
Abstract
Background:
Infection, including mixed infection, is not uncommon in orthopedic surgical incision. This study aimed to investigate the epidemiology and drug resistance of mixed infections after orthopedic surgical procedures.
Methods:
We retrospectively analyzed 533 orthopedic surgical site infections (SSIs) in a university hospital from 2012 to 2017. Eighty-six patients (218 strains) with bacterial culture results showing more than one strain were screened to explore their epidemiology and drug resistance.
Results:
Of 218 bacterial strains, 2–7 bacterial infections were noted in each wound. Most infections were caused by two kinds of bacteria (65.1%). The number of infections decreased with increased number of strains. The combinations of pathogenic micro-organisms were all gram-negative, 55.81%; gram-positive and gram-negative, 30.23%; all gram-positive, 12.79%; and gram-positive and fungi, 1.16%. Their resistance is consistent with the bacterial resistance of 447 cases of single bacterial SSI during the same period. Hospitalization duration was longer (9.8–20.6 d).
Conclusion:
Our study shows no significant changes in epidemiology and drug resistance caused by mixed infections in the orthopedic surgical site because of coordination and competition among micro-organisms. These bacteria are difficult to control, leading to extended hospitalization. Antibiotic agents should be chosen strictly according to drug sensitivity, and ineffective antibiotic agents must be avoided.
Use of surgical procedures is one of the most important methods for the treatment of orthopedic patients [1]. Local soft tissue injury, internal fixation, surgical bleeding, long operation duration, and other factors lead to increased risk of incision infection [2]. Incision infection is still the most common early complication after operations. It directly increases the medical expenses of patients, prolongs hospitalization, delays fracture healing, necessitates reoperation or multiple operations, and makes patients lose the trust of surgeons [3]. If infection is difficult to control, amputation may be indicated, which can even be life-threatening [3].
The basic idea of bone infection control is to eliminate bacteria that cannot be killed by antibiotic agents, improve body immunity, create an environment conducive to enhance body immunity and function of antibiotic agents, and kill planktonic bacteria through antibiotic agents. Thus, in the management of post-operative infection, besides effective debridement and drainage, it is particularly important to analyze the epidemiologic status and drug resistance of pathogens.
Mixed infection refers to infection caused by two or more pathogens at the same time (e.g., a patient experiencing nasal gangrene and epidemic lymphangitis because of bovine tuberculosis and brucellosis). Staphylococcus aureus and Pseudomonas aeruginosa are often found in the wounds of patients with extensive burns and whose condition is complex and difficult. Such patients often need large doses of antibiotic agents, which may not always control the infection effectively. In addition, synergistic effects among various pathogenic micro-organisms in mixed infections, such as synergistic gangrene caused by hemolytic S. aureus and Streptococcus microaerogenes, promote the reproduction of anaerobic bacteria because of the consumption of oxygen by aerobic bacteria.
Initially, the wound appears as local cellulitis, with red periphery and purple center, then progresses to gangrene and ulcer, and gradually expands. The ulcer edge is purple-black and accompanied by severe pain. Therefore, one of the intractable aspects of surgical site mixed infection is the increase in the number of pathogenic bacteria, and adjustment of antibiotic doses is still not effective in controlling infection.
Many studies have investigated the interaction of pathogenic bacteria at the molecular level, but few studies have focused at the human ecologic environment level to determine whether epidemiologic and drug resistance of pathogenic bacteria varied because of the interaction between multiple pathogens on mixed infection. Infection and mixed infection are not uncommon in an orthopedic surgical incision because of its proximity to the body surface, long operation duration, excessive bleeding during operation, and the need for internal implants. Thus, to improve the control and management of mixed infection in orthopedic incisions, this study aimed to observe and understand the characteristics of pathogenic bacteria and drug resistance of mixed infection after orthopedic surgical procedures.
Methods
General information and patients
This study retrospectively analyzed 86 patients with mixed infection of a surgical incision among 533 patients with nosocomial infection after orthopedic operation in the First Affiliated Hospital of Nanchang University from March 2012 to July 2017. The inclusion criteria were as follows: (1) Complete clinical data; (2) sterile surgical treatment; (3)
The exclusion criteria were (1) repeated isolation of strains from the same surgical site in the same patient; (2) contaminated bacteria; (3) infectious diseases; (4) complicated with autoimmune diseases; (5) complicated with infectious diseases; (6) complicated with severe diseases; and (7) impaired organ function.
Examination method
The isolation media for the drug susceptibility tests were 90-mm Chinese blue agar medium (Shanghai Kemajia Biotechnology Co., Ltd.) and Colombian blood agar medium (Shanghai Kemajia Biotechnology Co., Ltd.). Pathogen identification and the drug susceptibility test were performed using the VITEK-2 Compact automatic bacterial tester (bioMerieux, Hazelwood, MO). Drug sensitivity was evaluated according to the 2017 Clinical and Laboratory Standards Institute standards.
The study was approved by the Ethics Committee of The First Affiliated Hospital of Nanchang University (approval #20170720), and all participants provided written informed consent.
Statistical methods
SPSS 19.0 Statistical Software was used to establish a database and perform statistical analyses. The data normality test was performed using a normal curve histogram, Q-Q graph, P-P graph K-S, and Shapiro-Wilk tests. These data were not normally distributed; therefore, non-parametric tests, such as Mann-Whitney and Wilcoxon non-rank sum tests, were used in comparing differences, which were deemed statistically significant if p < 0.05.
Results
Bacterial distribution
A total of 218 bacterial strains from 86 patients were included in this study. There were 152 gram-negative bacteria (69.72%), 65 gram-positive bacteria (29.82%), and one fungus (0.46%). Enterobacter cloacae (12.3%), S. aureus (9.6%), P. aeruginosa (7.7%), Escherichia coli (7.5%), and Baumann/Acinetobacter haemolyticus (6.8%) were the most common (Table 1). The foot (32.56%), leg (23.74%), forearm (16.96%), and knee (15.81%) were the most common sites of infection (Fig. 1).
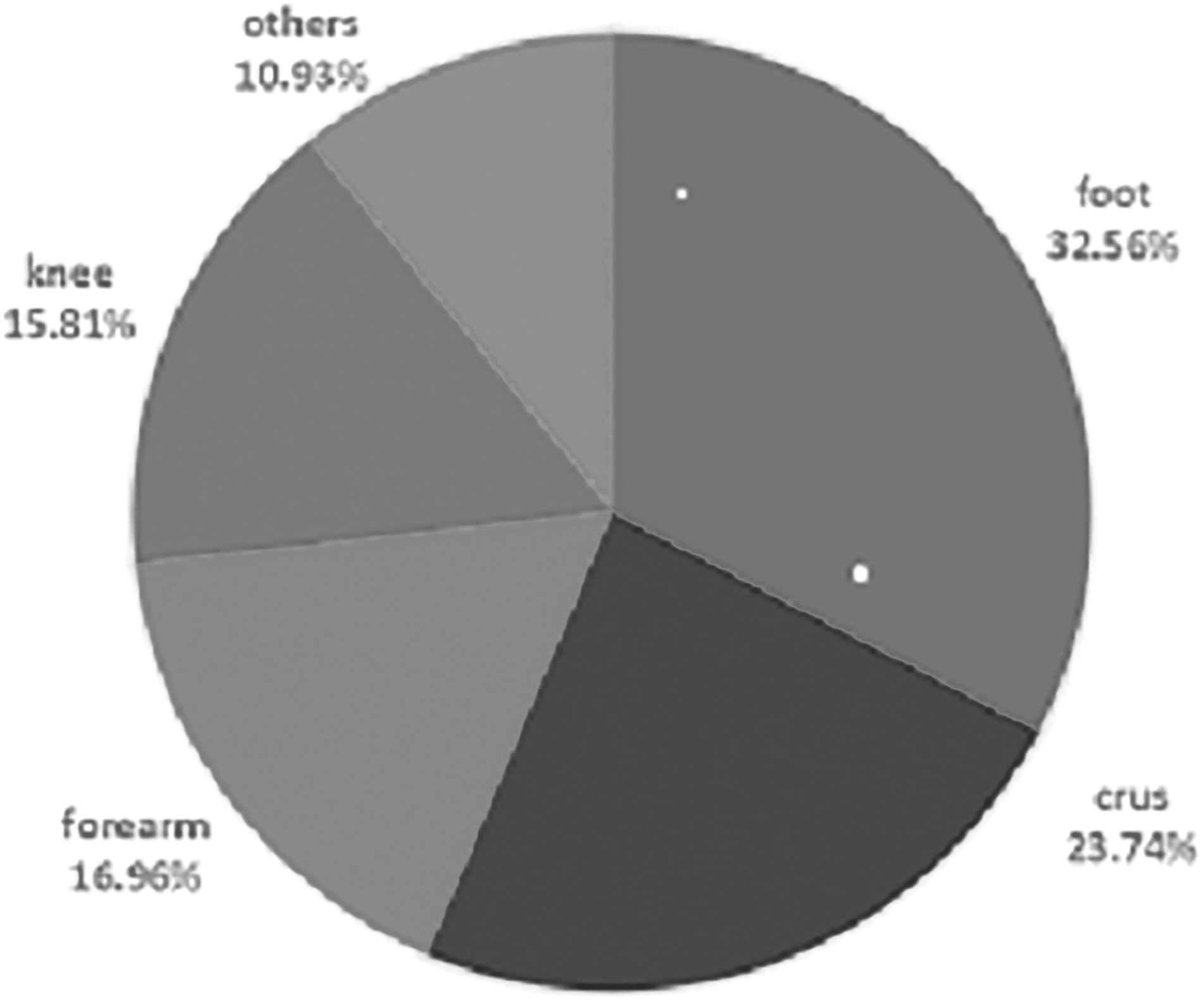
Surgical site distribution of mixed infection.
Distribution of Bacterial Species
There were 2-7 kinds of bacterial infections in each wound, of which two kinds of bacteria caused the most infections, accounting for 65.1% of the analyzed cases. With the increase in the number of strains, the number of infections decreased. There were four combinations of pathogenic bacteria: all gram-negative bacteria (55.81%), mixed gram-negative bacteria and gram-positive bacteria (30.23%), positive gram-positive bacteria (12.79%), and mixed gram-positive bacteria and fungi (1.16%). There are only two combinations of positive bacteria in the combinations of all gram-positive bacteria, but not in the combinations of all gram-positive bacteria. Mixed infections caused by more than two gram-positive bacteria were found (Table 2).
Combination Mode of Bacterial Species
Numb = number of strains, G+ = gram-positive bacteria; G— = gram-negative bacteria.
Drug resistance of pathogenic bacteria
Gram-negative bacteria showed good susceptibility to cefoperazone/sulbactam sodium (11.1%) and meropenem (13.3%) and drug resistance to ampicillin (82%), aztreonam (70%), and amoxicillin/clavulanate potassium (75%) (Table 3). Gram-positive bacteria were highly susceptible to linezolid (0%). Furantoin (resistance rate 0%) showed good sensitivity, and ampicillin (resistance rate 100%) and amoxicillin/clavulanate potassium (75%) had high drug resistance (Table 4). This is consistent with the bacterial resistance of 447 cases of single bacterial surgical site infections during the same period (Table 5). Patients with mixed incision infection were defined as patients with simple postoperative infection. The 95% confidence interval for extended hospital stay was (9.8-20.6) days.
Resistance of Gram-Negative Bacteria to Antibiotic Agents
Resistance of Gram-Positive Bacteria to Antibiotic Agents
Numb. = number of plants; R = drug resistance rate; “-“ = not applicable.
Drug Resistance of Single Bacterial Surgical Site Infections in Orthopedics
Num = number of bacteria tested for drug sensitivity; R = drug resistance rate.
Discussion
Our results revealed the presence of two to seven kinds of bacterial infections in each wound, of which two kinds of bacteria, accounting for 65.1%, caused the most infections. The number of infections decreased as the number of strains increased. The four combinations of pathogenic bacteria present in our study included all gram-negative bacteria, mixed gram-negative and gram-positive bacteria, all gram-positive bacteria, and mixed gram-positive bacteria and fungi. In particular, only combinations of two gram-positive bacteria were found in mixed infections caused solely by the combination of pure gram-positive bacteria, and no mixed infections caused by more than two gram-positive bacteria were found.
In the ecosystem of orthopedic surgical sites, when the absolute amount of living space and nutrients is insufficient, two or more microbial groups compete for the same resources. Antagonistic micro-organisms can also capture water and nutrients, occupy space, consume oxygen, and other resources by rapid growth and reproduction to eliminate other groups of pathogens in the same habitat [5,6]. These resources include nutrients, oxygen, and space. Therefore, competition types are divided into nutritional competition and spatial competition. This competition results in fewer infections as the number of strains increase.
No relevant literature reports that the coexistence of more than two gram-positive bacteria will lead to strong inter-specific competitions, which limits their strains. This may be related to the overall infection of bacteria—mainly gram-negative bacteria. From 2012 to 2017, 86 patients experienced mixed incisional infections after orthopedic operation. In all, the recorded 218 strains of bacteria, including 152 strains of gram-negative bacteria (69.72%), 65 strains of gram-positive bacteria (29.81%), and one strain of fungus (0.47%), confirm the report that the main infection after orthopedic surgical procedures is gram-negative bacterial infection.
E. cloacae, S. aureus, P. aeruginosa, E. coli, and Baumann/A. haemolyticus were the most common mixed infections in our hospital. This is generally consistent with the reported pathogenic bacteria in most orthopedic surgical site infections [7–9]. The foot, leg, forearm, and knee were the most common sites of infection. Gram-positive bacteria were susceptible to linezolid and furantoin, ampicillin, and amoxicillin/clavulanate potassium. Gram-negative bacteria are highly sensitive to cefoperazone/sulbactam sodium and meropenem and fairly sensitive to ampicillin, aztreonam, and amoxicillin/clavulanate potassium. This is consistent with the bacterial resistance of 447 cases of single bacterial surgical site infections during the same period.
The distribution, quantity, and drug resistance of bacteria in mixed surgical site infection after orthopedic operation are not significantly different from those caused by a single pathogen because of the interaction between pathogens. Mixed infections of orthopedic surgical sites form a small ecosystem. Its composition and stable population dynamics ultimately come from the interaction between organisms [10]. Various kinds and high concentration of micro-organisms exist in the biologic environment, but the existing and relatively small available space enables coevolution with unique physical and chemical interactions among species.
Some microorganisms have evolved mutually or even synergistically to promote cohabitation and efficient utilization of metabolic byproducts in the same ecosystem, while others have developed competitive antagonistic methods in the process of cocloning. One bacterium can affect the niche of the reproduction of another bacterium in the wound, making it easy to be colonized by pathogenic bacteria or caused by two or more non-pathogenic micro-organisms. For example, cystic fibrosis in the lung is often caused by P. aeruginosa, S. aureus, Haemophilus influenzae, Burkholderia cepacia, and other bacteria. These bacteria developed increased resistance through metabolic feeding or quorum sensing (QS)-related signaling mechanisms, bacterial tolerance, and biofilm development [11–14] in adults. S. epidermidis and S. aureus compete for nasal mucosal colonization and ESP-serine protease-producing S. epidermidis strains to eradicate S. aureus nasal colonization.
Mixed surgical site infection after orthopedic operation is not uncommon because the site is close to the body surface. Because S. aureus has always been a common bacterium in orthopedic surgical site infections, Regev-Yochay et al. [15] and Bogaert et al. [16] investigated another interaction: S. aureus carriers and the effect of pneumococcal conjugate vaccination on the increase of the carrying capacity of S. aureus and S. aureus-related diseases, and microbial interference with the protection ability of S. pneumoniae carriers, respectively.
Armbruster et al. [17] found that secretory staphylococcal protein ASpA inhibited biofilm formation of specific clinical isolates of P. aeruginosa and phagocytosis of neutrophils to all clinical isolates tested. Through reverse transcription polymerase chain reaction and other methods, Deng et al. [18] found that the cis-2-dodecanoic acid produced by B. cepacia mediated the communication with P. aeruginosa by interfering with the QS system and type III secretory system, which resulted in biofilm formation and virulence of P. aeruginosa. For down-regulation of force factor synthesis, Alex et al. [19] found that compared with single infection, the adhesion of E. coli and Citrobacter freundii to HeLa cells increased significantly. Moreover, E. coli carrying F-pili gene (traA) could form bacterial aggregates only in the presence of C. freundii.
Meanwhile, scanning electron microscopy analysis showed that both bacterial aggregates and enhanced biofilms formed by coinfection were mediated by flexible pili. In addition, the use of specific inhibitors of F-pili significantly reduced the formation of mixed infectious bacterial membranes. The results show, however, that the distribution, quantity, and drug resistance of mixed infections and post-operative infections caused by a single pathogen do not differ significantly because of the interaction between pathogens.
Our study shows that mixed surgical site infection significantly prolongs hospital stay. This may be related to the poor basic condition of patients with mixed infections, low immunity, and the difficulty of single antibiotic agents to cover the sensitive range of their bacteria. Other studies speculate that when mixed infections are found, doctors may extend the hospital stay to ensure infection control even after reaching discharge indications for fear that the infection will not be controlled completely.
Mixed infection after orthopedic operation is caused by many kinds of pathogenic bacteria and various combinations of pathogenic bacteria, which are difficult to control and prolonge hospitalization duration. It is difficult for conventional single or compound antibiotic agents to target surgical sites simultaneously caused by gram-negative bacteria and gram-positive bacteria. Moreover, published literature shows that more than two antibiotic agents are independent risk factors for infection after orthopedic surgical procedures, and various antibiotic agents aggravate the burden of patients, which necessitates strict matching of antibiotic agents sensitive to pathogenic bacteria according to drug sensitivity, so as to avoid unreasonable matching of antibiotic agents [20].
Age >60 years, body mass index >26.5 kg/m2, hypertension, diabetes mellitus [21], coronary heart disease, chronic obstructive pulmonary disease, malnutrition, hypoproteinemia, and so on, are all risk factors of infection after orthopedic operation [19]. (Thus, it is necessary o improve immunity by active symptomatic treatment before operation.
Factors affecting the contact probability and time of pathogenic bacteria can be prevented by adjusting the treatment plan and making full use of protective factors, such as controlling the operation duration and laminar flow in operating rooms. In addition, the presence of infection before operation is an important reason for early infection after operation; thus, it is necessary to screen for occult infection to avoid infection.
Conclusion
The importance of multi-microbial diseases and interaction between human health and disease-related microbial communities have been recognized by the medical community. The multi-microbial causes of diseases and the effects of treatment, prevention, and prognosis have also been considered. Actively enhancing the immune capacity of patients and actively controlling factors affecting the probability of contact and time of pathogenic bacteria are strategies to prevent infections.
Our study indicated that the distribution, quantity, and drug resistance of bacteria in mixed surgical site infection after orthopedic surgical procedures are not significantly different from those caused by a single pathogen because of the interaction between pathogens. Various kinds of pathogenic bacteria are present in mixed infections after orthopedic operations. These bacteria are difficult to control, resulting in significantly prolonged hospitalization.
Use of conventional single or compound antibiotic agents may be ineffective in managing surgical sites, when both gram-negative and gram-positive bacterial infections are present. This necessitates that antibiotic agents sensitive to pathogenic bacteria should be matched strictly according to drug sensitivity to avoid ineffective antibiotic matching and minimize unnecessary administration of antibiotic agents to patients, which would create a greater burden to the body.
Footnotes
Acknowledgments
The datasets used or analyzed during the current study are available from the corresponding author on request.
Funding Information
This project was supported by the Foundation of Health Commission of Jiangxi Province (20203120) (2016A073) and the Foundation of Education Department of Jiangxi Province (GJJ160127).
Author Disclosure Statement
No competing financial interests exist.