
Abstract
Introduction
In China, various laparoscopic workshops are important methods for continuing medical education (CME) related to laparoscopic training. It is an effective tool for continuing professional development. 1 Typical laparoscopic workshops in China often include lectures delivered by specialists and real-time demonstration of various laparoscopic procedures. 2 Live demonstrations also have a high educational value and contribute significantly to laparoscopic surgery because they are ideal for education and practical teaching of laparoscopic surgery, a technique based primarily on visual cues through the endoscope. 3,4 However, skilled clinicians face fatigue when traveling for real-time demonstrations at away institution. 5,6 On the other hand, live demonstration via the Internet makes it feasible for specialists from different countries to conduct real-time demonstrations remotely, 3,7 –9 thus eliminating the time and expense of travel. Because of bandwidth limitation, the traditional videoconference system based on the code/decode technique has disadvantages of dropped video frames or distortion of images. 9,10 A new videoconference system based on a digital video transport system (DVTS) has been set up between Shanghai and Japan since 2005. 10,11 Here we explored the feasibility and effectiveness of international videoconferences based on DVTS for CME programs related to laparoscopic surgery.
Materials and Methods
Endorsed by the Chinese Medical Association Council on Medical Education, we conducted four CME seminars from 2007 to 2010. The state-level CME Category 1 Credit certificate was awarded to the trainees finishing the course. The seminar's topics were focused on progress in minimally invasive surgery for digestive system malignancies. The course lasted for 30 h, including a specialist's seminar and the live case demonstration. International laparoscopic specialists were invited to deliver a lecture or perform a laparoscopic surgery demonstration via the superfast broadband Internet (Table 1). The detailed information for network and system configuration was described in our previous article. 10 The high-speed broadband Internet connection was provided by the China Education and Research Network and a nonprofit international consortium known as the Asia-Pacific Advanced Network, free of charge. To protect the patient's privacy, a virtual private network technique was applied to the multistation connection to keep the data transmitted safely from point-to-point. Because English is the official language for international videoconferences, simultaneous English–Chinese interpretation service was provided to attendees in need.
Basic Contents for International Videoconferences
LADG, laparoscopic-assisted distal gastrectomy.
Network Stability Evaluation
Stopwatch software was installed on a personal computer at the originating station. The stopwatch image was sent to the remote station and returned to the originating station via a DV camera and the network. The same time point stopwatch image was shown in each station. The time delay was determined by dividing the time difference between the originating station and the remote station in half (Fig. 1). Packet loss was monitored by DVTS software.
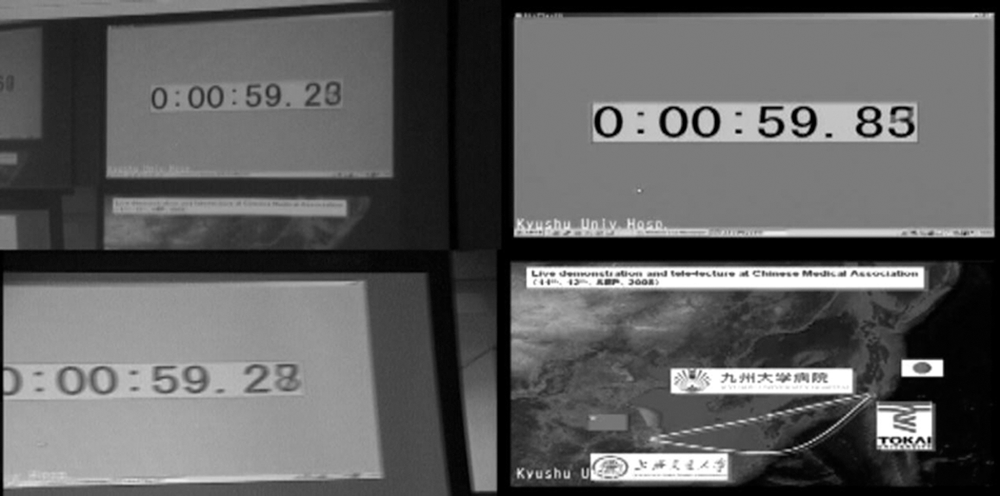
Stopwatch software was installed in the computer in Kyushu University, Japan. The stopwatch was shown on the screen in Kyushu
Attendees' Satisfaction Evaluation
An anonymous mini-questionnaire was conducted after each section to evaluate the satisfaction of attendees regarding the image and sound quality, content selection, and overall evaluation. It consisted of five multiple-choice questions as follows:
Question 1
What do you think about the quality of the image during the videoconference? The answer key was: 1, excellent; 2, good; 3, average; 4, poor; or 5, very poor.
Question 2
What do you think about the quality of voice during the videoconference? The answer key was: 1, excellent; 2, good; 3, average; 4, poor; or 5, very poor.
Question 3
How do you rank the selected contents of the videoconference? The answer key was: 1, excellent; 2, good; 3, average; 4, poor; or 5, very poor.
Question 4
What is your overall evaluation for the videoconference? The answer key was: 1, excellent; 2, good; 3, average; 4, poor; or 5, very poor.
Question 5
What kind of laparoscopic surgery do you wish to see next time? The (multiple choice) answer key was: 1, liver; 2, colon; 3, stomach; 4, pancreas; or 5, other (fill in the blank).
Results
Nine videoconferences were conducted during the past four successful CME workshops. Of these, four were telelectures, and five were live operation demonstrations. The topics covered were laparoscopic gastrectomy, pancreatectomy, and colectomy (Table 1).
Stability of the network was maintained throughout each videoconference. High-quality videos of 720×480 pixels at the rate of 30 frames per second were shown to the entire group of attendees. The attendees could hear clear and comprehensible voices synchronously transmitted with the image (Fig. 2). Actually every participant enjoyed the interactive international videoconference. The time delay between Shanghai and Fukuoka, Japan, was only 0.3 s, and the packet loss was 0% (Fig. 1).

The upper right part of the large screen shows the live laparoscopic-assisted distal gastrectomy performed at Kyushu University Hospital, Japan; the upper left part shows the Shanghai venue. The first author (in the center) works as the moderator and has just provided simultaneous Chinese–English interpretation to all the attendees in Shanghai. The bottom left part of the screen shows Tokai University Hospital, whereas the bottom right part is the still image being sent from Kyushu University, showing the geographic position of each station.
We obtained 129 valid responses from the questionnaire from a total of 146 attendees. The majority of the attendees were satisfied with the quality of transmitted images and voices. Furthermore, most attendees ranked the selected contents and the overall evaluation as excellent or good (Table 2). When attendees were asked what kind of laparoscopic surgery should be demonstrated for the next videoconference, pancreas and liver were the favorite selections, receiving 62 and 61 votes, respectively (Table 2).
Results of the Anonymous Mini-questionnaire After Videoconferences
Examples include spleen, hernia, and bariatric surgery.
Discussion
Laparoscopic surgery education in China was initiated in 1991. 2 In addition to the traditional teaching of minimally invasive surgery skills in the operating room, communication via conferences and workshops is increasingly used as a teaching method in laparoscopic surgery education. 2,4,5 Our hospital initiated laparoscopic surgeries since the early 1990s. As one of the leading institutions in laparoscopic surgery in China, our Department started to host national CME workshops for laparoscopic surgery beginning in 2004. Similar to most of the laparoscopic training workshops in China, these included face-to-face lectures and live demonstrations. The surgical images were transmitted from the operating room to the conference room via a direct cable connection in our hospital. Leading experts both domestic and from abroad were frequently invited to demonstrate cutting-edge laparoscopic techniques. In 2005, super-high-speed optical fiber was extended from the main campus of Jiao Tong University to our hospital, which enabled us to begin collaboration with Dr. Shuji Shimizu from Kyushu University in Japan. 10,11 An up-to-date videoconference system was subsequently introduced to our CME workshop.
Even though the effectiveness of live surgical demonstration at conferences is still controversial, 12 live demonstrations of laparoscopic surgery are of high educational value and provide a great opportunity for trainees to learn and master the skills of laparoscopic surgery, which has a steep learning curve. Advantages of live demonstrations of laparoscopic surgery include the capacity to educate larger groups, peer review by expert moderators, rigorous cross examination, and an exchange of ideas. 4,6,13 Furthermore, broadcasting to large audiences is more efficient and does not physically interfere with the flow of the operating room or cause distraction of the clinical staff. 7,14 But, we also encountered difficulties in our previous experience similar to those described by Toouli. 12 As the organizer, sometimes we could not provide enough time for the invited expert to conduct a full assessment of the patient's case. The invited faculty faced fatigue after a long trip and sometimes complained about our surgical instruments, despite our effort to provide the best available instruments in our hospital. Sometimes the expert was not familiar with the instruments provided. With live surgery demonstrated through telemedicine, the difficulties of such a situation can be avoided because the expert will not be fatigued by a long travel, and it is important that the surgery will be performed in the home institution in a familiar operating room setting. 6,15
Videoconferencing, like telementoring, is a common clinical tool for surgeons and provides a great opportunity to alter surgical practice and to offer patients the best expertise in surgical treatment despite long distances. 16 The live surgical demonstration through telemedicine has also been used at conferences for many years; it has been regarded as a useful tool for teaching and training. 7 –11,14 The satisfaction of attendees has been increasingly focused on recently. 10,11,13 The results of the questionnaire in this research show that the majority of the attendees ranked the image or sound as good or excellent (97.67% and 87.6%, respectively). Of the attendees, 95.35% were satisfied with our content selection. In fact, the live case demonstration and lecture via DVTS gave the audience “an unanticipated surprise” because of the crispness of the moving picture and positive interactive discussions. The Chinese surgeons showed great interest in live surgery demonstration through teleconferencing. When attendees were asked about the kind of laparoscopic operation that they would like to see next time, pancreas and liver were ranked as top choices.
The telemedicine system has developed in sync with equipment and network conditions. 17 Its limitation is still evident, in particular because of the time zone difference; sometime it is difficult to host a simultaneous daytime live demonstration between host and receiving venues. Furthermore, the equipment for telemedicine and the network should be updated to follow the trend of popularity of high-definition laparoscopic equipment in the near future. 17
In conclusion, international videoconferences are great learning channels for CME programs associated with laparoscopic surgical training.
Footnotes
Acknowledgments
The authors express sincere gratitude to Dr. Shuji Shimizu and colleagues from Kyushu University Hospital for sharing their cutting-edge laparoscopic experiences, especially laparoscopic-assisted distal gastrectomy. We also appreciate editing by Hongyan Zou, MD, PhD, from Mount Sinai School of Medicine in New York, NY.
Disclosure Statement
No competing financial interests exist.