
Abstract
Background:
Reference ranges for serum thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) established without considering age- and sex-based differences are currently used to evaluate thyroid function. Therefore, we investigated age- and sex-based differences in serum TSH and thyroid hormone levels in euthyroid individuals.
Methods:
We performed cross-sectional analyses of retrospective data collected from two Japanese institutions. We estimated sex-specific 95% reference ranges for TSH and fT4 according to age strata.
Results:
We included data from 14,860 participants undergoing screening with a Siemens thyroid testing kit and 8,132 participants undergoing screening with an Abbott kit during annual health check-ups at Takasaki Hidaka Hospital. In addition, 515 participants visiting a specialized thyroid-focused hospital were evaluated using Tosoh kits. The median TSH level of women in their 30s was 1.5 mIU/L (2.5th percentile, 0.5; 97.5th percentile, 4.6) using the Siemens kit, while that of women in their 60s was 1.9 (0.7–7.8) mIU/L. The corresponding levels were lower in men; the age-associated increase was small. The median serum fT4 level of men in their 30s was 1.3 (1.0–1.7) ng/dL and that of men in their 60s was 1.2 (1.0–1.6) ng/dL. These levels gradually but significantly decreased with age. fT4 levels in women were lower than those in men and remained consistent with age. Serum fT3 levels were significantly higher in men than in women and gradually but significantly decreased with age. The Abbott and Tosoh kits showed similar results. When using the Siemens kit, ∼60% (216/358) of women diagnosed with subclinical hypothyroidism using manufacturer-recommended reference ranges had normal results when age- and sex-specific reference ranges were applied, demonstrating the high percentage of overdiagnosis, especially in those aged ≥60 years. Conversely, some middle-aged individuals with normal thyroid function were reassessed and classified as having subclinical hyperthyroidism by age- and sex-specific reference ranges.
Conclusions:
Age- and sex-specific reference ranges should be used to avoid over- and underdiagnosis of subclinical thyroid dysfunction and appropriate therapies.
Introduction
Thyroid hormones (THs)
Therefore, it is used to diagnose subclinical hypothyroidism and hyperthyroidism. Subclinical hypothyroidism is defined as the presence of slightly elevated serum TSH levels with TH levels, particularly free thyroxine (fT4) levels, within the normal reference range. Conversely, subclinical hyperthyroidism is defined as the presence of reduced serum TSH levels with normal TH levels.
Establishing the normal reference range, especially for serum TSH, is critical in diagnosing subclinical thyroid dysfunction accurately. However, in clinical settings, single reference ranges of serum TSH, fT4, and free triiodothyronine (fT3) are generally used to evaluate thyroid function without considering natural physiological differences based on age and sex. Many investigators have investigated the effects of subclinical thyroid dysfunction on lipid metabolism, osteoporosis, cardiovascular events, and cognitive mental disease, and the benefits of medications for normalizing TH levels. 4 –14
However, a consensus is lacking regarding the optimal serum TSH level to initiate levothyroxine administration in individuals diagnosed with subclinical hypothyroidism, particularly in older adults. 5,7,9,10 In addition, the evidence of benefit of treatment for subclinical hyperthyroidism (e.g., antithyroid medications, radioiodine therapy, and thyroidectomy) remains unclear.
Therefore, several investigators have attempted to categorize several serum fT4 levels instead of using serum TSH levels to define subclinical thyroid dysfunction. 15 –17 Furthermore, several systematic reviews have reported the treatment effectiveness for subclinical thyroid dysfunction. 6,10 –12 However, in several articles in these systematic reviews, patients were diagnosed with subclinical thyroid dysfunction using single reference ranges of serum TSH, fT4, and fT3 levels. Therefore, substantial overdiagnosis and overtreatment of subclinical thyroid dysfunction are expected to occur on a global scale.
This study assessed serum TSH and TH levels in clinically euthyroid individuals and investigated age- and sex-based differences using kits from three different manufacturers in Japan, an iodine-sufficient country.
Materials and Methods
Among those who underwent annual health check-ups at Takasaki Hidaka Hospital (Takasaki, Japan), a total of 14,860 (8,904 men, 5,956 women) participants were tested using Siemens kits (Munich, Germany) in 2006–2013, and 8,132 (4,682 men and 3,450 women) participants were tested using Abbott kits (Chicago, IL) in 2020–2022 (Fig. 1). In Hidaka Hospital, while some participants were hospitalized, others were outpatients. In addition, to assess the Tosoh kits (Osaka, Japan), 515 euthyroid patients (99 men and 416 women) who visited Okamoto Thyroid Clinic, a specialized thyroid-focused hospital, in 2016–2019 were enrolled.
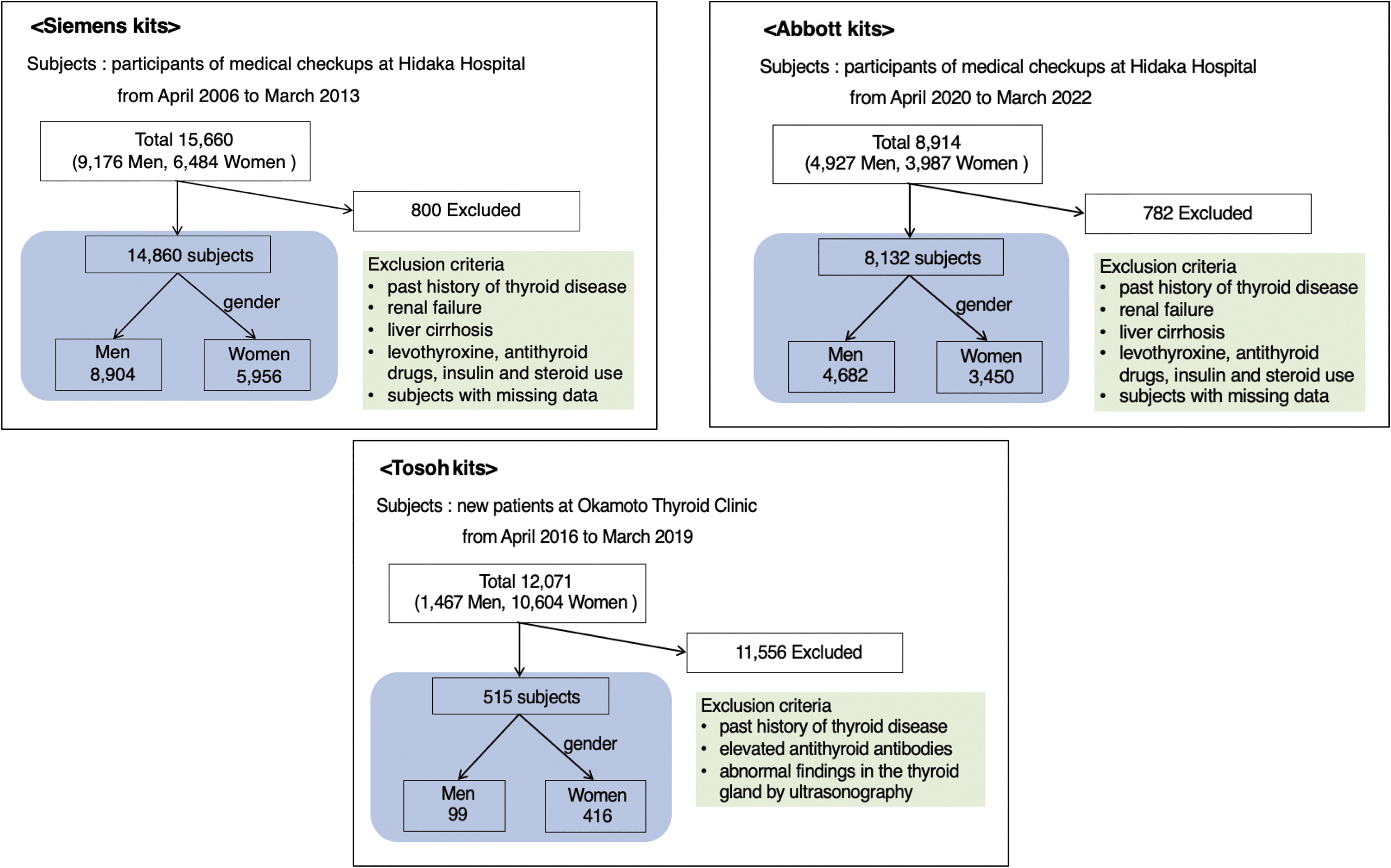
Flow diagrams for participants examined with Siemens kits (upper left panel), Abbott kits (upper right panel), and Tosoh kits (lower panel).
Patients who visited Hidaka Hospital were asked to complete a self-administered questionnaire, which included questions on medical history and medication use. The exclusion criteria were (i) any history of thyroid diseases, liver cirrhosis, or renal failure; (ii) current medications that affect TH levels, including levothyroxine, antithyroid drugs, insulin, and steroid hormones; and (iii) missing data. Furthermore, among patients who visited Okamoto Thyroid Clinic, patients with (i) a history of thyroid disease, (ii) elevated antithyroid antibodies, or (iii) abnormal findings in the thyroid gland by ultrasonography were excluded.
Subclinical hypothyroidism was defined as the presence of elevated serum TSH levels with fT4 levels being within the normal reference range. Conversely, subclinical hyperthyroidism was defined as the presence of reduced serum TSH levels with normal fT4 levels.
The study was performed in accordance with the relevant guidelines and regulations, including ethical guidelines for medical and health research involving human subjects presented by the Ministry of Health, Labour and Welfare in Japan. Approval was obtained from the ethics committee on human research of Gunma University Hospital (approval number HS2022-055) that oversaw the research conducted from both participating institutions. According to the aforementioned ministry guidelines, written informed consent was not required. Moreover, we widely disclosed the outline of our study and provided opportunities for disagreement and withdrawal at any time during the investigation. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Blood tests for serum TH and TSH levels
In Hidaka Hospital, blood samples were collected from patients in the morning between 8:00 am and 9:00 am, after fasting for at least 11 hours, and in Okamoto Thyroid Clinic, blood samples were collected ad libitum between 9:00 am and 6:00 pm. Serum TSH and TH levels were measured using the following kits:
TSH: Chemilumi ACS II, chemiluminescence immunoassay (CLIA), and Chemilumi E-FT4, CLIA (Siemens Healthcare Diagnostics) were used to measure TSH and fT4, respectively, using the Siemens tests. All samples were measured in the hospital laboratory. The manufacturer's reference ranges were 0.4–4.0 mIU/L and 0.8–1.9 ng/dL for serum TSH and fT4, respectively.
Architect TSH chemiluminescence immunoassay (CLIA), FT4•Abbott CLIA, and FT3•Abbott CLIA (Abbott, Inc.) were used to measure TSH, FT4, and FT3, respectively, using Abbott tests. The manufacturer's reference ranges were 0.35–4.94 mIU/L, 0.70–1.48 ng/dL, and 1.71–3.71 pg/mL for TSH, fT4, and fT3, respectively. All samples were measured using the Architect i2000SR in the hospital laboratory.
CL AIA-PACK TSH chemiluminescence enzyme immunoassay (CLEIA), CL AIA-PACK FT4 CLEIA, and CL AIA-PACK FT3 CLEIA (Tosoh Corp.) were used to measure TSH, fT4, and fT3 levels, respectively, using Tosoh tests. The manufacturer's reference ranges were 0.4–4.0 mIU/L, 0.75–1.9 ng/dL, and 1.8–3.5 pg/mL for TSH, fT4, and fT3, respectively.
Statistical analyses
Median, percentile, p-value, and confidence interval values were calculated using JMP 15.2.0 statistical software (SAS Institute Inc., Cary, NC). Multiple comparisons of median serum TSH, fT4, and fT3 levels were conducted using Dunn's multiple comparison test.
Results
The test results for serum TSH, fT4, and fT3 using the Siemens, Abbott, and Tosoh assays are summarized in Tables 1 (women) and 2 (men).
Reference Range (2.5th–97.5th Percentile) of Serum Thyrotropin, Free Thyroxine, and Free Triiodothyronine Levels in Women, Measured Using Assays from Three Different Manufacturers
fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin.
Serum TSH levels according to age and sex
Using the Siemens kit, the median serum TSH levels were 1.5 (2.5th–97.5th percentile: 0.5–4.6) mIU/L and 1.9 (0.7–7.8) mIU/L in women aged 30–39 and 60–69 years, respectively (Table 1). There was a gradual but statistically significant increase in TSH levels with age. The median serum TSH levels were 1.4 (0.4–3.7) mIU/L and 1.6 (0.5–5.7) mIU/L in men aged 30–39 and 60–69 years, respectively (Table 2). The TSH levels were lower in men than in women, with a smaller increase with age.
Reference Range (2.5th–97.5th Percentile) of Serum Thyrotropin, Free Thyroxine, and Free Triiodothyronine Levels in Men, Measured Using Assays from Three Different Manufacturers
Similarly, using the Abbott kit, the median serum TSH levels were 1.27 (0.39–3.81) mIU/L and 1.60 (0.47–5.55) mIU/L in women aged 30–39 and 60–69 years, respectively. The median serum TSH levels were 1.17 (0.40–2.82) mIU/L and 1.38 (0.43–4.60) mIU/L in men aged 30–39 and 60–69 years, respectively. The TSH levels were lower in men than in women, with a smaller increase with age.
Using the Tosoh kit, the median TSH levels were 1.46 (0.48–3.68) mIU/L and 1.70 (1.01–3.85) mIU/L in women aged 30–39 and 60–69 years, respectively. The median TSH levels were 1.14 (0.68–3.33) mIU/L and 1.33 (0.60–2.46) mIU/L in men aged 30–39 and 60–69 years, respectively. The number of patients tested using the Tosoh kit was not sufficient for further statistical evaluation.
Serum fT4 levels according to age and sex
Using the Siemens kit, the median serum fT4 levels were 1.2 (0.9–1.5) ng/dL and 1.2 (0.9–1.6) ng/dL in women aged 30–39 and 60–69 years, respectively (Table 1). The levels in women remained constant with age. fT4 levels in men (Table 2) were higher than those in women, particularly in younger men, and gradually but significantly decreased with age.
The results of tests performed using the Abbott kit were similar to those performed using the Siemens kit. The median serum fT4 levels were 1.02 (0.84–1.26) ng/dL and 1.03 (0.83–1.28) ng/dL in women aged 30–39 and 60–69 years, respectively. The levels of fT4 in women remained constant with age. The levels in men were also higher than those in women in samples tested using the Abbott kit, particularly in younger men, and decreased gradually but statistically significantly with age.
Using the Tosoh kit, the median serum fT4 levels were 1.11 (0.83–1.42) ng/dL and 1.04 (0.78–1.31) ng/dL in women aged 30–39 and 60–69 years, respectively. The levels in women remained constant with age. fT4 levels were higher in men than in women, particularly in younger men, and gradually decreased with age.
Serum fT3 levels according to age and sex
Using the Abbott kit, the median serum fT3 levels were 3.26 (2.58–3.91) pg/mL and 3.11 (2.44–3.73) pg/mL in men aged 30–39 and 60–69 years, respectively (Table 2). The serum fT3 levels were significantly higher in men than in women in the same age group and gradually but statistically significantly decreased with age.
Using the Tosoh kit, the median serum fT3 levels were 2.59 (2.28–3.18) pg/mL and 2.51 (2.30–2.74) pg/mL in men aged 30–39 and 60–69 years, respectively. The serum fT3 levels in men were significantly higher than those in women in the same age group and gradually decreased with age.
Significance of using age- and sex-specific reference ranges for diagnosing subclinical thyroid dysfunction
From the mentioned results, it appeared that the differences in serum TSH and TH levels according to age and sex suggest that age- and sex-specific reference ranges should be used to diagnose subclinical thyroid dysfunction. Thus, we investigated the potential clinical impact of using age- and sex-specific reference ranges on the diagnosis of subclinical thyroid dysfunction.
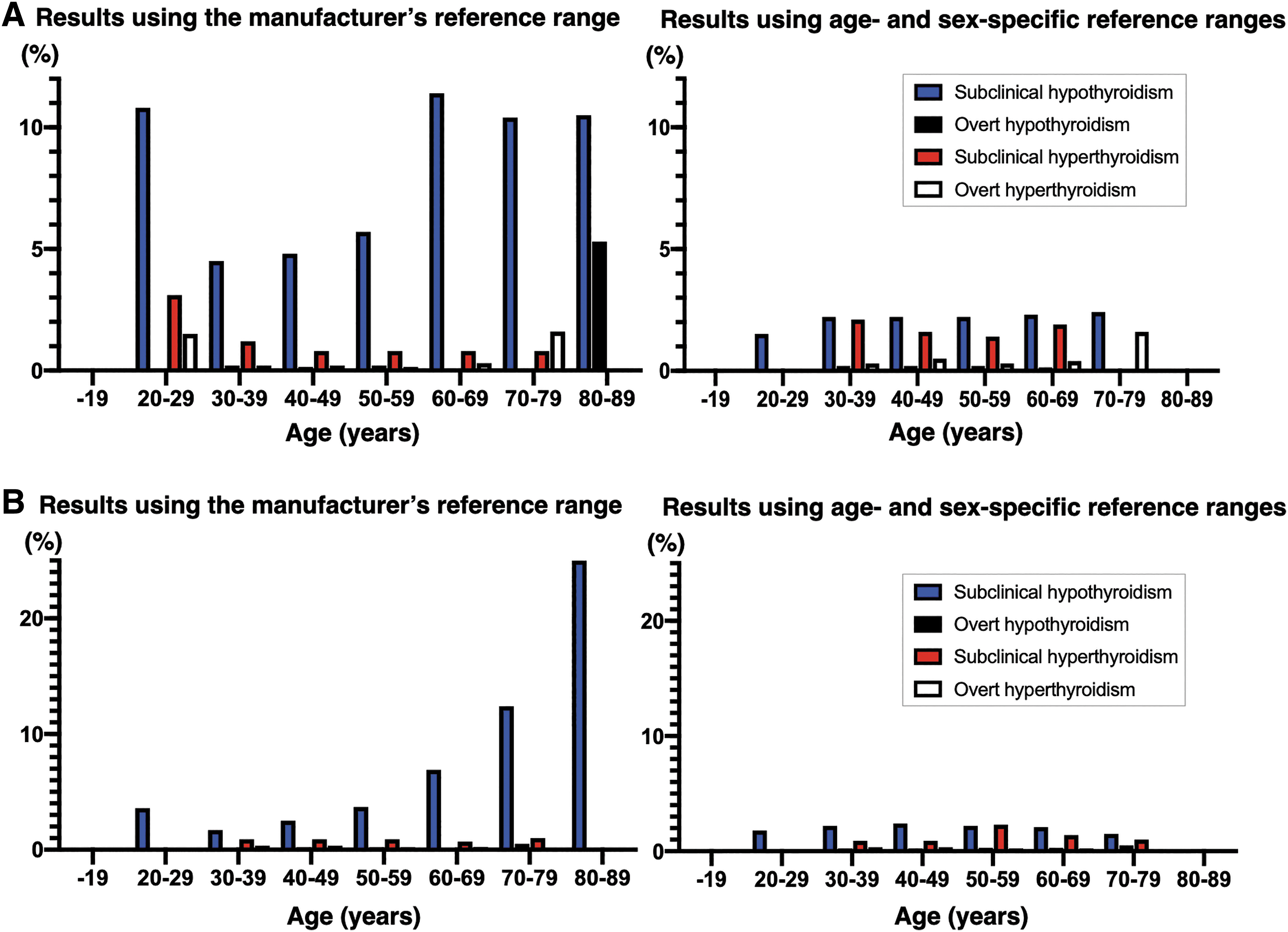
Tables 3 to 6, and Figure 2A and B show thyroid dysfunction prevalence according to the manufacturer's and age-/sex-specific reference ranges. Table 7 shows the percentage of patients with normal thyroid function using age- and sex-specific values who were classified as having subclinical hypothyroidism using Siemens kits and the manufacturer's recommended normal reference range.
Prevalence of Thyroid Dysfunction Using the Manufacturer's Reference Range with Siemens Kits in Women
No. of others indicates patients without subclinical or overt hypothyroidism/hyperthyroidism.
Prevalence of Thyroid Dysfunction Using the Age- and Sex-Specific Reference Range with Siemens Kits in Women
No. of others indicates patients without subclinical or overt hypothyroidism/hyperthyroidism.
Prevalence of Thyroid Dysfunction Using the Manufacturer's Reference Range with Siemens Kits in Men
No. of others indicates the number of patients without subclinical or overt hypothyroidism/hyperthyroidism.
NA, not applicable.
Prevalence of Thyroid Dysfunction Using the Age- and Sex-Specific Reference Range with Siemens Kits in Men
No. of others indicates the number of patients without subclinical or overt hypothyroidism/hyperthyroidism.
Percentage of Individuals Who Were Diagnosed with Subclinical Hypothyroidism Based on the Manufacturer's Reference Range and Reclassified as Normal According to Age- and Sex-Specific Reference Range
Particularly, in women, a substantial portion of individuals were overdiagnosed using the manufacturer's constant reference range instead of age- and sex-specific reference ranges. Among patients aged 30–39 years, ∼50% of those classified as having subclinical hypothyroidism using the manufacturer's recommended reference range were reassessed as having normal thyroid function when age- and sex-specific reference ranges were applied. The percentage of patients overdiagnosed increased with age: 78% of women aged 60–69 years who were classified as having subclinical hypothyroidism using the manufacturer's recommended reference range were reassessed as having normal thyroid function when the age- and sex-specific reference range was applied.
In contrast to women, among men aged 30–39 years, no patients were overdiagnosed. However, a small percentage (5%) of men aged 40–49 years were reclassified as having normal thyroid function when reassessed using the age- and sex-specific reference range. Similar to women, the percentage of men misclassified using the manufacturer's reference range increased with age, and 62% of men aged 60–69 years were reclassified as having normal thyroid function when reassessed using the age- and sex-specific reference range.
Although the percentage was relatively low (i.e., ∼1%) compared with that of overdiagnosis of subclinical hypothyroidism, some participants who were diagnosed as being normal using the manufacturer's recommended reference range were reassessed as having subclinical hyperthyroidism when the age- and sex-specific reference range was applied to women aged 30–69 years and men aged 50–69 years (Table 8).
Percentage of Individuals Who Were Diagnosed with Normal Based on the Manufacturer's Reference Range and Reclassified as Subclinical Hyperthyroidism According to Age- and Sex-Specific Reference Range
Discussion
In this study, we clearly demonstrated changes in serum TSH, fT4, and fT3 levels according to age and sex using assays from three different manufacturers in a relatively large sample of Japanese participants. These data clearly demonstrate the clinical relevance of using age- and sex-specific values, particularly serum TSH levels, when diagnosing subclinical hypothyroidism. We found a high rate of overdiagnosed subclinical hypothyroidism, especially in those aged ≥60 years. Although it is a low rate, patients with subclinical hyperthyroidism were underdiagnosed, particularly in middle-aged men and women.
Other recently published studies have also shown an age-dependent increase in serum TSH levels. 18,19 However, a few studies have investigated differences in serum TSH levels according to sex. 20 –22 The lack of studies on this topic may explain why age- and sex-specific reference ranges have not been used to evaluate thyroid function. Notably, the changes in serum fT4 and fT3 levels differed according to sex. The levels of both hormones were higher in men than in women. The levels gradually decreased with age in men but showed little variation with age in women. In addition, Haddow et al. 23 reported the importance of thyroid function during pregnancy, particularly during the first trimester, for the future neurocognitive development of their children and suggested that the optimal serum TSH level is <2.5 mIU/L in the 2011 American Thyroid Association (ATA) guidelines. 24 In recent guidelines published in 2017, this recommendation was changed to the use of the patient's own reference range during pregnancy in a hospital. 25 These considerations make it necessary to change the reference ranges used depending on sex and pregnancy status.
The prevalence of subclinical hypothyroidism and hyperthyroidism depends on the definition of the reference ranges of serum TSH and fT4 levels. However, most previous studies regarding the prevalence of subclinical thyroid dysfunction have used uniform reference ranges 26 –29 (Table 9).
Summary of Studies on the Prevalence of Subclinical Thyroid Dysfunction
CLEIA, chemiluminescence enzyme immunoassay; CLIA, chemiluminescence immunoassay; EIA, enzyme immunoassay; RERF, Radiation Effects Research Foundation; RIA, radioimmunoassay; SH, subclinical hypothyroidism; SHyper, subclinical hyperthyroidism; T3, triiodothyronine; T4, thyroxine.
In addition, several studies have investigated the effects of subclinical thyroid dysfunction on lipid metabolism, osteoporosis, cognitive mental diseases, and medications, including the use of levothyroxine-Na, antithyroid medications, or radioactive iodine radiation therapy to normalize TH levels, 4 –14 but these results remain controversial. Some studies have focused specifically on the elderly. Surks et al. 18 and Canaris et al. 26 reported a significant increase in the rate of subclinical hypothyroidism according to age. Stott et al. 7 reported that levothyroxine was not beneficial in treatment of subclinical hypothyroidism in older adults. The ATA and European Thyroid Association have stated that it may not be necessary to use levothyroxine to treat patients with subclinical hypothyroidism because of the lack of evidence of a beneficial effect. 30,31 Furthermore, an association between levothyroxine use and mortality in patients with subclinical hypothyroidism was observed in a systematic review and meta-analysis, such that the authors concluded that therapy was effective only for younger individuals aged <65–70 years. 10 It has also been reported that older adults with slightly high serum TSH levels might have a longer life expectancy. 32,33
All studies already cited used a constant reference range of serum TSH, fT4, and fT3 levels, and most studies did not consider sex and did not show awareness of the need to consider age and sex when drawing conclusions regarding the prevalence of subclinical thyroid dysfunction or the effectiveness of treatment. The discrepancies among these profiled investigations might be partly attributed to the utilization of consistent reference ranges without considering age or sex.
The data from National Health and Nutrition Examination Survey (NHANES)-III 1988–199427 and a report from a single hospital in Japan 34 calculated age- and sex-specific reference ranges of TSH and fT4 values and reported that TSH level was higher in women and elderly participants, and fT4 level was higher in men, which was consistent with this study. In this study, several kits were used to examine the effects of age and sex, including fT3. Notably, different thyroid function test kits showed different degrees of change according to age and sex, although they all showed a similar pattern of change. The recent development of highly sensitive hormone assays necessitates accounting for factors such as age, sex, and the specific kit used for the measurement, to accurately evaluate thyroid function (especially subclinical thyroid dysfunction).
Importantly, when using the 2.5th–97.5th percentile values in each decade of life and sex as the reference range, many patients who were classified as having subclinical hypothyroidism using the manufacturer's reference range had normal thyroid function (Table 7), particularly older adults and women. The results demonstrate that many patients were overdiagnosed with subclinical hypothyroidism using the manufacturers' reference ranges, particularly older adults. In addition, although at a relative low rate, some individuals with subclinical hyperthyroidism were reassessed. Therefore, the conclusions of previous studies regarding subclinical thyroid dysfunction may differ if age- and sex-specific reference ranges are used.
This study has several limitations. First, the number of participants aged <30 and ≥70 years was insufficient to determine definitive age-specific reference ranges. Second, this study included participants undergoing health check-ups (employees in companies and privately insured individuals); therefore, the participants were not representative of the general population and there is some potential bias relating to their socioeconomic status. Third, there is potential referral bias in the Okamoto Thyroid Clinic population, which may have influenced the Tosoh subgroup results. Fourth, ethnicity may influence serum TSH and TH levels and each population is evaluated using the local reference range. 27 However, in this study, >95% of the participants were Japanese and, therefore, the effects of race and place of residence are likely to have been minimal. Fifth, because this study was performed in Japan, which is an iodine-sufficient country, the conditions of iodine sufficiency in the country should be considered. Our findings should, therefore, be validated in future studies including other racial and ethnic groups, as the prevalence of autoimmune disease may differ according to ethnicity and geographic location.
Conclusions
This study clearly demonstrates a need for age- and sex-specific reference ranges of serum TSH, fT4, and fT3 levels. These should be considered to accurately assess thyroid function in clinical practice, particularly when diagnosing subclinical hypothyroidism and hyperthyroidism, to avoid over- and underdiagnosis and appropriate therapies. In particular, the high rate of overdiagnosed subclinical hypothyroidism in those aged ≥60 years should be considered. Finally, we should consider the used kits for diagnosis of thyroid function in a hospital as well as their characteristics.
Footnotes
Acknowledgments
We thank all the patients who participated in this study.
Authors' Contributions
M.Y., S.Y., and K.H. designed the trial protocol and applied for research grants. M.A., T.A., Y.A., and Y.O. coordinated the trial. M.A., K.S., E.Y., A.O., I.K., Y.S., Y.O., T.A., and Y.A. recruited participants. S.Y. and E.Y. performed statistical analyses. Y.O., K.S., and M.A. accessed and verified the data. M.Y. and S.Y. interpreted the data and wrote the article. All authors revised the article and approved the final submitted version.
Author Disclosure Statement
The authors have no actual or potential conflicts of interest to disclose.
Funding Information
This research received no grant from any agency in the public, commercial, or not-for-profit sectors.