
Abstract
Background:
The thyroid ultrasound examination (TUE) program was initiated among the residents of Fukushima Prefecture aged ≤18 years at the time of the Fukushima Dai-ichi Nuclear Power Plant accident. In this program, fine needle aspiration cytology (FNAC) was performed only in cases that conformed to the Japanese guidelines for the management of thyroid nodules. To analyze the suitability of the protocol in the TUE, we analyzed the implementation rate of FNAC and the detection rate of thyroid malignancy.
Methods:
There were 299,939 and 269,659 voluntary participants in the Preliminarily Baseline Survey (PLBS), first-round survey, and the first Full-scale Survey (FSS), second-round survey, of the TUE, respectively. FNAC is recommended for nodules with diameters 5.1–10.0 mm showing sonographic characteristics that are strongly suspicious for thyroid carcinoma; diameters 10.1–20.0 mm with characteristics that are suspicious for carcinoma; and all nodules with diameters >20 mm.
Results:
In the PLBS and the first FSS, 1362 and 1382 cases with thyroid nodules sized ≥5.1 mm in diameter were found, respectively. The implementation rates of FNAC in the PLBS were 20.1%, 63.2%, and 87.7% of subjects with nodules sized 5.1–10.0, 10.1–20.0, and ≥20.1 mm in diameter, respectively. In the first FSS, the FNAC implementation rates were 7.3%, 26.0%, and 50.0% in the subjects with nodules with diameters 5.1–10.0, 10.1–20.0, and ≥20.1 mm, respectively. In the subjects who underwent FNAC, the detection rates of malignant and suspected malignant nodules were 21.4% and 34.1% in the PLBS and first FSS, respectively. In the first FSS, malignant or suspected malignant nodules were found in 0.63% and 0.40% of subjects who had nodules of diameters ≤5.0 mm and 5.1–10.0 mm in the PLBS, respectively. In contrast, in the subjects with nodules measuring ≥10.0 mm in diameter in the PLBS, no malignancies were detected.
Conclusions:
The use of a protocol that conformed to the Japanese guidelines led to a reduction in the FNAC implementation rate and an increase in the malignancy detection rate in smaller nodules. In addition, the use of this strategy enabled us to avoid detection failure of thyroid carcinomas >10.0 mm.
Introduction
The pathological characteristics of thyroid cancer in children and adolescents are similar to those in adults. Papillary thyroid carcinoma (PTC) accounts for ≥90% of all childhood cases (1 –3). However, follicular thyroid carcinoma, medullary thyroid carcinoma (MTC), poorly differentiated thyroid carcinoma (PDTC), and anaplastic thyroid carcinomas are rare in young patients (1). Pediatric PTC may present as classic-type PTC or as a variety of histological variants such as solid (4), follicular (5), and diffuse sclerosing (6). Clinical features unique to thyroid cancer in children, adolescents, and young adults include higher survival rate (7,8), faster tumor growth rates (9 –11), and higher metastatic frequency (12) as compared with those in adults.
Childhood thyroid carcinoma was of great concern in Fukushima Prefecture, and anxiety regarding thyroid carcinoma was noteworthy, especially in the residents of Fukushima as previous studies had reported that one of the main adverse health effects of radiation fallout from nuclear power plant (NPP) accidents, specifically the Chernobyl NPP accident, had been a substantial rise in thyroid cancer among young people exposed to radiation (13 –15). Even though the radiation exposure levels of Fukushima residents were considered to be much lower than those of Chernobyl residents (16), surveys had to be conducted to fulfill both scientific and social concerns (17). Seven months after the Fukushima Dai-ichi NPP accident, the Fukushima prefectural government started conducting ultrasound thyroid examinations among residents aged ≤18 years as part of the Fukushima Health Management Survey (FHMS) (17 –19). The Preliminarily Baseline Survey (PLBS) and the first Full-scale Survey (FSS), also known as the first- and second-round surveys, of the thyroid ultrasound examination (TUE) program, were conducted from October 2011 to March 2014 and from April 2014 to March 2016, respectively. After the subsequent secondary confirmatory examinations in participants with thyroid nodules, 116 and 71 cases were interpreted to be malignant or suspicious for malignancy in the PLBS and the first FSS (20). Most of the patients who had an operation were found to have PTC (20).
The number of PTC cases has recently increased due to the improvement and widespread use of diagnostic imaging techniques in adults (21). It was reported that incidental detections on ultrasounds and computed tomographic scans that were ordered for other reasons might result in the overdiagnosis of thyroid cancer (22). In Japan, the risk of overdiagnosis of low-risk thyroid cancer has been reported since the 1990s, and guidelines for nonsurgical follow-up (active surveillance) (23) and fine needle aspiration cytology (FNAC) have been developed (24). In the TUE program, FNAC was performed if sonographic findings of nodules or cysts met the FNAC criteria in the Japanese guidelines (24). Here, we report the implementation rate of FNAC and the detection rate of thyroid malignancy and discuss the suitability of the diagnostic strategy in the TUE program.
Methods
Subjects of the TUE program
The target population for the PLBS of the TUE program comprised all inhabitants aged 0–18 years on April 1, 2011 in Fukushima Prefecture (17,19). The PLBS was conducted from October 2011 through March 2014 as part of the FHMS, and it was extended to April 2015 to provide an opportunity for nonparticipants to undergo the examination (17,19). The PLBS included 299,939 examinees, including evacuees currently living in other prefectures, who voluntarily participated in the survey. The ages of the examinees at the time of the earthquake ranged from 0 to 18 years, and their ages at examination ranged from 0 to 23 years.
The target population for the first FSS were all inhabitants aged 0–19 years on April 1, 2012 in Fukushima Prefecture, regardless of the results of the PLBS (20,24). The first FSS was conducted from April 2014 through March 2016 (20,24). The number of subjects in the first FSS was 269,659, including evacuees currently living in other prefectures who volunteered to participate in the survey. The ages of these subjects at examination ranged from 2 to 25 years. The number of subjects who participated in both the PLBS and the first FSS was 246,687.
The primary examination of TUE
The methods of the primary examination have been previously described (18,19,24), and the protocol is summarized in Figure 1. First, the invitation letter for the primary examination was mailed to the subjects' homes. After obtaining written consent for the TUE by mail, the appointments for the primary examination were arranged. Ultrasound examinations of the thyroid glands were performed mainly in schools, public facilities, and medical institutions. Interpretations of the primary examinations were categorized as Judgments A (A1, A2), B, and C (Table 1). Judgment A1 indicated the absence of thyroid nodules or cysts, and judgment A2 indicated the presence of a nodule sized ≤5.0 mm or/and a cyst measuring ≤20.0 mm in diameter. Judgment B indicated the presence of a nodule measuring ≥5.1 mm or/and a cyst measuring ≥20.1 mm in diameter. Judgment C indicated the presence of a very large suspicious thyroid nodule, an overt extrathyroidal extension, or a large metastatic lymph node, which required immediate examination. Participants categorized under Judgments B and C were encouraged to undergo the secondary confirmatory examination.
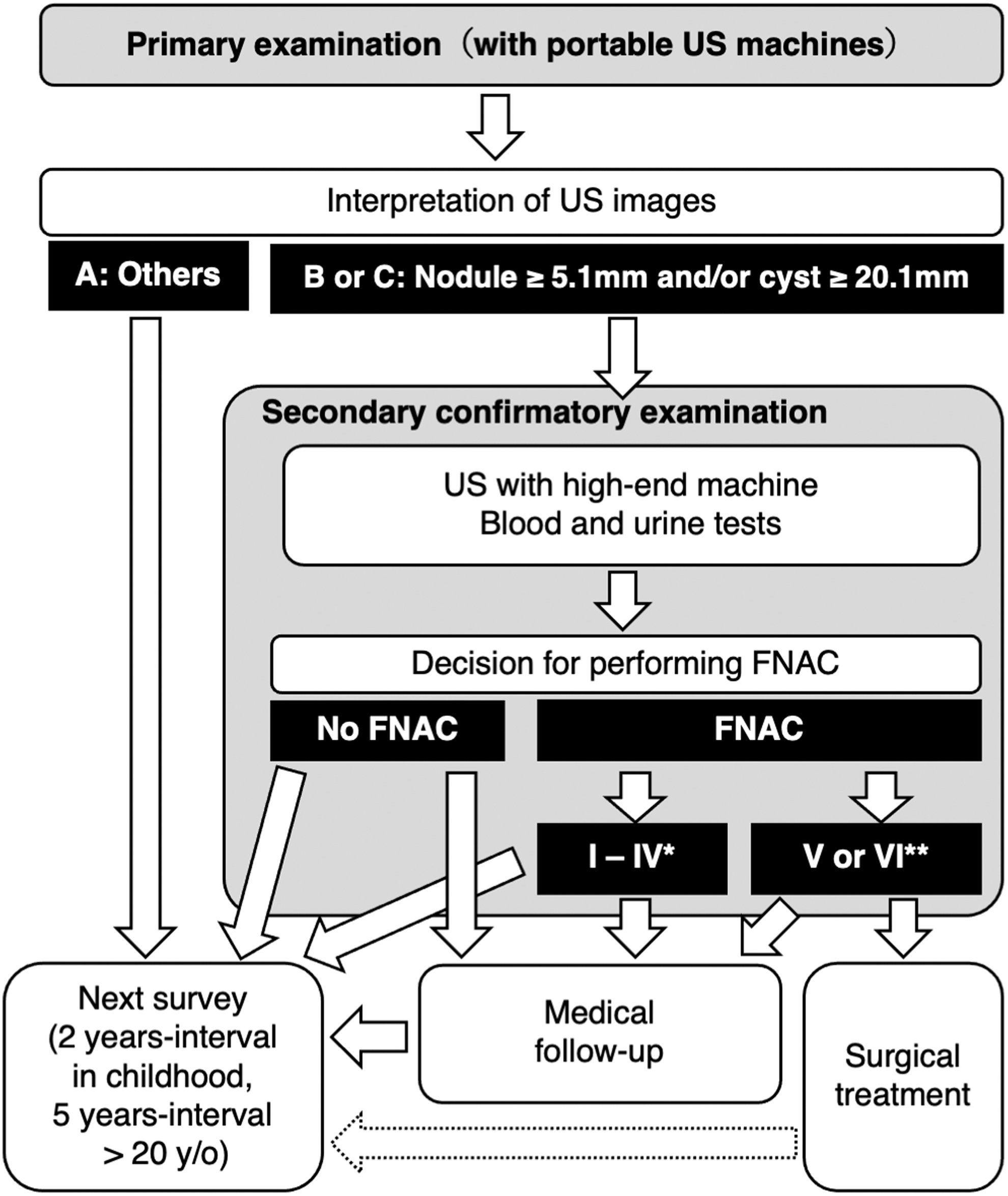
Flowchart of the TUE program. Judgment B means a nodule measuring ≥5.1 mm and/or a cyst measuring ≥20.1 mm in diameter. Category C required immediate secondary examination due to a large suspicious thyroid nodule or large suspicious regional lymph nodes. * Cytologic diagnostic categories I, II, III, and IV in the Bethesda System. ** Cytologic diagnostic categories V and VI, Suspicious for Malignancy and Malignant, in the Bethesda System. FNAC, fine needle aspiration cytology; TUE, thyroid ultrasound examination; US, ultrasonography.
Characteristics of Examinees in This Study
If multiple nodules were found in the secondary confirmatory examination, the size of the nodule that was the subject of the FNAC implementation decision was measured.
FNAC, fine needle aspiration cytology.
The secondary confirmatory examination of TUE
The subjects with nodules measuring ≥5.1 mm or cysts measuring ≥20.1 mm in diameter were recommended a secondary confirmatory examination. This examination included a precise ultrasound examination and blood and urine tests. The blood examinations measured the levels of TSH (thyrotropin), free T3 (triiodothyronine), free T4 (thyroxine), thyroglobulin, anti-thyroperoxidase antibody, and anti-thyroglobulin antibody, and the urinalysis measured the urinary iodine concentration. FNAC was also performed in the secondary confirmatory examination if the sonographic findings of nodules or cysts met the FNAC criteria according to the guidelines issued by the Japan Association of Breast and Thyroid Sonology (JABTS) (24,25). These guidelines for the FNAC criteria were based on the ultrasound diagnostic criteria for thyroid nodule published by the Japan Society of Ultrasonics in Medicine (JSUM), in which the primary findings indicating malignancy were irregular shape, the presence of an ill-defined nodule with a jagged border, and a low and heterogeneous internal echo level. The secondary findings indicating malignancy were fine strong echoes and a heterogeneous marginal hypoechoic zone (14). With respect to blood examinations, thyroid function tests were performed to evaluate the feasibility of FNAC, and FNAC was not performed in cases with overt thyrotoxicosis.
To avoid unnecessary cytological diagnoses of low-risk thyroid carcinomas, FNAC was recommended for nodules measuring 5.1–10.0 mm in diameter that were strongly suspicious for thyroid carcinoma according to the JSUM diagnostic criteria, that is, when most of the malignant sonographic findings were observed (Fig. 2) (24). FNAC was also recommended for nodules sized 10.1–20.0 mm in diameter that were suspicious for carcinoma according to the criteria described earlier, that is, when some of the malignant sonographic findings were observed (Fig. 2) (24). All the nodules sized >20 mm in diameter, nodules showing spongiform patterns, and all cystic lesions measuring more than 20 mm in diameter were subjected to FNAC (Fig. 2). Although nodules measuring <5.1 mm in diameter were not recommended for FNAC, subjects with obvious cervical lymph node metastases, family history of MTC, histories of treatment for high-risk thyroid cancer, or any symptoms indicating cervical extension of thyroid cancer were recommended for FNAC. In all the cases, the examinees and their guardians were able to choose options other than those recommended via a shared decision-making process. Cytological interpretations were reported by using the Bethesda System (26).
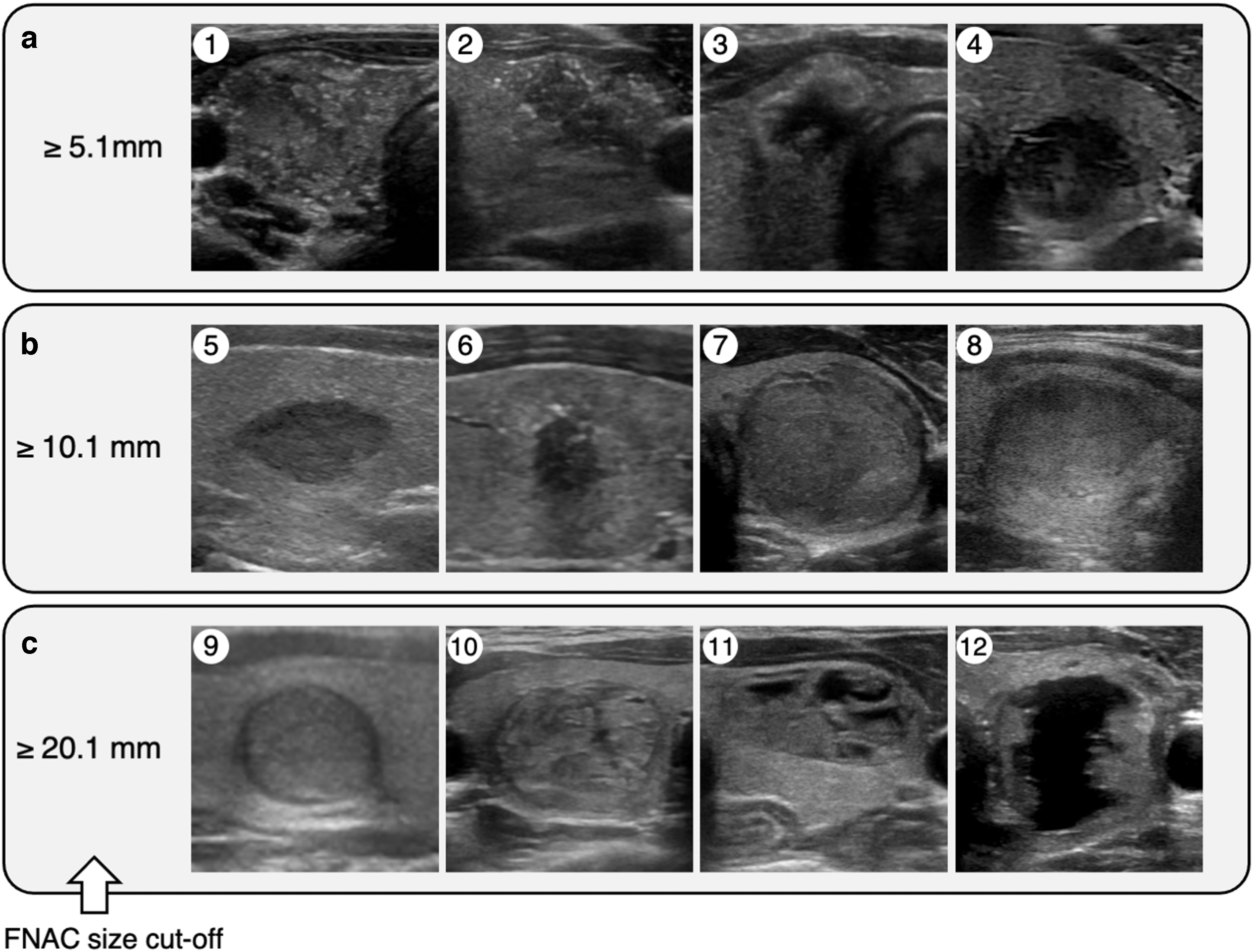
Cutoff sizes of nodule for FNAC and corresponding representative ultrasound images. (
If a benign lesion was detected, either solely by ultrasonography or by ultrasonography and FNAC, the subjects were recommended to undergo a medical follow-up under Japan's comprehensive medical coverage program (Fig. 1). If a malignancy was suspected or detected by FNAC, surgical treatment or medical follow-up was considered under the management guidelines of thyroid cancer issued by the Japan Association of Endocrine Surgery (27).
Statistical analyses
A dataset fixed on December 31, 2018 was used in this study. The results were tabulated by using nodule size, sex, and age at the time of the primary examination instead of age at the time of the 2011 disaster. The sizes of the nodules were assessed at both the primary and secondary confirmatory examinations. The FNAC implementation rate was calculated with the number of subjects who underwent FNAC and those who had thyroid nodules confirmed in the secondary confirmatory examination. Chi-square analyses were performed with JMP 14.3.0 software (SAS Institute, Cary, NC). p-Values <0.05 were considered statistically significant.
This survey was approved by the ethics review committee of Fukushima Medical University (No. 1318). Written informed consent was obtained from the parents or guardians of all the surveyed children.
Results
Characteristics of subjects in this study
In the primary examination, thyroid nodules were found in 3078 (1.33% of the subjects) and 3780 (1.40%) participants in the PLBS and the first FSS, respectively (Table 1). The majority of the nodules measured <10.1 mm, and the median thyroid nodule diameters were 5.6 and 5.7 mm in the PLBS and the first FSS, respectively (Table 1).
In the PLBS and the first FSS, 2089 and 1829 participants who had nodules sized ≥5.1 mm or cysts sized ≥20.1 mm were recommended to undergo secondary confirmatory examinations, and 1489 and 1517 subjects were confirmed to have thyroid nodules, respectively (Table 1). In both the rounds, thyroid nodules were predominantly observed in female subjects, and the median age of the subjects with thyroid nodules was 17 years. The most frequently measured size was 5.1–10.0 mm in both the rounds, and the median thyroid nodule diameters were 8.5 and 8.1 mm in the PLBS and the first FSS, respectively (Table 1). In the secondary examination, the ratio of examinees with nodules measuring ≤5.0 mm in diameter was relatively low because the examinees having nodules ≤5.0 mm were identified in the primary examination and excluded. These examinees were those who had nodules measuring ≥5.1 mm in the primary examination and whose nodules were found to be ≤5.0 mm in the secondary examination.
Implementation rate of FNAC
The FNAC implementation rates in the PLBS and the first FSS were 36.3% and 13.7%, respectively (Table 2). Similar implementation rates were observed in male and female subjects in both the rounds (p > 0.05). When subjects with thyroid nodules in the secondary confirmatory examination were divided into five age groups according to their ages at the primary examination, FNAC was most frequently performed in the groups aged 10–14 and 15–19 years in both the rounds. The categorization of thyroid nodules by maximal size at the secondary confirmatory examination showed that FNAC was performed in 1.6% (n = 2), 20.1% (n = 164), 63.2% (n = 275), and 87.7% (n = 100) of the subjects with nodules sized ≤5.0, 5.1–10.0, 10.1–20.0, and ≥20.1 mm in diameter, respectively, in the PLBS. In the first FSS, the FNAC implementation rates were 0.0% (n = 0), 7.3% (n = 66), 326.0% (n = 107), and 50.0% (n = 34) in subjects with nodules sized ≤5.0, 5.1–10.0, 10.1–20.0, and ≥20.1 mm in diameter, respectively. These results indicate that FNAC implementation rates with respect to smaller nodules were limited in this program.
Fine Needle Aspiration Cytology Implementation Rate in the Preliminary Baseline Survey and First Full-Scale Survey
Number of subjects with thyroid nodules confirmed at the secondary confirmatory examination.
Number of subjects who received FNAC at the secondary confirmatory examination.
Age at the primary examination.
Maximal sizes of nodules measured at the secondary confirmatory examination. When multiple nodules were observed, the nodules that were subjected to evaluation of sonographic findings to assess the necessity of FNAC were selected.
Detection rate of malignant cases
In the PLBS and the first FSS, there were 116 and 71 subjects whose nodules were interpreted as malignant or suspicious for malignancy, respectively, via the Bethesda System (Table 3). To the best of our knowledge, 102 examinees of the PLBS underwent thyroidectomy, of which 100 were pathologically diagnosed with PTC; 1 PDTC; and 1 benign tumor. In the first FSS, 54 examinees underwent thyroidectomy, of which 53 were pathologically diagnosed with PTC, and one was diagnosed with an unclassified type of thyroid cancer. The detection rate of malignant or suspicious for malignancy cases was 7.8% among all the subjects with thyroid nodules detected in the secondary confirmatory examination and that among the cases in whom FNAC was performed was 21.4% in the PLBS. Of the 116 examinees with thyroid nodules diagnosed with malignant or suspicious for malignancy in the PLBS, only 21 examinees underwent the primary examinations, and no additional malignant nodules were found in these examinees in the first FSS. Although the detection rate of thyroid nodules cytologically diagnosed as malignant or suspicious for malignancy was lower in the first FSS than that in the PLBS, the detection rate of malignant cases in the FNAC-performed cases was higher than that in the PLBS.
Detection Rate of Malignancy in the Preliminary Baseline Survey and First Full-Scale Survey
Number of subjects with thyroid nodules confirmed at the secondary confirmatory examination.
Number of subjects in whom FNAC was performed at the secondary confirmatory examination.
Number of subjects whose nodules were interpreted as malignant or suspicious for malignancy by FNAC.
Detection rate of cases that were interpreted as malignant or suspicious for malignancy by FNAC in subjects whose thyroid nodules were confirmed at the secondary confirmatory examination.
Detection rate of cases whose nodules were interpreted as malignant or suspicious for malignancy by FNAC in FNAC-performed cases.
Age at the time of the primary examination.
Maximal sizes of nodules measured at the secondary confirmatory examination. When multiple nodules were observed, the nodules that were subjected to evaluation of sonographic findings to assess the necessity of FNAC were selected.
Similar detection rates were observed in male and female subjects in the PLBS in subjects with thyroid nodules as well as in the cases that underwent FNAC cases. However, the detection rate of malignancy in subjects with thyroid nodules was significantly higher in male subjects (p < 0.05). In the subjects who underwent FNAC, the detection rate of malignancy in males was also higher than that in females, but the difference was not significant. When the subjects with thyroid nodules in the secondary confirmatory examination were divided into five age groups according to their ages at the primary examination, the detection rates of malignant cases in the subjects with nodules or in those who underwent FNAC were higher in the groups with examinees aged 15–19 and ≥20 years in the PLBS. There were similar tendencies in the first FSS, except in the group aged 5–9 years, in which this rate was unreliable because of the limited number of cases with thyroid nodules.
The categorization of thyroid nodules into four groups according to maximal size at the secondary confirmatory examination showed that the detection rate of malignant cases in subjects with thyroid nodules was the highest in the ≥20.1-mm group. However, the highest detection rate of those in the FNAC-performed subjects was observed in the 5.1- to 10.0-mm group. A similar tendency was also observed in the first FSS. These results indicate that the restricted performance of FNAC increased the detection rate of malignancy in subjects with smaller nodules who underwent FNAC.
Accuracy of the guideline-based FNAC
To investigate the accuracy of the guideline-based management of thyroid nodules that we employed for the TUE program, we divided the 245,719 subjects, who participated in both the PLBS and the first FSS, into five groups according to nodular size based on the results of the primary examination in the PLBS. Further, the detection rate of malignant cases found in the first FSS was determined (Fig. 3). In these subjects, the nodules in 70 examinees were diagnosed as malignant or suspicious for malignancy. In the first FSS, malignant nodules were found in 58 (0.02%) subjects with no nodule detected in the PLBS. Higher detection rates, 0.63% (n = 8) and 0.40% (n = 4), were observed in the subjects with ≤5 and 5.1–10.0 mm-sized nodules in the primary examination of the PLBS, respectively. On the other hand, no malignant cases were found in the subjects with nodules larger than 10.0 mm in the primary examination of the PLBS.
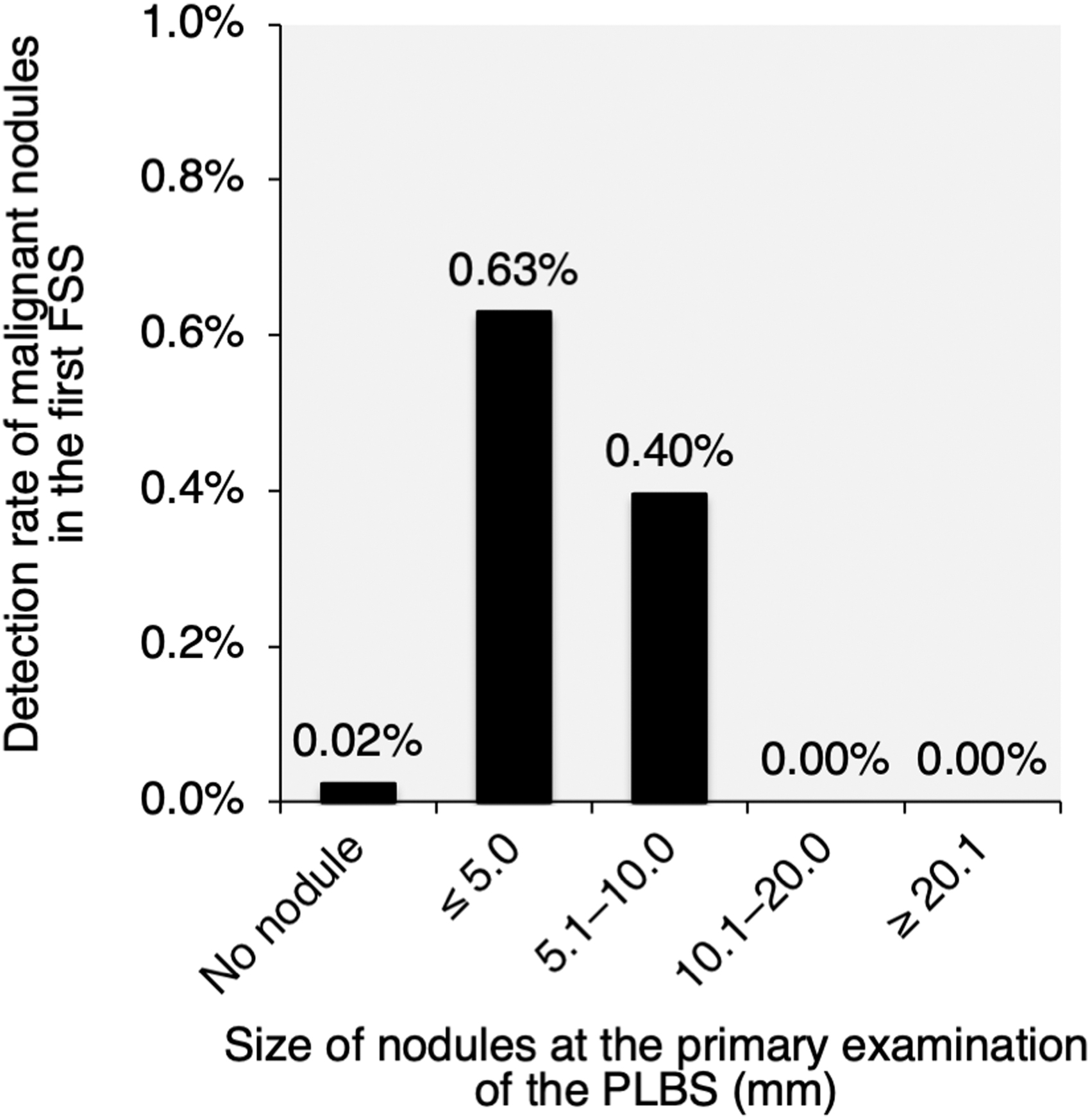
Detection rate of malignant nodules in the first FSS in each group categorized by the size of nodules at the PLBS. In total, 245,719 subjects, who participated in both the PLBS and the first FSS, were categorized into 5 groups based on the results of the primary examination in the PLBS. The detection rate of malignant cases found in the first FSS in each group is shown. FSS, Full-scale Survey; PLBS, Preliminarily Baseline Survey.
Discussion
In recent years, the incidence rate of thyroid cancer, especially small PTC, has been rapidly increasing worldwide (21). Davis et al. reported that 49% of thyroid cancers measured <10 mm in diameter in the United States; however, they also reported a 2.9-fold increase in papillary cancer in the United States between 1988 and 2002 (28). Further, Du et al. reported that 94.9% of the thyroid cancers diagnosed between 1972 and 2014 were papillary cancers, of which those measuring <10 mm accounted for 70.4% (29). It has been interpreted that this might be due to the prevalence and improved accuracy of imaging modalities such as ultrasonography. To cope with the recent advancements, FNAC implementation guidelines have been published by each country. The management guidelines for thyroid nodules employed in the TUE program, detailed in the Methods section, were published in 2012 by JABTS. These guidelines are essentially the same as those published in the United States and Europe for thyroid nodules measuring >10 mm in diameter (30 –34), in which risk classification is recommended based on ultrasound findings. Although these guidelines do not recommend FNAC for nodules measuring <10 mm in diameter, the Japanese guidelines recommend FNAC for nodules sized 5.1–10.0 mm when the sonographic findings are mostly malignant (24). Moreover, the American Thyroid Association (ATA) guidelines additionally state that FNAC can be considered at lower size cutoffs for nodules in which all the ultrasonographic findings indicate malignancy (30).
A few previous reports have shown the implementation rate of FNAC. Lee et al. reported that FNAC was performed in 94.4% of patients with nodules sized <0.5 cm in diameter (35). After the publication of management guidelines for thyroid nodules by the Korean Thyroid Association and the ATA, the percentage of FNAC implementation had decreased to 53.5% and 80.2% for nodules sized <0.5 cm and 0.5–1.0 cm in diameter, respectively (35). Further, Richman et al. reported that FNAC was performed in 102 (31.2%) out of 327 pediatric patients with thyroid nodules based on the American College of Radiology Thyroid Imaging Reporting and Data System (TI-RADS) (36). Although the detection processes of thyroid nodules might be different from those used in our survey, these FNAC implementation rates were higher than those obtained in the current study. Even though various FNAC implementation rates have been reported, an adequate implementation rate to diagnose clinically relevant thyroid cancers without excess or deficiency is yet to be determined.
The guideline-based examination in this survey resulted in a nodule size-dependent implementation rate, which was higher in larger nodules in both the rounds of the TUE program. In the cases of suspected thyroid microcarcinomas, surgical treatments were performed only in subjects who did not choose to undergo medical follow-ups after the shared decision-making process. Suzuki et al. reported that intrathyroidal spread, extrathyroidal extension, and lymph node metastasis were observed in 48.7%, 42.1%, and 80.0% of cases with PTC, respectively, by the pathological assessment of dissected PTC (37). These results suggest that the diagnostic strategies in the TUE program played roles in the diagnosis of clinically relevant thyroid cancers.
There was a difference in the implementation rates of FNAC between the PLBS and the first FSS. A proportion of this difference might be due to two reasons. First, 123 examinees who had undergone FNACs for their thyroid nodules in the PLBS revisited in the first FSS; among them, FNAC was not recommended in 115 participants since their thyroid nodules were interpreted as nonmalignant, and the size and sonographic appearances had not apparently changed. Another reason for the difference in the implementation rates was anxiety regarding the health effects of radiation exposure. Risk perception of later health effects of radiation exposure, such as thyroid cancer or genetic effects, was high in the first three years after the earthquake, and it was the highest in 2011 (38). Since FNAC was performed through shared decision-making processes, we speculated that the implementation rate of FNAC might have been heightened by the anxieties of the examinees and their guardians.
The adequacy of the management of thyroid nodules according to guidelines, including FNAC implementation criteria, is still under discussion (39). Excessively low implementation rates might result in failures in the detection of high-risk thyroid cancers. To analyze this risk, we evaluated the detection rate of malignant nodules in the first FSS in the subjects who participated in both the PLBS and the first FSS (Fig. 3). Although detection rates of 0.63% and 0.40% were observed in the subjects with ≤5 and 5.1–10.0 mm-sized nodules in the primary examination of the PLBS, respectively, no case with malignancy was found in subjects with nodules sized >10.0 mm in diameter in the primary examination of the PLBS. These results suggest that the protocol of the confirmatory examination according to the Japanese guidelines was able to avoid detection failure of malignant nodules measuring >10 mm in diameter.
The rate of malignancy in the subjects who underwent FNACs was the highest in the 5.1–10.0 mm group (Table 3). This tendency was more evident in the first FSS. This might be attributable to the performance of guideline-based FNAC in this survey. Gupta et al. reported that 22% of pediatric patients (≤18 years) with >1 cm-sized thyroid nodules were diagnosed with thyroid cancer whereas a 5–15% cancer rate was reported in adults (40). This detection rate in children and adolescents was higher than those in the ≥10.1 mm groups in our survey, that is, 13.5% and 7.3% in the PLBS and the first FSS, respectively.
There is limited evidence to reveal the natural history of pediatric thyroid nodules in nonradiated populations. However, similar reports discussing the detection rates of malignant diseases in subjects with thyroid nodules have been published from studies in three prefectures located far away from Fukushima (41,42). In the study in three prefectures, TUEs were carried out with the same ultrasound procedures as those used in the FHMS. The number of subjects analyzed was 4365; they were living in Aomori, Yamanashi, and Nagasaki prefectures, were located far away from Fukushima, and their ages ranged from 3 to 18 years. After thyroid ultrasonography, nodules sized ≥5.1 mm were found in 44 subjects. Further, of these 44 subjects, 31 who provided consent for the follow-up study agreed to undergo the confirmatory examination (43). As a result, one subject was diagnosed with thyroid cancer, and the detection rate of thyroid cancer was 3.3% among the nodules sized ≥5.1 mm. As the number of subjects was extremely small, it is difficult to compare the results with those of this study; however, the results are considered to be comparable.
A limitation of this study was that the pathological diagnoses of all the surgically treated cases were not fully available in the TUE program. To the best of our knowledge, of the 187 examinees diagnosed with malignant or suspected to be malignant nodules, 156 underwent surgery, and 155 cases (99.4% of 156 cases) were pathologically diagnosed with thyroid cancer. Therefore, in this article, cases diagnosed as malignant or suspicious in cytology were regarded as cases with thyroid cancer.
Of those who had undergone both the PLBS and the first FSS, 70 cases were cytologically diagnosed as malignant or suspicious in the first FSS, and 58 of them had no nodules in the PLBS. This result may reveal the rates of thyroid cancer formation in young children. The relationship between the rate of formation of childhood thyroid cancer in Fukushima and radiation exposure could be a major issue. The radiation doses were different between residents who evacuated early after the accident and those who evacuated late or did not evacuate. In the thyroid-absorbed dose estimated by the United Nations Scientific Committee on the Effects of Atomic Radiation (44), the estimated dose in the residents of the municipalities where the NPP was located was lower than that of the surrounding municipalities. Further, it is estimated that the amount of radiation exposure in Fukushima Prefecture varied according to the evacuation route of the evacuees (44). To evaluate the effects of radiation on the thyroid gland in detail, it may be necessary to estimate the absorbed dose to the thyroid gland of each individual from behavioral records. Additional studies, such as case–control studies between the high-dose and low-dose groups in Fukushima Prefecture, may be needed to clarify this issue.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Health Fund for Children and Adults Affected by the Nuclear Incident.