
Abstract
Abstract
Background:
Faulty cleaning of surgical instruments may lead to corrosion damage and a higher risk of surgical site infection. We have developed a method in which each instrument has an attached radiofrequency identification (RFID) tag for individual management. However, because of the structure of the instruments, a risk of corrosion from poor cleaning exists; therefore, observation during long-term usage is necessary.
Methods:
The cleaning effect at the jig of the RFID tag was verified by the amount of residual protein left by various cleaning methods. In our investigation of long-term usage, we examined 94 surgical instruments with RFID tags used in the operating room for 50 months employing a microscope to identify any corrosion at the jig.
Results:
The method using a washer disinfector (WD) was found to be highly effective. From observation after long-term usage, friction by the RFID tag occurred in about 70% of the jigs. However, no pitting or general corrosion was seen.
Conclusions:
When WD is used properly, there is only a minor risk of residual protein, and corrosion does not occur even with long-term use. By using surgical instruments with RFID tags, it is possible to determine the number of uses and the history at the individual level. This facilitates operation of safe surgical instruments by limiting the number of times a particular instrument is used.
According to incident reports, instruments or sponges are retained in approximately one in every 10,000 surgical procedures that involve an open cavity [1,2]. In addition, one-third of these cases involve surgical instruments. Remnants in bodies should not be allowed, as they lead to large physical, financial, and trust casualties for both the patients and the medical staff and medical facilities [3]. The presence of remnants within the body may occur because of human error in counting the number of pieces of equipment before and after the surgical process or the mixing of incorrect surgical implements in the set provided during the surgical process. For that reason, it is necessary to manage the equipment using an individual-item control system that reads the information of each surgical instrument [4]. Systems in which RFID tags are affixed to surgical instruments are being used in operations in order to avoid such errors [5,6]. Using RFID techniques with surgical instruments can aid in instrument counting before and after surgery, set-building of instruments, automated record capture and tagging of patient information, and maintaining the use history and traceability of surgical implements and the number and duration of use of instruments.
The occurrence rate of serious complications attributable to surgical site infection (SSI) during the peri-operative period is 3%–17% [7]. An SSI might occur owing to the presence of residual proteins because of insufficient cleaning of surgical instruments, and thus, a guideline regarding the cleaning method has been designed [8]. In addition, residual protein causes corrosion of surgical instruments because it becomes concentrated during the sterilization process, and corrosion is thought to be associated with damage to instruments [9]. This is because corrosion can cause a reduction in the strength of the instruments, thereby damaging them; however, this phenomenon has not been investigated fully.
Corrosion results from the adhesion of chlorides such as from blood or bodily fluids on the surgical instruments; it is believed that chlorides can remain on the instruments owing to insufficient cleaning or inappropriate handling. The concerns associated with surgical instruments having an attached RFID tag, as developed in this study, is that the tag may separate from the instrument because of corrosion and the lack of cleaning of the RFID tag jig.
Surgical Instrument with Attached RFID Tag
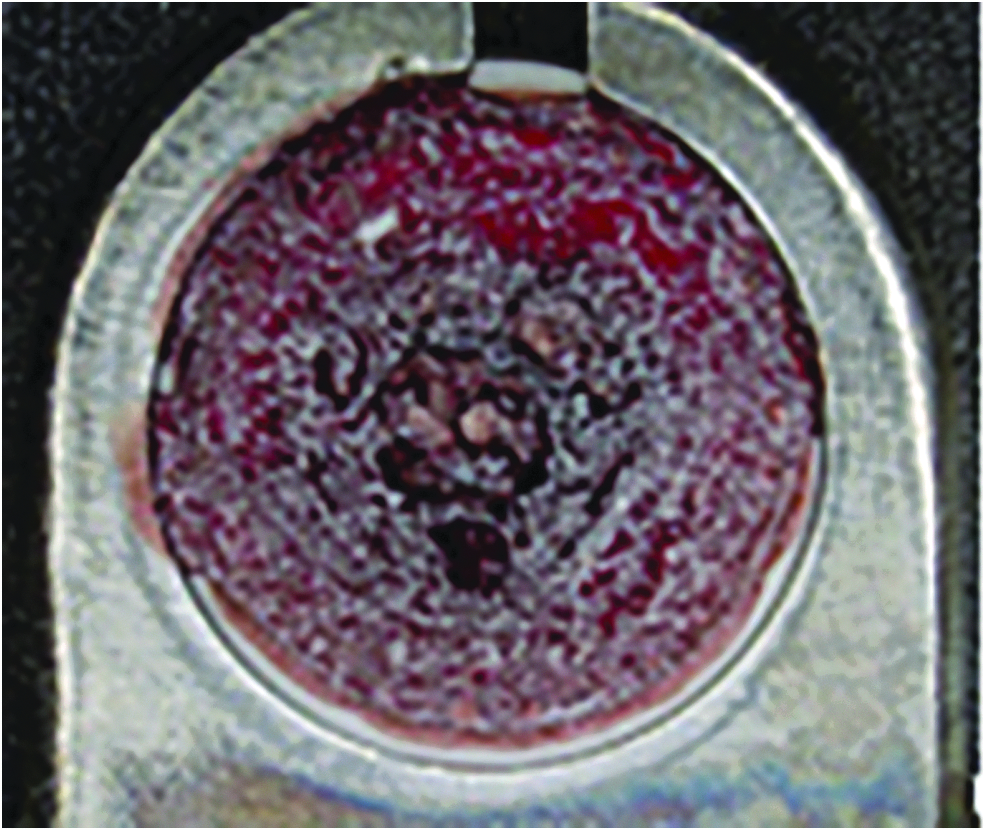
Figure 1 shows the exterior of a surgical instrument and the RFID tag attachment jig (arrow). The jigs are fixed on instruments by laser welding. One of the parts that may be cleaned insufficiently is the box-lock section, such as those present on forceps. Jigs have a hard-to-clean structure similar to the box-locks; thus, if chlorides remain on the surface, corrosion may occur, and the jig may fall out after long-term use. If the attachment of the jig is not sufficiently tight, moisture may enter the gap, thereby increasing the risk of corrosion and subsequent damage.

Surgical instrument with attached RFID and jig (arrow). Color image is available online.
The contamination risks caused by insufficient cleaning of surgical instruments are evaluated before introducing the instrument into the operating room, but the corrosion risk of instruments considering a combination of ultrasound and manual cleaning has not been investigated extensively [10]. Furthermore, evaluation of corrosion resulting from long-term use has not yet been performed.
In this study, verification was conducted in accordance with guidelines of the amount of residual protein left behind following cleaning of the jig by different methods on site in medical facilities. Further, corrosion of the jigs during long-term use was evaluated.
Methods
Evaluation of cleaning for surgical instruments having attached RFID tags
Fixation of Simulated Contaminants for Jigs
At present, it is recommended that primary cleaning of surgical instruments not be performed in environments involving patients, such as in the operating room [11]. Therefore, over time, blood adhering to the surgical instruments may congeal, and corrosion may occur. As an index to quantify the impact of cleaning of surgical instruments, the limiting value of the residual protein amount on the surgical instrument after washing has been set to 200 mcg (limit value) per surgical instrument, and the acceptable value is 100 mcg [8].
In this study, blood was affixed to the jig components, and evaluation was carried out in terms of the residual protein after cleaning of the instruments, as shown in Fig. 2. For the cleaning evaluation, a mock contaminant was created using whole sheep blood treated with heparin and 1% protamine sulfate in a 10:1 ratio. To assume the worst environment, as shown in Figure 2, 25 mcL of the contaminant was applied to the surface of the RFID tag, and after 2 min of direct heat treatment at 100°C, the same treatment was performed on the other side. As can be observed in Figure 2, the contaminant adhered to the RFID tag and in the space between the areas of attachment.
Jig for attaching RFID tag after contaminants added. Color image is available online.
Cleaning assumed to occur at a medical site
The cleaning appraisal guidelines state that residual protein should be cleaned off using washer disinfectors (WD) [8]. In this study, we considered combining possible cleaning methods to clarify the effectiveness. Thus, evaluations were performed for seven types of cleaning methods to compare their efficacy: WD, ultrasonic, manual + ultrasonic, thermostat chambers + ultrasonic, manual + thermostat chambers + ultrasonic cleaning group, thermostat chambers + WD, and no cleaning.
The WD used DECOMAT 8666, manufactured by Getinge Co., Ltd., and the ultrasonic cleaner used MU1100R, manufactured by Sharp Corporation.
In this experiment, based on an actual clinical cleaning process, the use of WD involved a two-minute pre-cleaning using cold water and a wash at 93°C for 10 minutes. The water temperature when introducing washing agents was set to be 40°C, and the concentration of the agents was 0.5%. Subsequently, a rinse at 60°C was carried out twice followed by a rinse at 70°C for one minute.
The cleaning effect of WD differs according to the loading state. In this experiment, we assumed the worst-case contamination; however, because the cleaning must have the best effect, contaminated surgical instruments with RFID tags were placed on the top level of the WD with the cleaning holders, etc., so that that the WD jet water stream could reach them sufficiently.
The group of instruments subjected to ultrasonic cleaning underwent a 15-minute cleaning with 0.5%-adjusted low-foaming alkali detergent (pH 11.4–12.4), and three rinses. To recreate ultrasonic cleaning, at the final rinse, reverse osmosis water was used. While cleaning, the effect of running water was negated as much as possible to study the effect only of the ultrasonic waves, and no swing was performed.
Manual cleaning involved the usual cleaning performed by staff experienced in cleaning surgical instruments. No special instructions were given regarding the cleaning method.
Water at 40°C was placed in the thermostat chamber, and a smooth water stream flow was used to soak the instruments. The thermostat chambers were used to reduce the adhesiveness of the attached contaminants and to enhance the cleaning effect.
The non-cleaned group underwent no cleaning process, and surgical instruments were left contaminated with the mock blood.
The sample instruments used were pairs of forceps used in surgery. The sample sizes were as follows: 20 in the WD group, 10 in the ultrasonic cleaning group, 5 in the manual cleaning + ultrasonic group, 10 in the thermostat chamber + ultrasonic cleaning group, 5 in the manual cleaning + thermostat chamber + ultrasonic cleaning group, 5 in the thermostat chamber + WD group, and 5 in the uncleaned group.
Methods to extract and measure the residual protein
The extraction and measurement of residual protein amounts were performed according to the cleaning guidelines. The method is described in detail below. After cleaning, surgical instruments that had received the mock contamination were inserted into a polyethylene bag containing 10 mL of 0.2 mol/L sodium hydroxide. Then they were placed in a circulative thermostat chamber, which was maintained at a temperature of 50°C. While lightly mixing the materials for two hours, the residual protein was extracted from the instruments [8]. An additional two hours was assigned to this step because the mock contaminants had adhered strongly to the instruments, and thus sufficient extraction time was required.
For detection, the Coomassie brilliant blue (CBB) method was used: 1 mL of the extracted liquid and 3 mL of the CBB reagent were mixed, and after being left at room temperature for 20 minutes, the measurement was performed using a spectrophotometer (Shimadzu Co.) at an absorption wavelength of 595 nm. The Coomassie Protein Assay Kit® (Thermo Fisher Scientific Co.) was used in the CBB method, and bovine serum albumin was employed to construct the protein standard curve. The detection limit of the CBB method is 10 mcg, which implies that if the amount of residual protein is less than 10 mcg, the measured amount will appear as 10 mcg. With this method, the risk of corrosion generation on tag attachment parts owing to insufficient cleansing in long-term use was investigated considering different cleaning methods.
Long-term corrosion generation risk of attachment part of surgical instruments with RFID
Surgical instruments are expected to be used in various ways depending on the environment and cases. To investigate the risk of corrosion of the jig of RFID tags during long-term use, direct investigation of the corrosion is more suitable than a biochemical approach such as measuring the residual protein.
This study differs from others in that each surgical instrument had an attached tag that enabled its full use history to be maintained. Jigs were removed from 94 surgical instruments being used in operations at the Japanese Red Cross Kyoto Daini Hospital, and the joints and jigs between the tags and the surgical instruments were observed. The instruments used in this study were cleaned and sterilized according to hospital guidelines. Specifically, they were cleaned by washing with WD in the central supply department in the hospital. Sterilization was carried out three times pre-vacuum and once post-vacuum at 135°C for eight minutes, followed by drying by eliminating air.
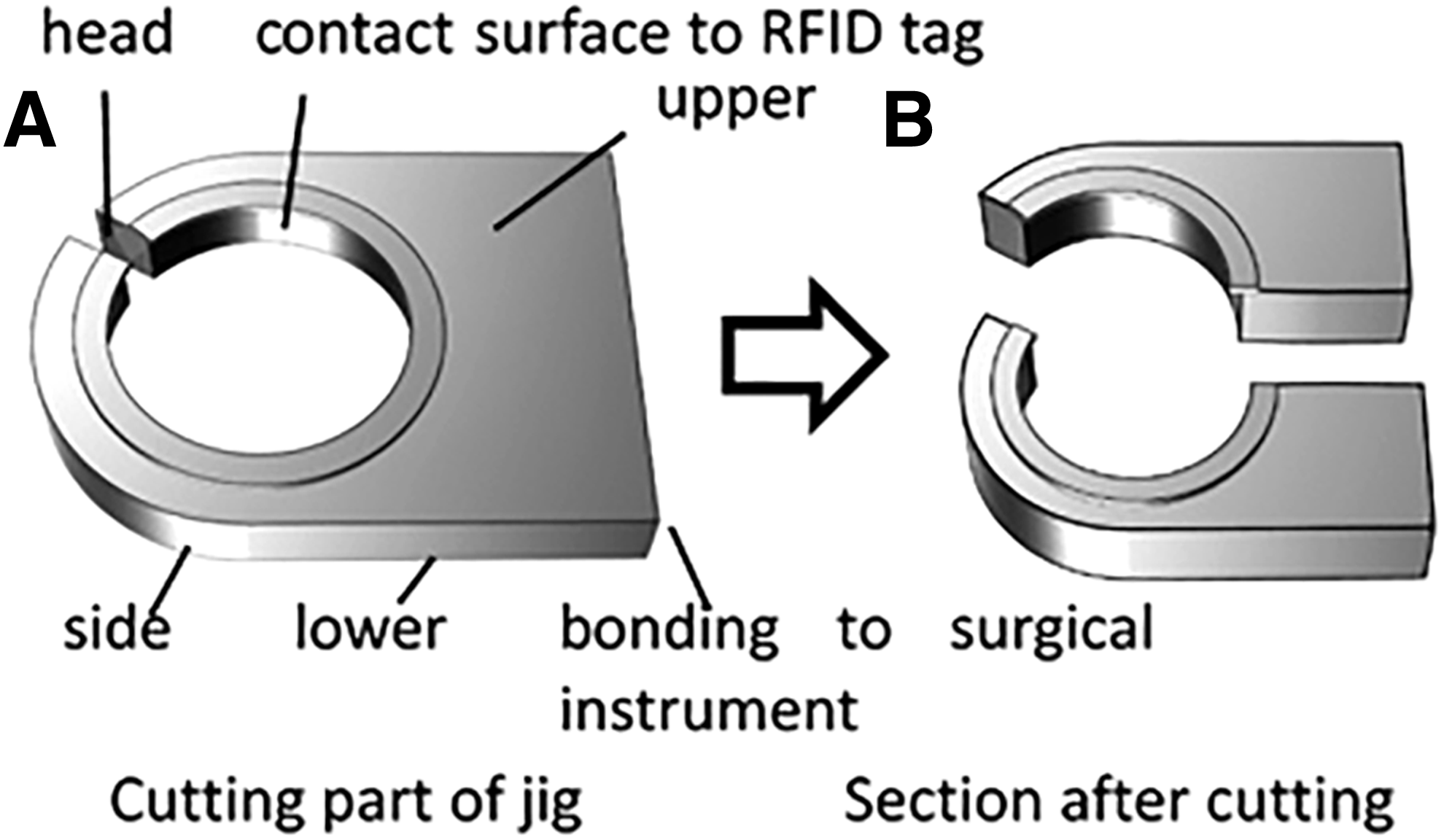
The jigs attached to the surgical instruments were removed, as shown in Fig. 3A, and cut at the half position of bonding to the instrument, as shown in Fig. 3B. Corrosion analysis was carried out at six sites (Fig. 3). A laser microscope (VK-9700, KEYENCE Co., Osaka, Japan) was used for shape analysis of the discoloration and friction marks.
Cutting (
Seventeen kinds of instruments were used 160 times on average for about 50 months. Observations were made of the external appearance using a stereoscopic microscope. Corrosions at the joints of the tag and the instruments, as well as the corrosion depth, were evaluated using a confocal laser scanning microscope.
Results
Effects of cleaning methods for surgical instruments with attached RFID tag
Table 1 lists the mass of residual protein left by each cleaning method. It can be seen that the mean masses of residual protein ± SD complied with the guideline-acceptable value in the following groups: WD (35.6 ± 23.7 mcg), thermostat chambers + WD (10.1 ± 0.5 mcg), thermostat chambers + ultrasonic cleaning (71.7 ± 53.9 mcg), and manual cleaning + thermostat chambers + ultrasonic cleaning (25.5 ± 25.3 mcg). The amount of protein complied with the limit value in the manual cleaning + ultrasonic cleaning group (101.0 ± 126.8 mcg). In these five groups, none of the measurement results of the WD group or the thermostat chambers + WD group exceeded the acceptable value. All the measurement results of the manual + ultrasonic cleaning group exceeded the limit value by 40% (largest 273 mcg), those of the thermostat chambers + ultrasonic cleaning group exceeded the acceptable value by 33% (largest 175 mcg), and those of the manual cleaning + thermostat chambers + ultrasonic cleaning group exceeded the acceptable value by 0 (largest 77 mcg).
Mass of Residual Protein According to Cleaning Method
Observation of corrosion during long-term use of RFID tag with jig
The bonding to the surgical instrument and the contact surface with the RFID tag of all jigs were observed using a stereoscopic microscope. As an example, Figure 4 shows an enlarged view obtained via the stereoscopic microscope of the bonding to the instrument and the contact surface with the RFID tag of the instruments with an tag used 199 times in 50 months. The interfaces of the 94 surgical instruments with the jig had some discoloration, but corrosion was not observed, as seen in Fig. 4 (above).
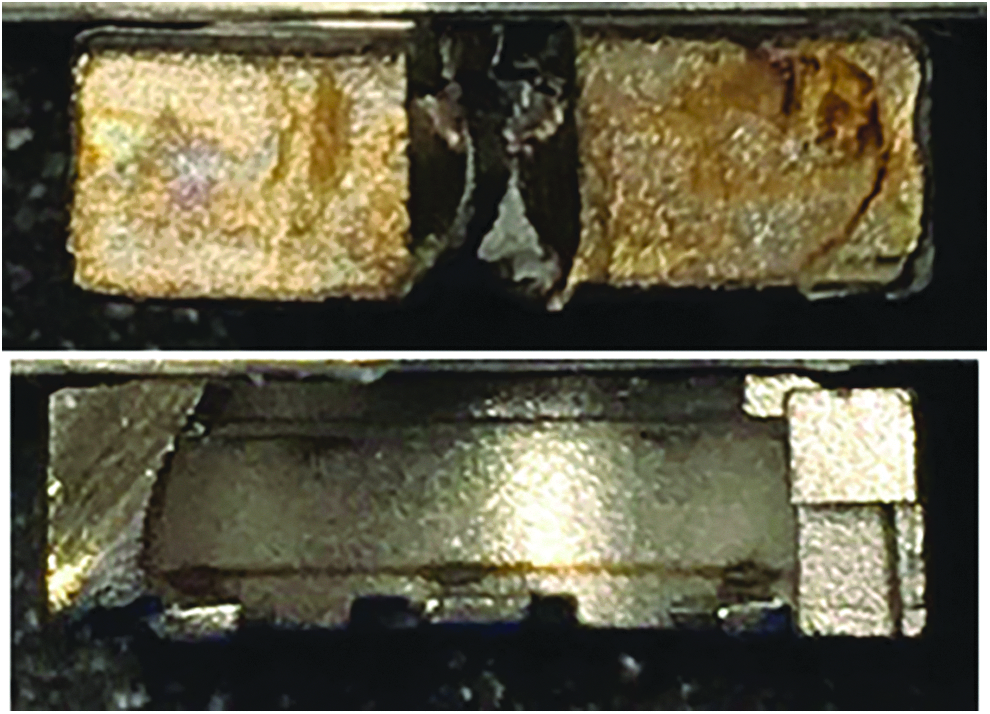
Bonding to surgical instrument (above) and contact surface of RFID tag (below) of jig and surgical instrument. Color image is available online.
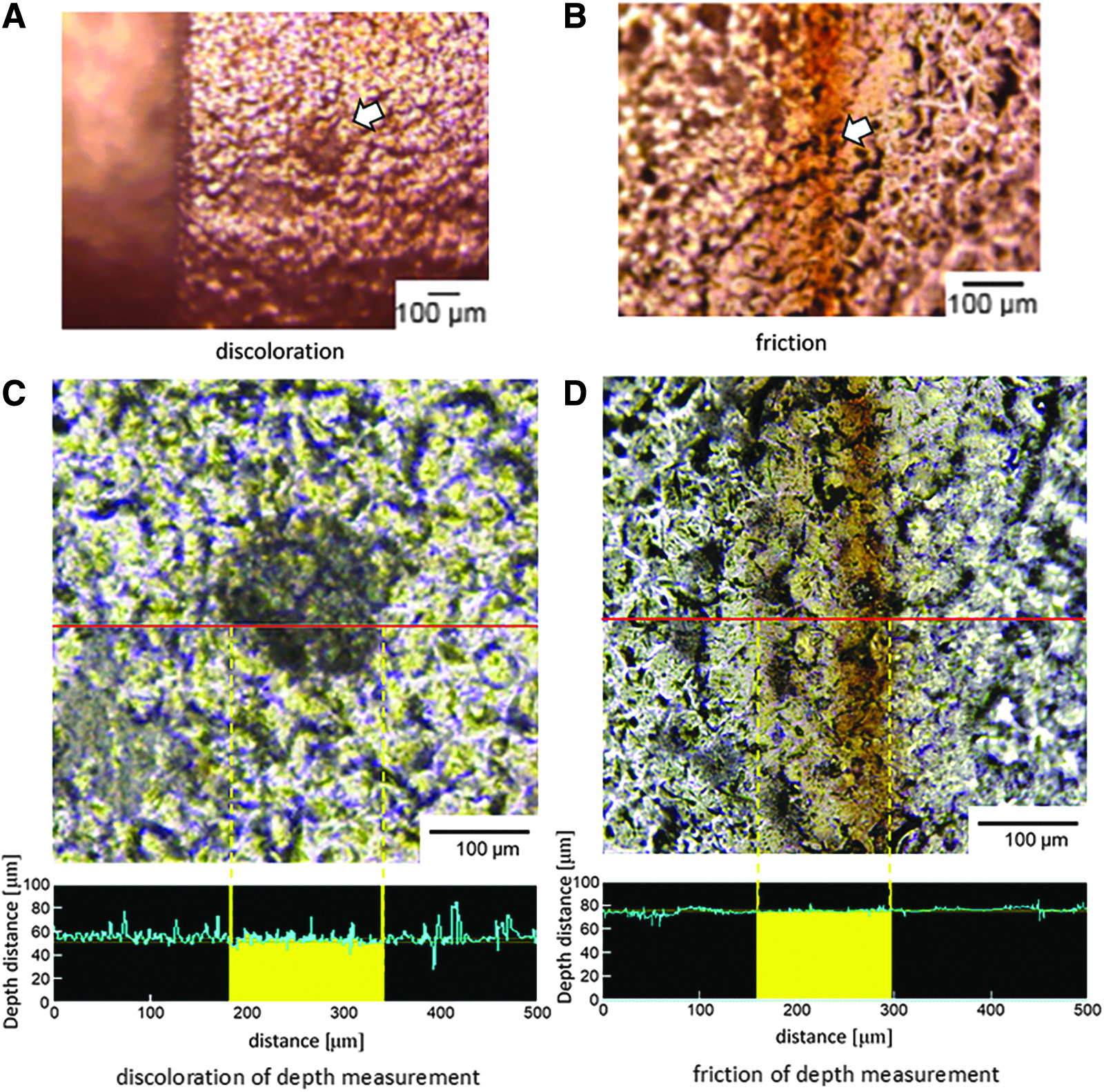
As shown in Fig. 4 (below), the stereoscopic microscope was used to view the surface of the interface between the RFID tag and the jig when the possibility of discoloration or corrosion was noted from observation; a laser microscope was used to view the discoloration (as in Fig. 5A) and friction with the RFID tag (as in Fig. 5B).
Damage to instruments with time. (
There was a less than a 5% frequency of discoloration and friction on the top, bottom, side, and head of the jig. The occurrence of discoloration on the bonding with the instrument was less than 20%. The discoloration of the contact with the RFID tag was less than 13%, but the rate of friction was 60% for sub-5-mm jigs and 20% for jigs 5 mm or larger. The rate of occurrence of friction and discoloration was 70% of the occurrence rate on bonding with the instrument and contact surface with the RFID tag.
A confocal laser microscope was used to measure the depths of the point of jig friction and discoloration on jigs to confirm the presence of pitting corrosion. Figures 5A and 5B show the magnified images, whereas Figs. 5C and 5D show the results of depth measurements. The depth could not be observed, and so was understood to be less than 20 mcm. The detection limit of the confocal laser microscope used is 20 mcm. All these observations were performed on the suspected area in the magnified images, and the same result was obtained in all cases.
Discussion
Effects of cleaning by different methods
In a previous study in the United Kingdom, an estimated 15% of new surgical instruments were found to be defective, and the incidence of defects increased as a function of the length of time each instrument had been used [12]. In a study in Japan, the breakage rate of instruments within two years was 9.1%, and two near-miss incidents (10 in 100,000 operations) were potentially critical [13].
As a cause of breakage, the presence of residual protein on surgical instruments increases the removal of metal ions, thereby increasing the rate of corrosion of certain instruments made of stainless steel [14]. In other words, instruments undergo pitting owing to adhesion of chloride-containing blood or physiologic saline. In addition, residual proteins may promote adhesion of bacteria through specific adhesion receptors, such as the fibronectin-binding protein found in Staphylococcus aureus [15]. Depending on the position and size of the pitting corrosion, cleaning may be insufficient. For corrosion, it was understood that where a high concentration of chloride is attached to a surgical instrument, the material of a typical instrument; i.e., SUS304, will undergo pitting corrosion.
This study minutely examined the effect of cleaning the RFID tag attachment site and is the first to conduct experiments to investigate the risk of corrosion from direct and sustained use. In terms of the results of the mass of residual protein found during investigation into the effects of cleaning, groups that used WD exceeded the guideline target amount, indicating satisfactory cleaning. In particular, it was observed that by softening the firmly stuck imitation blood beforehand in a thermostat chamber, washing became more effective.
In medical facilities without WD, ultrasonic or manual cleaning methods commonly are used. In our experiments, ultrasonic cleaning did not comply with the acceptable limit, and even when combined with manual methods, 40% of the instruments did not comply with the limit. This is not a satisfactory result. However, by combining ultrasonic cleaning with a thermostat chamber, compliance with the acceptable limit was achieved. By further combining this with manual cleaning, the target amount was met.
According to the report setting Japan's cleaning evaluation guidelines, by washing surgical instruments tainted with blood after routine surgery with WD, 7.7% of instruments were within the 100–200 mcg limit. Compared with these results, the RFID tag jig (which is thought to be cleaned insufficiently, as with the box-lock of forceps) can receive satisfactory cleaning.
From the above data, the results of cleaning surgical instruments having an RFID tag using WD have been made clear, as has the fact that using a thermostat chamber can further improve cleanliness. This experiment was designed to maximize the cleaning potential of WD, but it is supposed that by putting in too many surgical instruments, or piling them up, cleanliness will suffer. It is suggested that by using a preparatory constant-temperature bath, the risk of insufficient cleaning will decrease the risk of corrosion in RFID tag jigs from long-term use.
Risk of occurrence of corrosion of RFID tag jig in long-term use
The RFID tag jigs are installed by laser welding to the surgical instrument. It is thought that if the welding is insufficient, or if there is a gap inside, blood or other chlorides will get trapped, thus leading to a risk of corrosion. The washing process of instruments having RFID tags was conducted in accordance with the process used in the medical institutions that used WD; the instruments were washed following certain rules about their placement. By employing this cleaning method, even when using RFID-tagged surgical instruments over the long term, the interface between the instrument and the jig showed no corrosion, and there was no risk of it falling off.
There was a less than 5% frequency of discoloration and friction on the top, bottom, side, and head of the jig. The occurrence of discoloration of the contact with the RFID tag was less than 13%. The discoloration and friction shown in Fig. 5 can be viewed as the start of corrosion. However, the depths of the point of jig friction and discoloration were confirmed with a confocal laser microscope as being less than 20 mcm.
From its appearance, the change was suspected to be the metal surface being broken down and undergoing elution owing to the presence of chloride ions. We theorize that if it was the metal surface being broken down, with appropriate usage, a permanent new surface would form, so corrosion would not occur. As the interface between the jig and the RFID tag is covered with blood during use, it is thought that it is easy for corrosion to occur during or after surgery before washing. In these results, for RFID-tagged instrument jigs used more than once a week for four years, no downward corrosion was seen; and indeed, there was no corrosion at all. In other words, there was no risk of infection or falling out because of advanced corrosion from long-term insufficient cleaning.
In this study, when an RFID tag was attached to a surgical instrument, the usage frequency, the patient, the date, and the procedure were recorded automatically. When investigating the risk of corrosion with a laser microscope, precise information on usage frequency was available, so it was possible to evaluate the risks of harmful phenomena related to RFID-tagged instruments. This risk was found to be low.
Clearly, with an RFID tag attached, as the usage frequency (down to the usage during surgery) was available, appropriate maintenance settings and risk of damage to the instrument could be made clear [6]. In this study, cleaning was carried out with WD, and even when an implement had been used 200 times, there was no corrosion. However, it appears that medical institutions that use the same method find that there is corrosion below this frequency, so there might be an issue with the cleaning process, maintenance method, or handling of the instrument during surgery. To prevent SSI and damage to the surgical instrument, guidelines targeting corrosion are sought.
Study limitations
This experiment examined RFID-tagged instruments at one medical institution, and although the procedure was in accordance with the cleaning guidelines, it may be that the long-term corrosion risk is limited. If there is an institution that is not following the cleaning guidelines, it is predicted that there will be a high risk of SSI, and as such, the possibility that the rate of harmful phenomena in RFID-tagged instruments would rise cannot be denied.
As well as being caused by washing, the risk of corrosion is linked to the handling of the instruments during surgery. Primary causes of insufficient cleaning are human, such as not obeying cleaning order or usage protocols, as well as mechanical issues with the cleaning machines themselves. From this experiment, it became clear that to lower these risks, using a constant temperature bath was effective, and it is thought that this also would be effective in reaching hard-to-wash places such as the RFID tag fitting and box-lock.
Conclusion
We developed a method in which RFID tags are attached to surgical instruments and realized traceability in long-term use. In this study, to promote effective usage of RFID-tagged surgical instruments, a comparison of cleaning methods based on guidelines was undertaken and the risk of the harmful phenomenon of corrosion from long-term use examined.
It was established that cleaning efficiency could be enhanced by adopting a method following guidelines and using a thermostat chamber. Further, a more precise method of routine cleaning of instruments prior to sterilization in the autoclave was presented. In long-term use, corrosion of the jig was not observed, and the RFID tag attachment had no effect on slippage.
Footnotes
Acknowledgment
We thank Shinichi Tanaka, Masatake Shimizu, and Ryohei Kanda for their contributions to this study.
Author Disclosure Statement
This study was supported in part by JSPS KAKENHI Grant Numbers JP 15K12608 (K.Y.) and 17K12806 (K.K).
No competing financial interests exist.