
Abstract
Background:
Emergency laparotomy for abdominal trauma is associated with high rates of surgical site infection (SSI). A protocol for antimicrobial prophylaxis (AMP) for trauma laparotomy was implemented to determine whether SSI could be reduced by adhering to established principles of AMP.
Patients and Methods:
A protocol utilizing ertapenem administered immediately before initiation of trauma laparotomy was adopted. Compliance with measures of adequate AMP were determined before and after protocol implementation, as were rates of SSI and other infections related to abdominal trauma. Univariable and multivariable analyses were performed to determine risk factors for development of infection related to trauma laparotomy.
Results:
Over a four-year period, 320 patient operations were reviewed. Ertapenem use for prophylaxis increased to 54% in the post-intervention cohort. Compliance with individual measures of appropriate AMP improved modestly. Overall, infections related to trauma laparotomy decreased by 46% (absolute decrease of 13%) in the post-intervention cohort. Multivariable analysis confirmed that treatment during the post-intervention phase was associated with this decrease, with a separate analysis suggesting that ertapenem use was an important factor in this decrease.
Conclusions:
Development of a standardized protocol for AMP in trauma laparotomy led to decreases in infectious complications after that procedure.
Surgical site infection (SSI) is a common complication after laparotomy for abdominal trauma.1–5 Antimicrobial prophylaxis (AMP) is an effective practice for reducing SSI rates in patients undergoing high-risk abdominal surgery,6–8 and is recommended for patients undergoing trauma laparotomy, especially for penetrating trauma, even though prospective randomized controlled trials (PRCT) have not been performed to definitively demonstrate its efficacy.9,10
Fundamental principles of AMP for elective surgery include appropriate timing of initial antibiotic administration, appropriate antimicrobial spectrum for the specific procedure, appropriate dosing of agents particularly in obese patients, timely redosing of antibiotic agents during prolonged procedures, and limiting the duration of antibiotic use post-operatively.6–8 Adherence to these principles may be difficult in patients undergoing trauma laparotomy. The surgical site is frequently already contaminated because of skin and soft tissue or intra-abdominal injuries. Antimicrobial prophylaxis may not be timed ideally because of the exigencies of emergency laparotomy. Intra-operatively, prolonged operations or large blood losses may result in sub-therapeutic concentrations of prophylactic agents. Finally, an appropriate agent may not have been administered if a bowel injury was not suspected prior to laparotomy.
Use of protocols or bundles to optimize AMP has been associated with reduction of SSI rates in elective general surgery.12–14 However, there are sparse data regarding use of such protocols to prevent SSI in patients undergoing trauma laparotomy. 15 We therefore developed a protocol for AMP in these patients designed to facilitate adherence with the principles of AMP. The protocol promoted use of ertapenem as the preferred antibiotic for trauma laparotomy, to be given immediately prior to the start of laparotomy, with redosing only if massive blood loss occurred during the procedure. Ertapenem was chosen because of its spectrum of activity, its prolonged half-life, and its demonstrated efficacy for prophylaxis in elective colorectal procedures. 16 We hypothesized that use of this protocol would lead to decreased rates of SSI directly related to exploratory laparotomy in abdominal trauma patients compared to those rates in a patient cohort treated immediately prior to protocol implementation.
Patients and Methods
Consent
The study design and procedures were approved by the Washington University Institutional Review Board. Informed consent was not required for most patients in the study. Patients contacted by telephone after discharge for purposes of this study provided oral consent for interview according to a script approved by the Institutional Review Board.
Inclusion and exclusion criteria
All patients undergoing exploratory laparotomy for trauma at this level one trauma center from November 2009 to October 2013 were evaluated for inclusion in the study. Patients who underwent laparotomy between November 2009 and November 2011 were included in the pre-intervention cohort, and those who underwent laparotomy between December 2011 and October 2013 were included in the post-intervention cohort. Starting in November 2010, all patients were identified prospectively though screening by the research coordinators; prior to that, patients were identified through retrospective review of the trauma database.
Patients were excluded from any analysis if a resuscitative thoracotomy or cesarean delivery was performed in the emergency department, if the initial laparotomy was performed by a non-trauma service, or if the anesthesia record containing details of prophylactic antibiotic administration was missing.
Patients were excluded from analyses of infectious endpoints, but were included in analyses of process endpoints if they died within five days of admission, if laparotomy was delayed more than 24 hours from the time of injury or more than 12 hours from a traumatic bowel perforation, or if they underwent only laparoscopy or wound exploration in the operating room, without subsequent laparotomy
Patients who underwent other operations by the trauma service during the laparotomy, such as thoracotomy or groin exploration for a vascular injury, or who underwent a subsequent procedure by a non-trauma service, such as stabilization of a fracture, were included in all analyses. In the latter patients, the laparotomy procedure was considered finished when the skin was either closed or packed, or, in patients having delayed fascial closure, when a temporary abdominal closure had been fashioned. Patients who underwent minor procedures prior to laparotomy, such as tube thoracostomy or wound explorations were included in all analyses, even if antibiotic agents were administered for these procedures.
Intervention
Prior to December 2011, all AMP for patients undergoing trauma laparotomy was given according to attending surgeon preference. In December 2011, a standardized protocol for AMP agreed to by the trauma surgery and trauma anesthesia services was implemented for these patients. The protocol included use of 1 gm of ertapenem as the antibiotic of choice for all trauma laparotomies, to be delivered upon arrival in the operating room prior to incision. This antibiotic was to be given regardless of whether or not the patient received an antibiotic while in the emergency department; administration of antibiotic agents in the emergency department was strongly discouraged. Patients who had a documented carbapenem allergy, or who had had an anaphylactic reaction to a β-lactam antibiotic could receive alternative antibiotic agents considered appropriate by the attending surgeon. The protocol also called for re-dosing of ertapenem after 10 units of red blood cells had been transfused since the previous dose. It was recommended that no post-operative antibiotic agents be administered, but if given, they were limited to 24 hours after the operation except for patients undergoing delayed fascial closure, in whom antibiotic duration was left to surgeon discretion.
Data collection
Basic demographic, injury severity, and clinical data were collected on all patients, including age, gender, race, medical comorbidities, prior abdominal operations, mechanism of injury, lactic acid values, abdominal and extra-abdominal injuries, Injury Severity Score (ISS), abdominal ISS, calculated probability of survival, duration of laparotomy, number of units of blood transfused, whether or not delayed fascial closure was used, and whether or not the skin was closed at the time of the final abdominal procedure.
Post-operative data were obtained regarding temperature and leukocyte counts, administration of antimicrobial agents, culture results, imaging studies to investigate for infection, and all other operative or other procedures. All available records were utilized, including initial and subsequent hospital admissions, outpatient encounters, emergency department visits, and ancillary home health visits. Interactions were evaluated in detail up to 30 days after initial laparotomy, and additional information from 30 to 90 days after laparotomy was reviewed, if available.
In selected cohorts of patients during the pre-intervention and post-intervention phases of the study, an attempt was made to contact them by phone after 30 days if the final encounter was less than 30 days after laparotomy. This was done between November 2010 and June 2011 for the pre-intervention cohort and between November 2012 and October 2013 for the post-intervention cohort. Patients contacted by phone were asked whether or not they had had any further medical interventions, complications related to trauma, or antibiotic prescriptions since their last encounter.
Process endpoints
Antimicrobial prophylaxis was characterized according to timing of initial administration, dosage, spectrum of activity, redosing for length of operation or blood loss, duration of prophylaxis, and whether additional antibiotic agents were administered pre-operatively. Definitions of endpoints are shown in Table 1.
Definitions of Process Endpoints
AMP = antimicrobial prophylaxis.
Process endpoints were evaluated in all patients included in the study, including those excluded from infection endpoints. The primary process endpoint was the proportion of patients who were compliant with all standards related to prophylaxis during the first trauma laparotomy, including initial timing, dosage, antibiotic selection, and re-dosing for length or operation and blood loss. Secondary endpoints were the proportion of patients compliant with each individual standard. Additional secondary endpoints were the proportion of patients who received extra pre-operative antibiotic therapy, and the proportion compliant with discontinuation of prophylactic antibiotic agents at the end of laparotomy or within 24 hours of laparotomy.
Infection endpoints
Definitions for infections were developed prior to study initiation and are shown in Table 2. The primary endpoint for the study was the number of patients who sustained an infection directly related to the abdominal trauma within 30 days of laparotomy. This expanded endpoint was primarily related to incisional and intra-abdominal infections, but also included other infections that were directly associated with the abdominal trauma. Thus, infections in a thoracic cavity directly contaminated because of a thoraco-abdominal gunshot injury, or a soft tissue infection in the operative field related to an abdominal injury were included in this expanded endpoint. Subsequent pneumonias, urinary tract infections (UTIs), soft tissue infections away from the abdominal region, or bacteremias were not considered related infections. Secondary endpoints included the number of patients with an SSI, intra-abdominal infection (IAI), or any other type of infection at 30 days. Similar endpoints were assessed up to 90 days after laparotomy. Patients who lacked follow-up data at 30 or 90 days were assumed to have not had an infection if none had been documented at the time of the last available encounter. Data at 90 days were excluded in two patients because of a late death in one and a new trauma laparotomy in the other. All infections were identified through the medical records; no additional infections were uncovered in patients contacted via telephone.
Definitions of Infection Endpoints
SSI = surgical site infection; NHSN = National Healthcare Safety Network; IAI = intra-abdominal infection; SSTI = skin and soft tissue infection; CT = computed tomography; UTI = urinary tract infection.
Statistical analysis
Prior to initiation of the study, a power analysis indicated that approximately 106 patients would be needed in each group to detect a 25% decrease in the primary infection endpoint, based on an estimated 20% incidence of these infections in control patients. Based on usual numbers of laparotomies and potential exclusion of 10% of patients, it was estimated that 18 to 24 months would be required for each phase of the study.
The primary analyses were process and infection infectious endpoints in the pre- and post-intervention cohorts. Secondary analyses compared these outcomes in patients who received or did not receive ertapenem as their peri-operative antibiotic, regardless of cohort.
Data were presented as mean with standard deviation or median with interquartile ranges for quantitative variables, as appropriate, and frequency with percentage for qualitative variables. Two-sample t-test or Wilcoxon rank sum test was used to assess the differences of numeric factors (i.e., age, weight) between pre- and post-intervention cohorts, as appropriate. Either χ 2 test or Fisher exact test was used to assess the differences of primary/secondary outcomes between pre- and post-intervention cohorts, as appropriate. Univariable and multivariable logistic regression analyses were performed to detect the effects of demographic and clinical factors on primary outcomes. Odds ratios with 95% confidence intervals were provided to describe the magnitudes of the effects. Data were analyzed by SAS 9.4 (SAS Institute Inc, Cary, NC). A p value <0.05 was considered statistically significant.
Results
Patients and exclusions
A total of 320 operations for abdominal trauma in 309 patients were performed over the four-year study period. Except for one patient who underwent 12 separate procedures for recurrent self-inflicted stab wounds, no patient was entered into the database more than once. After exclusions, there were 158 patient operations in the pre-intervention cohort and 151 patient operations in the post-intervention cohort that were analyzed for process endpoints. After further exclusions, there were 139 patients in the pre-intervention cohort and 126 patients in the post-intervention cohort who were evaluable for infection endpoints. The reasons for exclusions are detailed in Figure 1.
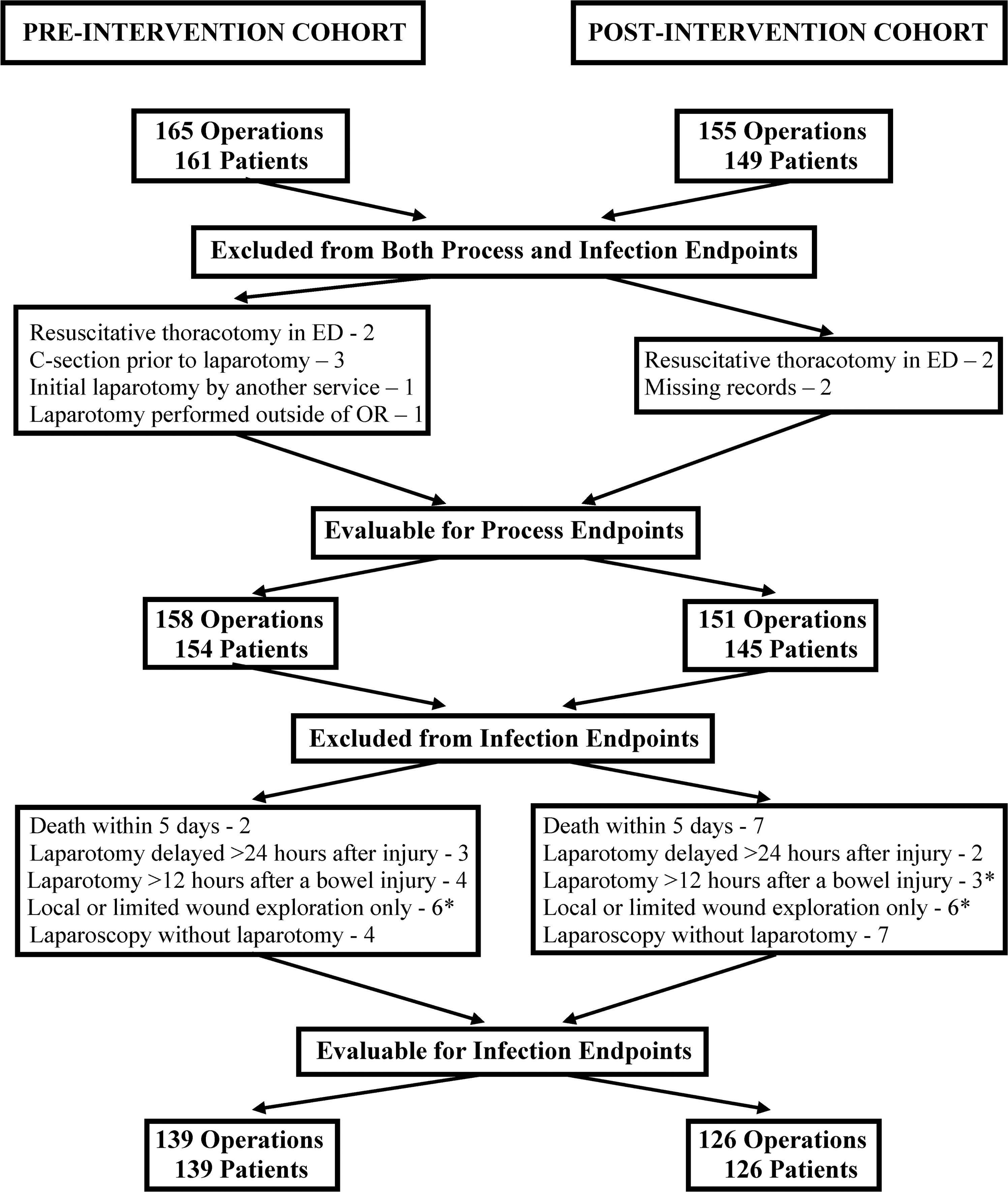
Patients excluded from analysis of process endpoints and both process and infection endpoints. *One patient was excluded five times in both the pre- and post-intervention cohorts for undergoing a local or limited wound exploration only, and twice in the post-intervention cohort for undergoing laparotomy more than 12 hours after a bowel injury. ED = emergency department; OR = operating room; C-section = cesarean delivery.
Compliance with the protocol
Ertapenem use for AMP increased from 2.5% of laparotomies during the pre-intervention phase to 54.3% of laparotomies during the post-intervention phase. This was associated with a concomitant decrease in the use of cefoxitin, cefazolin, or any cephalosporin in the post-intervention cohort (Table 3). During the first five months of the post-intervention phase, only 10% of patients (3/30) received ertapenem. After re-education of anesthesia and surgical personnel regarding the AMP protocol, ertapenem was used for AMP in 65% of patients (79/121; p < 0.001) during the final 18 months of the post-intervention phase. Nonetheless, use of ertapenem never exceeded 80% in any one quarter of the post-intervention phase, primarily because of a decision of the surgical or anesthesia provider to use an alternative regimen. This decision was because of a reported β-lactam allergy in only three of the 69 patients in whom ertapenem was not used.
Antibiotic Agents Used for Prophyaxis
Ampicillin/sulbactam, 1; piperacillin/tazobactam, 4; ciprofloxacin ± metronidazole or clindamycin, 4; vancomycin + metronidazole, 1.
Piperacillin/tazobactam, 1; ciprofloxacin ± metronidazole or clindamycin, 2; vancomycin, 1.
Antimicrobial prophylaxis usage was assessed for timely administration of the initial dose, antibiotic selection, correct initial dosage, and timely redosing for duration of laparotomy or large blood loss (Table 4). Overall compliance with these measures improved from 49% to 62% between the pre- and post-intervention cohorts. However, there were no statistically significant differences in any of the individual measures. Increased compliance in the post-intervention cohort was primarily because of fewer patients being at risk for non-compliance because of incorrect dosing, inadequate spectrum of activity, and failure to re-dose AMP for a prolonged procedure.
Compliance with Measures of Appropriate AMP Use
AMP = antimicrobial prophylaxis.
p = 0.033 comparing number of patients at risk in the pre- versus the post-intervention cohorts.
p = 0.019 comparing number of patients at risk in the pre- versus the post-intervention cohorts.
p = 0.001 comparing number of patients at risk in the pre- versus the post-intervention cohorts.
Pre-operative and post-operative use of antibiotic agents also declined with implementation of the protocol. Extra pre-operative administration of antibiotic agents (primarily in the emergency department), declined in the post-intervention cohorts, as did administration of any post-operative AMP or any AMP given for greater than 24 hours after laparotomy (Table 5).
Pre-Operative and Post-Operative Antibiotic Use
Ertapenem was used for AMP in this protocol to obviate necessity for dose adjustment for patient weight, addition of a second agent to the regimen to provide anti-anaerobic activity, or redosing for a prolonged procedure. When analyzed according to the actual antibiotic used, 75 of 86 patients who received ertapenem (87%) were compliant with all measures, compared with 100 of 199 patients who received any other antibiotic agent (50%; p < 0.001). Use of cefazolin or any cephalosporin was negatively associated with compliance (data not shown). A multivariable logistic regression analysis confirmed that ertapenem use was positively associated with improved compliance (data not shown).
Patient characteristics
The demographic and injury patterns of patients in the pre-intervention and post-intervention cohorts assessed for infection endpoints are shown in Table 6. Patients were well-matched for most characteristics. The only significant difference identified was a greater number of patients in the post-intervention cohort who had colorectal injuries. Follow-up was similar for patients in the two cohorts (Table 6). Overall, more than 70% of patients had follow-up 30 days or more after injury and 30% of patients had follow-up 90 days or more after injury.
Comparisons of Pre- and Post-Intervention Cohorts
SD = standard deviation; ISS = Injury Severity Score ; IQR = interquartile range; ED = emergency department; PRBCs = packed red blood cells; ICU = intensive care unit.
Infections
The primary endoint of the study (percentage of patients having an infection directly related to abdominal trauma at 30 days) declined from 27% (37/139) in the pre-intervention cohort to 14% (18/126) in the post-intervention cohort (Table 7). This represented an absolute decrease of 13% and a relative decrease of 46% in infections directly related to trauma laparotomy. This resulted in an overall relative decrease of 26% in the percentage of patients sustaining any infection, although this change just missed statistical significance. Results at 90 days were similar to those at 30 days, with the exception that the decrease in overall infections reached statistical significance in this analysis.
Infections in Pre- and Post-Intervention Cohorts
SSI = surgical site infection; SSTI = skin and soft tissue infection; UTI = urinary tract infection.
Patients in either cohort may have had more than one type of infection.
Pre-intervention cohort: ocular infection, 1; post-intervention cohort: osteomyelitis, 2; Meningitis, 1.
Pre-intervention cohort: ocular infection, 1; osteomyelitis, 1; post-intervention cohort: osteomyelitis, 2; meningitis, 1.
The types of infections patients in both cohorts sustained are shown in Table 7. There was a statistically significant decrease in the incidence of SSI in the post-intervention cohort, primarily due to a decrease in superficial SSI at both 30 and 90 days. Deep SSI, organ/space infections, and most other related infections declined among patients in the post-intervention cohort, although these decreases did not reach statistical significance. There were fewer patients with unrelated infections in the post-intervention cohort, but this did not reach significance except for primary blood stream infections at 90 days; this difference may have reflected misclassification, since the overall number of patients with blood stream infections (both primary and secondary) was not significantly different at 90 days (12 in the pre-intervention cohort, 7 in the post-intervention cohort; p = 0.332). Five patients developed Clostridiodes difficile-associated disease (CDAD) in the pre-intervention cohort whereas none did in the post-intervention cohort, although this difference did not reach statistical significance. Among the patients who developed CDAD, four of the five received a cephalosporin for AMP.
Univariable and multivariable analyses were performed to determine factors that increased the risk of a related infection. In univariable analysis, multiple risk factors were identified, which tended to segregate into two groups: those related to the severity of injury, such as a penetrating mechanism of injury, a higher ISS or abdominal ISS score, a colorectal or any gastrointestinal tract injury, a larger number of units of blood transfused, and fascia being left open at the end of the initial procedure; and those related to prophylactic antibiotic administration, including an operation prior to protocol implementation, non-compliance with measures of appropriate antibiotic use, longer post-operative use of prophylactic antibiotic agents, and use of an antibiotic other than ertapenem for prophylaxis (Table 8). Multivariable logistic regression of these risk factors revealed that laparotomy prior to protocol implementation was strongly associated with the risk of a related infection; additional risk factors included a penetrating mechanism of injury, ISS score, a colorectal injury, and the number of units of PRBCs transfused (Table 9).
Univariable Analysis of Risk Factors for Related Infection at Thirty Days
SD = standard deviation; ISS = Injury Severity Score ; IQR = interquartile range; ED = emergency department; PRBCs = packed red blood cells; ICU = intensive care unit.
For categorical factors with more than two subgroups, a global p value was presented for the relation between the factor and outcome; individual p values are presented for each odds ratio.
Odds ratio with 95% confidence interval was presented to measure the odds of having infection of the subgroup compared with the reference group, or the odds of having infection per one unit increase of the numeric factor.
Ampicillin/sulbactam, 1; piperacillin/tazobactam, 2; ciprofloxacin + metronidazole or clindamycin, 3.
Piperacillin/tazobactam, 2.
Multivariable Logistic Regression for Any Related Infection at Thirty Days
OR = odds ratio; CI = confidence interval; ISS = Injury Severity Score; PRBCs = packed red blood cells.
Secondary analyses were performed to explore whether ertapenem use contributed to the decreased risk of related infection after protocol implementation. Ertapenem use was associated with significant relative decreases of 49% and 46% in the number of patients who sustained a related infection at 30 and 90 days (Table 10). Although trends toward a decrease in overall infections were seen at both 30 and 90 days, these numbers did not reach statistical significance. When patient cohort was excluded, a multivariable logistic regression analysis showed that ertapenem use was strongly associated with a statistically significant decline in the number of patients with a related infection at 30 days (Table 11).
Infection Outcomes with Use of Ertapenem
Some patients in each group had both a related and an unrelated infection.
Multivariate Logistic Regression for Any Related Infection at Thirty Days, Excluding Cohort
OR = odds ratio; CI = confidence interval; PRBCs = packed red blood cells.
Other outcomes
Nine patients died from their injuries, all of whom were excluded from analysis of infection endpoints. There were no other patient deaths in either cohort at 30 days, although one elderly patient in the post-intervention cohort died more than 30 days after laparotomy at a long-term acute care facility from non-infectious causes. The number of hospital days, intensive care unit (ICU) days, and ventilator days did not differ significantly between the two cohorts, but the number of patients discharged to a long-term or skilled nursing facility was higher in the pre-intervention cohort, nearly reaching statistical significance (p = 0.0504). Overall days of anti-infective agent use were decreased in the post-intervention cohort, as were days of inappropriate antimicrobial use (Table 12).
Other Outcomes
IQR = interquartile range; ICU = intensive care unit
Discussion
Various series of infection after trauma laparotomy have documented rates of infection of 7.1% to 28.4% for superficial and deep SSI and 7.9% to 25.2% for IAI after trauma laparotomy.1–5 In a review of PRCTs on AMP for trauma laparotomy, rates of SSI and IAI were 18.4% and 8.6%, respectively. 5 In a previous analysis, we found that 31% of patients had infections directly related to laparotomy. 17
Given the high incidence of these infections, this study was undertaken to determine if a protocol designed to facilitate optimal use of AMP for trauma laparotomy, based on established principles for AMP for elective surgical procedures, could decrease this incidence. Important considerations were that tissue levels of the antibiotic should be maintained throughout trauma laparotomy, and that the agent selected have coverage of the organisms expected to contaminate the abdomen in these patients. Prior to protocol development, cefazolin and cefoxitin were the most common agents utilized for prophylaxis in patients undergoing trauma laparotomy. These were frequently administered in the emergency department prior to transport to the operating room. This resulted in a number of deviations from recommended processes used for AMP. Occasionally, the prophylactic agent was administered more than one hour before the operative incision was made. There were also failures to utilize larger dosages in obese patients, to re-dose the agent when the operative time exceeded two half-lives of the agent administered, and to include anaerobic coverage when a bowel injury was present.
To simplify the process of antibiotic selection, the protocol specified use of ertapenem as the preferred agent because of its prolonged half-life and spectrum of activity including anaerobic organisms. To ensure adequate drug levels, the protocol also specified that the drug was to be delivered in the operating room by the anesthesia team immediately prior to the start of the operation. The antibiotic was to be re-dosed in the event of blood loss exceeding one blood volume, based on use of blood products for patients placed on the massive transfusion protocol. Ertapenem re-dosing was otherwise recommended only if the duration of the laparotomy exceeded six hours. Unless there had been an anaphylactic reaction to a penicillin or cephalosporin, ertapenem could be used in patients with a reported history of a β-lactam allergy. No recommendation was made regarding antibiotic prophylaxis for a subsequent extra-abdominal procedure carried out by another service after trauma laparotomy. Antibiotic agents given for trauma laparotomy were to be discontinued within 24 hours after the end of the operation, with a preference for no antibiotic agents to be given post-operatively; however, no recommendation was made regarding duration of prophylaxis for patients whose abdominal fascia was left open after damage control laparotomy.
The primary endpoint for the study was the proportion of patients who developed a post-operative infection directly related to the abdominal trauma within 30 days of injury. A decrease of 46% in the percentage of patients sustaining these infections was noted. This was statistically significant and in excess of the predicted 25% decrease that had been hypothesized as part of the study design and sample size calculations. The multivariable analysis identified being part of the post-intervention cohort as a highly significant factor in the reduced rates of infections. With regard to specific infection type, the decrease was significant for superficial SSI or the combination of superficial and deep SSI. However, decreases were also seen in the incidence of more serious infections, including organ/space infections, although these did not reach statistical significance, in part because of their lower frequency.
Another goal of this study was to determine if compliance with measures thought important for optimal antimicrobial prophylaxis would be improved through use of the protocol. Although a statistically significant improvement in compliance with all measures was observed in the post-intervention cohort, no improvement was noted for compliance for any individual measure. Overall compliance was improved because fewer patients in the post-intervention cohort were at risk for failure to adjust dosing for obesity, to use a supplemental anti-anaerobic agent, or to re-dose for the length of the procedure. Implementation of the protocol also was associated with some improvements in antimicrobial stewardship. There was decreased utilization of extra pre-operative antibiotic agents in the emergency department prior to trauma laparotomy, and decreased use of prophylactic agents in the post-operative phase, with only 10% of patients, primarily those undergoing delayed fascial closure, receiving prophylactic agents for more than 24 hours.
Failure to use ertapenem as the preferred antibiotic in patients in the post-intervention cohort was quite frequent. The study called for roll-out of the protocol in November 2011, which ultimately had to be delayed for one month due to logistical issues. Prior to implementation, the protocol was not disseminated to avoid premature use of ertapenem in the pre-intervention cohort. However, this resulted in poor compliance with ertapenem administration during the first several months the protocol was in effect, because many anesthesiologists were unaware that ertapenem was the preferred agent. Compliance improved with further educational efforts, but there remained a reluctance on the part of some to use ertapenem for all trauma laparotomy, making compliance with ertapenem administration only 65% after renewed educational efforts.
Nonetheless, ertapenem use appeared to be a factor in reducing the number of patients with SSI and other related infections in the post-intervention cohort. A secondary analysis comparing patients receiving ertapenem with those who did not demonstrated virtually the same results as the comparison of patients in the pre-intervention and post-intervention cohorts. Moreover, the multivariable analysis of infection risk regardless of cohort demonstrated that ertapenem use was highly associated with a decreased risk of infection.
Studies of prophylaxis of elective colorectal surgery have suggested ertapenem use is more efficacious than some other agents. In a PRCT, ertapenem appeared to be superior to cefotetan for prevention of SSI. 16 In a large population-based analysis, ertapenem use was associated with fewer SSI than cefoxitin and cefotetan. 18
Alternatively, however, the development of the protocol and its implementation could have led to the decreased rate of infections in the post-intervention cohort. Apropos to this, Dellinger 19 has suggested that fostering teamwork and collaboration among the surgical team may be more important than specific measures in reducing rates of SSI.
There are a number of limitations to this study. The principal one relates to study design, being a before/after trial and not a randomized trial. No important changes were made in treatment approaches during the years of the study to our knowledge. Although there may have been a modest increase in the use of minimally invasive approaches in the post-intervention cohort, these patients were excluded from infection endpoints, and would not favorably influence infection rates in the post-intervention cohort. The risk factors identified in the multivariable analysis were fairly evenly distributed between the two cohorts; the only statistically significant difference was a higher number of patients with colorectal injuries in the post-intervention cohort, which would have favored the pre-intervention cohort. Ascertainment of infection could introduce a bias into the study because the investigators were not blinded to patient assignment. We attempted to avoid bias by having all patient records reviewed independently by a study coordinator and principal investigator to determine if an infection had occurred, utilizing criteria developed prior to the start of the study. To the extent possible, the study coordinators concurrently reviewed all study patients for any diagnosis of infection while they were in the hospital. In the event of ambiguity or disagreement between the principal investigator and the study coordinator with regard to the diagnosis of an infection, a second clinician reviewed the information. If there was disagreement between the clinicians, a third clinician reviewed the clinical information to make the final decision. The second and third reviewers were kept blinded to treatment assignment.
Conclusions
In this study, adoption of a protocol for standardized AMP in patients undergoing laparotomy for abdominal trauma was associated with a decrease in the risk of infectious complications directly related to that procedure. This result was obtained despite incomplete compliance with the protocol. The protocol had been designed specifically to facilitate adherence with established principles of AMP. For this study, ertapenem appeared to be a good choice for the prophylactic agent, although other agents might have produced similar results if included in the protocol. Overall, the development of this coordinated process to optimize AMP in this group of patients at high risk for SSI led to declines in this complication. This reinforces the concept that development of specific protocols emphasizing team-based approaches to optimize patient care can lead to improvements in outcomes.
Footnotes
Acknowledgments
The authors would like to express their appreciation to the other members of the Section of Acute and Critical Care Surgery who have contributed their clinical and investigational expertise to this research project.
We also acknowledge the contributions of Hongjie Gu from the Division of Biostatistics in analyzing the data.
Authors' Contributions
Conceptualization: Mazuski. Methodology: Mazuski. Validation: Mazuski, Symons. Formal analysis: Mazuski, Symons. Investigation: Mazuski, Symons, Jarman, Sato, Carroll, Bochicchio, Kirby, Schuerer. Data curation: Mazuski, Symons, Jarman, Sato. Writing–original draft: Mazuski, Symons. Writing–review and editing: Mazuski, Symons, Kirby, Schuerer. Supervision: Mazuski.
Project administration: Mazuski. Funding acquisition: Mazuski. Resources: Bochicchio.
Funding Information
Supported in part by an Investigator Initiated Studies Program Grant #37280 from Merck and Co.
Author Disclosure Statement
No financial conflicts of interest have been reported by the authors other than grant support provided by Merck and Co.