
Abstract
Surgical outcomes of pelvic organ prolapse (POP) surgery are poor, resulting in a 20% recurrence risk. Following the hypothesis that impaired wound healing is the main determinant of recurrent POP, growth factors have the potential to promote wound healing and may improve surgical outcomes. In this study, we systematically reviewed the effect of growth factors on vaginal wound healing in both in vitro and animal studies. For each independent comparison, the standardized mean difference and 95% CI were calculated using the Hedges' g correction. Of the 3858 retrieved studies, seven studies were included, of which six were included in meta-analysis (three in vitro studies and four in vivo studies). In vitro, basic fibroblast growth factor (bFGF) promotes proliferation, differentiation, and collagen types I and III production. Epidermal growth factor stimulates proliferation and connective tissue growth factor promotes Tenascin-C expression. These effects, however, are less pronounced in vivo; only bFGF slightly promotes collagen production. The review shows that growth factors, particularly bFGF, are able to promote vaginal wound healing in vitro. The uncertain in vivo findings suggest that preclinical models should be improved. The ultimate goal is to develop effective growth factor-supplemented therapies that improve surgical outcomes for POP.
Impact statement
Growth factors, particularly basic fibroblast growth factor, promote vaginal wound healing in vitro, but the effects are less prominent in vivo. To improve surgical outcomes for pelvic organ prolapse in the future, more research is required, including improved preclinical models.
Introduction
The lifetime risk for pelvic organ prolapse (POP) surgery is 12.6%, 1 corresponding to 166,000 operations in 2010 in the United States, which may increase to 310,050 in 2050. 2 POP is characterized by the descent of pelvic organs into the vagina, due to the weakening of the pelvic floor supportive tissues. Surgical outcomes of POP are poor with ∼20% recurrence after native tissue repair. 3 Compared to healthy tissues, POP tissues are characterized by an increased fibroblast contractility and an altered extracellular matrix (ECM) composition (growth factor densities and collagen content), resulting in disrupted tissue integrity and reduced load-bearing capabilities.4,5
Reciprocally, the disrupted tissue integrity has impairing effects on the subsequent wound healing processes. It has been hypothesized that the high recurrence rate originates from impaired wound healing, possibly through the altered functionality of POP fibroblasts. 5 To improve surgical outcomes, implants such as polypropylene meshes have been introduced with frequent severe adverse events after implantation. 6 Currently, there is an urgent need for developing alternative strategies to promote vaginal wound healing to improve surgical outcomes for POP.
A promising strategy is tissue engineering, which uses the combination of cells, biomaterials, and biomechanical and biochemical cues to regenerate tissues. 6 Multiple cell types have been investigated regarding pelvic tissue regeneration, such as fibroblasts, 7 bone marrow-derived stem cells, 8 adipose-derived stem cells (ADSCs), 9 endometrial mesenchymal stem cells (MSCs),10,11 and skeletal muscle-derived stem cells. 12 Biomaterials such as polycaprolactone, 13 polylactic acid,14,15 and polylactic-co-glycolic acid 9 have shown promise in triggering a regenerative pelvic tissue response.
Moreover, biomechanical cues are capable of stimulating fascia tissue regeneration. 16 As for biochemical cues, a recent systematic review details that estrogen improves vaginal wound closure, collagen production, and tissue strength in vivo. 17 Also, studies with growth factors have shown promising results; their signaling pathways are generally well understood as is their role in wound healing.5,18 Their true impact on stimulating vaginal wound healing, however, is still relatively unclear.5,19,20 Although systematic reviews have examined the potential of growth factors in bone regeneration,21,22 liver regeneration, 23 and periodontal regeneration, 24 no systematic review has been published covering the effect of growth factors in the context of vaginal wound healing.
In this study, we examine the effect of growth factors on vaginal wound healing by providing a systematic overview of both in vitro and animal studies. The former was included to provide a comprehensive overview of the field. Through conducting a meta-analysis, we quantitatively assess the efficacy of each growth factor on outcome measures describing vaginal wound healing. This systematic review improves understanding of the effect of these growth factors and suggests directions on how to improve translatability of in vitro results, which ultimately should aid the surgical outcomes for POP.
Method
To study the effect of growth factors on vaginal wound healing, this systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 25 The protocol was registered in the international prospective register of systematic review (PROSPERO) on January 15th, 2021 (CRD42021226841). An amendment to the protocol was made on May 21st, 2021, whereby an additional inclusion criterion during the abstract screening was added: outcomes describing vaginal wound healing.
Literature search
The systematic literature search was conducted in Ovid MEDLINE, through the PubMed interface, and Ovid EMBASE to identify all relevant studies up to March 22nd, 2021. The SYRCLE step-by-step guide was used to design a comprehensive search strategy. 26 The search strategy consisted of MeSH and EMTREE terms for PubMed and EMBASE, respectively, as well as title/abstract (tiab) terms for all three search domains: (1) growth factors; (2) vaginal wound healing, POP, pelvic floor, or vaginal reconstruction/repair; and (3) in vitro and animal filter (for complete search strategy, see Supplementary Tables S1 and S2). No additional restriction was applied. Cited articles of included studies and relevant reviews were crosschecked for potentially relevant studies. The studies were imported and de-duplicated in EndNote X9 (Clarivate Analytics).
Study selection
The studies were independently screened by two reviewers (M.J.J.v.V. and A.N.G.). The initial round of screening was based on title and abstract, which was conducted using the Rayyan web tool. 27 The following inclusion criteria were used: (1) an original research article, (2) a preclinical (animal/in vitro) study, (3) growth factor administration/supplementation, and (4) outcome measures describing vaginal wound healing. In the second round of screening, full texts were screened using the same exclusion criteria as mentioned above, including an additional fifth inclusion criterion: in the case of animal studies, growth factor(s) should be locally delivered. Discrepancies between the reviewers were resolved through discussion between the two reviewers, and when no consensus was reached, a third reviewer (Z.G.) was consulted. At last, screening was performed based on reference lists of included studies and relevant reviews to check for potentially missing studies.
Study characteristic extraction
The following study design characteristics were extracted from all included studies: bibliographical data (author and year), experimental and control groups, time point outcome assessment, type of growth factor, growth factor administration method, dosage, and reported outcome measures (both descriptive and quantitative data) describing vaginal wound healing. For in vitro studies, the following in vitro model details were reported: cell type, passage number, healthy or diseased, and premenopausal or postmenopausal status. For in vivo studies, the following animal model characteristics were reported: species, strain, healthy or diseased, premenopausal or postmenopausal, parous state, location of intervention, and survival. Authors were contacted in the case of missing study characteristics.
Quality assessment
For the in vitro studies, quality assessment was performed using an adapted version of the commonly used OHAT tool (Supplementary Table S3). 28 Risk of bias was assessed for all included animal studies using the SYRCLE Risk of Bias tool for animal studies. 29 Since reporting of experimental details on animals, methods, and materials is generally very poor,30,31 we added two items on reporting to overcome the problem of judging too many items as unclear risk of bias: “reporting of any measure of randomization” and “reporting of any measure of blinding.” Two independent reviewers assessed the risk of bias in the included studies (M.J.J.v.V. and F.S.). Discrepancies were solved through discussion, and when no consensus was reached, the methodologist (C.R.H.) was consulted.
Meta-analysis
The mean, variability and uncertainty measures (standard deviation [SD], standard error of the mean [SEM] or 95% confidence interval [95% CI]), and sample size (n) were extracted for each independent comparison of all quantitative reported outcome measures described in Supplementary Tables S4 and S5. Data applicable for meta-analysis were extracted independently by two reviewers (M.J.J.v.V. and A.N.G.). The first reviewer (M.J.J.v.V.) checked the data for discrepancies and the data of M.J.J.v.V. were used for the meta-analysis. When the data were only visualized in the figures, a digital ruler software was used (FIJI). Authors were contacted through e-mail in the case of incomplete data.
Meta-analysis was performed with Comprehensive Meta-Analysis (CMA; version 3.0) only when a minimum of four independent comparisons was reached for each reported outcome, per growth factor type, and separately for in vitro and in vivo studies. When the mean, variability and uncertainty measures, or sample size could not be extracted, the comparison was excluded for meta-analysis.
In case sample sizes were provided in a range or there was a mismatch between methods and results, the lowest number was used for meta-analysis. When it was unknown whether the SD or SEM was reported, we assumed SEM to prevent overestimation of the variability and uncertainty measures. For the meta-analysis, the SEM and 95% CI were translated to SD using the following formulas: (1)
For each independent comparison, the standardized mean difference (SMD) and 95% CI were calculated using the Hedges' g correction. When similar outcomes were reported in the same study, priority was given to the primary outcome described in the PROSPERO protocol. For in vitro studies, we assumed that in the case of outcome assessment on multiple time points, independent experiments were conducted. The random-effects model was used to calculate the overall effect, which assumes that the observed treatment effect can vary between studies due to differences in treatment effect in each study as well as sampling variability. 33 The statistical method I2 was used to assess heterogeneity.
For the following predefined study, characteristic subgroup analysis was conducted in the case of at least five independent comparisons in a minimum of three studies: species, administration route, type of surgical procedure, dosage, and time point outcome assessment. For time point outcome assessment, we categorized “short” as the first 7 days, “middle” as 8–14 days, and “long” as more than 14 days.
Sensitivity and publication bias analyses
Sensitivity analyses were conducted in the case of at least four comparisons to examine the robustness of the main analyses. First, we investigated the effect of a possible interaction based on time point outcome assessment for the in vitro outcomes. We checked whether the assumption that all reported time points were independent comparisons showed similar results compared to the assumption that multiple time points are repeated measures. Second, we investigated the effect of a possible interaction based on different methods reporting the same outcome, by performing sensitivity analyses for each method independently. For the assessment of publication bias, funnel plots were generated in the case of a minimum of 15 studies of a specific outcome.
Experiment
Study selection
The comprehensive literature search resulted in 3858 unique records, which were assessed for eligibility (Fig. 1). Twenty-two studies met our inclusion criteria based on title and abstract screening. After full-text screening, seven studies were included in this systematic review, of which six studies could be included in the meta-analysis.
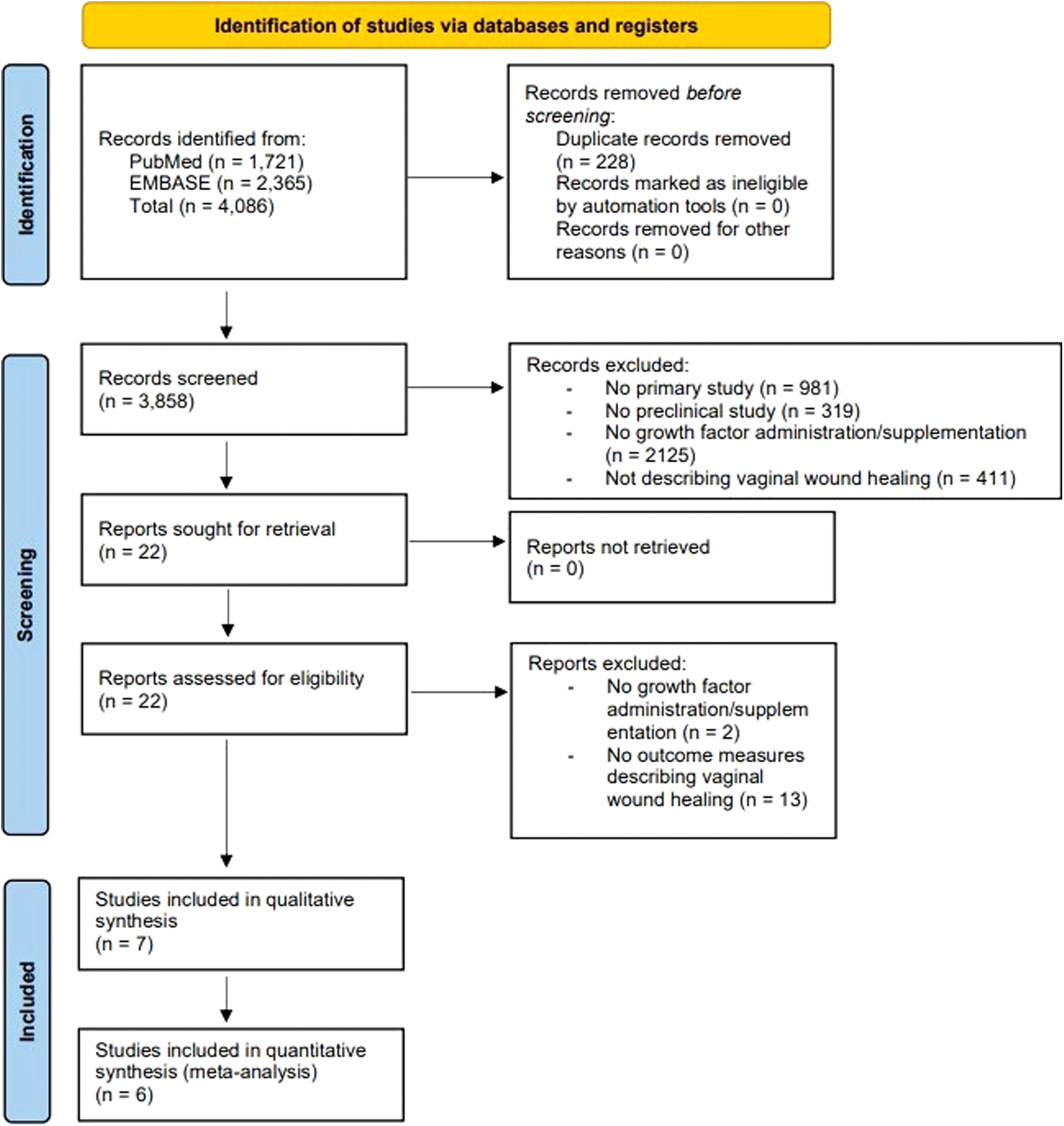
PRISMA flow diagram. Color images are available online.
Study characteristics
The study characteristics of the included in vitro and in vivo studies are summarized in Table 1 (Supplementary Tables S4 and S5 for detailed version). Of Jin et al., only the in vitro section was included in the systematic review as the in vivo experiments did not include an appropriate control. 8 Basic fibroblast growth factor (bFGF) is the most reported growth factor (six studies), followed by connective tissue growth factor (CTGF) (two studies) and epidermal growth factor (EGF) (one study).
Study Characteristics of All Included Studies
Descriptive outcome measure.
eMSCs cultured on a polyamide mesh.
Co-cultured with fibroblasts.
Conditioned medium of bFGF-transfected ADSCs cultured on HUVECs.
10 mg/mL bFGF in 10 mM Tris, pH 8.5.
ADSC, adipose-derived stem cell; BMSC, bone marrow-derived stem cell; eMSC, endometrial mesenchymal stem cell; GF, growth factor; bFGF, basic fibroblast growth factor; EGF, epidermal growth factor; CTGF, connective tissue growth factor; PLGA, poly(lactic-co-glycolic) acid; MOI, multiplicity of infection; NR, not reported; ECM, extracellular matrix; IL-1β, interleukin-1β; TNF-α, tumor necrosis factor α; IL-6, interleukin-6; HUVEC, human umbilical vein endothelial cell.
Regarding in vitro studies, dosage and type of administration varied across the studies, such as soluble administration (three studies), loaded in nanoparticles, incorporated into a polypropylene mesh, and transfected (each one study). The main reported in vitro outcomes related to vaginal wound healing are proliferation (four studies), (stem)cell differentiation into fibroblasts (two studies), and protein expression of collagen type I (two studies), type III (one study), and Tenascin-C (TNC) (one study).
Regarding in vivo studies, bFGF is the most reported growth factor (three studies). In addition, one study also investigated the effect of CTGF on vaginal wound healing. The administration method and location of implantation are similar across all in vivo studies: incorporated into a mesh implanted in the abdominal wall (three studies). In this study, the main reported outcomes related to vaginal wound healing are macroscopic evaluation (two studies), biomechanical properties (three studies), histological assessment focusing on the inflammatory response (two studies) and collagen expression (three studies), gene and protein expression of collagen type I and type III (two studies), and total collagen measurements (three studies).
Quality assessment
To assess the quality of included studies, we assessed risk of bias in all studies. In 33% of the in vivo studies, authors reported randomization of animals across various groups. In contrast, in none of the in vitro studies, authors reported any randomization protocol during the conduct of their experiments (Supplementary Fig. S1). Randomization was not performed in any of the included studies regarding random selection during outcome assessment. Blinding at any level was reported in 66% of the in vivo studies and not reported in the in vitro studies. Sixty-six percent of the in vivo studies inadequately addressed incomplete outcome data, resulting in a high risk of bias. Many risk of bias domains scored an unclear risk of bias, which indicates that methodological details of included studies were often incomplete. For example, in none of the in vivo and in vitro studies, the allocation sequence was described.
Meta-analysis
As not always all outcome data could be retrieved, only six studies were included in the meta-analysis (Fig. 1). Jin et al. was excluded from the meta-analysis, as the sample size of the reported outcome could not be retrieved. The meta-analysis consists of both in vitro and in vivo analyses. In the in vitro analyses, we assessed the effect of growth factors on proliferation, differentiation into fibroblasts, and the expression of ECM proteins collagen type I and III and TNC. In the in vivo analyses, we determined the effect of growth factors on collagen expression and biomechanical properties.
In vitro analyses
Proliferation
bFGF significantly stimulates proliferation (SMD = 1.54, 95% CI = [1.10–1.98], n = 45, I2 = 69%, p < 0.001) (Fig. 2A and Supplementary Fig. S2). To determine the effect of bFGF on proliferation at different time points, subgroup analysis was performed based on time point outcome assessment. Regarding short term, the effect size is similar to the main analysis (SMD = 1.43, 95% CI = [1.00–1.86], n = 43, I2 = 65%) (Fig. 2B and Supplementary Fig. S3). We could not assess the effect on proliferation at middle or long term, due to the limited number of independent comparisons reporting at later time points. EGF also promotes proliferation (SMD = 0.69, 95% CI = [0.23–1.15], n = 21, I2 = 48%, p = 0.004), but the effect size is lower in comparison to bFGF (Fig. 2A and Supplementary Fig. S4).

Overview of the meta-analysis results of the effect of growth factors on proliferation
(Stem) cell differentiation into fibroblasts
Meta-analysis revealed that treatment with bFGF significantly promotes ADSC to fibroblast differentiation based on histological expression of fibroblast-specific protein 1 (FSP-1) (SMD = 3.96, 95% CI = [1.54–6.39], n = 4, I2 = 61%, p = 0.001) (Fig. 2C and Supplementary Fig. S5).
ECM metabolism
bFGF significantly upregulates collagen type I (SMD = 5.77, 95% CI = [3.03–8.52], n = 7, I2 = 75%, p < 0.001) and collagen type III (SMD = 4.27, 95% CI = [2.15–6.39], n = 7, I2 = 71%, p < 0.001) (Fig. 2D and Supplementary Fig. S6). CTGF significantly increases the expression of TNC (SMD = 4.74, 95% CI = [2.61–6.86], n = 8, I2 = 88%, p < 0.001) and collagen type I (SMD = 1.72, 95% CI = [0.69–2.76], n = 8, I2 = 76%, p = 0.001) (Fig. 2E and Supplementary Fig. S7A, B).
In vivo analyses
Collagen expression
No effect of bFGF on COL1A1 (SMD values) and COL3A1 expression was observed (SMD values) (SMD = 0.16, 95% CI = [−0.61 to 0.92], n = 5, I2 = 59%). For total collagen production, bFGF has a slight promoting effect (SMD = 0.83, 95% CI = [0.05–1.60], n = 9, I2 = 71%, p = 0.036) (Fig. 3A and Supplementary Fig. S8A–C).

Overview of the meta-analysis results of the effect of growth factors on collagen expression
Biomechanical properties
bFGF has no effect on the biomechanical properties (Fig. 3B and Supplementary Fig. S9). The effect of bFGF was assessed for the following biomechanical properties: elastic modulus (SMD = −0.28, 95% CI = [−1.00 to 0.45], n = 8, I2 = 64%), ultimate tensile strength (UTS) (SMD = 0.47, 95% CI = [−0.04 to 0.98], n = 8, I2 = 37%), strain at UTS (SMD = 0.24, 95% CI = [−0.27 to 0.75], n = 5, I2 = 4%), and explant thickness (SMD = −0.35, 95% CI = [−1.47 to 0.78], n = 5, I2 = 79%).
Sensitivity and publication bias analyses
Sensitivity analyses were performed to test the robustness of our main analysis. First, when only the last reported time points were included instead of all reported time points, the promoting effect of CTGF on collagen type I in vitro appeared to be diminished (SMD = 1.87, 95% CI = [−0.04 to 3.77], n = 4, I2 = 85%), in contrast to a significant increase in the main analysis (Supplementary Fig. S7C). Second, on a histological level, bFGF does not affect collagen production in vivo, whereas in the main analysis, bFGF significantly increased collagen production (SMD = 0.56, 95% CI = [−0.32 to 1.44], n = 5, I2 = 60%) (Supplementary Fig. S8D). Publication bias could not be assessed due to the limited number of studies.
Discussion
Main findings
The meta-analysis provides evidence, in the context of vaginal wound healing, that in vitro bFGF and EGF stimulate proliferation, bFGF promotes protein expression of collagen type I and III and differentiation into fibroblasts. In addition, CTGF stimulates the ECM protein expression of TNC in vitro. However, no promoting effect of bFGF on COL1A1 and COL3A1 expression, and biomechanical properties was observed in vivo. We note that bFGF significantly stimulates total collagen production, but this effect did not appear to be robust. A schematic overview of the key findings is presented in Figure 4.
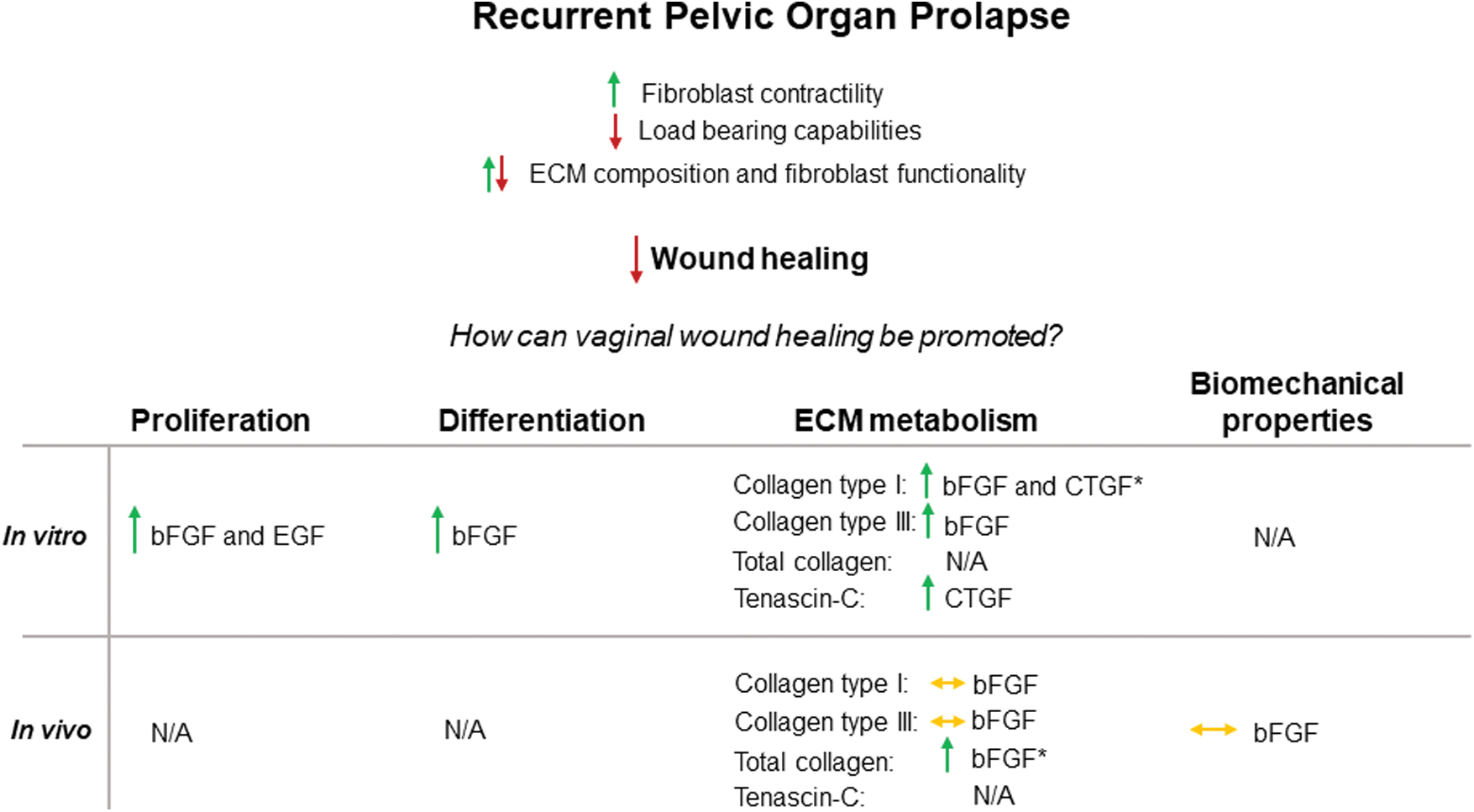
Schematic overview of the key findings. Impaired vaginal wound healing is a major determinant of recurrent POP. Growth factors have the potential of promoting vaginal wound healing regarding proliferation, (stem) cell differentiation into fibroblasts, ECM metabolism and biomechanical properties. The effects of the individual growth factors are summarized for in vitro and in vivo separately (green = promoting effect, red = impaired effect, green/red = altered effect, orange = no effect and N/A = not applicable). The *marks the effects that did not appear to be robust upon sensitivity analyses. POP, pelvic organ prolapse. Color images are available online.
Strengths and limitations
Although it is the first systematic review describing the effect of growth factors on vaginal wound healing in vitro and in vivo, this review also has some limitations. First, the number of included studies in the meta-analysis is rather low, which may result in the imprecision of the overall effects, emphasizing that more research in the context of vaginal wound healing is required. Second, there was substantial heterogeneity between the included studies.
To account for the substantial heterogeneity between the included studies, we used the SMD and the random-effects model. Third, due to the limited number of included studies, we were not able to perform subgroup analyses for the following study characteristics: species, administration route, type of surgical procedure, duration, and dosage. In the case of treatment duration, we were able to perform subgroup analysis solely for the outcome proliferation upon bFGF treatment. Fourth, we were not able to assess the risk of publication bias due to a limited number of included studies.
We expect that our results are slightly overestimated as systematic reviews of preclinical studies have reported the presence of publication bias. 34 Fifth, most of the included studies poorly reported all essential methodological details, which hampered the risk of bias assessment and possibly affected the reliability of our findings. Sixth, some potentially relevant outcomes could not be included due to a lack of methodological details or the use of proper control groups in multiple studies. Seventh, all in vivo studies used healthy premenopausal animals, whereas the majority of patients is postmenopausal. Postmenopausal status negatively affects vaginal wound healing due to reduced estrogen levels, 35 making it more challenging to translate our findings to the clinical setting.
Interpretation
Proliferation
Fibroblasts play a critical role in all three phases of wound healing as they deposit and remodel the ECM, and facilitate wound contraction. Fibroblast proliferation is crucial in (vaginal) wound healing and it is well established that cell proliferation is stimulated with growth factor treatment. 5 Our meta-analysis indicates that bFGF and EGF promote proliferation in vitro. It has been reported that bFGF stimulates proliferation in the context of tendon 36 and cartilage regeneration 37 in vitro, and salivary gland regeneration in vivo 38 ; and EGF in urothelial regeneration in vivo. 39 So far, no in vivo research has been conducted regarding the effect of growth factors, such as bFGF, on proliferation during vaginal wound healing.
(Stem) cell differentiation into fibroblasts
During wound healing, MSCs become activated, are recruited to the wound, and differentiate into fibroblasts. 40 For example, platelet-derived growth factor (PDGF) 41 and vascular endothelial growth factor (VEGF) 42 can promote wound healing in patients with diabetic foot ulcers, whereby PDGF and VEGF act as chemoattractants for MSCs. 43 The meta-analysis revealed that bFGF significantly promotes ADSC differentiation into fibroblasts. However, the effect of growth factors on the recruitment and differentiation of (stem) cells into fibroblasts is still unknown for vaginal wound healing in vivo.
ECM metabolism
The relation between POP and connective tissue metabolism suggests that improved vaginal wound healing requires the regulation of ECM metabolism.5,44 The meta-analysis showed that bFGF stimulates collagen I and III production in vitro. CTGF also plays a key role in regulating ECM production. For example, an in vitro study demonstrated a promoting effect of CTGF on collagen deposition. 45 Although our meta-analysis also showed that CTGF promotes the deposition of collagen type I in vitro, sensitivity analysis could not validate this effect. 46 In line with our findings, Zhang et al. also demonstrated that in vitro CTGF treatment resulted in an upregulated expression of TNC in the context of renal tubulointerstitial fibrosis, 47 emphasizing its important role in wound healing by upregulating collagen expression and maintaining the integrity of the ECM. 48
Upon bFGF treatment, upregulation of collagen type I and III could not be observed in vivo. Moreover, the slight promoting effect of bFGF on total collagen content in vivo could not be validated by sensitivity analysis, which suggests that the effect of bFGF on collagen synthesis in vivo is still uncertain. In line with these findings, other in vivo studies presented contradictory results: both promoting 49 and impairing 50 effects of bFGF on collagen synthesis during wound healing were reported. A possible explanation for these contradictory results could be that collagen deposition during wound healing is intricately linked to fibrosis, which is caused by excessive collagen deposition in the case of impaired wound healing. 51
Another explanation could be that the effect of growth factors on collagen expression is dependent on the dosage and duration of the growth factor treatment. However, this dependency could not be investigated through subgroup analysis, which prevented us from determining “optimal” growth factor concentrations. It should be noted that the optimal dose not only depends on the growth factor type but also varies according to the administration method and animal model.
Biomechanical properties
The pelvic floor is continuously exposed to mechanical loading; therefore, sufficient tissue strength is crucial for providing pelvic organ support. In POP patients, tissue integrity and strength 52 of the pelvic floor are impaired, whereas the tissue of the (anterior) vaginal wall is stiffer compared to healthy tissue. 53 This increased stiffness may contribute to POP as it can induce vaginal fibroblast to myofibroblast differentiation. 54 Introducing a growth factor to the injured tissue could trigger a wound healing response characterized by tissue remodeling, which eventually affects the biomechanical properties. The meta-analysis showed that bFGF has no effect on the following biomechanical properties: elastic modulus (as an indication for tissue stiffness) and strain at UTS or UTS (indicators for tissue strength).
In the context of skin wound healing, Lu et al. demonstrated that bFGF administration resulted in an insignificant increase in tissue stiffness and a significant increase in tissue strength. 55 However, data regarding POP-related biomechanical properties are limited in animal models. 56 Whether POP biomechanics are adequately mimicked in these animal studies remains doubtful. Clearly, more research is required to determine the “optimal” vaginal tissue strength and stiffness in healthy tissue, as these are currently still unknown.
Implications
Based on this systematic review, we conclude that growth factors have a promoting effect on vaginal wound healing in vitro. bFGF is the most promising candidate as it promotes proliferation, stem cell differentiation into fibroblasts, and collagen production. In vivo, bFGF promotes total collagen production as well, but this effect did not appear robust. This emphasizes that the effect of bFGF on collagen synthesis in vivo in the context of POP is still uncertain and that more research is required to determine the potential of bFGF in promoting collagen production, while avoiding fibrosis. In general, this discrepancy emphasizes that the effects observed in vitro do not translate to the (pre)clinical situation.
We suggest that the translation from in vitro to in vivo can be enhanced by developing more complex in vitro models, which better resemble the wound healing process of POP patients. In such a model, an organ-on-a-chip, for example, growth factors can be investigated under more relevant physiological conditions, which would reduce animal use in accordance with the 3Rs principle (replacement, reduction and refinement). 57
To account for the fact that growth factor delivery is potentially suboptimal in promoting vaginal wound healing, these devices can be used to more accurately assess growth factor delivery and dosage in comparison to conventional in vitro assays. Furthermore, we advise that clinicians contribute to these in vitro models by defining which biological parameters should be included. We also suggest that future research should include other growth factors, such as VEGF, PDGF, and transforming growth factor β. By studying the effect of different growth factors in an in vivo-mimicking environment, translation to in vivo studies can be improved.
For the translation of animal studies to the clinic, it is crucial that the effect of growth factors on vaginal wound healing is investigated in validated vaginal (larger) animal models. We note that for this systematic review, only studies with healthy, abdominal rat and rabbit models were retrieved; these models provide an indication of growth factor effects on wound healing in general, but miss the vaginal context. We suggest that animal models with larger species are used for in vivo studies, such as sheep or nonhuman primates 58 (e.g., rhesus macaques 59 or squirrel monkeys 60 ).
These animals can spontaneously develop POP and are therefore considered good models for POP. Furthermore, the anatomy of these animals better resembles the human vaginal architecture and physiology compared to the small animal models included in this review. As sheep are more ethically acceptable, we advise that future in vivo studies that examine the effect of growth factors on vaginal wound healing are performed in an ovine vaginal model. We also advise that during animal studies, the delivery and dosage of the growth factor are critically evaluated.
Growth factors are able to promote vaginal wound healing in vitro. Improved in vitro models as well as validated larger animal models can stimulate the translation from these preclinical findings to the clinic and thus the development of effective growth factor-supplemented therapies. In the future, these therapies have the potential to improve the surgical outcomes for POP, resulting in a lower recurrence rate in patients.
Authors' Contributions
M.J.J. v.V.: conceptualization, investigation, data curation, formal analysis, funding acquisition, writing – original draft, and writing – review and editing. A.N.G.: conceptualization, investigation, data curation, and writing – review and editing. F.S.: investigation and writing – review and editing. E.O.: supervision and writing – review and editing. J.P.R.: conceptualization, supervision, funding acquisition, and writing – review and editing. Z.G.: conceptualization, supervision, funding acquisition, and writing – review and editing. C.R.H.: conceptualization, investigation, methodology, supervision, and writing – review and editing. P.H.J.K.: conceptualization, supervision, funding acquisition, and writing – review and editing. All authors read and approved the final article.
Footnotes
Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This project has received public funding from ZonMw for the project “Synthesis of Evidence, more evidence with less animals” (project number: 114024158) and the TOP project (grant number: 91218030).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.