
Abstract
Background:
Despite excellent survival rates, health-related quality of life detriments are common in differentiated thyroid cancer survivors and can be driven by fear of cancer recurrence (FCR). This review aims to report the incidence of FCR in thyroid cancer survivors and synthesize evidence regarding contributing factors. An overview and appraisal of the range of tools used to measure FCR is presented.
Methods:
A systematic review of the English literature was performed. The search across six electronic databases generated 3414 studies. Two reviewers independently screened the citations and full-text articles, of which 31 were included. The data were extracted independently by two reviewers.
Results:
The incidence of FCR was reported in 27/31 studies and ranged from 15% to 91%. Direct comparisons regarding incidence and severity of FCR were not possible due to heterogeneity in cut-points used to define FCR. A total of eight validated tools were used to measure FCR across all studies, with five studies using self-developed nonvalidated items. There was minimal repetition of validated tools and no clear consensus as to a preferred survey tool. Factors influencing FCR were reported in 11 studies. There was minimal overlap of factors influencing FCR. Risk factors contributing to increased FCR reported in more than one study included young age and an upcoming clinical appointment. Male gender and higher education levels were reported in more than one article as protective. No literature evaluating interventions to address FCR in thyroid cancer survivors was found.
Conclusion:
FCR is common in thyroid cancer survivors, but significant heterogeneity in the current evidence base limits assessment of incidence, severity, or risk factors. There is a need to use validated tools to assess FCR in both research and clinical contexts. Reliable assessment of FCR may permit routine assessment of FCR in clinical practice and allow interventions to be prospectively evaluated to optimize the holistic well-being of thyroid cancer survivors.
Introduction
In most developed nations, the number of patients diagnosed with thyroid cancer has increased threefold in 30 years. 1 Much of this increase has been attributed to the use of neck imaging for various indications, leading to incidental detection and potential overdiagnosis of some thyroid cancers. 1 –4 Despite excellent clinical outcomes for the majority with differentiated thyroid cancer (DTC), some survivors experience significant ongoing psychosocial concerns, which decrease their health-related quality of life (HRQoL) and can impact their return to work, education, and family and caring roles. 5 –8 These impacts can be comparable with, or more severe than, survivors of other cancer types with a less favorable prognosis. 9,10
Fear of cancer recurrence (FCR) is defined as “fear, worry, or concern relating to the possibility that cancer will come back or progress.” 11 Clinical FCR manifests as (1) high levels of preoccupation, worry, rumination, or intrusive thoughts about cancer; (2) maladaptive coping; (3) functional impairments; (4) excessive distress; and (5) difficulties making plans for the future. 12 FCR is common among all cancer survivors, affects psychosocial function, and is one of the most common unmet needs. 13,14
In thyroid cancer survivors, FCR is common and the severity correlates poorly with the true risk of recurrence. 15 –17 FCR has been suggested as a prominent driver of HRQoL detriments 17 –19 and may impact on decision-making regarding the extent of surgery in those with low-risk thyroid cancer. 16,20
A better understanding of FCR in DTC survivors is a crucial step in improving HRQoL outcomes. An evidence-based foundation is essential to providing a framework for assessing FCR in clinical practice and for developing and evaluating interventions aimed at reducing the impacts of FCR in thyroid cancer survivors. This article sets out to systematically review and analyze the FCR research in thyroid cancer, including identifying the incidence of FCR; describing factors that contribute to FCR; and reporting the range of tools used to identify and describe FCR.
Methods
A systematic literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement, 21 and prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD42021293277). The aim of the search was to identify all studies that assessed FCR in adult thyroid cancer survivors. The aim of this study was to examine from the available literature (1) the incidence of FCR in thyroid cancer survivors; (2) factors that increase or decrease FCR; and (3) to examine the instruments used to measure FCR.
Search strategy
The literature search was conducted in September 2023 using the electronic databases Medline, EMBASE, CENTRAL, PSYCInfo, Emcare, and CINAHL. There were no limitations on year of publication. The full search strategy is presented in Supplementary Data S1. In brief, the terms “thyroid neoplasm” or “thyroid cancer” or “thyroid malignancy” or “thyroid tumour” were combined with “quality of life” or “health related quality of life” or “fear of recurrence” or “fear of cancer recurrence” or “fear of progression” or “fear of cancer progression.”
Studies were limited to English language publications in peer-reviewed journals. The literature search and associated data were managed using Covidence. 22 A reference check and hand search were also conducted to capture all available literature.
Study selection
Studies were included if the total cancer population studied contained more than 50% of survivors with DTC and reported outcomes related to FCR that addressed the study aims. Publications were excluded if the study had >20% of participants <18 years of age; the study focused on patients who were terminally ill (life expectancy <6 months); or the study focused on survivors with thyroid disease other than DTC.
Two authors (J.H. and A.A.) independently screened the titles and abstracts of the studies identified to exclude those that did not meet the inclusion criteria (Supplementary Data S2). Any discrepancies were resolved between the two reviewers after discussion and those that could not be resolved required arbitration by a third author (C.O.). Data were independently extracted from the included studies into a pre-piloted template by the two reviewers (Supplementary Data S3).
The extracted data were subsequently compared by the two authors and discrepancies resolved. The outcomes included reported incidence of FCR; factors associated with increased or decreased FCR; and the tools used to measure FCR in the thyroid cancer populations of the included studies. Additional data points extracted included authors, country, year of publication, study design, number, and characteristics of participants.
Quality appraisal of studies
For this review, two authors (J.H. and A.A.) independently appraised the study quality using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-sectional Studies and the JBI Checklist for Qualitative Research (Supplementary Data S4). 23,24
Results
Studies and characteristics
The search strategy identified 3414 records of which 978 were duplicates. A further 2373 records were excluded based on title and abstract screening leaving 63 articles to be assessed. Of these, 38 were excluded on full-text review (Fig. 1). Reference checking and a hand search identified a further 6 studies (1 additional FCR and 6 additional fear of progression (FoP) studies; 25 –31 however, 1 was excluded as it used the same cohort of recruited survivors over 2 studies). 31
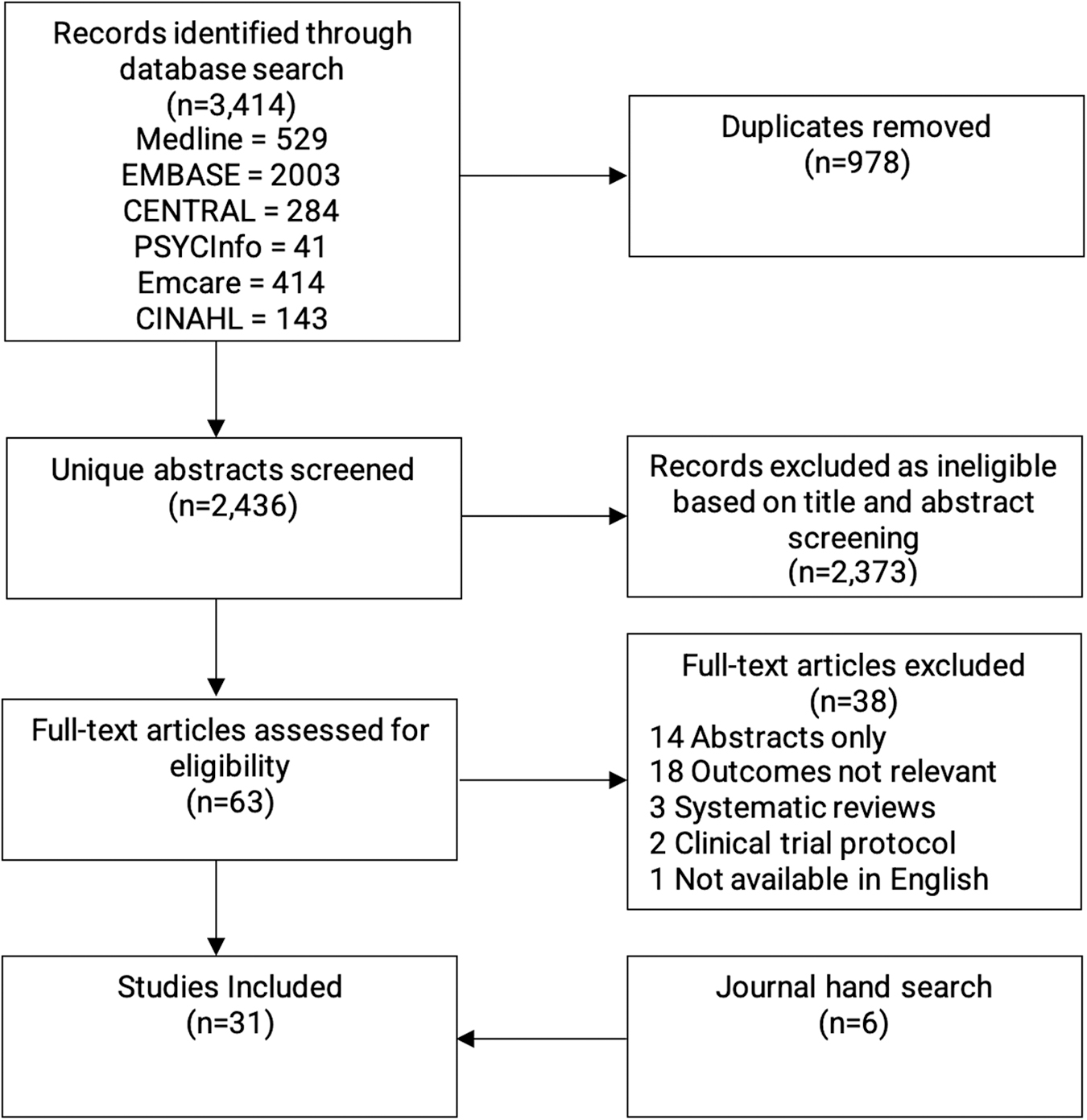
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram.
The primary findings of the 31 included studies are summarized in Table 1. 15,17 –19,25 –30,32 –52 The included studies ranged between 14 and 2215 participants in size, with a wide geographic distribution. The earliest date of publication was 2011. 28
Study Characteristics and Inclusion of Incidence of FCR, Factors Influencing FCR, and Tools Used to Measure FCR
AS, active surveillance; ATA, American Thyroid Association; CNB, core needle biopsy; DTC, differentiated thyroid cancer; FCR, fear of cancer recurrence; FNA, fine needle aspiration; HT, hemithyroidectomy; MDT, multidisciplinary team; PTC, papillary thyroid cancer; PTH, parathyroid hormone; PTMC, papillary thyroid microcarcinoma; RAI, radioactive iodine; RFA, radiofrequency ablation; SEER, The Surveillance, Epidemiology, and End Results; TT, total thyroidectomy.
Of 31 studies, 25 cross-sectional studies and 1 randomized control trial reported FCR using either validated FCR scales; small numbers of items embedded within validated HRQoL surveys or used self-developed nonvalidated items specific to their study. The remaining 5 studies either reported qualitative data or used quantitative data from nonvalidated items specific to their study.
Incidence and severity of FCR
The incidence of FCR was reported by 27 studies and ranged between 15% and 91% of thyroid cancer survivors. 18,37 Most studies simply reported the presence of FCR as a binary outcome, while a small proportion attempted to quantify the severity of FCR. The widest range of responses was found in Rogers et al., where on a single 5-point Likert scale item, 91% of cancer survivors reported some FCR (>1/5) and 14% reported significant FCR (>3/5). 18 In quantitative studies, survivors were asked to rate FCR through a Likert scale that allowed for some gradation of severity.
Comparisons of scores using the same validated tools between studies was limited by differences in the populations studied and comparisons of studies with similar populations but using different tools, limited by a lack of consensus regarding cut-points for FCR in any tool. This lack of a clear definition of FCR, and the substantial variation in the methodology used to assess FCR, limited meaningful comparison of incidence and severity across studies and prevented any meta-analysis of results.
A few studies attempted to quantify FCR, either against other HRQoL issues or as an independent issue. For example, as part of the Phase 1 development for the thyroid cancer module to accompany the European Organisation for Research and Treatment of Cancer quality of life questionnaire–THY34 (EORTC QLQ-THY34), Singer et al. undertook research to identify quality of life priorities in thyroid cancer survivors. 17 A list of HRQoL issues was devised after a literature review, refined by a panel of experts and presented to 110 survivors who were asked to rank the issues in order of priority. FCR was ranked as very important by 67% of respondents, the most frequent of all HRQoL issues presented. 17
Tools to measure FCR
For the purposes of this review, we defined a validated tool as any survey tool where an explanation of the development process could be found in the published literature and followed basic psychometric principles. Eight validated survey tools were identified from the 31 studies included (Table 2). Six tools relate specifically to FCR/FoP, and two thyroid cancer disease-specific HRQoL tools have been included that contain items relating to FCR. 33,37,42,51
Study Tools and Incidence of Fear of Cancer Recurrence as Described in the Literature
This was defined as the number of questions directly related to FCR/number of questions in the tool being used.
Barbus et al. and Kong et al. uses the Romanian and Korean translations of the QOLTV, respectively. Some items were not included with the translation, hence the difference values.
Study identified by hand search of the literature.
There were 5 subcategories: affective reactions, partnership/family, work, loss of autonomy, and coping with anxiety. Only the results of the affective reactions subcategory were used in the table for simplicity. NB: higher scores do indicate greater anxiety for all subcategories, except the final subcategory (coping with anxiety) where a higher score in fact indicates better coping.
ASC, Assessment of Survivor Concerns; Dx, diagnosis; EORTC QLQ-THY34, European Organization for Research and Treatment in Cancer Quality of Life Questionnaire-THY34; FCR7, Fear of Cancer Recurrence Scale 7 items; FCRI, Fear of Cancer Recurrence Inventory; FoP-Q, Fear of Progression Questionnaire; FoP-Q-SF, Fear of Progression Questionnaire–Short Form; HRQoL, health related quality of life; IQR, interquartile range; Mx, management; QOLTV, City of Hope Quality of Life-Thyroid Version; SEM, standard error of the mean; Sx, surgery; T1, timepoint 1; T2, timepoint 2; Tx, treatment.
5-Point Likert scale: 1, not at all; 2, a little; 3, somewhat; 4, quite a bit; 5, very much.
4-Point Likert scale: 1 (least worry) to 4 (most worry).
No single survey tool was used more than five times and comparisons between studies using the same tool were limited by differences in the study populations. The remainder of the studies were either qualitative (evaluating FCR and its impact through interviews and qualitative thematic analysis); 53,54 or used self-developed nonvalidated single items to assess FCR through a Likert scale. 15,17,18,38,39
Specific FCR survey tools
Six FCR-specific survey tools have been used in thyroid cancer survivorship studies (Table 2). Fear of Cancer Recurrence Inventory (FCRI) is a 42-item survey tool that has been used widely in the mixed oncology literature and validated in a number of languages. 55 It has a 7-factor structure (trigger, severity, psychological distress, coping strategies, functioning impairment, insight, and reassurance). 56 It has only been used once in thyroid cancer survivors (in French) as part of the ESTIMABL2 trial, 44 a randomized control trial investigating adjuvant radioactive iodine (RAI) in low-risk DTC. In this study, there was no difference in FCRI between the survivors who received RAI and those who did not. 44
Fear of Cancer Recurrence 7 items was originally used in a group of head and neck survivors from England (excluding thyroid cancer survivors). 57 The scale has subsequently undergone psychometric testing in other cancer types 58 but has only been used in one thyroid cancer study. 18
The Fear of Progression Questionnaire is a 43-item scale validated in chronically ill patients (cancer, diabetes mellitus, and rheumatic disease). 59 It has a 5-factor structure (affective reactions, partnership/family, work, loss of autonomy, and coping with anxiety). 59 It was originally validated in German and then with English and Korean translation. It has since been used in three Korean thyroid cancer studies looking at FCR in survivors with papillary thyroid microcarcinoma who underwent surgery or active surveillance (AS) as well as in postoperative survivors with DTC. 25,28,41
It showed no difference in FCR within their comparison groups. The Fear of Progression Questionnaire Short Form score has 12 items and correlates with the original 43-item score of FoP. 60 It has been validated in mixed oncology patients and used in Chinese, English, and Korean in five thyroid cancer studies to date. 26,27,30,43,48,61
Assessment of Survivor Concerns Scale (ASC) is a validated 5-item brief scale assessing FCR. 62 The original scale had 6 items and included 3 items of cancer worry and 3 items of health worry. After further testing the question on “worry about children's health” was removed. Two studies have used ASC in thyroid cancer survivor cohorts, with Bresner et al. 36 using the 6-item ASC and Bongers et al. 35 using the 5-item tool.
The “Worry scale,” used in the two studies from Papaleontiou et al. 47 and Jackson Levin et al., 40 was adapted from similar scales used in breast cancer and was refined after a literature review, input from clinicians and pilot testing in thyroid cancer survivors. It included five items asking respondents to rate their worry on a 5-point Likert scale related to (1) harms from treatments, (2) changes in HRQoL, (3) other family members risk of thyroid cancer, (4) thyroid cancer coming back, and (5) death from thyroid cancer. Subsequent items asked respondents to rate (on a 5-point Likert scale) the impact of worry on their home and work, family and friends, and if it made them feel upset both at diagnosis (by recall) and during the past month.
Thyroid cancer-specific HRQoL surveys including FCR items
Ten studies used either one of two HRQoL surveys specific to thyroid cancer, which include items relating to FCR.
City of Hope–Quality of Life Thyroid Version (QOLTV) is a 30-question 56-item validated thyroid cancer-specific tool that gives an overall HRQoL score as well as subdomain scores in each of physical, psychological, social, and spiritual domains. 63 FCR is addressed in a single question but with four items addressing future diagnostic tests, a second cancer, recurrence of cancer and spread or metastasis of cancer.
EORTC QLQ-THY34 is a 34-item thyroid cancer-specific survey tool that has recently been validated with a Phase IV study. 52 It contains a subcategory on fear (item specific to worry about disease recurrence, coming off thyroid hormone replacement for RAI and lifelong medication management) but also a subcategory related to worry about important others (items related to worry about the future of those important to you, how those close to you will cope with your illness/treatment and worry that you will be a burden to others). 35
Qualitative studies
There were four semi-structured interview studies included in this review. 19,46,49,50 All specifically explored FCR within their interview scripts. Common themes included anxiety associated with cancer diagnosis and fear of recurrence after treatment. In addition, many felt that their perceptions of the significance of their diagnosis and FCR were invalidated or under-recognized by clinicians and that this contributed to their distress.
Factors influencing FCR
Characteristics that increased or decreased FCR were explored in 11 of the included studies. 15,18,19,36,40,45 –47,49 –51 Apart from age, there was variability between studies regarding characteristics associated with FCR (Table 3). Of the 11 characteristics identified, the majority (8/11) were found to increase FCR: younger age, parenthood, shorter duration since diagnosis (≤5 years), an upcoming appointment related to cancer, greater number of complications or side effects (physical and psychological), distrust in health care, personal experience with cancer-related death, and “good cancer” terminology invalidating fears. Factors that decreased FCR included male gender, a higher level of education (tertiary degree or higher), and planning a daily routine.
Factors Influencing Fear of Cancer Recurrence
Age
Age was the most studied outcome, being reported in six studies. 18,36,40,45,47,49 Younger age was heterogeneously defined between studies as <65, <50, <55, <45, or <40 years of age. Younger people were more likely to report FCR (61.3% vs. 47.6%) 40 and also reported more severe worry (33% of younger people had “a lot of fear” or were “fearful all the time” compared with 5% of older people). 18 Older people were less likely to report any worry 47 and also reported less concerns about scarring, headaches, side effects of cancer treatment, and thyroid-function-related problems. 18
Gender
The impact of gender was examined in three studies. 18,36,51 In Rubic et al. and Rogers et al., women reported a statistically significant higher severity of FCR 18,51 while in other studies the association of higher FCR in women was not significant. While in Rubic et al., men reported lower FCR and less difficulty with some physical symptoms, they generally scored higher for levels of distress about treatment and thyroid hormone withdrawal than women. 51 Bresner et al. reported increased cancer-related worry (3-item subscale of ASC) in women who were married or had children. 36
FCR and extent of surgery or treatment
Four studies assessed FCR in cohorts based on extent of surgery. 35,41 –43 Kong et al. used the Korean version of QOLTV to compare two cohorts of survivors with low-risk papillary microcarcinoma who chose either AS or immediate surgery. 42 Surveys were performed at diagnosis and during follow-up (median = 8 months). Better physical, psychological, and overall health was observed in the AS group compared with the surgical group both at baseline and during follow-up, as well as comparable FCR between the two groups. 42
Bongers et al. used the 5-item ASC to compare low-risk thyroid cancer survivors. Those who underwent hemithyroidectomy (HT) compared with total thyroidectomy (TT) expressed a statistically significant increased severity of FCR utilizing a single item (mean score 2.4 vs. 2.1, p = 0.021). 35
Leboulleux et al. did not find any difference of FCR (total or in any of the 7-factor subscales of FCRI) in a trial randomizing postoperative survivors to RAI or observation after TT. 44
Patient perception of risk of recurrence
Chen et al. focused on survivors with low-risk DTC as defined by 2015 American Thyroid Association risk stratification system where estimated risk of recurrence is ≤5%. 15,64 Mailed surveys captured survivors' estimation of their risk of recurrence and measured how much they worried about recurrence and death from thyroid cancer. An overestimation of their own risk of recurrence was associated with increased worry and a lower HRQoL. 15
Trajectory of FCR over time
Six studies measured FCR quantitatively with repeated measures over time. 39,40,42,44,45,52 Hedman et al. found that the incidence of any FCR was lower at 12 months (69%) than at the time of diagnosis (75%). At this 12-month timepoint after diagnosis, only 23% of survivors reported experiencing FCR “often” rather than “seldom” (46%) or “no fear of recurrence” (31%). 39 In contrast, Jackson Levin et al. reported 13.4% of survivors had an increase in worry over time and 39.6% had sustained the same level of high worry over time.
Less than 20% of survivors experienced a decrease in FCR. Jackson Levin et al. collected data at two different timepoints. The first timepoint was 2–4 years after diagnosis and the second timepoint was 1–2 years after the first survey. 40 Leboulleux et al. measured FCR as a secondary end point over a 3-year period and showed that FCR declined in that time. Two groups were measured at randomization then 2 months, 10 months, and 3 years after randomization. Total scores from all seven FCRI domains fell from 48.3 to 39.8 (mean values out of FCRI scoring system from 0 to 168) and from 49.6 to 41.8 over 3 years in the two groups. 44 The clinical significance of any decrease in FCRI scores is not clear.
Quality assessment
The JBI critical appraisal checklist for each study is summarized in Supplementary Data S4. Quantitative studies scored well on patient selection, although some lacked detail of the included study population. 18,26,33,36,40,41,52 Low scores on the exposure measurement domain in 8 studies were due to failure to elaborate on the validity or reliability of the tool used to assess FCR. 15,18,25,27,28,38,39,47 Poor performance on the confounding domain was due to a failure identify potential variables that could affect the outcome, 33,40,42,44,51 or strategies to mitigate their effect. 15,18,25,28,29,33,36,38,39,41,42,44,45,51 All the studies used appropriate and adequate statistical methods for analysis of their results.
The qualitative studies scored well in most JBI domains, with 3 studies lacking adequate patient representation in their cohort and a failure to report the researchers' background or influences. 19,49,50
Discussion
With increasing incidence of low-risk DTC, 1 it is imperative to understand the implications of a “thyroid cancer” diagnosis to patients and to study both disease and psychosocial outcomes. In this review, we have summarized the available literature evaluating FCR in thyroid cancer survivors. Despite the significant heterogeneity of the data, the lack of a clarity around the measurement of clinically significant FCR and the limited ability to compare between studies, collectively, these data confirm that FCR is common, persists over time, and is affected by age, education level, and social circumstances.
Chen et al. have shown that there is discordance between survivors' perception of risk and the true risk of recurrence, and that this contributes to ongoing “worry.” 15 Some studies suggest that survivors with FCR report lower HRQoL, 38 and that FCR can vary based on the extent of surgery. 35 Meaningful comparison between studies is limited by the heterogenous nature of reporting and lack of use of validated tools and repeated measures. It is also concerning that despite finding 31 studies reporting FCR in thyroid cancer survivors, that there are no studies evaluating interventions to address FCR in this group.
Characteristics associated with FCR
Understanding the demographic associations between the incidence and severity of FCR can help clinicians to support thyroid cancer survivors more effectively. Despite only 11 of the 31 studies in this review discussing characteristics associated with FCR, the findings are consistent with the wider FCR literature. Younger age is the most consistent factor both in thyroid cancer and wider cancer survivorship to be associated with increased FCR. 13,18,36,40,47,65,66
There is also evidence in the wider oncology literature that FCR persists for many years in young cancer survivors. 36 Clinicians should be aware that despite the improved prognosis associated with younger age in thyroid cancer, conversely, these survivors are at increased risk of clinical FCR, which can drive HRQoL detriments and adversely affect their social functioning and family interactions. 46,67
The wider oncology literature also suggests that female gender is associated with increased FCR, 11,68 particularly among those who are mothers 69 and those who become pregnant after their cancer treatment. 70 There is also evidence of significant FCR in the caregivers and families of survivors with cancer. 71,72 It is important to be aware of these impacts on thyroid cancer survivors, particularly given the female preponderance and young age of many thyroid cancer survivors.
Other characteristics associated with FCR identified in this review include a shorter duration since diagnosis, an upcoming appointment related to cancer, increased physical side effects, and a distrust in health care. A higher level of education was protective. The evidence is less strong for these associations but collectively the data suggest that all thyroid cancer survivors are at risk of FCR and that this may adversely affect HRQoL. Clinicians need to be educated regarding FCR, open to discussing FCR during consultations, and given tools to assist with screening survivors.
It is important that clinicians are aware that follow-up consultations themselves can trigger FCR, and although many survivors derive reassurance from their consultations, some survivors may suffer more psychological harm than clinical benefit with prolonged follow-up. 36,49 An individualized approach addressing both clinicial and psychosocial well-being is likely to be of benefit to many thyroid cancer survivors. There is also a need to develop and evaluate appropriate pathways to support thyroid cancer survivors with FCR and other psychosocial needs.
Extent of surgery
With recent thyroid cancer guidelines suggesting that de-escalation of thyroid cancer surgery is appropriate, 64 there is a need to understand the impacts of extent of surgery on FCR and HRQoL. 73 There are only four studies included in this review that addressed the impact of extent of surgery on FCR. In Kong et al., Korean survivors with papillary microcarcinoma who chose AS (over surgical intervention) had a higher baseline HRQoL. These survivors experienced less deterioration in HRQoL although their FCR was similar to the surgical intervention group. The median time of follow-up was 8.2 months. 42
In Bongers et al., where survivors selected HT over TT, overall HRQoL did not show a statistically significant difference but FCR was higher in the HT group. 35 The potential for bias in these trials must be acknowledged as survivors self-selected their treatment. While scientifically this may not reach the high level of evidence of randomized trials, it is more likely to reflect real-world outcomes where patient's values (including FCR) should be heard, acknowledged, and incorporated within shared decisions regarding the extent of surgery.
This is consistent with the wider oncology literature, where there is evidence that shared decision-making builds resilience in survivors who suffer adverse events and improves trust in health care providers. 74 When considering the extent of surgery for thyroid cancer, it has been suggested that FCR, along with voice change and the need for thyroid hormone replacement, are critical issues for survivors. 75,76 Future studies regarding the extent of surgery should measure FCR with validated tools. Within clinical consultations, there is a need to assist clinicians with strategies to discuss and evaluate FCR, ensuring that it is openly addressed both at the time of diagnosis and in follow-up. 77
FCR assessment
Many studies in this review have measured FCR alongside HRQoL. Most HRQoL tools do not address FCR specifically, including those used widely in thyroid cancer (Short Form-36, EORTC QLQ-30, and Thyroid Cancer–Specific Quality of Life Questionnaire). 76,78,79 Although EORTC-THY34 and QOLTV contain items relating to FCR, the analysis of single items within these tools is not validated. In addition, none of the tools used in these studies can be used as utility weights or to calculate quality of life adjusted years to enable cost-effectiveness research.
Where dedicated tools are used to assess FCR, the data in this review highlight the lack of agreement as to which FCR tool is most appropriate in thyroid cancer survivors. FCRI is the most used FCR tool in the wider oncology literature. Despite a 42-item scale with a fairly robust 7-factor structure, there is no agreement as to a cutoff score for clinical FCR and its use as a screening tool is not established. 13,80 These limitations highlight the issues of FCR assessment in the wider oncology literature and its relevance to clinical practice.
A recent international Delphi study involving 65 FCR experts identified four key characteristics of clinical FCR: (1) high levels of preoccupation; (2) high levels of worry; (3) that are persistent; and (4) hypervigilance of bodily symptoms. 81 Currently available survey tools may not assess all of these four characteristics; in addition, shorter surveys may both identify survivors with “worries about recurrence” that are occasional and cause little preoccupation (and hence should be normalized) while missing those with more severe FCR but who somatize their concerns or have FCR triggered by physical symptoms. 56,82,83
Nevertheless, shorter FCR surveys are more pragmatic for use within a clinical context. The 9-item short form of FCRI 84 and a 5-item rapid screener 85 have been suggested for screening. Despite the psychometric properties of these tools being assessed, there is debate regarding cutoff points for clinical FCR 86 and concern regarding the clinical utility of isolating the assessment of FCR from other factors that may contribute to anxiety or detriments in psychosocial function. 87 Despite these concerns, it is of interest to note that a single-item screening tool for FCR in the wider oncology population is being proposed. 88
There is a need to reach some consensus regarding the use of FCR tools in thyroid cancer survivors within both a research context and routine clinical practice. Despite the limitations of the current literature, it is imperative that clinicians and researchers wishing to evaluate FCR in thyroid cancer survivors chose a validated FCR tool and attempt to define cut-points of severity. The specific choice of tool needs to balance comprehensive assessment and minimize patient burden. 89
Interventions addressing clinical FCR
While the identification of FCR in thyroid cancer survivors is important, there is a need to develop and evaluate accessible referral pathways and interventions for FCR. The lack of supportive care is a significant unmet need in thyroid cancer survivors. 46,90 High levels of FCR can be associated with increased health care utilization 91,92 and poor psychosocial functioning. 12,20,93,94 There is emerging evidence of the effectiveness of psychological interventions for FCR in mixed oncology survivors. 95 –97
Psychological and behavioral interventions have been trialled in thyroid cancer survivors and although some improvement in psychosocial functioning was seen, these interventions did not specifically target FCR. 98,99 A recent study in breast cancer involved clinicians (oncologists and surgeons) screening survivors for FCR and delivering a brief intervention, including normalization of FCR, provision of individualized prognostication, advice on managing worry, and psychological referral where FCR was severe. 100 –102
This type of approach to screening for FCR within a clinical context, normalizing mild FCR for the majority and referring those with moderate to severe FCR for stepped interventions is a suggested care model currently undergoing investigation. 103 –105 Clinicians involved in thyroid cancer care should be aware of high rates of FCR in thyroid cancer survivors and be educated in FCR screening and brief interventions. There is a need to evaluate interventions for mild, moderate, and severe FCR in thyroid cancer survivors as well as to assess their impact not just on FCR but on global HRQoL.
Limitations and strengths
This review was limited by a lack of unity and agreement regarding the tools used to assess FCR, the cut-points to define FCR and the evaluation of factors that may contribute to FCR. Rather than limit inclusion criteria for studies, we elected to include all studies that reported FCR in DTC survivors and focus on the breadth of findings. Despite a list of search terms designed to capture this breadth, and specifically including both “fear or cancer progression” and “fear of cancer recurrence,” our search strategy did not identify all relevant articles.
In particular, hand searching was required to identify FoP studies. We also acknowledge that by including only studies that addressed FCR, we have not included all studies evaluating HRQoL in DTC survivors, in particular omitting some that have used thyroid cancer disease-specific tools but have not commented specifically on FCR items. We also did not include studies that were not published in the peer-reviewed literature.
The heterogeneity of methodology, wide range of incidence and lack of reporting of associated factors with FCR found by this review, limits our understanding of how survivors experience FCR and how this can be mitigated. In particular, the associations regarding FCR and other factors must be interpreted in this context. Even young age, for which the evidence base is strongest, 13 lacked any consistency with five different age cutoffs used in this review alone.
The number of tools also reflects a lack of unity and agreement within the FCR research community. 79 Instead of using the existing survey tools, many studies used their own questions. These questions were often similar but not immediately comparable, exacerbating the insufficiencies in the literature.
Despite these inconsistencies, this review highlights the breadth and extent of FCR in thyroid cancer survivors. It also emphasizes the value of using validated tools in FCR assessment that will assist survivors, clinicians, and researchers to quantify FCR and its risk factors. Accurate measurement and quantification of FCR is essential to FCR assessment throughout the patient journey; allowing survivors who would benefit from supportive care to be identified and interventions to be developed and evaluated.
Acknowledging and openly discussing potential FCR with survivors is important in deciding the extent of surgery and in screening for psychosocial concerns during follow-up. 83 There is an urgent need to develop and evaluate interventions for survivors with significant FCR such that patient well-being can be optimized. 11,77,106
Conclusion
FCR is over-represented in DTC survivors with younger women most at risk. While there is no clear consensus on the most appropriate tool to measure FCR in thyroid cancer survivors, a validated tool should be used in both clinical and research settings. At the time of diagnosis, the role of FCR in shared decision-making around the extent of surgery should be openly discussed. There is an urgent need to evaluate the clinical utility of screening for FCR during thyroid cancer follow-up. Where FCR is significant, supportive care pathways and FCR interventions are required to support optimized well-being.
Footnotes
Acknowledgment
The authors would like to thank Ms. Jennifer Goh, a Teaching Liaison Librarian through the University of Newcastle Library, for her support in defining the term for the search strategy of this systematic review.
Authors' Contributions
Methodology, screening, full-text review, extraction, analysis, and writing by J.H. and A.A. Conceptualization, supervision, methodology, and editing by N.Z. and C.R. Conceptualization, supervision, and methodology by E.F. Conceptualization, methodology, supervision, writing, and editing by C.O.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4