
Abstract
Background:
The prophylactic use of antibiotics in parotid region surgery continues to be a subject of debate. The aim of this study is to elucidate the impact of antibiotic prophylaxis on surgical site infections (SSIs) in parotid region surgery.
Patients and Methods:
Patients who received antibiotic prophylaxis during the peri-operative period were designated as group 1, whereas those who did not were categorized into group 2. Group 1 cases were further subdivided into three subgroups based on different antibiotic usage patterns. Patient individual information was collected. Clinical data such as surgical duration, post-operative hospital stay, incision infection status, and antibiotic usage were recorded. All data were compared and analyzed among different groups.
Results:
A total of 357 patients were included in the study, with no statistically significant differences in baseline characteristics. Pre-operative American Society of Anesthesiologists scores did not significantly differ between groups (p = 0.151), but there was a significant distinction in National Nosocomial Infection Surveillance (NNIS) index values (p = 0.044). Furthermore, surgical duration (p = 0.001) and pathology types (p = 0.016) differed significantly. The post-operative hospital stay in group 1 was longer than that in group 2 (p < 0.01). The post-operative SSI rate in group 1 was lower than that in group 2 without statistical significance (2.55% vs. 5.59%, p = 0.141). The logistic regression analysis showed that malignant tumors, longer surgical durations, and higher NNIS index scores correlated positively with post-operative SSI rates. Meanwhile, compared with non-use, all three different antibiotic use modes correlated negatively with SSI occurrence.
Conclusions:
Antibiotic prophylaxis in parotid gland surgery shows no significant reduction in SSI occurrence. If there is a compelling reason to administer prophylactic antibiotics, pre-operative single dose may be a relatively feasible measure for preventing SSIs.
Standardized antibiotic use is not only a professional competence for clinical doctors but also a responsibility. Although there are explicit guidelines in place, the inappropriate use of antibiotics persists in certain situations.
For instance, in surgeries involving clean incisions, the literature reports a post-operative surgical site infection (SSI) rate of approximately 2%. 1 The majority of practitioners agree that the incision for parotid region surgery is considered a clean incision, and, as a routine, prophylactic antibiotic use during the peri-operative period is not necessary. 2 However, some doctors argue that, given the communication between the parotid gland and the oral cavity through the Stensen’s duct, the incision in this region should be classified as clean-contaminated.3,4 Therefore, these doctors insist on antibiotic prophylaxis during the peri-operative period for parotid surgeries.
Although these two divergent viewpoints may coexist within the same medical institution, their respective validity cannot be easily proven. One thing is clear: the abuse of antibiotics not only is ineffective but also can be potentially harmful. It is essential to provide evidence-based information to clarify the use of prophylactic antibiotics in parotid gland surgery.
With the hypothesis that prophylactic antibiotic use is essentially unnecessary in surgeries involving the parotid gland, this study conducts a retrospective analysis of cases within a single hospital. The primary objective is to elucidate the effect of antibiotic prophylaxis on post-operative infection rates, while inferring potential reasons for physicians’ adoption of prophylactic antibiotics, ultimately assisting clinicians in making more informed and rational decisions regarding antibiotic prophylaxis in these surgeries.
Patients and Methods
This study adhered to the World Medical Association’s Code of Ethics (Declaration of Helsinki as revised in 2013). Ethical approval was granted by the Ethics Committee of the First Affiliated Hospital, School of Medicine, Zhejiang University (reference number: 2024-0009). This institution recognizes parotid gland surgery as a clean incision surgery and, in principle, does not recommend the prophylactic use of antibiotics in such surgeries.
All case data for patients who underwent parotid gland surgery at the Department of Oral and Maxillofacial Surgery, performed by the same group of surgeons, from January 2023 to December 2023, were collected. The exclusion criteria comprised pre-existing infections or trauma, antibiotic use within one week, a history of conditions such as diabetes and kidney disease indicating compromised immune function, and abnormal pre-operative body temperature.
The SSI in the parotid region was defined as the occurrence of local swelling, redness, tenderness, and abscess formation after surgery.
The collected data included individual information like gender, age, and body mass index (BMI), as well as clinical details such as pathological diagnosis, surgical duration, the American Society of Anesthesiologists (ASA) pre-operative assessment score, post-operative hospital stay, and infection status.
In this study, the National Nosocomial Infection Surveillance (NNIS) index was introduced to predict the risk of post-operative SSIs. 5 Considering the actual circumstances of parotid surgery, the surgery duration cut point “T” was set at 2 h. As the incision for parotid surgery does not fall under the category of contaminated or dirty, the NNIS index would ultimately range from 0 to 2.
Exploration of possible reasons for antibiotic usage
Initially, patients were divided into two groups based on whether prophylactic antibiotics were used during the peri-operative period: the antibiotics use group (group 1) and the non-use group (group 2). Subsequently, a comparative analysis was conducted to analyze the differences in baseline characteristics and post-operative clinical outcomes between patients in group 1 and group 2, and to infer the possible reasons behind physicians’ decisions regarding the use of prophylactic antibiotics.
Analysis of factors associated with SSI
To analyze the factors associated with SSI, patients were categorized into infection and non-infection groups for both uni-variable analyses and multi-variable regression. Then, patients in group 1 were further categorized into three subgroups based on different modes of antibiotic administration: pre-operative single dose (subgroup 1), peri-operative use within 24 h (subgroup 2), and extended use beyond 24 h (subgroup 3).
Uni-variable analysis was conducted on eight potential risk factors for SSI, including NNIS index, ASA, BMI index, age, pathology, antibiotic usage, gender, and operation duration.
After completing the relevant uni-variable analysis, logistic regression was employed to explore potential risk factors and their correlation with the occurrence of SSI. On the basis of the results of the uni-variable analysis and clinical expertise, and in line with the purpose of this study, relevant variables were selected as independent variables, with SSI serving as the dependent variable for binary logistic regression analysis. All variables were forcibly included in the regression model, with the entry method for independent variables set as “Enter.”
This aspect of the study specifically focused on three subgroups within group 1, representing different antibiotic administration methods, aiming to assess the relative risk of SSI compared with not using antibiotics. Three subgroups were analyzed in comparison with group 2 (antibiotics non-use group) as a reference in regression analysis.
Statistics
The data were processed using SPSS 22.0 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics for measurement data are presented as mean ± standard deviation. Group means were compared using t-tests and enumeration data were analyzed using frequency, Chi-square tests, and non-parametric rank sum tests. A significance level of p < 0.05 was considered statistically significant.
Results
Patients basic information
During the study period, there were a total of 403 cases of parotid gland surgery, of which 357 were included in the study based on the exclusion criteria. Group 1 comprised 196 patients (102 males and 94 females), whereas group 2 included 161 patients (83 males and 78 females). The three subgroups within group 1 each included 18 (subgroup 1), 62 (subgroup 2), and 116 (subgroup 3) patients, respectively.
The average age in group 1 was 49.0 ± 15.7 years, and in group 2, it was 48.1 ± 16.2 years. No statistically significant differences in gender or age were observed between the two groups.
The BMI index of the two groups were compared, and no statistically significant differences were observed (23.7 ± 3.8 vs. 23.7 ± 3.4, p = 0.939).
Clinical data
All patients underwent surgery under general anesthesia following standard surgical procedures. Patients in group 1 received prophylactic antibiotics during the peri-operative period. The selection of antibiotic types was based on empirical principles. The most commonly chosen antibiotic was cefuroxime sodium, with clindamycin selected in cases where patients were allergic to cephalosporin. The antibiotics were administered intravenously. Pre-operative single doses (subgroup 1) were administered before the start of the surgery (cefuroxime 1.5 g or clindamycin 600 mg). Subsequently, some patients continued to receive antibiotics either within 24 h (subgroup 2) or beyond 24 h (subgroup 3), using the same administration method (cefuroxime 1.5 g every 12 h or clindamycin 600 mg every 12 h).
The patients’ ASA scores, NNIS index scores, and surgical durations were recorded. There was no significant difference in ASA scores between the two groups. National Nosocomial Infection Surveillance index (Table 1) and surgical durations (Fig. 1) showed statistically significant differences.
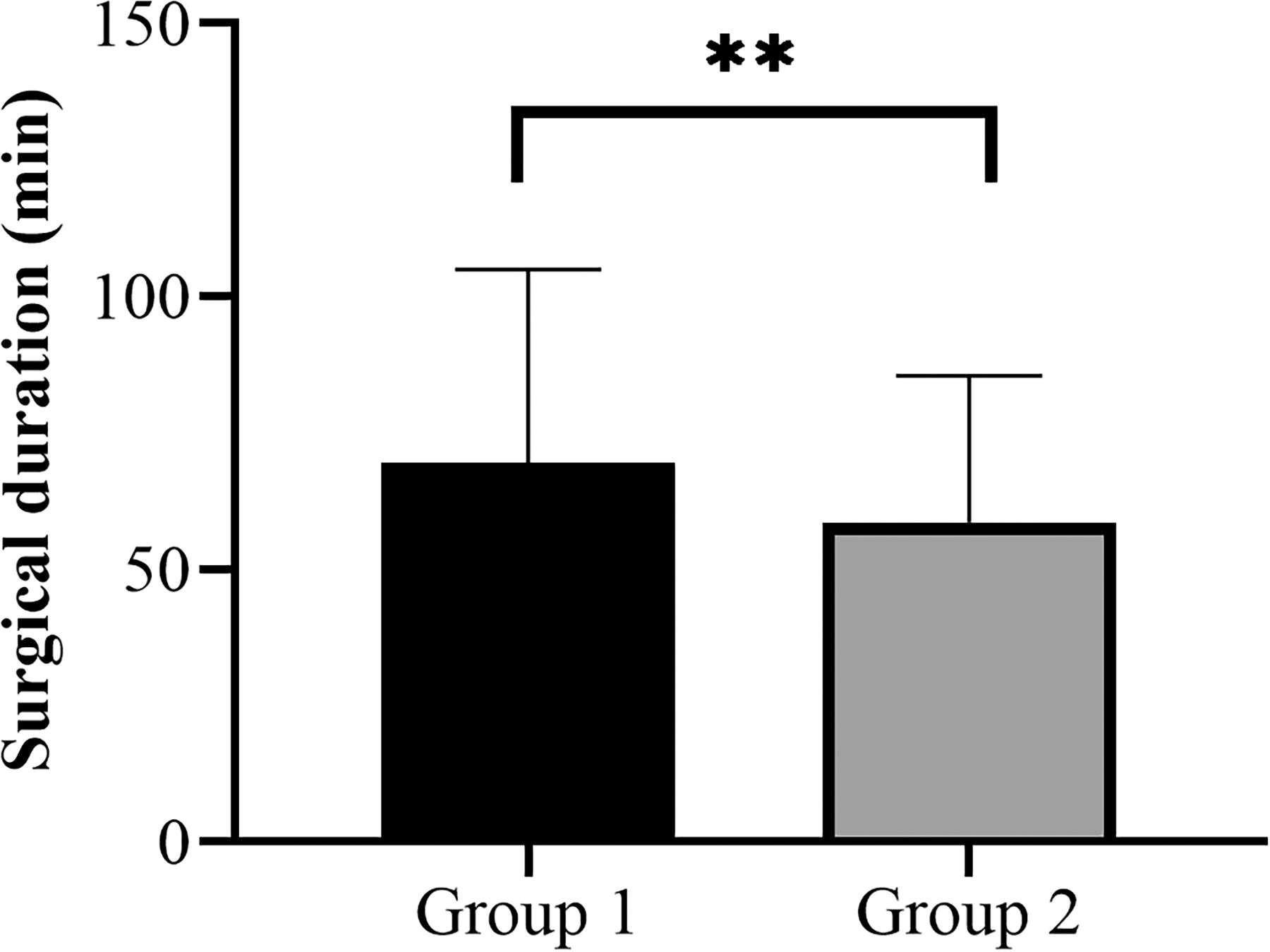
Surgical durations showed statistically significant differences between the groups (69.54 ± 35.45 min vs. 58.60 ± 26.79 min, p = 0.001).
Comparison of Pre-Operative Assessment Between the Two Groups
Both “Asymp. sig.” and “Exact sig.” were <0.05, indicating a statistically significant difference in NNIS index between the two groups. With group 1’s average rank (184.29) higher than that of group 2 (172.56), it suggested a higher NNIS index in group 1.
ASA = American Society of Anesthesiologists; NNIS = National Nosocomial Infection Surveillance.
The pathological types of all cases were confirmed post-operatively and categorized into benign and malignant for statistical analysis (Supplementary Table S1). Statistically significant differences were found in pathology between the two groups (p = 0.016). The most common benign tumors in both groups were pleomorphic adenoma and Warthin’s tumor, whereas lymphoepithelial carcinoma and mucoepidermoid carcinoma were the most common malignant tumors (Supplementary Fig. S1).
The post-operative hospital stay was longer in group 1 compared with group 2, and this difference was statistically significant (3.3 ± 1.3 d vs. 2.8 ± 1.1 d, p < 0.01).
Post-operative infection and wound healing
In group 1, there were five cases of infection (2.55%), whereas in group 2, there were nine cases of infection (5.59%). The difference in SSI rates was not statistically significant (p = 0.141) (Fig. 2). All non-infection cases achieved Grade A wound healing. However, among the 14 infection cases, only 4 achieved Grade A wound healing, whereas the rest were Grade B.
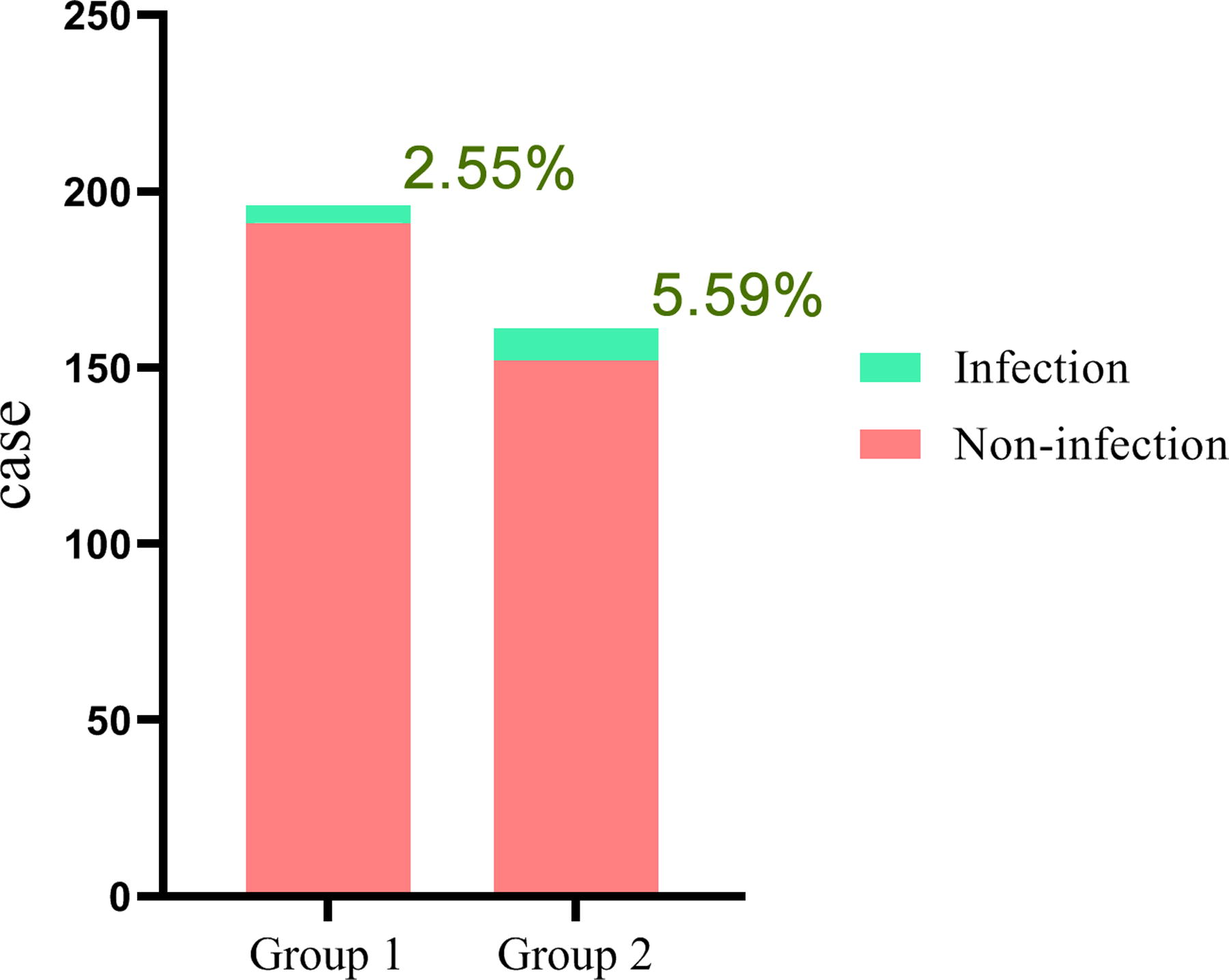
Group 1 had five infections (2.55%), whereas group 2 had nine infections (5.59%). Despite group 1 having a lower surgical site infection (SSI) rate than group 2, the difference was not statistically significant.
In addition to infections, there were other complications observed in both groups of cases, including eight cases of salivary fistula and one case of hematoma. Complications did not exclusively occur in cases of infection.
It is noteworthy that subgroup 1, which received pre-operative single-dose antibiotics, had neither infection cases nor any other complications.
Uni-variable analysis and multivariable logistic regression
Uni-variable analysis indicated that the NNIS index and operation duration showed significant differences, suggesting a clear association with the occurrence of SSI (Table 2). Finally, logistic regression analysis was performed, using NNIS index, operation duration ≥2 h, malignant pathology, and diverse antibiotic usage modes as independent variables.
Uni-Variable Analysis of Surgical Site Infection Risk Factors
Statistical method: 1 – Independent samples Chi-square test; 2 – Cochran’s and Mantel-Haenszel statistics; 3 – Mann-Whitney U test.
Fisher exact test was employed.
Results showed a significant difference.
BMI = body mass index; ASA = American Society of Anesthesiologists; NNIS = National Nosocomial Infection Surveillance.
The logistic regression analysis revealed that malignant pathology, surgical duration ≥2 h, and higher NNIS index scores were positively correlated with post-operative SSI rates, and these associations were statistically significant.
All three modes of antibiotic use showed a negative correlation with SSI occurrence. However, pre-operative single-dose use mode (subgroup 1), despite displaying the highest negative correlation, did not reach statistical significance (Table 3).
Results of the Multi-Variable Logistic Regression Analysis for Surgical Site Infection
Antibiotics usage modes: subgroup 1: pre-operative single dose; subgroup 2: peri-operative use within 24 h; subgroup 3: extended use beyond 24 h.
Dummy variables for different antibiotics usage modes were created, with the group not using antibiotics selected as the reference.
OR = odds ratio; NNIS = National Nosocomial Infection Surveillance.
Discussion
Infection after surgery remains one of the common complications following surgical procedures; it not only increases patient suffering and delays recovery but also leads to additional healthcare expenses. 6 In addition to adhering to surgical aseptic principles during procedures, the prudent antibiotic prophylaxis is essential to minimize the risk of post-operative infections.
After accumulating extensive clinical experience over time, preventive measures for post-operative infections have become clear and well-defined, leading to a significant reduction in infection rates. 1 The prophylactic use of antibiotics is one of the measures. The Scottish Intercollegiate Guidelines Network distinguishes antibiotic prophylaxis into two regimens based on whether the duration of use exceeds 24 h. 7 But, some researchers believe that the optimal timing for prophylactic antibiotics is 30–60 min before the start of surgery.8,9 Regardless, the goal of prophylactic antibiotic use is to ensure antibiotics reach the surgical site and maintain sufficient concentrations during the infection risk period, typically not exceeding 24 h, to combat potential pathogens or colonizing microbes.10,11
However, the irrational use of antibiotics continues to be a prevalent concern in clinical settings. 12 The reasons are diverse, occasionally extending beyond the scope of medical necessity itself. Inappropriate prescription can be attributed to various factors, such as patient-requested antibiotics, drug cost-containment policies, pharmaceutical company advertisements, and the inadequacy of physician education in pharmacology. 13
According to the classification standards for surgical incisions, most oral and maxillofacial surgical incisions fall under the categories of clean or clean-contaminated. Existing research has consistently shown that, with the exception of preventing infective endocarditis or in cases of foreign body implantation, prophylactic antibiotics are generally not recommended for the majority of dentoalveolar surgeries. The use of antibiotic prophylaxis for other maxillofacial procedures depends on the classification of the incision and whether it is exposed to the oral or pharyngeal cavity.14–16 However, not all doctors adhere to widely accepted practices, perhaps influenced by non-medical factors. Particularly in surgeries involving incisions like the parotid and submandibular glands, there is a notable incidence of inappropriate antibiotic use.
In parotid surgery, the prophylactic use of antibiotics aims to further reduce the SSI rate. However, this study showed that the use of prophylactic antibiotics did not significantly reduce the incidence of SSI, similar to the findings of Meccariello et al. and Shkedy et al.2,4 Therefore, there is insufficient justification for antibiotic prophylaxis in parotid surgery, regardless of the reasons.
In this study, patients in group 1 received prophylactic antibiotics, with various administration methods. Although this study did not identify specific criteria, there was some discretion in deciding whether to administer prophylactic antibiotics and how to administer them. However, the selection of antibiotics generally followed certain principles: ideally, antibiotics should be highly effective in killing bacteria, possess an optimal spectrum of activity, exhibit good tissue penetration, maintain sustained effective concentrations within tissues, have minimal side effects, and be cost-effective. 17
According to the first part of this study, certain factors showed statistically significant differences between the two groups, indicating that they may serve as the basis for physicians to decide whether to use prophylactic antibiotics. These factors included the NNIS index, surgical duration, and pathological characteristics.
The operation duration is an important component of the NNIS index, and malignant pathology often indicates longer surgical duration. Ultimately, these factors are all correlated with surgical duration. Meanwhile, uni-variable analysis demonstrated a significant association between operative duration ≥2 h and SSI rate, and multi-variable logistic regression analysis indicated that operative duration ≥2 h was an independent variable positively correlated with the SSI rate. Therefore, using surgical duration as a sole criterion to determine prophylactic antibiotic use is reasonable.
In this study, results of uni-variable analysis and logistic regression analysis indicated that higher NNIS index score was another independent risk factor for the occurrence of SSI. Higher NNIS score may be regarded as sole predictor for post-operative SSI.
However, although malignant pathology showed a significant positive correlation with SSI in regression analysis, it did not reach statistical significance in uni-variable analysis, and therefore, cannot be considered a standalone risk factor for SSI.
On the basis of the above analysis, it can be concluded that operation duration ≥2 h and higher NNIS index can serve as predictive risk factors for SSI occurrence and be used as criteria for prophylactic antibiotic administration. Surgical duration can be reduced through more skilled operations and better pre-operative preparation, leading to a decrease in NNIS scores. Perhaps shortening the duration of surgery might reduce the SSI rate.
The current study also suggests that although the use of antibiotics during parotid gland surgery did not significantly affect the overall SSI rate, all three different modes of usage showed a negative correlation with SSI occurrence compared with non-usage, indicating a protective effect to some extent. The protective effect of pre-operative single-dose antibiotic use was the most pronounced. The clinical summaries or prospective studies by other researchers have also indicated that a single dose of antibiotics prior to skin incision in parotid surgery is sufficient to reduce SSI rates, and prolonging the duration of use does not further decrease infection rates.4,18,19 Only a few surgeries lasting longer than 2–3 h may require additional antibiotic administration intraoperatively. 20 The lack of statistical significance in current logistic regression may be attributed to factors such as the small sample size of the single-dose antibiotic subgroup in this study.
The above analysis indicates that it is not appropriate to solely criticize the prophylactic use of antibiotics in parotid gland surgery as overtreatment based on existing guidelines. Instead, a more objective and comprehensive analysis is needed, particularly considering the individual circumstances of each patient. Furthermore, evaluating the benefits of prophylactic antibiotics in parotid surgery requires careful consideration of the risks associated with prolonged use, such as adverse reactions and microbial resistance. Moreover, increased treatment costs should be taken into account. It’s also important to consider non-medical influences on physicians’ decisions regarding antibiotic use. To standardize the appropriate antibiotic prophylaxis in parotid surgery, it remains necessary to adhere to some existing guidelines, such as those provided by the Surgical Care Improvement Project on how to reduce SSIs. 21
This is a retrospective study with some limitations. For example, although this medical institution performs a relatively large number of parotid surgeries, it is still challenging to achieve an ideal sample size. Moreover, various confounding factors can influence the research results. Because the retrospective study includes all compliant cases, there are certain degrees of variability in some patient characteristic information. Despite measures being taken, selection bias is still inevitable. In the future, more persuasive and authoritative conclusions can be drawn regarding antibiotic prophylaxis in parotid region surgeries if a larger sample size is achieved and/or a randomized controlled prospective study is conducted.
Conclusions
This study indicates that prophylactic antibiotic use in parotid surgery does not significantly reduce the occurrence of SSI. Therefore, we recommend adhering to established guidelines and limiting the prophylactic use of antibiotics whenever feasible. If there are compelling reasons for its use, it should be approached cautiously, taking into account patient-specific factors such as elevated NNIS scores and prolonged surgical durations. If a choice of antibiotic usage mode must be made, prioritizing pre-operative single-dose administration is advisable.
Footnotes
Acknowledgments
The authors extend their heartfelt thanks to all the patients who contributed to this study.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Authors’ Contributions
Conceptualization: Wei. Investigation: Wei, Zheng. Writing—original draft: Wei. Methodology: Zhang. Writing—review and editing: Bi. Supervision: Bi. Project administration: Bi. Funding acquisition: Bi.
Funding Information
This work was supported by the Natural Science Foundation of Zhejiang Province, China (grant number TGY24H290014). The funding sources had no involvement in this study.
Author Disclosure Statement
The authors have declared that no competing interest exists.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.