
Abstract
Background:
Some studies reported that among athyreotic patients on levothyroxine (LT4) after total thyroidectomy, patients with normal serum thyrotropin (TSH) levels had mildly low serum free triiodothyronine (fT3) levels, whereas patients with mildly suppressed serum TSH levels had normal serum fT3 levels. The reduction of the thyroid volume (TV) after radioiodine treatment for Graves' disease is well known; however, a few studies evaluated thyroidal function including serum triiodothyronine (T3) levels of hypothyroid patients on LT4 after radioiodine treatment in detail.
Methods:
We retrospectively studied 446 patients treated with LT4 for radioiodine-induced hypothyroidism and who had undergone ultrasonography. We compared serum fT4 and fT3 levels in hypothyroid patients on LT4 who presented an atrophic thyroid change after radioiodine treatment, with those in the euthyroid matched control group with intact thyroids. We also stratified patients with normal TSH levels according to TV and evaluated serum thyroid hormone levels.
Results:
In 356 of 446 (80%) patients, TV was lower than the lower limit of the 95% reference range of controls. Excluding 43 patients with high serum TSH levels, we assessed thyroid function test results in 313 patients with atrophic thyroid glands. Of these cases, eight patients with strongly suppressed TSH levels had serum fT3 levels that were significantly higher than those in controls (p < 0.001). Overall, 27 patients with mildly suppressed TSH levels had serum fT3 levels equivalent to those in controls (p = 0.386), whereas 278 patients with normal TSH levels had serum fT3 levels that were significantly lower than those in controls (p < 0.001). We also assessed fT3 levels relative to TV in 326 patients with normal TSH levels. Of these cases, in 267 patients with TV less than 5 mL and in 46 patients with TV between 5 and 10 mL, serum fT3 levels were significantly lower than those in controls (p < 0.001). In 13 patients with TV more than 10 mL, serum fT3 levels were equivalent to those in controls (p = 0.844).
Conclusions:
Serum thyroid hormone balance in most patients on LT4 after radioiodine treatment for Graves' disease was similar to that in athyreotic patients on LT4. Mild TSH suppression with LT4 is needed to achieve normal fT3 levels in such patients.
Introduction
There are two thyroid hormones, thyroxine (T4) and triiodothyronine (T3). T3 is the biologically active thyroid hormone. In normal subjects, 100% of T4 is secreted by the thyroid, ∼20% of T3 is secreted from the thyroid gland, and ∼80% of T3 is derived from the conversion of T4 to T3 in extra-thyroidal peripheral tissues (1). A relative T3 deficiency may, thus, be present in athyreotic patients during levothyroxine (LT4) monotherapy. We and other investigators (2 –5) compared postoperative T3 levels in patients on LT4 therapy with their own preoperative levels or with those in controls. These studies indicate that in the athyreotic condition after total thyroidectomy during LT4 therapy, patients with normal serum thyrotropin (TSH) levels had mildly low serum free triiodothyronine (fT3) levels, and patients with suppressed serum TSH levels had normal serum fT3 levels.
Radioiodine (131I) is used as the definitive treatment in many patients with Graves' hyperthyroidism. Of the patients who receive radioiodine treatment for Graves' disease, most eventually develop hypothyroidism after radioiodine treatment and require thyroid hormone replacement therapy (6,7). Biological effects of 131I include necrosis and impaired replication of follicular cells, fibrosis, and a chronic inflammatory response, which, ultimately, result in permanent atrophic changes of the thyroid gland (8 –10). Although reduction of the thyroid volume (TV) after radioiodine treatment by using ultrasonography has been reported, a few studies have evaluated thyroidal function including serum T3 levels of hypothyroid patients on LT4 after radioiodine treatment, because patients who had normal serum TSH and fT4 levels were generally considered to have euthyroidism.
In this study, we compared serum fT4 and fT3 levels in hypothyroid patients on LT4 who presented atrophic thyroid changes after radioiodine treatment with those in a healthy control group to evaluate the effect of the reduction of the TV after radioiodine treatment for serum thyroid hormone balance. We also evaluated serum thyroid hormone levels in groups of patients who were stratified according to their TVs.
Materials and Methods
Patients
From their medical records, we identified 446 consecutive patients who had been treated with LT4 for radioiodine-induced hypothyroidism and who had undergone ultrasonography between April 2017 and March 2018 at the Kuma Hospital. Ultrasonography was performed at least 12 months (median 7.90 years) after radioiodine treatment for Graves' disease. The subjects included 359 women and 87 men (aged 53 ± 14 years [mean ± standard deviation]). Thyroid function tests were performed one month after radioiodine treatment and every six months after stabilization. If patients developed hypothyroidism, LT4 was administered and doses were adjusted to provide resolution of patients' symptoms and signs of hypothyroidism or to maintain the patients' serum TSH values within the reference range. Patients with thyroid profiles, including thyroid dysfunction other than Graves' disease such as thyroid dyshormonogenesis, or an autonomous functioning thyroid nodule, were excluded from the study. Patients with thyroid malignancies were also excluded. Patients with serious chronic diseases such as cardiac, pulmonary, hepatic, and renal diseases were not eligible for study participation. We also excluded patients receiving drugs known to affect thyroid function or thyroid hormone metabolism, such as thyroid hormone, steroids, estrogen, amiodarone, lithium, β blockers, sucralfate, and iron or iodine-containing drugs.
Matched control subjects
A continuous series of 3028 subjects (2511 women and 517 men) who were confirmed to have normal thyroid function at the Kuma Hospital during the same period as the test subjects and who did not have clinical or laboratory signs of thyroid diseases served as controls. Subjects with positive anti-thyroid peroxidase or anti-thyroglobulin antibody test results were excluded. Subjects with a thyroidal nodule or a goiter (TV: men ≥20 mL and women ≥18 mL) (11) on an ultrasound examination were also excluded. The other exclusion criteria were the same as those used for the selection of the patients described earlier. We balanced covariates including age, sex, and body mass index (BMI) for choosing the control subjects for each patient group. Control subjects for each group of patients were chosen from among the 3028 subjects selected earlier by 1:1 matching.
This study was approved by the Ethical Committee at Kuma Hospital, and all patients gave informed consent.
Laboratory serum tests
For the patients who were taking LT4, blood samples were obtained in the morning after the ingestion of LT4. The patients' serum levels of TSH, fT4, and fT3 were measured by using a chemiluminescent immunoassay (ARCHTECT i2000; Abbott Japan, Tokyo). The intra-assay coefficients of variation and the inter-assay coefficients of variation were 1.1–5.0% and 1.7–5.3% for the TSH assay, 2.3–5.3% and 3.6–7.8% for the fT4 assay, and 1.4–4.2% and 2.3–5.0% for the fT3 assay, respectively. The reference ranges in our hospital are 0.3–5.0 μIU/mL for TSH, 0.7–1.6 ng/dL for fT4, and 1.7–3.7 pg/mL for fT3. The serum levels of TSH receptor antibodies (TRAbs) were measured by using an electrochemiluminescence immunoassay (ECLusys 2010; Roche Diagnostics Japan, Tokyo; normal range: <1.9 IU/L). The volume of the thyroid gland was measured by ultrasonography as previously reported (12).
Statistical analysis
Grouped data are expressed as the mean ± standard deviation or the median (25th to 75th percentiles). Group comparisons among the three postradioiodine treatment groups were analyzed by unpaired t-tests in case of a normal distribution and by Mann–Whitney U tests in case of a nonparametric distribution; Bonferroni corrections were applied for multiple comparisons. Treatment effects (control vs. patients on LT4 for radioiodine-induced hypothyroidism) were analyzed by using the paired t-test for data with a normal distribution and by the Wilcoxon signed-rank test for data with a nonparametric distribution. Significance was defined as a corresponding p-value <0.05 (two-sided). Statistical analyses were performed by using StatFlex (version 6.0.; Artech Co., Ltd., Osaka, Japan).
Results
The TVs of healthy subjects and patients on LT4 after radioiodine treatment for Graves' hyperthyroidism
The median TV of healthy volunteers was 13.8 mL (6.9–19.5; 95% reference range) for 517 men and 11.0 mL (5.4–17.2; 95% reference range) for 2511 women. The TV after radioiodine treatment was 4.2 mL (1.1–23.1; 95% reference range) for men and 2.8 mL (0.4–14.1; 95% reference range) for women. In 356 of 446 (80%) patients after radioiodine treatment (68 men and 288 women), TVs were lower than the lower limit of the 95% reference range of healthy control subjects, and the thyroid glands showed atrophic changes in most patients.
Characteristics among the three patient groups stratified by serum TSH levels and with an atrophic thyroid gland
In this study, we first examined 313 of 356 patients with atrophic thyroid glands; we excluded 43 patients with high serum TSH levels from this analysis. These 313 patients with atrophic thyroid glands were divided into three groups according to serum TSH levels, as follows: those with TSH less than 0.03 μIU/mL, those with TSH levels between 0.03 and 0.3 μIU/mL, and those with TSH levels between 0.3 and 5 μIU/mL.
Characteristics of the three patient groups are given in Table 1. Age, BMI, TV, total 131I-dose, and TRAb were similar among the groups. Follow-up times from radioiodine treatment to ultrasonography of patients with TSH levels between 0.3 and 5 μIU/mL were significantly longer than those of patients with TSH levels between 0.03 and 0.3 μIU/mL (p < 0.05). Serum fT4 levels of patients with TSH levels between 0.3 and 5 μIU/mL were significantly lower than those of the other two groups (p < 0.01). Serum TSH and fT3 levels of each of the three groups were different from those of each of the other two groups (p < 0.01, and p < 0.05, respectively).
Clinical Characteristics Among the Three Patient Groups with Atrophic Thyroid Glands, Stratified by Serum Thyrotropin Levels
Statistical significance was analyzed by the χ 2 test (sex), unpaired t-test, or *Mann–Whitney U test by using Bonferroni corrections for multiple comparisons. Values are expressed as mean ± standard deviation or median (25th–75th percentiles).
BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; LT4, levothyroxine; TRAb, TSH receptor antibody; TSH, thyrotropin.
Serum thyroid hormone levels in patients with atrophic thyroid glands compared with those of the matched control subjects
In patients with TSH levels less than 0.03 μIU/mL, the serum fT3 levels were significantly higher than those of the matched controls (3.01 [2.91–3.08] vs. 2.62 [2.55–2.67] pg/mL, respectively; p < 0.001) (median [25th to 75th percentiles]). In patients with TSH levels between 0.03 and 0.3 μIU/mL, the serum fT3 levels were equivalent to those of matched controls (2.57 [2.45–2.72] vs. 2.56 [2.32–2.73] pg/mL, p = 0.386). In patients with TSH levels between 0.3 and 5 μIU/mL, the serum fT3 levels were significantly lower than those of matched controls (2.30 [2.08–2.48] vs. 2.46 [2.29–2.73] pg/mL, p < 0.0001) (Fig. 1A).
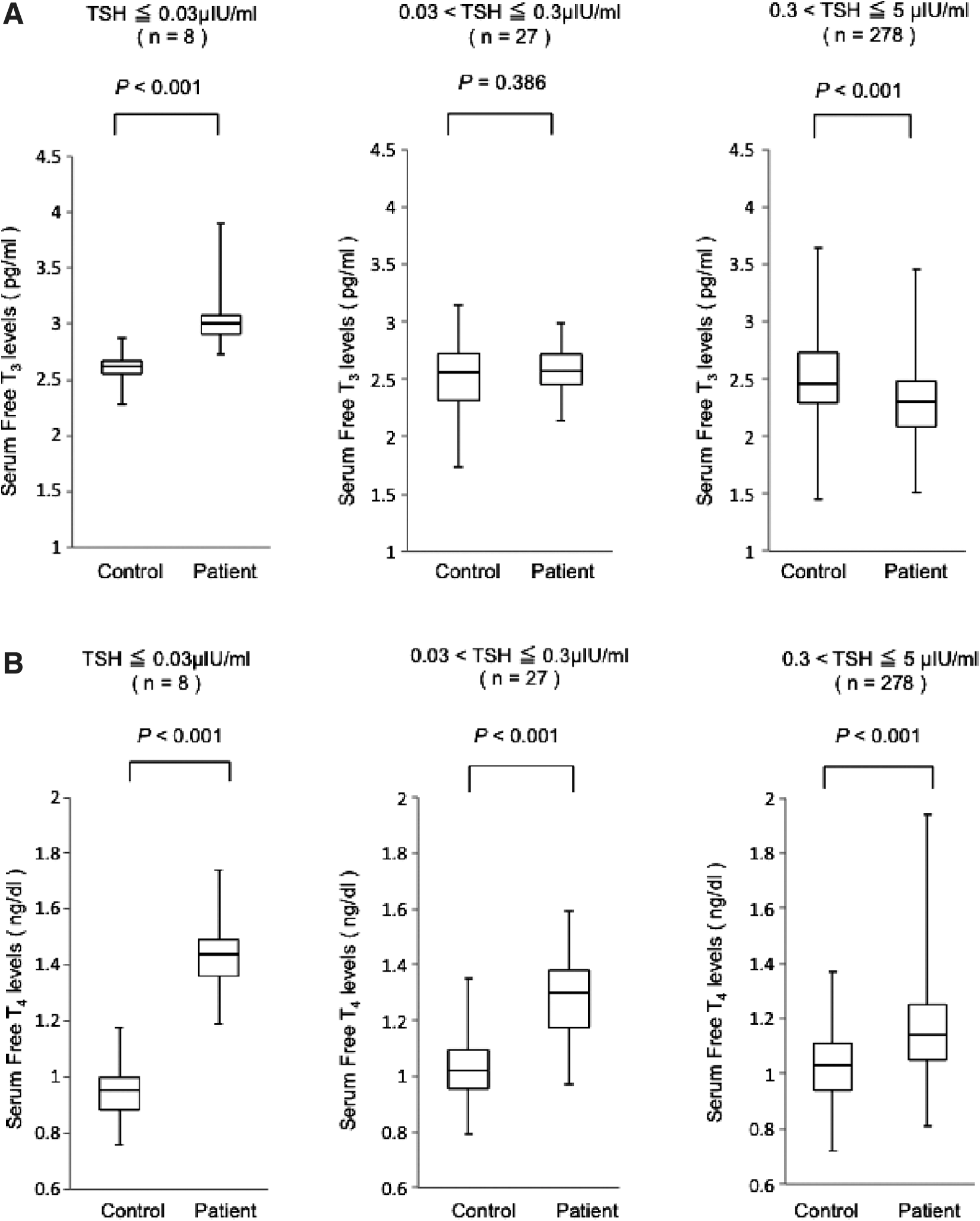
Serum levels of fT3
Serum fT4 levels were significantly higher than those of the matched controls in all three groups (1.44 [1.36–1.49] vs. 0.96 [0.89–1.00] ng/dL, p < 0.001, 1.30 [1.18–1.38] vs. 1.02 [0.96–1.10] ng/dL, p < 0.0001, and 1.14 [1.05–1.25] vs. 1.03 [0.94–1.11] ng/dL, p < 0.0001, respectively). However, the magnitude of increase varied according to the TSH levels (Fig. 1B).
Serum thyroid hormone levels in patients stratified according to TV
In this study, 326 patients had normal serum TSH levels. We also stratified these 326 patients into three groups according to their TVs, as follows: those with TV less than 5 mL, those with TV between 5 and 10 mL, and those with TV more than 10 mL. In 267 patients with TV less than 5 mL, the serum fT3 levels were significantly lower than those of the matched controls (2.29 [2.08–2.47] vs. 2.46 [2.28–2.83] pg/mL, respectively; p < 0.001) (median [25th to 75th percentiles]). In 46 patients with TV between 5 and 10 mL, the serum fT3 levels were significantly lower than those of the controls (2.27 [2.10–2.43] vs. 2.47 [2.32–2.75] pg/mL, p < 0.001). In 13 patients with TV more than 10 mL, the serum fT3 levels were equivalent to those of the matched controls (2.58 [2.33–2.83] vs. 2.48 [2.36–2.74] pg/mL, p = 0.843) (Fig. 2).
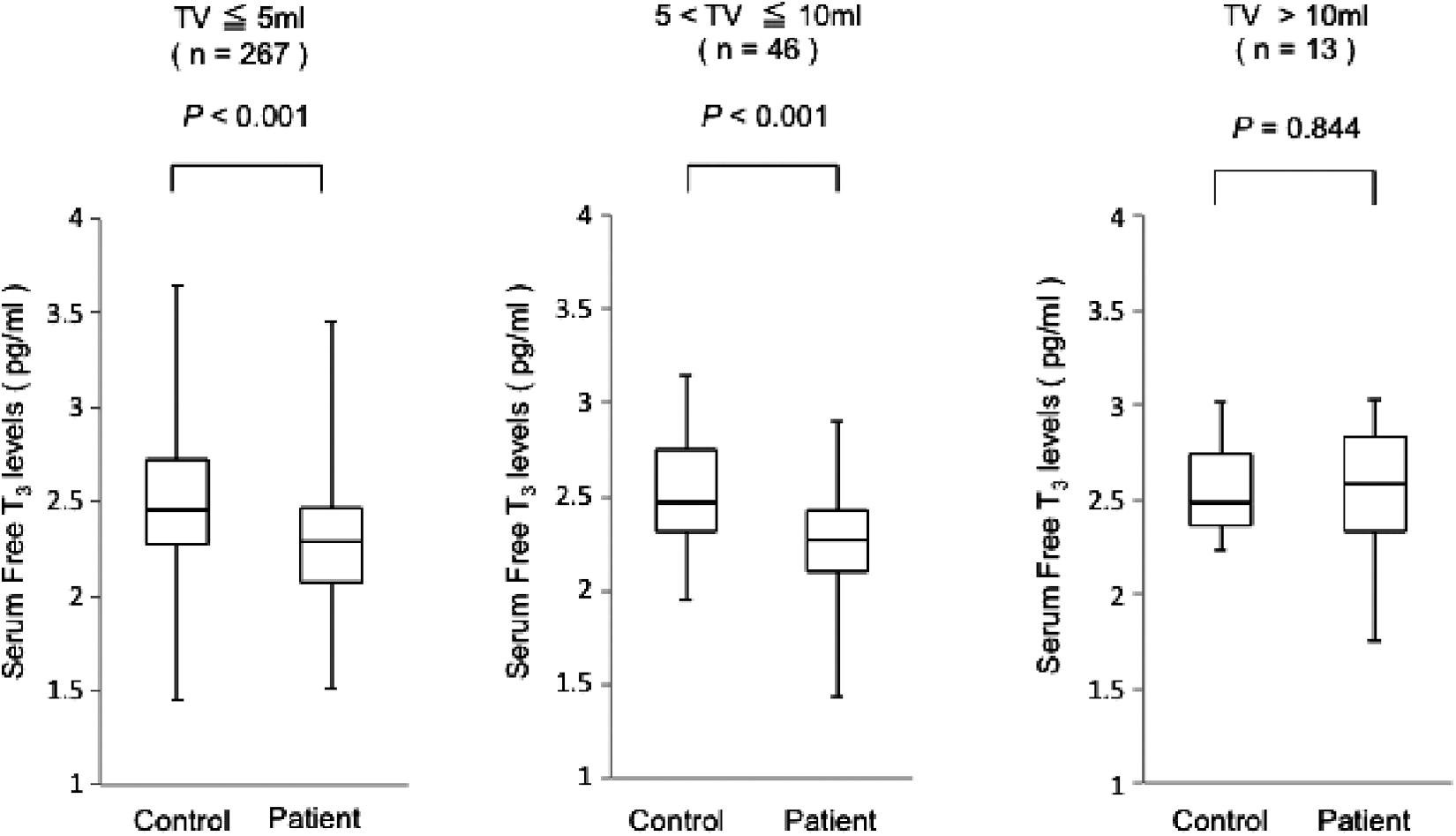
Serum fT3 levels in patients stratified according to their thyroid volumes and those in euthyroid controls matched by age, sex, and BMI. Patients with normal serum TSH levels were divided into three groups according to thyroid volume. The top, bottom, and middle lines of the boxes correspond to the 75th, 25th, and 50th percentiles (median), respectively. The whiskers extend from the minimum to the maximum.
Serum fT4 levels in patients with TV less than 5 mL and those between 5 and 10 mL were significantly higher than those of the matched controls (1.14 [1.05–1.26] vs. 1.03 [0.94–1.10] ng/dL, p < 0.001, and 1.12 [0.98–1.23] vs. 1.08 [0.96–1.11] ng/dL, p < 0.05, respectively). However, the serum fT4 levels were equivalent to those of the matched controls in patients with TV more than 10 mL (1.14 [0.95–1.27] vs. 1.15 [1.01–1.22] ng/dL, p = 0.798).
Discussion
After radioiodine treatment for Graves' disease, most patients develop hypothyroidism in conjunction with atrophic changes of the thyroid gland, and are treated with LT4. In this study, in such cases, patients with normal TSH levels had serum fT3 levels that were significantly lower than those of controls. Patients with mildly suppressed TSH levels had serum fT3 levels equivalent to those of controls, and patients with strongly suppressed TSH levels had significantly higher serum fT3 levels. Thus, these data obtained for patients who underwent radioiodine treatment were similar to those from our previous studies of athyreotic patients on LT4 who underwent total thyroidectomy (2,13,14), and also similar to those reported by Gullo et al. (4) and Hoermann et al. (5). These findings suggest that the reason underlying the decreased serum T3 levels in such patients is the lack of intra-thyroidal T3 production caused by atrophy or loss of the thyroid gland.
In this study, serum fT3 levels in patients with TV 10 mL or less were significantly lower than those of the controls; whereas in patients with TV more than 10 mL, serum fT3 levels were equivalent to those of the controls. In our previous study, in patients on LT4 who underwent a hemithyroidectomy, postoperative serum fT3 levels were equivalent to those of matched controls (13). Maia et al. reported that deiodinase 2 (D2) is expressed in the human thyroid gland and is postulated to play an important role as a source of plasma T3 (15). It has been suggested that increased D2 expression in a large thyroid gland may account for the relatively high circulating T3 levels in several thyroid diseases, such as those resulting from thyroglobulin gene abnormalities (16), McCune-Albright syndrome (17), and T3-predominant Graves' disease (18). Hoermann et al. indicated that LT4-treated patients with a postinterventional lower residual volume (<5 mL) have significantly reduced deiodinase activity and lowered T3 levels, compared with patients with a higher residual TV (19). These results suggest that thyroid tissue capacity plays a significant role in the physiological process of T3 homeostasis in humans; this concept fits well with the results from this study.
In athyreotic or atrophic thyroid patients on LT4 after thyroidectomy or radioiodine treatment, patients with normal TSH levels had relatively low serum fT3 levels, whereas patients with mildly suppressed TSH levels had normal serum fT3 levels. The question arises as to which of such two patient groups is in a euthyroid condition. The extensive literature on “subclinical hyperthyroidism” has demonstrated an increased risk of atrial fibrillation, as well as low bone density and fractures in patients who have low TSH levels while receiving LT4. Moreover, in the athyreotic patients with normal TSH and low T3 levels, the relatively higher serum T4 levels that accompany LT4 monotherapy seem to result in normal T3 receptor occupancy and TSH in pituitary thyrotrophs. On the other hand, in peripheral tissues, the relatively higher serum T4 levels could impair intracellular T3 production via downregulation of D2 (20). In fact, an animal study has shown that LT4 alone administered to thyroidectomized rats at doses to normalize plasma TSH levels does not normalize T3 contents in some tissues (21). In another study of rats, Werneck et al. reported that a combination of high serum T4 and low serum T3 levels during T4 monotherapy rats had consequences for thyroid hormone action, as reflected in the brain, liver, and skeletal muscle, all of which exhibited indications of hypothyroidism despite normal serum TSH levels (20). In a previous study conducted in humans, we compared serum levels of lipoproteins, sex hormone-binding globulin (SHBG), and bone metabolic markers before and after thyroidectomy (14). The postoperative serum SHBG and bone alkaline phosphatase levels were significantly increased in the patients with strongly suppressed TSH levels. The postoperative serum low-density lipoprotein cholesterol levels were significantly increased and the serum tartrate-resistant acid phosphatase 5b levels were significantly decreased in patients with normal TSH levels. In patients with mildly suppressed TSH and fT3 levels equivalent to their preoperative levels, all metabolic markers remained equivalent to their preoperative levels (14). Recently, in a large LT4-treated population with normal serum TSH, participants exhibited lower serum T3 levels and differed in terms of both objective and subjective measures (22). In addition, a meta-analysis performed by McAninch et al. showed that serum total cholesterol and low-density lipoprotein levels remain high in LT4-treated euthyroid patients (23). Overall, the presence of biochemical markers of thyroid function in animal and human studies of LT4-treated athyreotic conditions suggests that patients with normal TSH might not be euthyroid in all tissues, whereas patients with a low TSH are less likely to have hyperthyroid symptoms.
Symptoms suggestive for thyroidal dysfunction in LT4-treated patients have also been reported by several prior studies. Larisch et al. conducted a retrospective longitudinal study including 319 patients with differentiated thyroid carcinoma on LT4. As a result, 26% of patients expressed hypothyroid and 9.7% expressed hyperthyroid complaints at any one visit. Although rates of both hypothyroid and hyperthyroid symptoms were significantly related to all three thyroid parameters, hypothyroid symptoms correlated well with fT3 levels when TSH levels were below the reference range (24). Hirata et al. studied patients with central hypothyroidism and athyreotic patients who underwent total thyroidectomy. In central hypothyroidism and total thyroidectomy patients, those with median-lower to normal levels of serum fT4 exhibited lower serum fT3 levels and lower body temperature (25). These data support an important role of serum fT3 levels in the manifestation of symptoms, which has implications for clinical decision making on dose adequacy, particularly in athyreotic patients.
There are some possible limitations in this study. First, the limited number of study patients, unequal group distribution, and assessment at a single time point reduces the internal validity of the study. Second, we did not evaluate biochemical markers and the symptoms reflecting thyroid function. Studies including measures of these clinical parameters are, thus, needed to clarify the best method of managing patients' thyroid function after radioiodine treatment.
Patients who have undergone radioiodine treatment and subsequently experience hypothyroidism live in a chronic condition of abnormal thyroid hormone status for the remainder of their lives. Therefore, even if the thyroidal dysfunction is subtle, its long-term effects cannot be ignored. The American Thyroid Association stated in its guidelines that for the treatment of hypothyroidism such as in athyreotic patients, there is insufficient evidence of benefit to recommend LT4 treatment for achieving low-normal TSH values or high-normal T3 values (26). The results of this study suggest that mild TSH suppression with LT4 monotherapy is needed to achieve normal fT3 levels in patients who experience an atrophic thyroid condition after having undergone radioiodine treatment. Our findings may provide novel information that could assist in the management of a large number of patients who experience hypothyroidism after having undergone radioiodine treatment for Graves' disease.
Authors' Contributions
M.I. constructed the study design and analyzed the data. The other coauthors contributed by administering patient care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.