
Abstract
Background:
To construct a prediction model based on the clinical characteristics of epidermoid cysts to identify pathologic infections, evaluate the diagnostic accuracy of the model, and conduct preliminary verification.
Patients and Methods:
We conducted a retrospective analysis of 314 patients diagnosed with epidermoid cysts that had been removed surgically. The clinical and pathologic data of all patients were collected. The patients were divided randomly into modeling group and verification group in a 75:25 ratio. In the modeling group, the multifactor logistic regression method was used to construct a prediction model for identifying epidermoid cyst pathologic infection, and the receiver operating characteristic (ROC) curve was used to evaluate the diagnostic accuracy of the model, which was then validated in the verification group.
Results:
All 314 patients with epidermoid cysts were divided into non-infected group (183 cases) and infected group (131 cases) according to the pathologic results. Logistic regression analysis showed that the disease course, growth trend, redness, and texture of epidermoid cysts were independent factors affecting pathologic infection. The above four indicators were selected to construct the prediction model of epidermoid cyst pathologic infection. In the modeling group, the prediction model showed an area under the curve (AUC) of 0.898, with the sensitivity of 0.830, specificity of 0.890, positive likelihood ratio of 7.523, and negative likelihood ratio of 0.191. The AUC of the prediction model in the verification group was 0.919, which was not significantly different from that of the modeling group (p = 0.886).
Conclusions:
The prediction model based on the clinical characteristics of epidermoid cysts had good diagnostic accuracy and high specificity; it can be used to identify pathologic infections of epidermoid cysts.
Epidermoid cysts are a common skin inflammatory disease, which mostly occurs in young people. The cyst is highly enriched in keratin, which is arranged in a ring-like layer; its outer layer is wrapped by lamellar squamous epithelium or non-lamellar squamous epithelium. 1 Most epidermoid cysts are located in the dermis, some protrude to the superficial fascia layer, and a few epidermoid cysts on the hip can reach the muscle layer. The true epidermoid cyst has no skin appendages on the wall, and mostly occur on the face, neck, peri-ear area, and upper trunk, however, nipple, genitals, and palm areas may also be affected. Most epidermoid cyst lesions are spontaneous, but some could be caused by genetic factors, especially in individuals with multiple lesions. For example, in Gorlin syndrome, 1% of epidermoid cysts transformed into squamous cell carcinoma and basal cell carcinoma. 2
Some imaging examinations are used to evaluate the conditions of soft tissue masses. Ultrasound and magnetic resonance imaging (MRI) can be used to assess the anatomic position of the mass and its relation to surrounding structures; these techniques can also reveal the characteristics of the mass, including echo, size, edge, and the nature of the mass,3–5 all of which greatly improve the accuracy of epidermoid cyst diagnosis.
Most epidermoid cysts grow slowly and appear as painless subcutaneous masses, which are mostly ignored by patients. The fact that these cysts are benign could suggest a conservative management with planned follow-up.6,7 However, as time passes, epidermoid cysts tend to expand and some patients actively seek treatment because of health concern and cosmetic needs. In addition, once the cyst is infected, it will grow rapidly, and intervention is necessary. At present, surgical treatment is still the only radical treatment. For uninfected cysts, the whole cyst wall can be removed easily, and the surgery often results in minimal scarring and low recurrence rate, which can satisfy the patients. On the contrary, the infected cyst wall is highly fragile and ruptures easily during the infection, which leads to the spread of its contents and the formation of severe adhesions. Therefore, it is difficult to remove the infected cyst completely and the rate of residual cyst wall increases.
There is no doubt that the risk of cyst recurrence and local scars also increases after surgery. If the infection is severe and cysts are ruptured, abscesses can form, which may further cause skin ulceration. In this case, the wound is difficult to heal by itself and often requires incision, drainage, and long-term dressing changes, which prolongs the disease course; a second operation might be necessary. In addition, postponed surgery can lead to prolonged treatment time, increased medical costs, and cosmetic and functional impairment. Therefore, if the susceptible cases can be identified early, and the wound can be closed via the resection method combining sharp and blunt dissection, patients can often achieve stage 1 healing. 8 Especially for facial cysts, early resection will not affect the appearance.
The gold standard for diagnosing cyst infection is pathologic examination. However, the imaging methods including ultrasound and MRI still lack the relevant parameters to assess infection accurately; moreover, these examinations are usually performed repeatedly, which increases economic burden for patients. So far, most current studies focus on the improvement of treatment method after the occurrence of infection events, but few studies discuss the prediction of infection before cyst resection, 9 and early prediction of infection can help patients choose proper treatment strategies. This study analyzed retrospectively the clinical characteristics of patients with epidermoid cyst and the morphologic characteristics of the mass and constructed a prediction model for identifying epidermoid cyst infection, to improve the predictive accuracy for the pathologic infection of epidermoid cyst.
Patients and Methods
Clinical data
This study analyzed retrospectively patients who were diagnosed with epidermoid cysts that had been surgically removed from July 2018 to August 2019. The inclusion criteria included: patients met the clinical diagnostic criteria of epidermoid cyst; the lesion had been surgically removed; the epidermoid cyst was confirmed by pathologic diagnosis. The exclusion criteria were: basic information and pathologic data were incomplete; severely infected epidermoid cyst that could not be completely surgically removed and required multiple dressing changes; patients with epidermoid cysts in internal organs and skull; patients with infectious diseases; patients with immune system disease, or had recently taken oral and intravenous antibiotic agents; and patients with nephropathy and renal insufficiency.
The following data were collected from each patient: age, gender, cyst morphology and structural characteristics (maximum diameter, shape, location, disease course, growth trend, redness, pain, fluctuating sensation, itching, skin damage, higher skin, texture), and post-operative pathologic results. Growth trend is limited to seven days. Epidermoid cysts that grow quickly within seven days are considered as rapid growth, and those that grow in more than seven days are considered as gradual growth. Because this was a retrospective analysis, it did not require the consent of patients nor the approval of the ethics committee.
Surgical treatment
All patients received epidermoid cyst excision under local infiltration anesthesia, with 2% lidocaine and 1:200,000 epinephrine. The surgery procedure was as follows. The incision opening point on the cyst skin was determined according to the size of the mass, and the incision direction along the dermatoglyph was determined. Afterwards, a narrow fusiform incision including the opening point was made, and the skin was separated along the surface of the mass. If the mass envelope was intact, it could be peeled off as a whole. If the mass was infected and ruptured, the mass was removed along with the surrounding normal tissues to ensure that no cyst contents remained in the surgical field. When the opening was not visible, the suspicious area was also resected. All excised tissues were sent for pathologic examination.
Criteria for pathologic infection
The excised surgical specimens were used for pathologic examination. There are lymphocytes, neutrophils, macrophages, plasma cells, and other inflammatory cells infiltrated in the interstitium. Patients with acute infection were mainly infiltrated by lymphocytes and neutrophils, 10 whereas patients with chronic infections were mainly infiltrated by macrophages and plasma cells.
Statistical analysis
For continuous data, the normally distributed variables were expressed as mean ± standard deviation (SD), and the non-normally distributed variables were expressed as P50 (P25, P75). Categorical variables were expressed as frequency (%). For continuous variables, unpaired Student t-test or Mann-Whitney non-parametric test was used to compare between groups; and for categorical variables, Pearson χ 2 test or Fisher exact test was used for comparison between groups.
The multifactor logistic regression method was used to establish a prediction model, and the optimal model parameters were selected according to the minimal Akaike's information criterion (AIC), using the bootstrap re-sampling (times = 500) method recommended by the TRIPOD report specification to verify the model internally. The odds ratio (OR) and 95% confidence interval (CI) were calculated. The nomogram of prediction model was plotted, which can visually display the prediction results of each patient. In addition, the calibration curve was plotted to show the prediction accuracy of the nomogram. The receiver operating characteristic (ROC) curve of the prediction model was plotted, and the area under the curve (AUC) and its 95% confidence interval were calculated. The z statistic, Hanley, and McNeil programs were used to compare the AUC of modeling group and verification group. 11 All statistical analysis was performed using R 3.4.3 software package. All statistical tests were two-sided, and p < 0.05 was considered statistically different.
Results
Comparison of baseline data between modeling group and verification group
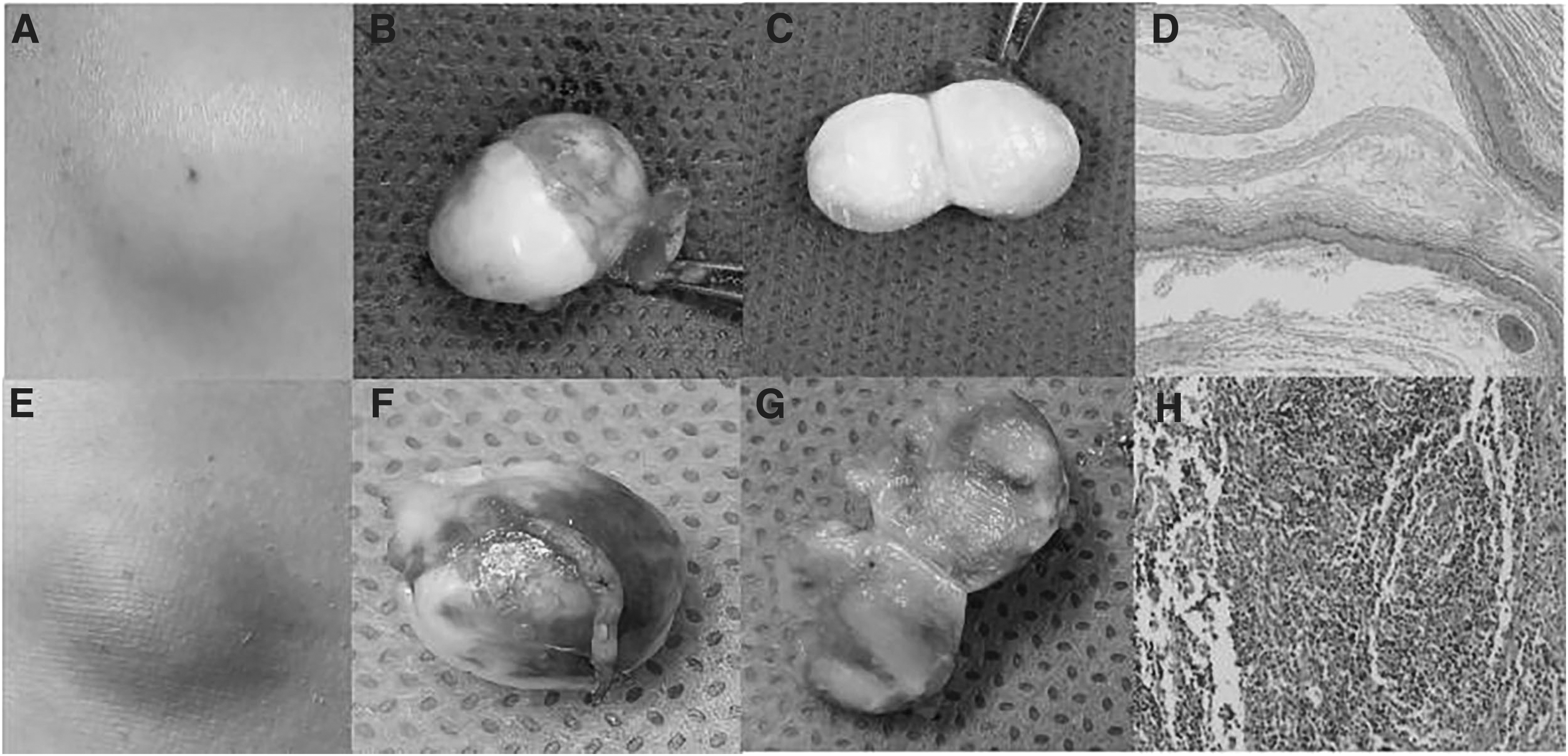
This study included 314 patients with epidermoid cysts, including 201 males and 113 females, with an average age of 48.3 ± 17.5 years. Among all patients, males accounted for 64.0% (201/314); most cysts were round/quasi-circular, accounting for 76.8% (241/314); head and neck cysts accounted for 41.4% (130/314), chest and abdomen cysts accounted for 27.1% (85/314), and limb cysts accounted for 29.9% (94/314). Disease course longer than 30 days accounted for 77.4% (243/314); for symptoms, 24.5% (77/314) had redness and swelling, 25.5% (80/314) had pain, 4.5% (14/314) had itching, 5.7% (18/314) had fluctuating sensation, 26.4% (83/314) had broken skin, and 82.2% (258/314) had masses higher than skin (Fig. 1); 298 patients underwent incisions and the whole tissue was removed, achieving stage 1 healing.
(
Although 16 patients underwent wound expansion, incision and drainage, multiple dressings, and wounds reached stage 2 healing in four to six weeks. All patients were divided randomly into the modeling group (230 cases) and the verification group (84 cases) by split-sample function of R software at a 75:25 ratio. According to post-operative pathologic results, all patients were divided into infection group (131 cases, 41.7%) and non-infection group (183 cases, 58.3%). The comparison of baseline data between the two groups is shown in Table 1. There was no statistical difference in the clinical data and epidermoid cyst morphologic parameters between the modeling group and verification group (all p > 0.05).
Comparison of Baseline Data Between Modeling Group and Verification Group
D set = modeling group; V set = verification group; WBC = white blood cell.
Comparison of infected and non-infected patients in the modeling group
The proportions of epidermoid cyst cases with redness, swelling, pain, and toughness were higher in the infected group than that in the non-infected group (p < 0.001), and the number of cases with disease course longer than three years was higher than that in the infected group (p = 0.001). There was no difference between the two groups in age, gender, maximum diameter of cyst, shape, location, growth trend, fluctuating sensation, itching, skin damage, higher than skin, etc. (all p > 0.05; Table 2).
Single-Factor Analysis of the Clinical Characteristics and Epidermoid Cyst Features of Infected and Non-Infected Patients in Modeling and Verification Group
WBC = white blood cell.
Construction and verification of a multifactor model based on epidermoid cyst characteristics
By using pathology result as the dependent variable, and 15 indicators of clinical and morphologic characteristics of cysts as independent variables, we performed a binary multivariable logistic regression analysis, and established a regression model to obtain the independent factors distinguishing epidermoid cyst infection, odd ratio value, and 95% confidence. The results are shown in Table 3. The disease course, growth trend, swelling, and texture of epidermoid cysts were the independent factors predicting pathologic infection. The formula of the prediction model is: Logit(P) = −1.277–0.551 × [(<30 day) = 1] −0.436 × [(30 day to 3 month) = 1] − 1.439 × [(3 month to 3 year) = 1] − 2.630 × [(>3 year) = 1] + 0.884 × (gradual enlargement = 0, rapid enlargement = 1) + 2.604 × (no redness = 0, yes = 1) − 1.639 × (soft quality = 0, toughness = 1) −0.581 × (softness = 0, hardness = 1).
Multivariable Analysis of Independent Influencing Factors for Epidermoid Cyst Infection in Modeling Group
OR = odds ration; CI = confidence interval.
The ROC curve of the prediction model in modeling group was plotted. The AUC was 0.898 (95% CI, 0.853–0.943), with a sensitivity of 0.830, specificity of 0.890, positive likelihood ratio of 7.523, and negative likelihood ratio of 0.191. The ROC curve of the prediction model in verification group was also plotted. The AUC was 0.919 (95% CI, 0.862–0.976), with a sensitivity of 0.892, specificity of 0.787, positive likelihood ratio of 4.192, and negative likelihood ratio of 0.137. There was no difference in the diagnostic accuracy of the prediction model between modeling group and verification group (AUC, 0.898 vs. 0.919; p = 0.886; Fig. 2). The diagnostic performance of the predictive models in the modeling group and the verification group was better than that by the single factor index white blood cell (WBC) count and neutrophil ratio (AUC, 0.898 vs. 0.558 vs. 0.555; AUC, 0.919 vs. 0.518 vs. 0.537; p ≤ 0.001; Fig. 3).
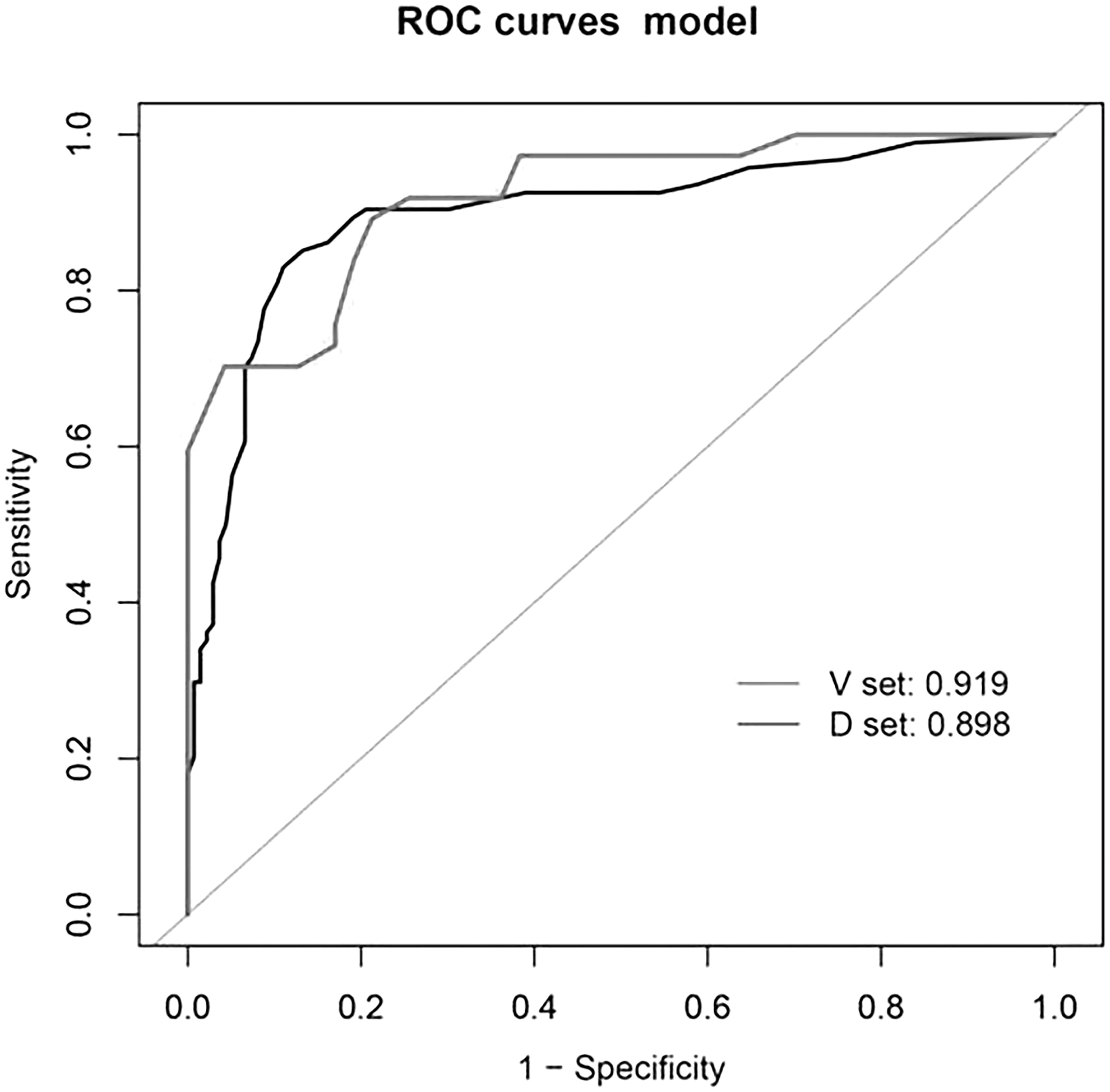
Receiver operating characteristic (ROC) curve of the prediction model in the development and validation sets.
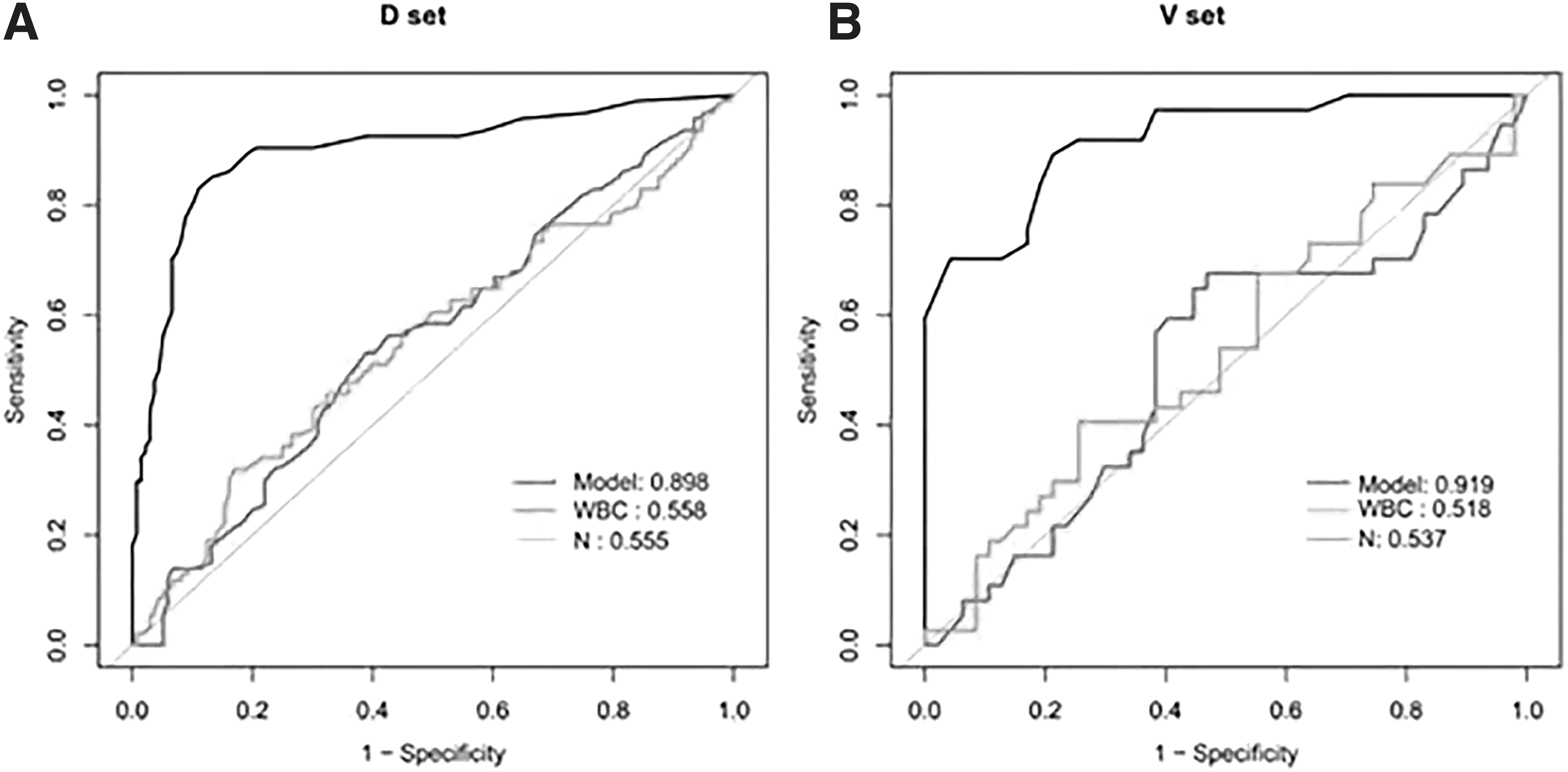
Receiver operating characteristic (ROC) curves evaluate the white blood cell (WBC) count, neutrophil ratio (N), and the prediction model's accuracy in predicting pathologic infection.
Furthermore, the nomogram (Fig. 4) and calibration curve (Fig. 5) of the prediction model were plotted. The calibration curve showed that there was good consistency between the predicted value and observed value in the modeling group and verification group.
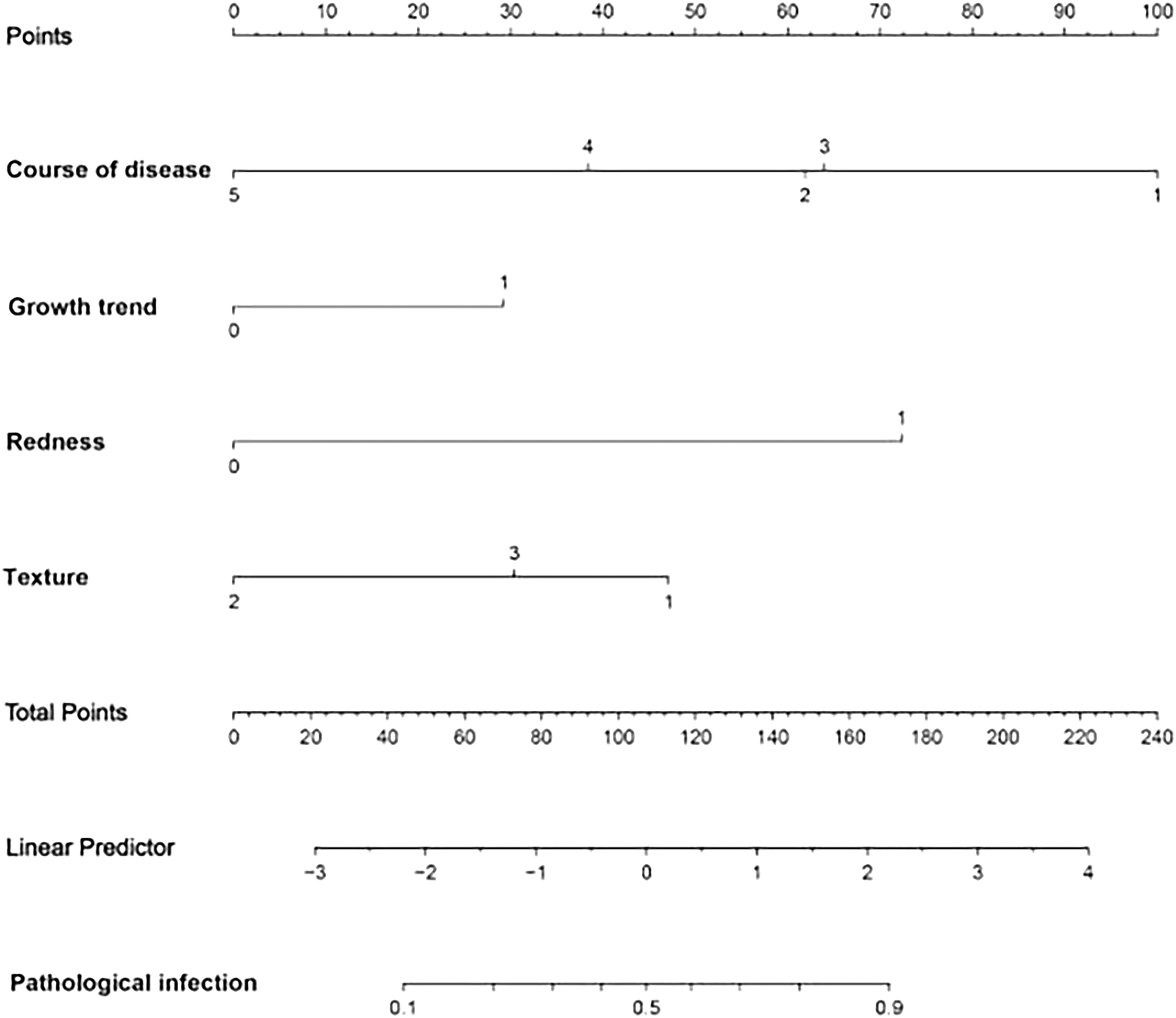
The nomogram of the prediction model for identifying epidermoid cyst infection.
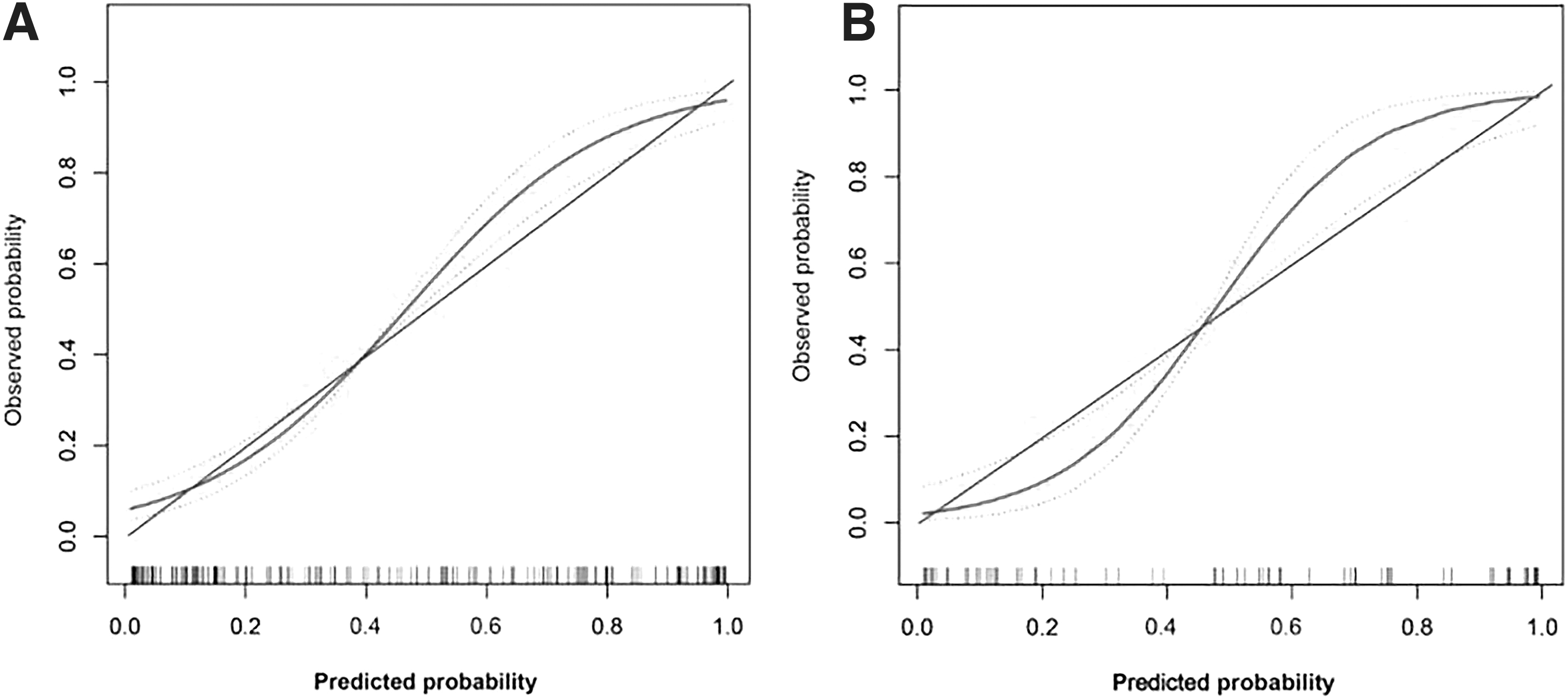
The calibration curve of the epidermoid cyst infection prediction model in the modeling group (
Discussion
An epidermoid cyst is a common intracutaneous or subcutaneous benign tumor. Its wall is composed of epidermis or follicular funnel on the skin surface. Epidermoid cysts are more common in males, and mostly occur on the face. Surgical resection is the main treatment method. An epidermoid cyst without infection can be removed easily. However, because the wall of an infected cyst is fragile and easily broken, it is difficult to remove the cyst wall and its contents completely. Therefore, identifying non-invasive indicators such as clinical and morphologic characteristics of epidermal masses to predict infections can help clinicians make better treatment choices. This study analyzed retrospectively the morphologic characteristics and clinical data of 314 patients with epidermoid cyst. Based on the post-operative pathology examination, we constructed a prediction model based on the clinical features of epidermoid cyst that had been removed surgically to identify pathologic infection. The diagnostic accuracy of the model was confirmed in the modeling group and verification group, and the stability was confirmed by calibration curve.
In this study, the growth trend, redness, and swelling were independent risk factors for epidermoid cyst infection. The rapid growth, redness, and swelling symptoms of cysts were associated with higher possibility of infection, which is consistent with the pathology of infection. In addition, disease course of more than three years, tough quality, and hardness were predictive factors for pathologic infection. The possible reason is that this type of epidermoid cyst has a thicker wall, which prevents the overflow of the contents. As the disease course extends, the substance in the cyst becomes tough, hard, and stabilized. In addition, this study also plotted the nomogram of the prediction model, which integrated multiple predictive indicators such as disease course, redness, texture, and growth trend, and used scaled line segments to represent them on the same plane with a certain ratio. After assigning a value to each influencing factor, the total score of infection probability for each individual was calculated. At the same time, the calibration curve showed that the model had good prediction accuracy in the modeling group and verification group.
The pathogenesis of epidermal cysts is still unclear. It is generally believed that the epidermal cyst originates from the infundibular portion of the hair follicle, but this hypothesis does not explain the epidermal cysts that occur in glabrous skin. Some studies proposed another etiological hypothesis that human papillomavirus (HPV) infection may be closely related to the palmoplantar epidermoid cyst.12,13 To investigate the mechanism of epidermoid cyst infection, Brook 14 cultured 231 epidermoid cyst abscesses, and found the anaerobic bacteria and Staphylococcus aureus were important for cyst infections. However, Dayna et al. 15 found that the microbiologic characteristics of infected and non-infected epidermoid cysts were similar and hypothesized that the rupture of the cyst wall and the extrusion of the cyst contents into the dermis were the causes of inflammation. Therefore, more large-scale etiologic and prospective controlled studies on the pathogenesis of infection are needed for the future study.
The early diagnosis of infectious lesions can help optimize the treatment strategy. When there are vague signs of infection around the cyst, such as simple erythema or pain, the choice of treatment usually depends on the operator. However, in many patients, the infection is more serious than expected, and the cyst cannot be completely removed. Min et al. 16 found that there was a strong positive correlation between the thickness of epidermis and the thickness of the cyst wall in people with a history of infection. Therefore, when the facial infected epidermoid cyst is removed, a complete stripping operation should be performed to prevent the recurrence of the cyst.
The epidermoid cysts in this study were all located on body surface. The head and neck cysts were most common, followed by chest, abdomen, and limbs. There was no relation between cyst location and infection. According to the literature, epidermoid cysts have also been found in various internal organs, including brain, 17 cecum, 18 kidney, 19 and thymus. 20 We also found that there were more patients with fluctuating sensation, itching, and skin breakage in the infected group, but these factors were not included in the prediction model. This may be due to the small number of cases with these factors, which is also a limitation of this study. Moreover, this study is a single-center retrospective study, and it is necessary to conduct a multicenter study to expand the sample size further to optimize the prediction model and conduct external verification. In addition, the development of radiomics and artificial intelligence3,21 also promotes the accurate measurements of cyst features. These inspection indicators can be integrated to develop a model with better predictive performance.
In summary, this study constructed and verified a prediction model based on the clinical characteristics of epidermoid cyst to identify cyst infection. The disease course, growth trend, redness, and texture of epidermoid cysts were independent factors for predicting infection. The constructed model had good diagnostic accuracy and high specificity. It can detect infection cases in early phase, avoid abscesses formation, facilitate stage 1 healing, and prevent disease progression.
This study is limited by its retrospective nature, and future multicenter and prospective investigation is needed to confirm the findings. Furthermore, this study did not establish other prediction models (such as random forest, cluster analysis, etc.) to objectively evaluate the accuracy of the prediction model. Finally, uninfected epidermoid cysts may have early inflammatory reactions, but they have not yet shown clinical symptoms or characteristics.
Footnotes
Acknowledgments
Over the course of researching and writing this paper, I would like to express my thanks to all those who have helped me. First, a special acknowledgement should be given to Dr. Yuxia Miao, from whose suggestions and encouragement I benefited greatly. Despite a very busy schedule, she still gave my paper a careful reading and detailed comments. Without her keen insights and constant encouragement, it would not have been finished. In addition, I am also extremely grateful to all my friends and family who have kindly provided me assistance and companionship in the course of preparing this article. Moreover, I wish to extend my thanks to the staff of the library and electronic reading room for providing much useful information for my thesis.
Authors' Contributions
Ren, Li, and Xie participated in research design, data analysis and interpretation, and writing of the manuscript; Xie, Xu, and Gao participated in sample collection, and contributed to the acquisition and interpretation of data; Xie, Xu, and Yang participated in the execution of the experiments; Xie and Xu participated in research design and supervised the course of the project. All authors read and approved the final manuscript.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding information
This work was supported by Changzhou City Health Bureau Project (QN202208); Changzhou City Health Bureau Project (KY20221362).
Author Disclosure Statement
The authors declare no potential conflict of interest.