
Abstract
Introduction
Health information exchange (HIE), defined as the electronic transmission of healthcare information among organizations, 1 is expected to improve quality of care, reduce medical error, and lower healthcare costs, 2 –9 and HIE systems have become more prevalent worldwide as many countries have recognized the potential of the technology. 3,6,10,11 The need for efficient and effective ways to exchange clinical information among providers is particularly great in South Korea, where physician care at clinics is discontinued when a patient moves to a hospital or other clinic for further management. In South Korea, hospitals employ their own medical staff, and practicing physicians in community clinics do not have the privilege of seeing patients in a hospital. Although users of an uncoordinated healthcare delivery system would likely benefit from an HIE, previous studies suggested considerable challenges with respect to technical limitations, financial and organizational constraints, implementation issues, and physicians' and patients' acceptance of the new technology for a successful implementation of an HIE. 2,7,12 –19 In their study of the use of electronic health records and HIEs in seven nations, Jha et al. 11 concluded that a significant amount of financial investment, diligence in the difficult work of building standards and interchanges, and concerted efforts in aligning financial incentives and redesigning administrative work processes are needed before a nation attains any benefits from an HIE.
The challenges are particularly great in South Korea as hospitals and clinics compete with each other for outpatients as well as for inpatients requiring simple medical or surgical services. More than 80% of physicians in South Korea are board-certified specialists, and approximately one-half of them practice in a community clinic where the scope of care is broadening with the advancement of medical technology. Furthermore, hospitals have a large share of their revenue coming from outpatient care. The care offered in hospital outpatient and inpatient services overlaps with that offered by individual physician practices in the community, and conflicts and competition often characterize the relationship between hospitals and clinics. Physicians in both settings are unaccustomed to allowing other physicians to see records of the treatment they gave a patient. Further complicating HIE implementation is that hospitals and clinics are paid through the National Health Insurance program by a fee-for-service mechanism such that payments are proportional to medical service provision. Despite wide adoption of health information technology, including electronic medical records (EMRs) and computerized provider-order entries, an HIE has not been implemented in South Korea. Studies that shed light on barriers of HIE adoption and utilization of exchanged clinical information in the delivery of care are in demand so that an HIE adoption strategy can be formulated and the potential benefits of the technology can be realized. As technological limitations and financial barriers are overcome through the efforts such as those of the Health Information Technology Standards Panel of the United States, ensuring major stakeholders' acceptance of an HIE has become the most important factor for its successful implementation. 12,14 Through investigations of physicians' perceptions and attitudes toward the technology, other studies have examined the potential costs and benefits of an HIE as well as motivators and barriers of HIE adoption in recent years. 20 –25 However, few researchers have investigated the way physicians use exchanged clinical information in their clinical decision-making.
In this study, we investigated physicians' perceptions of an information exchange and their usage of exchanged information based on data obtained through an HIE pilot program in South Korea. We also investigated the influence of the practice settings (tertiary-care hospital and community clinics) on their perceptions and usage to see whether the system design and implementation strategy should be differentiated for different practice settings. The study protocols were approved by the Institutional Review Board of the Seoul National University Bundang Hospital (SNUBH).
Materials and Methods
Settings
A 3-year HIE pilot project funded by the government was launched in November 2007 to facilitate its efforts to introduce HIE systems in South Korea. 26 The SNUBH, a medical school–affiliated tertiary-care facility, and 35 clinics (or physician practices) with referral arrangements with the SNUBH participated in the pilot program. All facilities had been using EMRs at the time of the project launch. The HIE system is based on a federated architecture model (Fig. 1). We applied the ebXML RS and ebXML RIM standards to the HIE system to ensure the semantic interoperability for exchanged clinical document architecture documents, the HL7 V2.x standard for notification messages, and the DICOM standard for images. The first version of the HIE system was rolled out in June 2008, and updates were completed in October 2009. Information exchanged in the final system includes patients' demographic data and information on diagnoses with chief complaints, medications, lab results, diagnostic images, duration of treatment, contents of treatment and care plans, vital signs, patient history, and summaries. The system requires patients' consent prior to physician participation in the HIE. Approximately 2,500 cases referred to the hospital from the clinics have been accommodated by the system annually since its rollout.
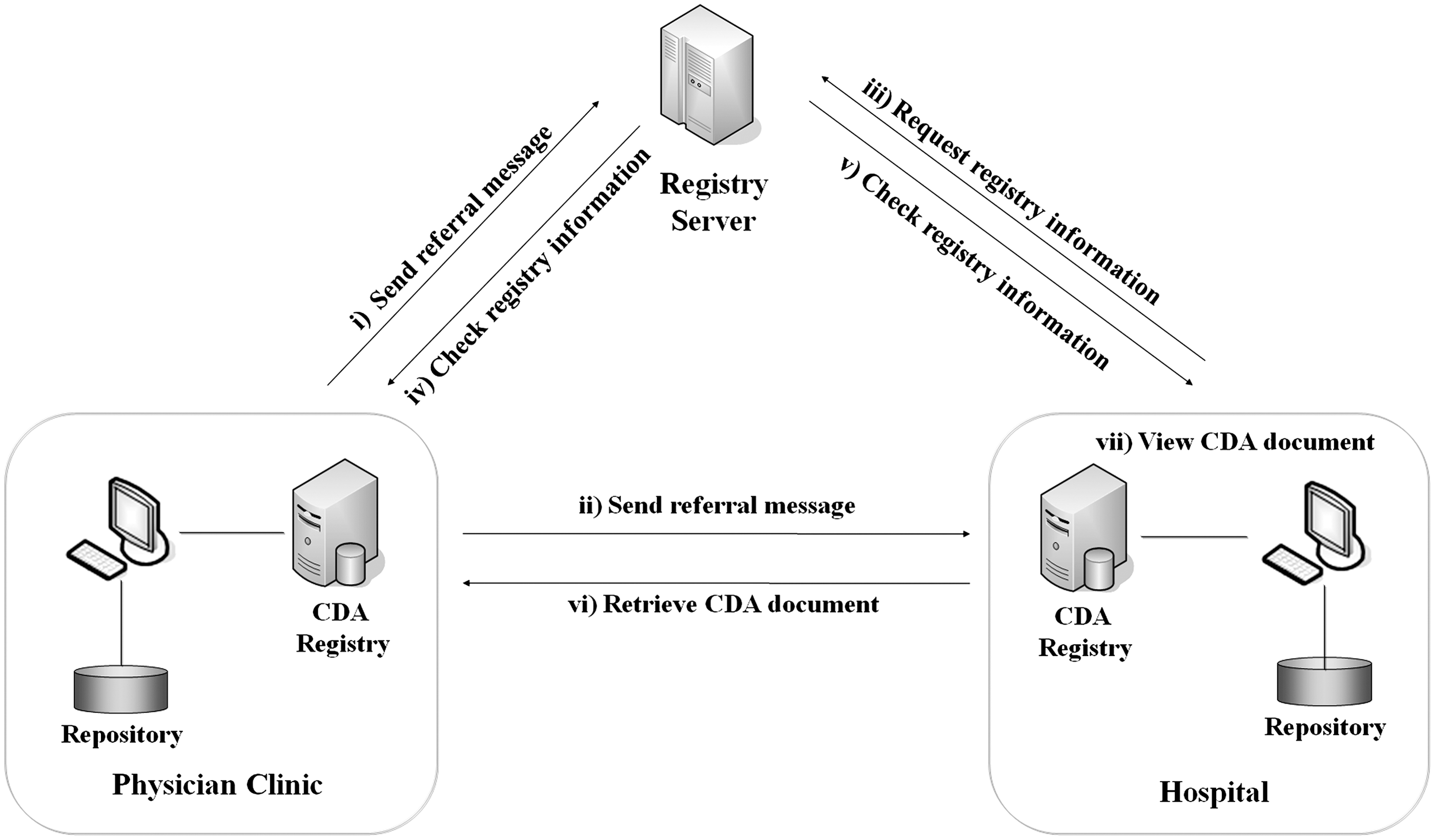
Overview of the health information exchange system architecture. CDA, clinical document architecture.
Pre-Implementation Survey
We constructed a survey instrument to collect data on physician perceptions about an HIE. The questionnaire consisted of four sections. Section 1 provided respondents with brief descriptions of the HIE technology. Section 2 obtained information about respondents' assessment of the need for the overall HIE system and specific HIE items. Section 3 obtained information about respondents' expectations about benefits and concerns regarding the HIE. Section 4 solicited information concerning respondents' practice and demographic characteristics. To develop survey questions for benefits and concerns, we first reviewed literature on the effects of an HIE and frameworks for quality evaluations of services in general, healthcare services, and information technology services. 22,27 –29 The finalized list of benefit domains were quality, time, cost, safety, and managerial aspects of providers. The concerns domain included information safety and security, system reliability, and managerial aspects of providers. Then, through team discussions, we defined survey questions that matched the selected domains. We completed the instrument through an iterative process of review, revision, and pre-test. Three physicians in each practice setting participated in the pre-test and checked the clarity of wording and time they took to complete the survey. The finalized questionnaire contained 11 questions regarding the perceived needs for specific HIE items, 16 questions on expected benefits, and 6 questions related to concerns. We used a 5-point Likert scale to measure physician perceptions of an HIE: 1=strongly disagree, 2=disagree, 3=neutral, 4=agree, and 5=strongly agree.
At the beginning of the first week of June 2008, we mailed the survey questionnaire to 50 physicians at the SNUBH and 147 physicians at clinics with a referral agreement with the SNUBH, regardless of their participation in the HIE pilot program. We called the physicians to solicit their participation in the survey 1 week after the mailing and finalized the collection of completed questionnaires by the end of the second week of June 2008. In total, 71 physicians—23 at the SNUBH and 48 at 20 clinics—returned the questionnaire, and response rates were 46% and 33%, respectively. We analyzed 68 responses—23 from the SNUBH and 45 from the clinics—after deleting 3 responses in which the respondents had completed fewer than 50% of the survey items.
Post-Implementation Survey
We developed a computerized survey tool to capture a physician's subjective assessment of the usefulness of information transmitted to him or her by the HIE system. The computerized instrument was composed of data-entry areas where a physician indicates whether an information item transmitted by the HIE system was useful in making clinical decisions for an individual case. Information items were classified into six types of medical services: medication, laboratory or imaging results, clinical findings, working diagnosis, operation or procedure, and medical history.
We invited all physicians using the HIE system to participate in the post-implementation survey, and 40 of them accepted our invitation (15 from the SNUBH and 25 from the clinics). Physicians had routine consultations with their patients referred via the HIE system and then entered data using the computerized survey tool after the consultation session. It was not feasible for physicians to undertake the survey during encounters with patients because of heavy patient loads during the sessions. We collected data for all cases which the participating physicians treated in the HIE pilot program, and in total 895 cases (702 from the SNUBH and 193 from the clinics) were included in the analysis. Cases from the clinics reflect patients who were referred back to the clinics for routine care after completion of care at the SNUBH and likely represent those with chronic conditions.
Analysis
For the pre-implementation survey, we computed descriptive statistics for responses measured on the 5-point Likert scale and frequency distributions for categorical responses. We performed one-way analyses of variance to examine whether physician practice settings significantly affected their perceptions. The response rates of survey questions were over 94%, and we deleted nonresponses from the analysis that involved the particular data item.
For the post-implementation survey, we defined two indices to identify the patterns of information transmission and utilization: Information transmission rate (ITR) and information utilization rate (IUR). The ITR for each information item was computed as the proportion of the number of cases with a specific information item transmitted via the HIE system to the total number of cases in the post-implementation survey. The IUR for each information item was defined as the proportion of the number of cases in which the physician indicated that the transmitted information item was useful in making clinical decisions to the number of cases in which the specific information item was transmitted via the HIE system. We reported ITRs and IURs at the SNUBH and clinics separately, and we performed Fisher's exact test to assess the significance of the differences in indices between the SNUBH and clinics. SAS version 9.2 for Windows (SAS Institute Inc., Cary, NC) was used for statistical computations and tests.
Results
Physician Characteristics
Most physicians participating in the pre-implementation survey were in their 30s, and all of them were specialists (Table 1). Internal medicine was the most frequent specialty, followed by ophthalmology, obstetrics and gynecology, and otorhinolaryngology. We found no significant differences in gender, age, and specialty distributions between physicians at the tertiary-care hospital and those at clinics. Most physicians who participated in the post-implementation survey were in their 40s, and internal medicine was the most common specialty, followed by pediatrics, ophthalmology, and otorhinolaryngology (Table 1).
Physicians' Demographic and Practice Characteristics
Data are n (%) values.
Perceived Need for Hie
Physicians in both the tertiary-care hospital and clinics agreed, with the mean score of 4.2, that an HIE is needed (Table 2). The extent of endorsements was not significantly different between the two groups. Physicians expressed the most agreement with statements regarding the need for the exchange of information about pathology and lab reports, medication information, and diagnoses with chief complaints. However, they expressed less agreement with statements regarding the need for the exchange of the data items, functional test images and charts, care plans at the referring clinic/hospital, and duration of treatment.
Perceived Need for the Overall Health Information Exchange System and Specific Health Information Exchange Items
Data are mean±standard deviation values.
The p value indicates significance of the difference as measured by one-way analysis of variance between the responses of physicians in the tertiary-care hospital and clinics.
Scoring scale: 1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree.
HIE, health information exchange.
Although the levels of agreement with the overall need assessments were not different for the two groups of physicians, the levels of agreement regarding specific information items differed by physician group. Respondents from the tertiary-care hospital, who are usually users of exchanged information, expressed significantly higher agreement than those at clinics regarding the need for lab reports (p=0.005), diagnostic images (p=0.038), and duration of treatment information (p=0.027). However, responses regarding information about the care plan at the referring clinic/hospital were significantly higher among physicians at clinics compared with responses by physicians at the hospital (p=0.028).
Perceived Benefits and Concerns Regarding Hie
The statements about HIE benefits to which respondents most strongly agreed were in the quality domain: Elimination of duplicated medication as well as lab and imaging tests, prevention of drug–drug interactions, better decision on the care plan and expedited diagnosis, and better ability to explain care plans to patients (Table 3). Physicians also agreed that the HIE would improve the accuracy of diagnoses, expedite decisions on care plans, improve patients' trust in doctors, and help hospital and clinic reputation. Respondents ranked statements articulating the benefits in the cost and time domains lower than those in the quality domain: Savings in healthcare and administrative costs and time in patient care and administrative jobs. We did not find any significant difference in the perceptions of the two groups.
Perceived Benefits and Concerns Regarding the Health Information Exchange
Data are mean±standard deviation values.
The p value indicates significance of the difference as measured by one-way analysis of variance between the responses of physicians in the tertiary-care hospital and clinics.
Scoring scale: 1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree.
However, the HIE concerns of the two groups differed significantly, except in regard to revenue decreases. The physicians at the tertiary-care hospital strongly agreed with statements regarding the possibility of patient privacy and information security breaches and the possibility of disruption in patient care caused by system breakdown. They also indicated concern about possible disputes among care providers in cases of malpractice incidents. The largest perception gap between physician groups was found in the responses to statements of concern about the increase in information system costs. Physicians at the both hospital and clinics were least worried about a decrease in revenue, indicating their consistently expressed low expectations about HIE-generated savings in healthcare costs.
Pattern of Information Transmission
The ITR from clinics to the tertiary-care hospital was the highest for clinical findings (79.8%) followed by working diagnosis (70.5%), whereas the ITR from the tertiary hospital to clinics was the highest for working diagnosis (99.5%) followed by laboratory or imaging result (80.3%) (Table 4). The volume of transmission, measured by ITRs, was significantly lower for information sent from clinics to the tertiary-care hospital than for that from the tertiary-care hospital to clinics for most items, except for clinical findings.
Pattern of Information Transmission Within the Health Information Exchange System
The p value indicates significance of difference in information transmission rate (ITR) based on Fisher's exact test between the information transmission from clinics and the transmission from the tertiary-care hospital.
Pattern of Information Use
Physicians at the tertiary-care hospital found lab or imaging results useful in 88% of cases referred to them with the information, and physicians at clinics found the information useful in 73% of cases referred back to them with the information (Table 5). The IUR for lab or imaging results in the tertiary-care hospital was larger than the rate in clinics (p<0.0001). The IUR for medication was the second highest as ranked by physicians in both clinics and the tertiary-care hospital (70% and 43%, respectively), and the medication information at the tertiary-care hospital was more valuable for cases referred back to clinics than the information at clinics for cases referred to the tertiary-care hospital (p<0.0001). The usefulness of information on clinical findings, working diagnosis, operation or procedure, and medical history was ranked relatively low even when it was available in the HIE system.
Pattern of Information Utilization Within the Health Information Exchange System
The p value indicates significance of difference in information utilization rate (IUR) based on Fisher's exact test between clinics and the tertiary-care hospital.
Discussion
In this study, we conducted a quantitative survey of physicians in a tertiary-care hospital and clinics prior to the rollout of an HIE system to examine physicians' pre-experience perceptions of an HIE and conducted a survey about the usefulness of information transmitted to physicians in the participating hospital and clinics to examine their usage of exchanged information in clinical decision-making after an HIE pilot program was launched in South Korea. Consistent with findings of previous studies from other nations, Korean physicians in both hospital and clinics indicated a strong agreement with statements about the need for an HIE and the benefits of the technology, but they also expressed concerns about information safety and security, system costs, and medical disputes between providers in cases of malpractice. 21,22,24,25 However, we found significant differences in the details of HIE endorsement between the physician groups as reflected by characteristics of their practice settings. Tertiary-care hospitals have a large, complex organizational structure with many physicians in more than 20 specialties. Patients are most typically referred to the hospital for further management by physicians at a clinic. On the other hand, clinics have a relatively simple organizational structure with fewer physicians in a few specialties than hospitals. Patients are typically referred back to a clinic for routine care after the completion of care at the tertiary-care hospital. Furthermore, physicians at the tertiary-care hospital are likely to be more experienced with health information technology than their counterparts in clinics. The data from an information item-specific needs assessment indicated that physicians at the tertiary-care hospital had greater need for most information items than their counterparts at clinics and that the hospital doctors also expressed greater perceived concerns. However, the data from the post-implementation survey indicated that those in clinics were more likely to find useful information in the HIE system than those in the tertiary-care hospital. The results indicated that a greater volume of information, including data about a larger variety of medical services, flows from the tertiary-care hospital to the clinics compared with the information flow in the opposite direction. Hincapie et al. 20 concluded in a focus group study of 29 physicians who have experienced the Arizona Medical Information Exchange program that the data availability in the system would be the limiting factor in realizing the expected effects of the technology, and the finding implies that the benefit potential of the technology would be larger in clinics than in hospitals.
We found in both the pre-implementation and the post-implementation survey that information containing pathology and lab results, diagnostic imaging, medication, and working diagnosis were the most needed and valued by physicians in both practice settings, which implies a potential of the HIE for saving healthcare costs by reducing duplicate lab or imaging tests and improving the quality of care by assisting physicians in clinical decision-making. However, we also found different patterns of physician-ranked value for specific information transmitted to a tertiary-care hospital from a clinic and information sent to a clinic from a tertiary-care hospital: Physicians at the tertiary-care hospital found a significantly higher proportion of transmitted information containing lab and imaging results useful than did their counterpart at clinics did (88.2% versus 72.9%), whereas physicians at clinics found significantly higher proportions of transmitted information containing medication and working diagnosis useful than their counterparts at the tertiary-care hospital did (70.1% versus 43.1% and 13.5% versus 0.6%, respectively). The finding indicates that the potential benefit of the exchange of specific information will vary by the type of care providers and the diseases of patients (or the case mix of patients).
Physicians in both practice settings agreed or strongly agreed with statements about the quality-domain benefits of an HIE, and they least agreed that time and cost savings in the delivery of healthcare would be benefits of an HIE. This finding stands in refutation of the frequently quoted benefits of the technology in literature. 2,3,8,9,25 Physicians also indicated they were least worried about the compromise in their revenue as the result of the technology. Although this finding needs further study with empirical data, it suggests that the much-discussed physicians' concern about the reduction in revenues may not be the biggest hurdle in introducing an HIE in South Korea, where medical services are paid by a fee-for-service method.
We may draw three implications for successful implementation of the HIE technology from these study findings. First, the adoption and diffusion strategy needs to be tailored to the type of physician practice and patient disease as guided by an understanding of physicians' specific needs and perceived value of exchanged information. Also, policy makers need to account for the uneven costs and benefits of the technology among physicians in tertiary-care hospitals and clinics. Second, education and a strict guideline for patient information safety and security may be needed, particularly for physicians in clinics as they indicated a relatively lax attitude on this issue. Finally, the government and payers may need concerted efforts, including payment reform and other initiatives, in addition to an HIE to realize the much anticipated potential of saving healthcare costs. Sharing information through an HIE appeared to be insufficient in achieving the goal.
The study findings and implications are subject to limitations. The generalizability of results drawn from the study of an HIE pilot program in South Korea should be carefully examined when one attempts to apply them to other countries with different healthcare and sociopolitical environments from those of South Korea. Furthermore, we studied a fairly restricted segment of physicians who practice medicine in a government-owned tertiary-care hospital and private clinics in the Seoul metropolitan area and who have been using EMRs, an indicator of high exposure to the information technology. The findings may not represent perceptions and attitudes of physicians in other practice settings. Lastly, physicians participating in the post-implementation survey did not represent the demographic and specialty characteristics of all physicians in the HIE system.
Despite the limitations, the study findings provide policy makers and practitioners with further knowledge needed to formulate effective policy for adoption of HIE technology and to design a system such that providers and users can reap the expected benefits from it. Further study concerning the association between patients' clinical characteristics and physicians' perceived value of an HIE would close an important knowledge gap in the search for an effective implementation strategy in HIE efforts. Also, additional studies with empirical data that could be used to examine costs and benefits of the technology from the perspectives of physicians in different practice settings are needed to design an effective nationwide implementation policy.
Footnotes
Acknowledgments
The authors thank the staff of the Center for Electronic Health Record, the Seoul National University Bundang Hospital, who wrote the computer software used in the post-implementation survey and assisted in the data collection. The authors also thank the physicians who took their time to participate in the study. This study was funded by grant A050909 of the Korea Healthcare Technology R&D Project of the Ministry of Health and Welfare of the Republic of Korea. Dr. H. Hwang was supported by the Industrial Strategic Technology Development Program (grant 10038690, Global Healthcare Software Framework Development) funded by the Ministry of Knowledge Economy of the Republic of Korea. The study sponsors had no role in the study design, the collection, analysis, and interpretation of data, the writing of the manuscript, or the decision to submit the manuscript for publication.
Disclosure Statement
No competing financial interests exist.