studies reported on the level of agreement between optometrist clinical findings as rated by an ophthalmologist or optometrist. 29,37 Furthermore, telerehabilitation emerged as an area where optometrists can deliver teleoptometry to patients who have low vision (usually supported by technicians who are with the patient in-person), 39 –42 or as part of a collaboration with other optometrists and ophthalmologists. 39 Teleoptometry was utilized by optometrists to remotely conduct comprehensive eye examinations using a platform supported by technicians present with the patients. 52
Teleoptometry was reportedly utilized during the COVID-19 pandemic to support the delivery of primary eye care, 46 however, the details of how teleoptometry was conducted were not reported.
Thirteen of the included studies exclusively examined optometry-facilitated telehealth in rural settings. 16,30 –34,36,39 –42,45,53 In these rural settings, synchronous telehealth was most commonly utilized (n = 8), as opposed to asynchronous (n = 2) or mixed-format telehealth (n = 3).
Discussion
This review highlights the unique and important role optometrists have in meeting the eye care needs of populations at different levels of the health care system. A strength of this study is that it is the first review to synthesize what is known about how telehealth is being utilized to provide optometric care in the form of teleoptometry. The studies exploring optometry-facilitated telehealth varied by country, population, and mode of telehealth. The common utilization of comanagement arrangements between optometrists and ophthalmologists emerged as an area with great potential that is already highly utilized. In delivering optometric care via telehealth independent of ophthalmology, teleoptometry emerged as an area where contact lens consultations can be conducted, 29 subjective refractions may be performed, 37 and low-vision services can be delivered to patients. 39 –42
Of the 215 studies identified in the search, only 27 studies were deemed relevant to the research question. This review highlights a paucity of published research in teleoptometry, and more broadly, research supporting optometry's role in telehealth. Although the delivery of optometry has drastically changed during the COVID-19 pandemic to improve patient access to eye care 46 ; only 11 studies published in the area of telehealth expanded the role of optometrists in the telehealth service beyond sending referrals, collecting data required for asynchronous teleophthalmology, and supporting the telehealth consultation between the ophthalmologist and the patient. 29,36 –42,44,46,52
The role of optometrists in the remaining 16 publications is as an indirect facilitator in the delivery of telehealth, 16,30 –35,43,45,47 –51,53,54 primarily referring patients into a teleopthalmology service. 16,30 –35,43,50,51,53 Other indirect roles of optometrists in telehealth services include the following: collecting clinical data required for the teleophthalmology consultation 16,30,31,35,43,45,47 –50,54 ; providing support to the patient during the video consultation 16,30 –34,45,51 ; suggest a management plan to accompany the referral 35,49 ; and initiate the management plan recommended by the ophthalmologist if the patient is referred back to the care of the optometrist. 35,43,45,47,48
ACCEPTABILITY OF OPTOMETRY-FACILITATED TELEHEALTH
The published literature exploring practitioner and patient acceptability of teleoptometry is limited; however, the literature that does exist in the area reports high levels of satisfaction. Two studies examining synchronous teleophthalmology services in rural Western Australia report an overall acceptance of teleoptometry by patients. In addition, patients in rural locations highly value the role of optometrists when attending teleophthalmology consultations. 16,31 Furthermore, Patel et al. 52 report that most patients were highly satisfied with the quality of care they received when attending a comprehensive teleoptometric eye examination.
Interestingly, one study identified older patients as having a greater acceptance of optometric care delivered via telehealth. 32 Research by Verma et al. 44 also highlights increased management continuity and patient engagement via the role of collaboration with optometrists to deliver teleophthalmology services.
In the area of telerehabilitation, Bittner et al. 42 found that all patients were satisfied and comfortable receiving low-vision evaluation and rehabilitation via teleoptometry. Patients who received low-vision services via teleoptometry perceived the accuracy of the evaluation as equal to an in-person consultation. Providing low-vision services via teleoptometry allowed additional follow-up consultations that would not usually occur at in-person services. Similarly, Ihrig 41 states veterans who attended the low-vision telerehabilitation service report being highly satisfied with the care they received. Vision aids significantly improve quality of life 55 ; the area of telehrehabilitation is an area with great potential to assist patients who cannot access low-vision rehabilitation at in-person services.
THE ROLE OF COLLABORATIVE PARTNERSHIPS
The literature highlights the significance of the collaboration between optometrists and ophthalmologists in the delivery of teleophthalmology. Despite the lack of financial reimbursement, optometrists have the greatest utilization of telehealth consultations with ophthalmologists of any of health care provider. 31 At present, only a single study explores the positive impact of introducing financial incentives for optometrists to deliver telehealth services. 34 Furthermore, Karthikeyan et al. 46 reported that in India, 50.94% of optometrists offered teleoptometry services at the beginning of the COVID-19 pandemic; however, 85.19% of those optometrists did not charge for the service.
Studies report increased efficiency and access to ophthalmology surgical care when optometrists facilitate teleophthalmology services between the patient and the ophthalmologist. 30,31,36,43,54 Improved referral refinement 50 and triaging of specialist referrals has also been demonstrated to reduce unnecessary in-person consultations, 43 thereby reducing the workload of tertiary services, 47 and increase case detection. 53
Keenan et al. 49 highlights how the skills of optometrists can be effectively and safely utilised in colloborations with ophthalmologists to evaluate glaucoma referrals at the community level via telehealth in the form of comanagement arrangements. Comanagement plans were determined by the ophthalmologists and implemented by the optometrist. 38 This application of task sharing increases the capacity of tertiary ophthalmology services. However, Verma et al. 44 reported limitations in comanagement arrangements where there was a lack of infrastructure with respect to data collection needed to understand optometrist adherence to management plans outlined by the ophthalmologist.
The application of teleoptometry in primary eye care reduces some of the logistical barriers vulnerable patients face. 39,54 Utilizing optometrists to virtually comanage glaucoma 45 reduces the need for some patients to attend in-person consultations with ophthalmologists 44 and reduces the indirect costs of care. In contexts where optometrists have a limited scope of practice, optometrists are involved in telehealth comanaged screening. 48 In addition, utilizing optometry-facilitated telehealth to prebook in-person ophthalmology procedures via telehealth reduces the number of practice visits and increases the efficiency of in-person consultations. 43 This is further highlighted by Turner et al. 34 who reported that 44% of patients who attended an optometrist-facilitated telehealth consultation were directly booked for surgery.
Optometrists who provide teleoptometry services and are involved in comanagement arrangements benefit from the learning opportunities that arise from continuous feedback given by ophthalmologists; these collaborative arrangements foster upskilling. 48,53 In addition, optometrists in rural locations who are involved in teleophthalmology delivery directly benefit by having greater access to teleophthalmology services available when seeking timely specialist consultation. 31
A study examining interobserver agreement is favorable. A meeting abstract published by Randhawa et al. 37 examining telehealth-delivered subjective refraction found no statistically significant difference between in-person and telehealth-delivered subjective refraction.
A single study has been published on the cost-effectiveness of optometry-facilitated telehealth services; Ihrig 41 demonstrated the delivery of low-vision telerehabilitation significantly reduced the cost to the individual and increased access to the low-vision service compared to in-person services.
LIMITATIONS
The literature review has several limitations. This review represents peer-reviewed literature published in English only. Another flaw in the review is the fact that many of the studies included assessed the role of optometry in telehealth as a secondary research outcome. Furthermore, the dates of publication vary widely and extend back to 1999. Technological innovation in telehealth has rapidly evolved over the past two decades, and therefore the results from the studies should be considered in the context of publication date.
The scope of practice in optometry varies between countries. At present, comanagement between ophthalmology and optometry is commonplace in many countries. As a result, the studies included presented recommendations about the role of optometry in telehealth that varied depending on the location and may not reflect what is available globally. This variability reflects a paucity of studies in the area of teleoptometry and the need for further research.
Conclusion
The role of optometrists in telehealth is rapidly emerging, and the field has great potential. Teleoptometry appears to be a viable adjunct to the delivery of eye care, or where necessary, an alternative to in-person optometric services. The literature highlights the multiple applications of optometry-facilitated telehealth, including care delivered as part of a collaboration with ophthalmology, or independently through telerehabilitation and teleoptometry.
The suitability of teleoptometry as an adjunct to face-to-face optometric care using telehealth is feasible. The literature demonstrates teleoptometry to be highly acceptable to patients and practitioners. The role of optometrists in providing eye care services via telehealth has value for many individuals, including the elderly, people living with a disability, and people living in rural locations. However, there is a scarcity of evidence regarding clinical benefits, safety, and outcomes of optometry-facilitated teleoptometry. More significant research is required to determine safe and effective models of integrating optometry into the delivery of telehealth services.
Furthermore, there is only a small number of peer-reviewed policies and protocols published at present to guide the delivery of optometry services via telehealth platforms. This review of the current evidence base in optometry services delivered via telehealth will guide future research and policy creation. The continued creation of focused, inclusive teleoptometry strategies and policies will support achieving equitable access to optometry services. Further, additional advocacy surrounding increased research that supports policy development and appropriate reimbursement for optometric services is needed to address financial barriers to uptake. Policymakers should heed caution in recommending ongoing and increased use of teleoptometry applications pending further research.
This review demonstrates the severe paucity of evidence-based research in teleoptometry. Providers of teleoptometry should be mindful that none of the studies included an economic analysis of optometric telehealth. No studies included a safety analysis, highlighting the urgent need for research in the area. As the field of teleoptometry is in its infancy, outside of the area of low-vision telerehabilitation, there is limited peer-reviewed evidence to support optometry services delivered via telehealth as a safe, acceptable and cost-effective means to provide health care. Findings of the review did not constitute evidence of the safety of optometric care via telehealth, unless under the supervision of an ophthalmologist where a comanagement plan is in place.
Footnotes
Authors' Contributions
Conceptualization: J.M., P.M., and S.S.B.; writing—original draft preparation: J.M.; writing—review and editing: J.M., P.M., and S.S.B. All authors have agreed to the published version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This review has been funded by the World Council of Optometry.