
Abstract
Background:
Surgical site infections (SSIs) are costly and associated with poorer patient outcomes. Intra-operative surgical site irrigation and intra-cavity lavage may reduce the risk of SSIs through removal of dead or damaged tissue, metabolic waste, and site exudate. Irrigation with antibiotic or antiseptic solutions may further reduce the risk of SSI because of bacteriocidal properties. Randomized controlled trials (RCTs) have been conducted comparing irrigation solutions, but important comparisons (e.g., antibiotic vs. antiseptic irrigation) are absent. We use systematic review-based network meta-analysis (NMA) of RCTs to compare irrigation solutions for prevention of SSI.
Methods:
We used Cochrane methodology and included all RCTs of participants undergoing a surgical procedure with primary site closure, in which method of irrigation was the only systematic difference between groups. We used a random effects Bayesian NMA to create a connected network of comparisons. Results are presented as odds ratios (OR) of SSI, where OR <1 indicates a beneficial effect.
Results:
We identified 42 eligible RCTs with 11,726 participants. Most were at unclear or high risk of bias. The RCTs included groups given no irrigation or non-antibacterial, antiseptic, or antibiotic irrigation. There was substantial heterogeneity, and a random effects model was selected. Relative to non-antibacterial irrigation, mean OR of SSI was 0.439 (95% credible interval: 0.282, 0.667) for antibiotic irrigation and 0.573 (0.321, 0.953) for antiseptic agents. No irrigation was similar to non-antibacterial irrigation (OR 0.959 [0.555, 1.660]). Antibiotic and antiseptic irrigation were ranked as most effective for preventing SSIs; this conclusion was robust to potential bias.
Conclusions:
Our NMA found that antibiotic and antiseptic irrigation had the lowest odds of SSI. There was high heterogeneity, however, and studies were at high risk of bias. A large RCT directly comparing antibiotic irrigation with both antiseptic and non-antibacterial irrigation is needed to define the standard of care for SSI prevention by site irrigation.
Surgical site infections (SSIs) are site infections that occur after an operative procedure. They are costly and associated with poorer patient outcomes, increased death, morbidity, and re-operation rates [1]. Reported rates of SSI vary depending on patient characteristics, degree of wound contamination, and type of surgical procedure. Conservative estimates indicate that SSI may occur in approximately 1% of all surgical hospital admissions [2–4], although this estimate will increase when infections presenting after discharge are included [5–7]. In patients undergoing gastrointestinal procedures, especially large bowel operations, 10% are reported as experiencing SSI, and this may be higher in emergency surgical procedures [8].
The SSIs also have substantial financial impact, with the increased cost per patient undergoing a major surgical procedure who has an SSI estimated as more than £5,000 [9]. Multiple pre-, intra-, and post-operative approaches are taken to reduce SSI; this includes site irrigation.
Surgical site irrigation and intra-cavity lavage (henceforth collectively termed irrigation) involves washing out the site during operation [10]. This irrigation may reduce the rate of SSIs through removal of dead or damaged tissue, metabolic waste, and site exudate. Solutions may contain antibiotic or antiseptic agents that may reduce bacterial contamination and SSI. Irrigation of the site during operation can be achieved with physiologic saline alone or in combination with antimicrobial agents. There is concern, however, that antimicrobial agents may damage tissue and prevent normal healing [11]. In the case of antibiotic agents, there are concerns about overuse given the increasing prevalence of bacteria with antibiotic resistance.
Another potential risk of irrigation is that the introduction of large volumes of any type of fluid into a cavity or surgical site could wash away inflammatory cells vital to the host defence [11]. Careful evaluation of the use of intra-operative irrigation is therefore essential.
Systematic reviews seek to identify all the primary studies that meet pre-specified criteria and to collate and assess these, using transparent and rigorous methods [12]. The UK National Institute for Care and Health Excellence (NICE) guidelines reviewed evidence from 20 randomized controlled trials (RCTs) and concluded that the use of surgical site irrigation or intra-cavity lavage could not be recommended to reduce the risk of SSIs [7]. The search used to inform this guideline is now almost 10 years old, and a more recent systematic review found a benefit to intra-operative irrigation over no irrigation in abdominal surgical procedures [13], although this review included studies that we consider to be quasi-RCTs.
A recent review restricted to RCTs of prophylactic surgical site irrigation (excluding opoerations with high levels of contamination) [14] informed recent World Health Organization guidance that suggests considering the use of antiseptic irrigation; suggests that antibiotic agents not be used; and makes no recommendation about saline irrigation [15].
We previously conducted a Cochrane review of surgical site irrigation in operations employing a broad focus that included sites with infection already present, and also lavage of deeper cavities [16]. It identified all relevant RCTs and used meta-analysis to combine trials that evaluated similar comparisons. In common with all previous systematic reviews in this area, the Cochrane review used pairwise meta-analysis [17]. Pairwise meta-analysis can only look at two interventions simultaneously, and each comparison is based only on the primary studies that compared directly those two interventions. Pairwise meta-analysis cannot be used to coherently compare multiple interventions, it cannot provide a ranking of multiple interventions, and it cannot answer questions of relative effectiveness for interventions that were not directly assessed in the primary research studies (but where indirect comparisons are possible).
The Cochrane review identified substantive evidence for several comparisons of different types of irrigation and no irrigation, but also identified a clear gap in the direct evidence—that there were no trials directly comparing antibiotic irrigation with antiseptic irrigation solutions.
Network meta-analysis [NMA] is a commonly used method to overcome the limitations of pairwise meta-analysis when there are multiple interventions [18]. The NMA combines evidence from all the RCTs available on the multiple interventions of interest, as long as they form a connected network of intervention comparisons. This means that any two interventions (A and D, say) are linked by a chain of direct comparisons (for example, A v B, B v C, and C v D). The NMA provides estimates comparing any pair of interventions in the connected network of evidence, each of which can be thought of as a weighted average of the direct pairwise estimate (where it exists) and the indirect estimate from the evidence in the rest of the network [19]. For example, evidence from RCTs comparing antiseptic vs. saline irrigation and RCTs comparing antibiotic vs. saline irrigation can be combined to indirectly compare antiseptic vs. antibiotic irrigation, even in the absence of any head-to-head RCTs directly assessing this comparison.
The NMA assumes that there are no systematic differences between the direct and indirect evidence for each comparison, and it is therefore important to check the validity of this assumption both statistically (if there is sufficient evidence) and clinically by assessing homogeneity of the included study populations. The results from an NMA can be used to simultaneously compare multiple interventions and to rank the interventions in terms of effectiveness [19].
This article presents the results of applying NMA to the data from the Cochrane systematic review and is, to the best of our knowledge, the first application of network meta-analysis for intra-operative irrigation (including no irrigation) and their effects on SSI. The objective was too explore (a) whether irrigation reduces SSI compared with no irrigation and, if so, (b) which type of irrigation might be most effective to prevent SSI.
Methods
Systematic literature review
Full details of the systematic review have been published elsewhere [16], but a summary follows. We conducted a systematic literature search for published and unpublished RCTs of participants undergoing surgical procedures in which the use of a particular type of intra-operative washout (irrigation or lavage) was the only systematic difference between groups, and in which surgical sites underwent primary closure. In this review, we grouped irrigation types as non-antibacterial, antiseptic, antibiotic, no treatment. Four subgroups of antibiotic agents were identified for an alternative model conducted as a sensitivity analysis (penicillin, aminoglycoside, cephalosporin, and other).
On our search date of February 1, 2017, we searched the Cochrane Wounds Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE; Ovid Embase, and EBSCO CINAHL Plus. We also searched three clinical trials registries and references of included studies and relevant systematic reviews. There were no restrictions on language, date of publication, or setting. The primary outcome was SSI defined by the Centers for Disease Control and Prevention (CDC) criteria [20], or the study authors' definition of SSI. We did not differentiate between superficial and deep incisional infection. Two researchers independently assessed titles and abstracts for relevance and conducted full-text eligibility checking, with disagreements resolved by discussion or by a third researcher.
Two researchers independently assessed included studies using the Cochrane approach for assessing risk of bias as detailed in the Cochrane Handbook for Systematic Reviews of Interventions [21]. Disagreements were resolved through discussion or by consulting a third author. This Cochrane tool addresses seven specific risk of bias domains: For the present NMA, we combined domains to form an all-domain risk of bias that categorized studies as low, unclear, high, or very high risk of bias. Because issues with performance bias are common in such irrigation RCTs, we did not include it in the all-domain definition for the NMA. Low required all domains to be at low risk of bias; unclear required one or more domains at unclear risk of bias and no domains at high risk; high required one domain at high risk of bias; and very high required two or more domains at high risk of bias.
NMA
For this analysis, we used a Bayesian NMA to combine evidence from RCTs that form a connected network of intervention comparisons [22]. This methodology strengthens intervention effects by combining both direct and indirect evidence and allows the comparison of interventions not directly compared in head-to-head RCTs, so long as the interventions form part of a connected network. We estimated odds ratios (OR) of SSI after operation using a binomial outcomes logistic link NMA [23]. Vague priors were assumed for all parameters. The model was implemented in the Bayesian OpenBUGS version 3.2.3 rev 1012 software [24].
Several measures of model assessment were employed. Deviance information criteria (DIC) assessed both the fit and complexity of the model, residual deviance assesses the overall fit compared with the number of independent data points, and leverage plots assessed whether individual data points have undue influence on their model predictions [25]. Code and further detail are provided in Appendix A and Appendix C.
Previous publications identified several classes of antibiotic solutions used for irrigation—for example, cephalosporins and aminoglycosides. Three modelling assumptions were considered for intervention effects of these classes. The first assumed all antibiotic intervention effects to be the same; the second assumed all antibiotic intervention effects to be independent; the third used a hierarchical class effects model assuming antibiotic intervention effects to be different but following a common Normal distribution [18]. We also considered both fixed and random intervention effects for the three models. Selection of model, and of fixed or random intervention effects, was made using DIC and residual deviance.
The contribution of each set of RCT direct comparisons to each intervention comparison (i.e., intervention contrast) was estimated using the contributions matrix [26]. We combined this with a risk of bias assessment of the RCTs, and thus quantified the proportion of evidence on each contrast that was at low, high, or unclear risk of bias [27]. Assuming that the recommended irrigation technique is the one with the lowest estimated OR of SSI, we explored the sensitivity of this recommendation to potential bias in the direct estimate for each intervention comparison [28].
This threshold analysis is represented by an invariant interval within which the direct estimate for the intervention comparison could vary without changing the recommendation (in terms of irrigation intervention for SSI prevention). Inspecting the results from the threshold analysis and the proportion of evidence at risk of bias can identify which direct evidence the recommendations are most sensitive to, and whether it is at risk of bias.
Heterogeneity within contrasts across studies was assessed using the I2 measure, which represents the percentage variation across studies not because of chance. The I2 was estimated by conducting a frequentist random effects meta-analysis on each contrast for which direct evidence was available. Very broadly, we considered that I2 values of 25% or less may not indicate important heterogeneity and values of more than 75% indicate considerable heterogeneity [29]. The random effects heterogeneity variance, interpreted in line with empiric ranges in the literature, was used as an across-contrast assessment of heterogeneity [27,30]. Comparison of fixed and random effects DIC and posterior mean deviances was used as a final assessment of heterogeneity.
Inconsistency between direct and indirect evidence is a heterogeneity issue specific to NMA [31]. Evidence of inconsistency was assessed globally using an unrelated-mean effects model and locally by comparing the direct and indirect evidence via node-splitting on contrasts on which both sources exist [31].
High variation in publication date of identified RCTs was expected. It was also expected that this would be a source of considerable differences between participants, surgical techniques, definitions of SSI, and use in antibiotic agents over time, which may make results from early studies less directly relevant to current practice. To address this concern, we conducted a sensitivity analysis excluding all studies published before (exclusive of) 1990.
Because surgical site contamination was a potential source of heterogeneity, we conducted a network meta-regression on degree of contamination [32]. A three-level categorization was planned, dividing RCTs into clean; clean-contaminated; and contaminated, dirty, or mixed. Where studies included a mixture of contamination classes, we classed the study at the highest level of contamination represented. A further source of heterogeneity is the surgery type. We conducted a network meta-regression on the two-level categorization of abdominal operation or operation with prostheses. This assumed a common log OR across contamination categories for all interventions log ORs relative to non-antibacterial irrigation.
Results
Results of systematic literature review
Our systematic literature review identified 59 RCTs across 64 publications on 14,738 patients. Of these 59 studies, we were able to include 42 on 11,726 patients in this NMA. Study characteristics are shown in the Appendix. A list of those studies included in the Cochrane review but excluded from the NMA, with reasons, is also given in Appendix B.
All non-antibacterial interventions included in the network analysis were saline. Most antiseptic interventions involved povidone iodine, and a range of antibiotic agents was used; these fell into the following three primary classes of antibiotic agents: Cephalosporins (cefazolin, cephapirin, cefoxitin, cefotetan, cefamandole, cephalothin, cefoxin, and moxolactam); penicillins (ampicillin and clindamycin); and mono or combination therapy aminoglycosides: (kanamycin sulphate + cephalothin sodium, kanamycin, gentamicin, gentamicin + clindamycin); other antibiotic agents (taurolidine polyvinyl pyrrolidine; tetracycline; chloramphenicol succinate) were classed as “other.”
No studies directly compared an antibiotic solution with an antiseptic, and no studies compared different volumes of irrigation. Two included studies in the Cochrane review compared different techniques of administering the same volume of saline irrigation; these were not included in our NMA [33,34]. The reason was that we focused on the type of irrigation solution rather than administration techniques.
Most included studies enrolled adult participants. A small number included only children, and in several others, there was a mixture of adult and pediatric participants or participant ages were unclear. Because of the nature of the surgical procedures assessed (e.g., caesarean sections), many studies enrolled only women. A wide range of surgical procedures and all classes of operation (clean, clean-contaminated, contaminated, dirty) were represented in the included studies. Use of prophylactic antibiotic agents varied but was, as anticipated, more likely to be reported for studies enrolling participants undergoing surgical procedures with higher levels of contamination.
Most studies in the review assessed SSI as a primary outcome, and a majority also reported usable dichotomous data for this outcome although the definitions employed by the study authors varied and in some cases were not clearly reported. Hence, we were able to include the majority of identified studies in this NMA.
NMA results
The systematic review identified 42 RCTs (Fig. 1) for inclusion in the NMA.
PRISMA diagram for systematic literature review.
The evidence network is presented in Figure 2; the size of nodes represents the number of RCTs on that intervention while edge thickness represents number of RCTs on that contrast. Non-antibacterial irrigation was selected as the reference intervention against which intervention effects are estimated, but intervention effects for all pairs of connected interventions can be obtained.
Network of connected irrigation solutions, and no irrigation, for prevention of surgical site infection.
Model assessment statistics strongly favored random effects models, suggesting evidence of heterogeneity. There was limited difference in assessment statistics, however, between the three models for different approaches on antibiotic classes. Therefore, to focus on the primary biologic mechanisms, which may drive differential effectiveness of the main irrigation types (non-antibacterial, antiseptic, antibiotic, no intervention), and given the primary clinical questions faced in practice, we opted to group all antibiotic agents in a single intervention node for our base case analysis. Posterior mean residual deviance and leverage (provided in Appendix A) suggested reasonable fit of this model and no undue influence of outliers.
The estimated ORs relative to non-antibacterial irrigation are presented in Figure 3; lower ORs favor the comparator over non-antibacterial irrigation, while 95% Bayesian credible intervals (CrI) that do not cross 1 represent evidence of a difference that is classically “statistically significant.” On this basis, there is evidence that antibiotic agents and antiseptic agents have lower odds of SSI than non-antibacterial irrigation, and no evidence of a difference between non-antibacterial irrigation and no irrigation.
Median and 95% credible intervals for odds ratio of surgical site infection (SSI) versus non-antibacterial irrigation.
The median (95% CrI) estimated ranking of the interventions was 1st (1st, 2nd) for antibiotic agents, 2nd (1st, 3rd) for antiseptic agent, 3rd (2nd, 4th) for no irrigation, and 4th (3rd, 4th) for non-antibacterial irrigation. The cumulative probability rank plot (Fig. 4) provides probabilities that each intervention is at least the 1st, 2nd, 3rd, and 4th most effect intervention for prevention of SSI, respectively. Antibiotic and antiseptic agents again have the highest probabilities of being 1st or 2nd best. Cross tables of OR comparing all interventions are provided in the Appendix. However, The OR of antibiotic agents vs. antiseptic agents, however, was 0.77 (95% CrI: 0.4, 1.54) favoring antibiotic agents, but suggesting no evidence that one is superior to the other.
Rank probability plots for all irrigation solutions using random effects models. Median (95% CrI) ranks were 1st (1st, 2nd) antibiotic, 2nd (1st, 3rd) antiseptic, 3rd (2nd, 4th) no irrigation, and 4th (3rd, 4th) non-antibacterial.
The favoring of a random effects model by the model assessment statistics suggests the presence of substantial heterogeneity across RCTs within intervention contrasts with heterogeneity standard deviation of 0.661 95% CrI (0.396, 1.004), which is similar in magnitude to the estimated log odds ratios. Comparing the heterogeneity variance of 0.44 with published empiric distributions for heterogeneity of semi-objective outcomes places our network in the 50%–75% quantile, suggesting moderate heterogeneity [30].
Moderate or substantial heterogeneity was also indicated by the I2 of 48.4% and 64.3% for comparisons of no irrigation and antiseptic with non-antibacterial irrigation, respectively, strengthening our choice of random effects. Conversely the I2 was 26.6% for antibiotic agents with non-antibacterial irrigation, which does not necessarily suggest important heterogeneity.
Publication dates of included studies showed a wide range (1968 to 2016) with a substantial number (16 studies, 3,638 participants—one third of participants) published before 1990. Our sensitivity analysis excluding studies published before 1990 did not have substantial impact on conclusions, although results shifted slightly in favor of antiseptic irrigation (OR with 95% CrI vs. non-antibacterial irrigation: 0.35 [0.11, 0.84]] over antibiotic irrigation [0.41 [95% CrI 0.18, 0.89]). Full results are presented in the Appendix.
The unrelated mean effects model gave similar model fit to the NMA model, and the between studies heterogeneity standard deviation was unchanged, suggesting no evidence of inconsistency. We explored this further using local node-splitting tests that, again, did not indicate inconsistency on either of the two loops on which the test could be conducted (No irrigation-non-antibacterial-antiseptics, and No irrigation-non-antibacterial-antibiotic agents). Full details are provided in the Appendix.
We found 21 studies with clean-contaminated surgical sites and 17 studies with contaminated, dirty, or mixed sites. Only four studies, however, were on clean surgical sites and three of these [35–37] had zero events in one arm, meaning results were largely reliant on a single study [38]. It was therefore necessary to merge clean with clean-contaminated in a two-level meta-regression giving 25 studies in the combined class. There was no evidence that intervention effects differed according to contamination level (log OR between intervention log ORs across contamination categories 0.229 95% CrI [-0.408, 0.873]).
The meta-regression comparing abdominal operation and operation with prostheses did not produce reliable results because of limited data on operation with prostheses. The four studies on operation with prostheses were the same four on clean surgical sites, so again affected by zero events. Full details of meta-regressions are provided in the Appendix.
The models using different class effects for antibiotic agents gave a similar fit, and so in the results above, we have used the simplest model that assumes a common effect for all antibiotic agents. In Figure 5, we provide results of the hierarchic class effects model assuming antibiotic intervention effects to be different but following a common mean. Inspecting the results of this model for the different antibiotic agents allows us to make tentative comparison between the types of antibiotic agents for prevention of SSI. They indicate that aminoglycoside had the lowest OR of SSI compared with non-antibacterial irrigation (0.301 95% CrI [0.135, 0.588]), followed by penicillin (0.349 95% CrI [0.099, 0.823]), other (0.498 95% CrI [0.265, 0.977]), and cephalosporin (0.579 95% CrI [0.307, 1.16]).
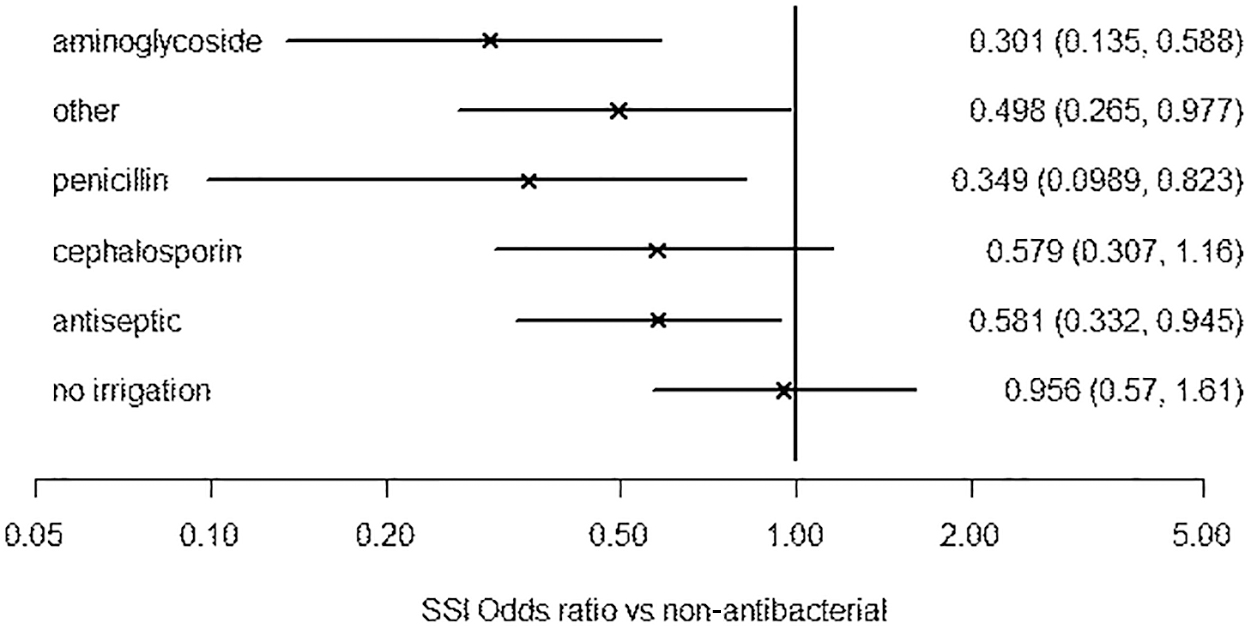
Median and 95% credible intervals for odds ratios of surgical site infection (SSI) versus non-antibacterial irrigation using a hierarchic class effects model assuming antibiotic intervention effects to be different but following a common mean.
Risk of bias assessment
The proportion of evidence contributing either directly or indirectly to each contrast that is at low, unclear, or high/very high risk of all-domain, excluding performance, bias is presented in Figure 6. Performance only risk of bias is presented in Figure 7. All of the evidence on the interventions is at unclear or high/very high risk of all-domain bias even without considering performance bias. The main effect of considering performance bias in the assessment is to increase the number of studies at very high rather than high risk of bias; issues were not restricted to inevitable problems with blinding of personnel. Reporting was generally poor, meaning that a large number of studies have multiple domains at unclear risk of bias.
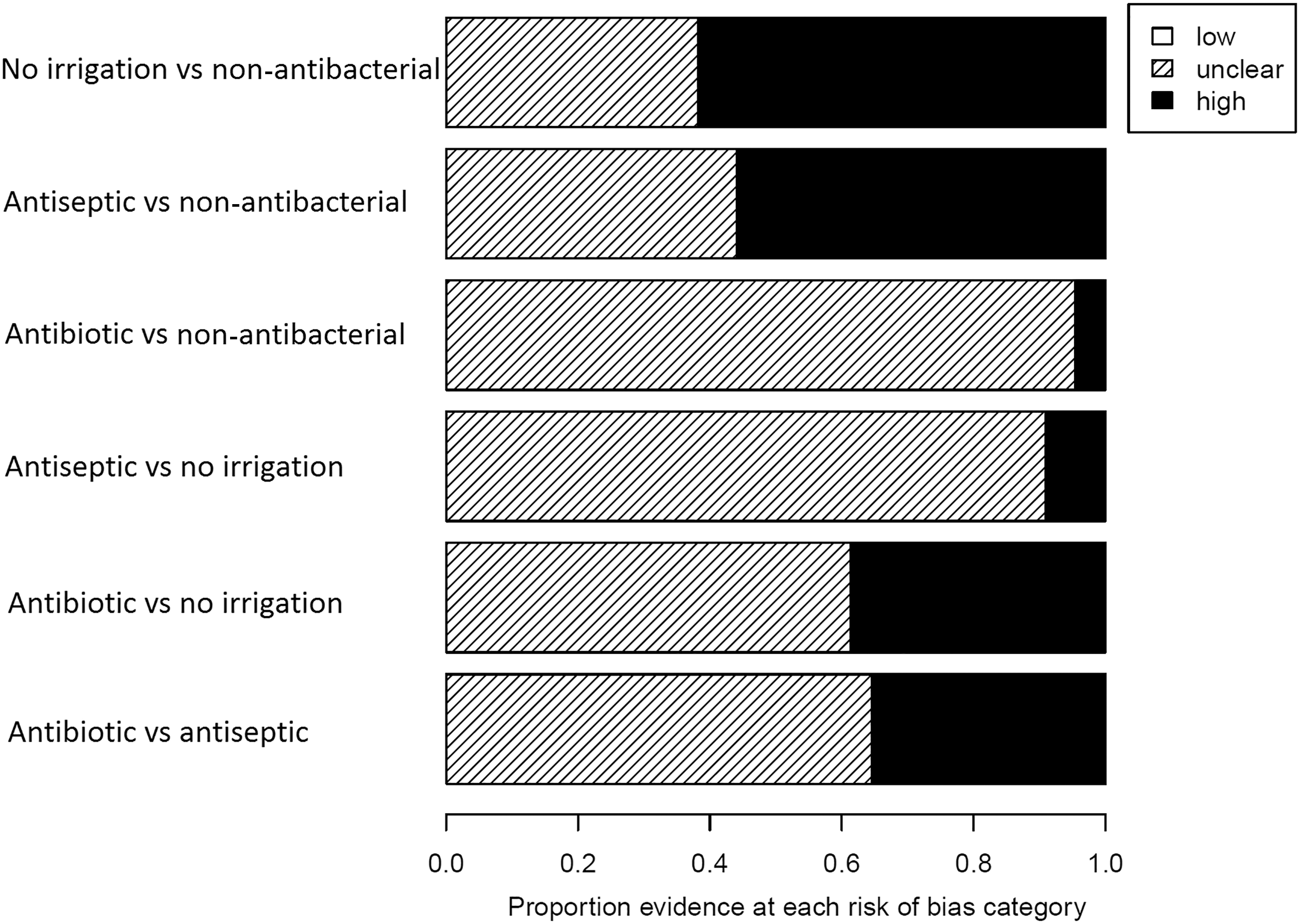
All domain risk of bias (excluding performance bias) of studies directly or indirectly contributing to each contrast.
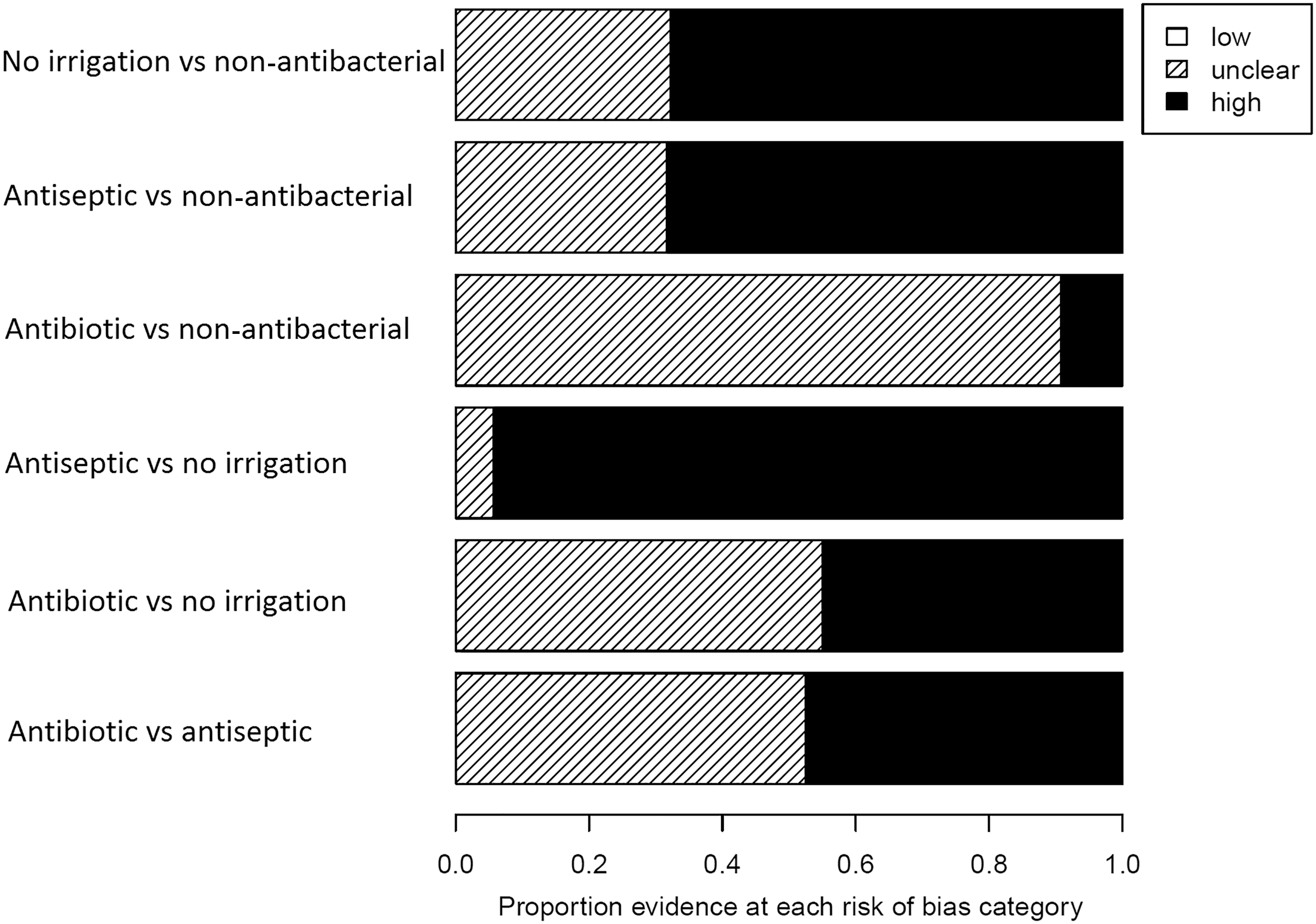
Performance (issues with blinding) risk of bias of studies directly or indirectly contributed to each contrast.
Our NMA consists of studies conducting five contrasts (i.e., no irrigation vs. non-antibacterial, antiseptic vs. non-antibacterial, antibiotic vs. non-antibacterial, antiseptic vs. no irrigation, and antibiotic vs. no irrigation). These are contrasts on which direct evidence is available. The bias threshold analysis, with results in Figure 8, tests the sensitivity of the choice of intervention with lowest odds of SSI (i.e., antibiotic agents) to bias in the studies conducting each of these five contrasts.
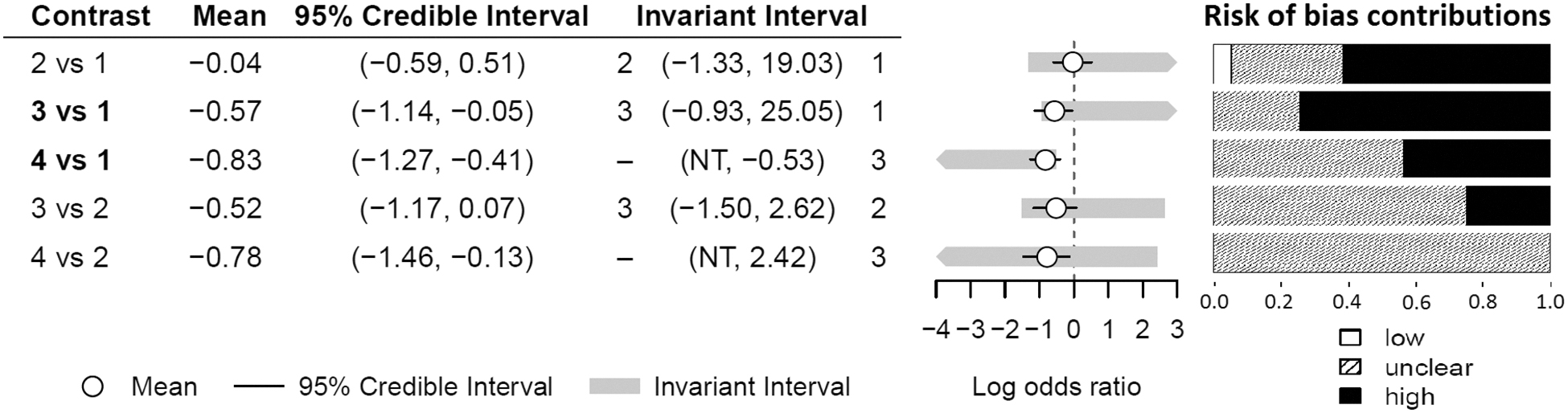
Contrasts level risk of bias (all domain excluding performance bias) and threshold sensitivity analysis. Risk of bias contributions are the proportion of direct (not including indirect) evidence on each contrast at each risk of bias category. 1 = non-antibacterial, 2 = no irrigation, 3 = antiseptic, 4 = antibiotic agents. Percentages low:unclear:high risk of bias for each contrast are (5:33:62) 2 vs. 1, (0:30:70) 3 vs. 1, (0:56:44) 4 vs. 1, (0:75: 25) 3 vs. 2, and (0:100:0) 4 vs. 2.
For each of the five intervention contrasts on which there is direct study evidence, and in addition to a mean log OR and 95% CrI, this figure presents a decision invariant interval. The decision invariant interval is the interval over which the log OR can vary without changing the optimal decision (i.e., that antibiotic agents have lowest odds of SSI); the interventions that become optimal if the log OR were changed to being below or above the invariant interval are also presented in Figure 8. Limits of the 95% CrI falling outside the invariant interval indicate high sensitivity of the choice of optimal intervention to evidence on that contrast.
The final component of Figure 8 is a plot of the risk of bias contributions; this is the proportion of the direct evidence on each contrast that is at each level of risk of bias, as distinct from the proportion of both direct and indirect evidence on each contrast in Figure 6 and Figure 7. The risk of bias contributions suggests the risk that the log OR for each contrast is biased and likely to change if less biased evidence were available or collected.
This analysis indicates highest sensitivity of the optimal decision to studies comparing antiseptic agents versus non-antibacterial and antibiotic agents versus non-antibacterial, which is sensible because antiseptic and antibiotic agents are the interventions with lowest OR of SSI. Bias in these studies can lead to the optimal intervention switching from antibiotic to antiseptic irrigation. Further, the proportion of studies that are at high risk of bias is 70% on antiseptic agents versus non-antibacterial and 44% on antibiotic versus non-antibacterial, indicating high scope for our conclusion to be incorrect because of bias.
For context, the Cochrane review found that the direct evidence for all antibacterial agents versus non-antibacterial was low certainty because, in part, of risk of bias (excluding performance bias). The analysis suggests, however, that no intervention other than antibiotic agents or antiseptic agents could be optimal; the invariant thresholds for evidence that lead to non-antibacterial irrigation or no irrigation becoming optimal are much wider than the corresponding 95% CrIs.
Discussion
This NMA included the majority of studies, and participants, identified in a recent Cochrane review [16]. We were able to use SSI data from 42 studies with a total of 11,726 participants across a range of interventions involving intra-operative washout procedures. As with the Cochrane review, most participants in the NMA were adults, and a majority were female, a consequence of many studies being in women undergoing caesarean sections. The NMA enabled us to rank interventions from most to least likely to have the lowest SSI rates. We found antibiotic irrigation most likely to have lowest SSI rates relative to non-antibacterial irrigation, followed by antiseptic irrigation; No irrigation, with non-antibacterial irrigation was most likely to be ranked worst. These results indicate that the use of intra-operative antibacterial—and in particular antibiotic—irrigation, for appropriate procedures, may confer benefit in terms of SSI prevention.
A wide range of surgical procedures and all classes of these procedures (clean, clean-contaminated, contaminated, and dirty) were represented, although there were very limited data from clean surgical procedures. Trials in these operations frequently reported low or zero events in one or more trial arms, making sensitivity or regression analyses difficult [35–38]. Most participants were undergoing procedures classed as clean-contaminated or higher, and most events occurred in these surgical classes. Meta-regression comparing clean or clean-contaminated to contaminated, dirty, or mixed surgical sites found no evidence of higher rates of SSI in the latter category.
Publication dates of included studies also showed wide variation (1968 to 2016) with almost a third of trials and patients dating from before 1990. A sensitivity analysis excluding studies published before 1990, however, did not have substantial impact on conclusions, only shifting results in favor of antiseptic over antibiotic irrigation. There were variations in the use of prophylactic antibiotic agents given by alternative routes (e.g., oral, intravenous), as anticipated given the different types and contamination levels of operation involved and the time span across which studies were conducted and published. These variations, however, were not restricted to any one comparison, and so were not likely to bias the results.
Heterogeneity may also stem from the volumes and methods of application of the irrigation interventions. While we are able to determine the range of planned irrigation volumes administered, we acknowledge that there may be additional variance in the volumes successfully delivered. The Cochrane review did not formally assess studies against the reporting checklist for interventions (TIDieR), but the level of information available in most studies for most of the domains was markedly low [39].
In particular, we have very little information on implementation and adherence—intervention fidelity—because volumes of liquids successfully transferred were only reported where the surgical team members were able to vary the volume delivered within given parameters. Where this was the case in the Cochrane review, there were relatively large variances/ranges in the volumes reported; however, we cannot extrapolate from protocols that incorporated discretion to those that did not.
The clinical differences noted above lead to substantial heterogeneity in our NMA. High statistical heterogeneity was also indicated by I2 statistics and size of the heterogeneity standard deviations. Conversely, statistical tests did not indicate evidence of inconsistency. Heterogeneity is a limitation of our analysis, and although we conducted network meta-regression and sensitivity analyses, the heterogeneity remained unexplained.
Many of the studies contributing data to the NMA were at high risk of bias, including risks of bias other than performance bias (blinding of participants and personnel), which is almost inevitable in some of the comparisons directly assessed. Our bias threshold analysis did suggest that the relative ranking of antiseptic and antibiotic irrigation was sensitive to bias in our evidence base, although we have reasonable confidence that the optimal intervention for SSI prevention is at least one of these two. A sensitivity analysis in the original review also found that excluding studies at high risk of bias from sources other than blinding of personnel did not materially alter the results for their primary analyses.
Heterogeneity and risk of bias may limit the conclusions that can be drawn from this NMA. While we did not formally perform GRADE on the NMA, we note that the main direct comparisons in the source Cochrane review were considered to be of low certainty—meaning that further evidence may substantially alter the conclusions [40]. Further, we conducted a bias threshold analysis, which has been proposed as an alternative to GRADE in the context of guidelines.[41] This analysis highlighted the sensitivity of the conclusions to potential biases in the evidence. Together with the high level of risk of bias in the evidence, this also points to a low confidence in the results.
Further rigorous studies at low risk of bias would provide valuable further data, and this is supported by current NICE recommendations. The NICE guidance currently states: “Only apply an antiseptic or antibiotic to the wound before closure as part of a clinical research trial” while maintaining their 2008 recommendation against use of surgical site irrigation [42]. This article suggests that consideration should be given to such an appropriately powered trial comparing an appropriate antibiotic agent (to be determined based on the profile of the surgical population) and an antiseptic such as povidone iodine. A third, control arm using non-antibacterial (i.e. saline) irrigation may also be considered. This control group would control for the impact of antibacterial activity while maintaining both the effect of irrigation and blinding.
This trial would address the clear evidence gap in the direct evidence that we have identified. The primary outcome of this study should be incidence of SSI assessed using a recognized measure such as the CDC criteria, the ASEPSIS measure, or the Bluebelle Wound Healing Questionnaire [43–46]. The presence of resistant and multi-drug resistant bacteria at surgical sites should also be assessed. Such a trial will also require an exploration of cost effectiveness.
There have been a number of previous reviews on aspects of intra-operative irrigation, although none had exactly the same scope as ours, instead focusing on a particular type of surgical procedure [13], a particular agent or class of agents [47,48], or even more narrowly on a specific intervention for a certain operation [49,50]. Some reviews also included studies other than RCTs making estimates obtained vulnerable to higher levels of bias and therefore uncertainty, whereas we employed a strictly defined randomization requirement for inclusion.
Definitions of irrigation varied and many reviews also included any method of topical application including, for example, assessments of aerosols, dry powder, or very low volumes of liquid, which meant that the contribution of irrigation as opposed to application of a particular agent was not assessed. These things need to be considered carefully in any future trial. Several reviews also considered comparisons that were outside the scope of our review because the use of irrigation of a particular type was not the only systematic difference between the intervention groups, making it impossible to isolate the contribution of irrigation to the effect estimate.
The most recent review (2017), and the one with the closest scope to ours, is De Jonge et al. [14], which focused on prophylactic irrigation and supported the recent recommendations of the World Health Organization on prevention of SSI—that povidone iodine irrigation, but not antibiotic irrigation should be considered [15]. De Jonge et al. [14] included fewer studies than our review because of excluding studies where surgical sites were already infected, and by restricting to irrigation at the level of the site rather than allowing deeper (e.g., peritoneal) irrigation. The authors also required a description of appropriate antibiotic prophylaxis, which we did not; many of the studies included here had very limited reporting of co-interventions, and reporting of antibiotic use varied. All these factors are likely to contribute to our different findings on the potential value of antibiotic irrigation.
Unlike previous reviews, this NMA maximally uses available RCT data to examine comparisons not assessed by extant RCTs. Our use of indirect comparisons used data from large numbers of patients to estimate a previously unavailable relative effect, in terms of incident SSI, for antiseptic versus antibiotic containing irrigation. Despite the clear delineation of eligibility criteria, however, risk of bias and heterogeneity mean we cannot be confident that effect estimates are driven solely by the assessed interventions.
There are several on-going trials for prophylactic SSI interventions; this analysis suggests that a further large, and ideally definitive, trial of irrigation, likely with three arms, could be a priority to explore clinical and cost effectiveness, and could lead to large patient benefit. Careful thought needs to be given to the patient group selected for this trial, which is likely to be based on baseline SSI risk, volume of surgical procedures conducted, and appropriateness to the use of irrigation. Stakeholder and decision-maker engagement will be vital to optimizing trial design. Linked research is also suggested to explore the extent and variation in current irrigation practices and their relationship to SSI rates in differing surgical populations.
Footnotes
Funding Information
This research was supported by the United Kingdom (UK) National Institute for Health Research (NIHR) Manchester Biomedical Research Centre (BRC) (IS-BRC-1215-20007). HT, NJW, and JB were supported by the NIHR Biomedical Research Centre at University Hospitals Bristol National Health Service (NHS) Foundation Trust and the University of Bristol (IS-BRC-1215-20011). The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
The Cochrane review which provided the data on which this research was based was supported by the NIHR via Cochrane Infrastructure and Cochrane Programme Grant funding (NIHR Cochrane Programme Grant 13/89/08 - High Priority Cochrane Reviews in Wound Prevention and Treatment) to Cochrane Wounds.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.