
Abstract
Abstract
Background:
In August 2010, the U.S. Food and Drug Administration issued draft guidelines for developing antibiotics for treating acute bacterial skin and skin structure infections (ABSSSI), with the outcome measure of such treatment relying primarily on the cessation of spread or on the decrease in size of skin lesions at 48–72 h after the initiation of such treatment. In 2012, the Foundation for the National Institutes of Health proposed an interim outcome measure defined as a reduction in lesion size by ≥20% at a 48–72 h examination. These recent changes make it necessary to identify reliable methods for measuring the lesions in acute infections of the skin.
Methods:
In the first study of the Efficacy and Safety of 6-day Oral Tedizolid in Acute Bacterial Skin and Skin Structure Infections vs. 10-day Oral Linezolid Therapy (ESTABLISH–1), the sizes of ABSSSI lesions were evaluated with the two methodologies of: (1) Digital planimetry (DP) of photographed lesions, and (2) a ruler technique (RT) with measurement of the longest head-to-toe length and greatest perpendicular width of lesions, to compare the respective response rates of lesions to the two antimicrobial regimens in the study.
Results:
The RT method and DP showed similar percentages of subjects in which treatment stopped the spread of ABSSSI lesions (93.2% vs. 94.2%, respectively) but showed less agreement for a reduction in lesion size, of ≥20% (87.7% vs. 62.0%, respectively) across all categories of lesions (cellulitis/erysipelas, major cutaneous abscess, and acute wound infection) at 48–72 h after the initiation of treatment.
Conclusion:
The results of the ESTABLISH–1 study show that both the RT method and DP are consistent and reliable techniques for measuring the sizes of ABSSSI lesions. Ultimately, changes in lesion size, rather than the absolute value of lesion size, will be used to assess the outcomes of treatment for ABSSSI in clinical research.
C
Methods for measuring skin lesions have been developed primarily to monitor the progression of healing of chronic wounds. With the measurement of lesion size being the primary means of assessing therapeutic effect in the treatment of ABSSSI, and in the absence of a gold standard for this, there is a need to identify measurement methods that reliably reflect the effect of treatments for ABSSSI. Methods for measuring chronic wounds range from simple to sophisticated and vary with respect to their accuracy, reliability, and objectivity. The degree of precision required in measuring such wounds depends on whether an accurate estimation of surface area is needed, such as in a research study, or whether a general understanding of wound healing progression is sufficient [5,6]. The ruler technique (RT), with measurement of the longest head-to-toe length and greatest perpendicular width of lesions, and digital planimetry (DP) (using acetate tracings or photographs), are the methods used commonly for assessing the sizes of chronic wounds in clinical practice [7]. The advantages and disadvantages of each method are described below and summarized in Table 1.
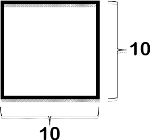
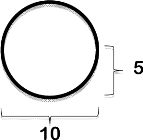
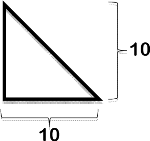
The RT method is the simplest method for measuring the sizes of skin lesions and determines their area through a manual measurement of their length and width (L x W) with a ruler or tape measure. A number of different measurement strategies can be used for the L x W method, including the longest head-to-toe length and longest perpendicular width of a lesion; the longest length and width perpendicular to one another; the longest head-to-toe length and greatest width at any angle; and the longest length and greatest width at any angle. A study done by Langemo et al. demonstrated that measurement of the longest head-to-toe length and greatest perpendicular width of a lesion was the most accurate method for all of the three wound shapes (symmetrical, L-shaped, and pear-shaped) in the study [8]. However, although it is simple to use and inexpensive to implement, the RT method is accurate mathematically only for rectangular or square lesions. Consequently, the more the shape of a lesion deviates from a rectangle or square, the greater is the potential for overestimation of its true surface area (Table 2).
Accuracy of range depends on number of photographs.
Percent difference is calculated as (ruler technique-digital planimetry)/(digital planimetry x 100).
L=length; W=width; r=radius.
Skin lesion surface area can also be determined by tracing the margins of the lesion on transparent acetate placed over the lesion and counting, on a grid, the number of square centimeters within the traced area. Although this method is relatively easy and has good reliability, variability in its results arises when determining whether or not to count partial squares within a trace [8,9]. Digital planimetry may provide a more precise and objective approach than the RT method with grid-square counting for calculating the surface area of wounds and is more amenable to calculating the areas of irregularly shaped wounds (Table 2) [10]. For DP, a digital rendering of the trace along the margins of a lesion is created, and software is used to calculate the wound surface area. In the case of photographs of lesions taken with a digital camera, PictZar CDM Software (Biovisual Technologies, Elmwood Park, NJ), provides a unique method of measuring these lesions' surface area without having to measure the distances between the camera lens and the lesions. However, a ruler in the same plane as the lesion is still required to accurately calibrate lesion sizes in the photographs made using this method [11].
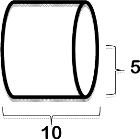
Both the RT method and DP use two-dimensional (2D) renderings of three-dimensional (3D) objects for calculating the sizes of lesions. As a result, patient positioning, the curvature of the body at the site of a lesion, the tapering of limbs, and skin folds are all confounders in calculating the surface area of a lesion with these methods [5,12]. Calculating the external surface area of an arm or leg (represented as a cylinder) is one of the most difficult of such measurements. Digital planimetry requires several photographs for adequate assessment of the surface area of a 3D object, and approximate length and width measurements made with the RT method may not accurately reflect the size of a lesion on a curved surface (Table 2). Stereophotogrammetry, which uses 3D surface imaging technology, can overcome some of the limitations of 2D renderings, but the method is impractical and expensive for clinical use.
In the first study of the Efficacy and Safety of 6-day Oral Tedizolid in Acute Bacterial Skin and Skin Structure Infections vs. 10-day Oral Linezolid Therapy (ESTABLISH–1), the sizes of ABSSSI lesions were assessed with the DP measurement of photographed lesions and with the RT method done with measurement of the longest head-to-toe length and greatest perpendicular width of lesions, to determine whether the response rates of chronic wounds to treatment in an acute setting were comparable with the two methods of measurement, which are the methods traditionally used for chronic wounds.
Patients and Methods
Study design and study population
The ESTABLISH–1 study was a phase 3, randomized, double-blind study of the comparative efficacy and safety of 6-d oral tedizolid phosphate and 10-d oral linezolid for the treatment of ABSSSI (ClinicalTrials.gov Identifier: NCT01170221). The study population included subjects with suspected or documented gram-positive cellulitis/erysipelas, major cutaneous abscesses, or wound infections as defined by the FDA guidance statement for developing drugs for the treatment of ABSSSI [3]. An ethics committee, institutional review board (IRB), or research ethics board approved the study at each of the 81 study sites. All subjects provided their signed consent to participate and all clinical investigations were conducted according to the principles of the Declaration of Helsinki.
Ruler technique
Investigators at each of 81 ESTABLISH–1 clinical trial sites outlined the skin margins of erythema caused by severe abscesses, cellulitis, and infected wounds with a surgical marker. Using the RT method, they then measured manually the longest head-to-toe length and greatest width perpendicular to that length of each area of erythema around each of the three types of lesions as measured with a disposable ruler (Fig. 1) and entered these measurements into an electronic case-report form. The lesion surface area (cm2) as calculated from these manual measurements was automatically calculated and entered on the form by an electronic case report system.
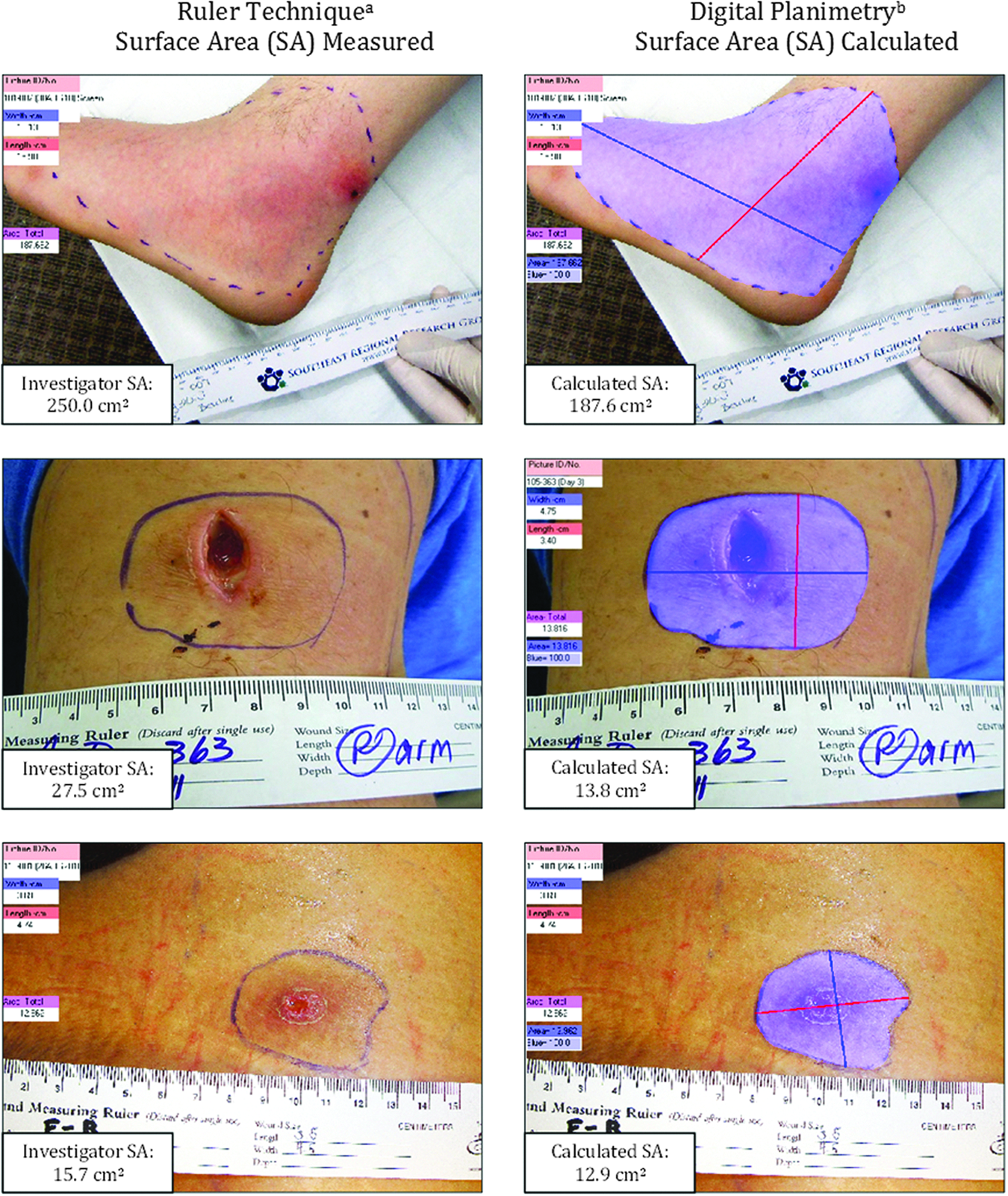
Determination of lesion sizes for ESTABLISH–1. Investigators were instructed to measure erythema surrounding a lesion in a head-to-toe orientation by measuring the greatest head-to-toe length of the lesion and then the greatest width perpendicular to that length. The shaded blue region is the area outlined with a pen with a digital graphics tablet while observing the image on a computer screen.
Digital planimetry
After outlining the edge of erythema around skin lesions with a surgical marker, investigators at the ESTABLISH–1 clinical trial sites took digital photographic images of the lesions with a digital camera. If a lesion was of a 3D nature (i.e., wrapping around the circumference of body parts, such as an arm, leg, or torso), site personnel were instructed to capture two to four images of the lesion at an angle perpendicular to the body surface for more accurate measurement. The digital images were then uploaded into the clinical trial database and organized and processed by on of the authors (P.B.) at Cubist Pharmaceuticals (San Diego, CA) with Photoshop CS5 image editing software (Adobe Systems, San Jose, CA). Images were enhanced with the Photoshop cropping, levels, curves, color correction, image rotation, and sharpening tools to facilitate analyses. PictZar-CDM version 5.9 software for skin lesion measurement was used to assess lesion size. This software calculates the area of a lesion by counting pixels after a photographic image of the lesion has been scaled with a ruler that is placed in the same plane as the lesion (Figure 1).
Results
Of the 667 subjects randomized to treatment with linezoid or tedizolid phosphate, 292 had lesion length and width manual measurements for RT and quality photos of lesions for DP at baseline, at the 48–72 h visit, and at the end-of-therapy visit. Approximately 30% of the subjects who presented with lesions at baseline required multiple images of their lesions, taken at various viewing angles, to adequately describe the 3D nature of their lesions. Abscess was the most common type of lesion (in 42% of the patients), followed by cellulitis (34%) and wound infections (23%).
Table 3 shows the percentage of lesions whose treatment produced various levels of categorical responses at the 48–72 h visit after the initiation of treatment and at the end of treatment (up to 11 d after its initiation). At baseline, the median surface area of lesions measured with DP (131 cm2) was approximately one-third smaller than that calculated with the RT method (195 cm2). The median baseline surface area of abscesses was slightly smaller than that of cellulitis and wound lesions with both the RT method and DP. The mean baseline surface area of each category of lesion was larger than the median value, indicating that the distribution of lesion sizes was skewed by a small number of large lesions.
Data are median or mean±SD values, or number or percent of subjects.
% of patients with decrease in lesion surface area from baseline to designated endpoint.
≥0% is equivalent to cessation of spread.
Difference=ruler technique value minus the digital planimetry value.
Cessation of the spread of lesions was evaluated at the 48–72 h visit. High rates of response were observed with both the RT method and DP across all three categories of lesions examined in the ESTABLISH–1 study, although the rates of response for abscesses and wound infections (≥95%) were greater than that for cellulitis (≥85%), suggesting that cellulitic lesions may decrease in size more slowly than the other two types of lesions. A greater percentage of patients achieved a ≥20% reduction in lesion size when evaluated by the RT method than the DP method for each type of lesion (abscess: 94.3% vs. 63.4%, cellulitis: 77.0% vs. 60.0%, wound: 91.0% vs. 64.2%, respectively). Similarly, the difference between the two measurement methods across all three categories of lesions was most prominent for subjects in whom a ≥20% reduction in lesion size was achieved at 48–72 h after the initiation of treatment (87.7% response rate with the RT method – 62.0% with DP=26% as the difference between the methods). To determine whether large lesion sizes at baseline influenced the response rate at 48–72 h after the initiation of treatment, the analysis was repeated after exclusion of the data for 87 patients who required multiple photographic views of their lesions at baseline. The percentages of patients requiring only a single baseline photograph and of those in whom a ≥20% decrease from their baseline lesion size was seen at 48–72 h after the initiation of treatment were nearly identical for both the RT method (87.7% vs. 86.3%) and DP (62.0% vs. 61.5%).
The response rates of patients with lesions measured with the RT method and DP were fairly comparable, at 88.0% and 81.8%, respectively, for subjects who presented with a reduction of ≥90% in lesion size at the end-of-treatment visit. At least a 75% reduction in the size of lesions of any type as measured with both the RT method and DP was also achieved in most subjects at the end-of-treatment visit. Differences between the two measurement methods were smaller (<6.2%) for lesions that were essentially unchanged (cessation of spread) or had largely regressed at the end-of-treatment visit (Figure 2).
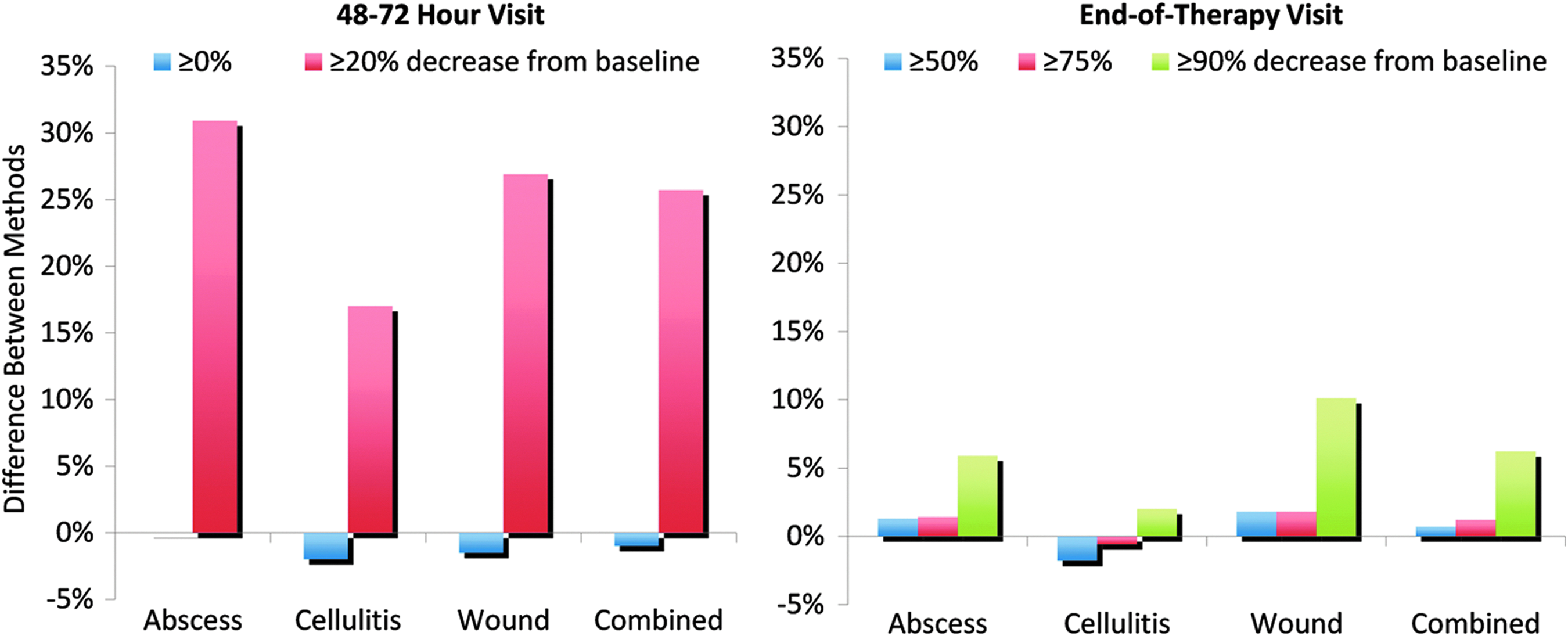
Differences in measurements of four types of skin lesions with a ruler technique (RT) and digital planimetry (DP) at a patient visit made at 48–72 h after the initiation of treatment of the lesions and at an end-of-treatment visit at up to 11 d after the end of treatment.
Discussion
Accurate and consistent measurement of the size of skin lesions is an important aspect of the overall treatment of acute bacterial infections of the skin, because some interventions or referrals to specialists may depend on the perceived size of a lesion. In terms of clinical trial-based research on ABSSSI, the FDA has an interest in understanding the advantages and limitations of various measurement methods, having recently enacted a size-based primary outcome measure for the efficacy of treatment of ABSSSI.
The results of the ESTABLISH–1 study indicate that both DP and the RT method of measurement of the sizes of skin lesions are appropriate for assessing clinical response to treatment as defined by the cessation of lesion spread or a reduction in lesion size by the FDA. Median lesion surface area as calculated with DP was one third smaller than with the RT method, most likely because of the overestimation of area inherent in the RT method. Both methods showed a similar response to treatment in terms of the cessation of spread of lesions observed at 48–72 h after the initiation of treatment (93.2% of subjects with use of the RT method and 94.2% of subjects with DP). Less agreement of the two methods was observed when assessing a ≥20% reduction in lesion size as defined by the FNIH. This level of response was achieved in 87.7% of the study subjects at the 48–72 h visit with the RT method vs. only 62.0% of the subjects with DP (Table 3). Thus, approximately 25% fewer subjects whose lesions were assessed with DP than with the RT method would have been categorized as treatment successes according to the proposed FNIH definition. The FNIH specifies that the RT method be used when assessing the outcome of treatment of ABSSSI [4]; however, our results suggest that if a different method such as DP is used to quantify treatment success, then a different threshold may be needed to yield comparable response rates.
Although DP appears to be a more refined method for measuring skin-lesion size than the RT method, approximately 30% of the photographs made in the ESTABLISH–1 study were of insufficient quality for analysis, often because of failure to place the ruler used for measurement in the same plane as a lesion, refusal by the patient to be photographed, or omission of the ruler or wound tracing from the photograph. In no case was there an opportunity to replace unusable photographs with usable ones (unless site personnel assessed the photographs at the time they were made), and DP data for that time point was therefore lost. These deviations from protocol illustrate an inherent problem with digital methods of measurement when numerous clinical research sites are involved in a single study, as compared with a study conducted at a single clinic with experienced personnel. Despite the great reduction in inter-rater variability in the analysis of lesion-size data that occurs with central image processing [11], DP requires substantial training and monitoring to ensure the gathering of high-quality data. On the other hand, the RT method, because of its simplicity of use, almost always yielded a result sufficient for analysis in every instance of its use in ESTABLISH–1. The results of the ESTABLISH–1 study show that both methods are consistent and reliable for measuring the sizes of ABSSSI lesions.
Although a number of techniques for the measurement of skin-lesion size could be used in the course of a clinical trial, the most effective ones would be those that are simple and practical to implement across broad geographic and diverse clinical settings, and which allow consistent and accurate estimations of lesion size. In the absence of a gold standard for measurement of the sizes of skin lesions caused by acute infection, it is difficult to conclude which of two methods investigated in a comparative clinical study is superior to the other. Ultimately, changes in lesion size, rather than the absolute values of the sizes of lesions, will drive the assessment of outcomes of clinical research in treating ABSSSI. Hence, measurement error may not invalidate any particular method as long as the degree of error is consistent among measurements. In the context of clinical research for acute skin infections, the RT method offers advantages in practicality, feasibility, and cost. Additional research is required to assess various lesion-measurement techniques for use in clinical trials of treatments for ABSSSI.
Footnotes
Acknowledgments
Cubist Pharmaceuticals thanks Brenda M. Clapper, of BioMedCom, Inc. (Santee, CA), and Michelle M. Merrigan, of Merrigan Medical Communications (San Diego, CA), for providing support in the medical writing of this report, and Dr. Martin Wendelken of PictZar for providing training services for the planimetry software used in the ESTABLISH–1 study.
Author Disclosure Statement
PB, CDA, and PP are employees of Cubist Pharmaceuticals, San Diego, CA.