
Abstract
Abstract
Background:
The administration of appropriate antibiotics in a timely fashion with discontinuation post-operatively is the first of the Surgical Care Improvement Project (SCIP) initiatives and was expected to reduce post-operative infections significantly. This study aimed at determining whether SCIP has had an effect on surgical site infections (SSIs).
Methods:
A retrospective cohort study was conducted to evaluate the infection rates of adult patients (age≥18 years) having elective cholecystectomies, laparoscopic cholecystectomies, and colectomies from 2001–2006 using the Nationwide Inpatient Sample (NIS) database. The population consisted of all patients older than 18 years who had colon resection or cholecystectomy and were discharged from a hospital included in the NIS. Annual infection rates were determined for each of the operations.
Results:
Post-operative infections rose steadily and significantly (p<0.0001) in colon surgery from 2001 to 2006. A significant increase in SSIs also was seen in open (p=0.0001) and laparoscopic (p<0.0001) cholecystectomy from 2001 to 2006. Length of stay was significantly longer in infected than in non-infected patients.
Conclusion:
The factors that contributed to the observed increase in the infection rate should be identified to improve the SCIP initiatives.
The goal of our project was to evaluate SCIP in the years before its national mandate and at its beginning. Whereas SCIP included requirements for prophylactic antibiotic use in hysterectomy and open heart, colon, prosthetic joint, and vascular surgery, our study included patients who were undergoing surgery where a SCIP directive for prophylactic antibiotics existed (elective colectomy) along with patients in whom antibiotics were not required routinely (cholecystectomy). This study was undertaken to evaluate the rate of surgical site infections (SSIs) with anticipation of some evidence of improvement, especially as CMS expects a 25% reduction in the infection rate by the end of 2010.
Materials and Methods
Data source
This retrospective cohort study examined the annual SSI rates using discharge data from the Nationwide Inpatient Sample (NIS), Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality [4]. The NIS is the largest all-payer inpatient care database in the United States and contains about a 20% stratified sample of U.S. community hospitals. The stratification is based on five hospital characteristics: Geographic region (Northeast, Midwest, West, and South), control (government non-federal [public], private not-for-profit [voluntary], and private investor-owned [proprietary]), location (urban or rural), teaching status (teaching or non-teaching), and bed size (small, medium, and large). It contains data from about eight million hospital stays each year.
Diseases and procedures of interest
Adult patients (age≥18 years) who underwent elective cholecystectomy or elective colectomy from 2001 through 2006 were the population of interest. The disease status and procedures were categorized according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
Groups with ICD-9-CM codes
The elective colon surgery group was comprised of patients with a primary diagnosis of diverticulosis of the colon without hemorrhage (ICD-9-CM codes: 562.11and 562.12) or malignant neoplasm of the colon (ICD-9-CM codes: 153.x, where x represents the possible digits within this ICD-9-CM code category), with procedures of partial excision of the large intestine (ICD-9-CM codes: 45.7x) or total intra-abdominal colectomy (ICD-9-CM code: 45.8) or intestinal anastomosis (ICD-9-CM codes: 45.9x).
The elective cholecystectomy group was comprised of patients with cholelithiasis (ICD-9-CM codes: 574.xx) or other disorders of the gallbladder (ICD-9-CM codes: 575.xx). The open cholecystectomy group was comprised of patients undergoing cholecystectomy (ICD-9-CM codes: 51.21 or 51.22). The laparoscopic cholecystectomy group was comprised of patients with procedures of laparoscopic cholecystectomy (ICD-9-CM codes: 51.23 or 51.24).
Age is a known risk factor for post-operative infection. Therefore, for comparison purposes, we classified patients further into two groups: age≥65 years vs. age<65 years.
Outcome variables
The primary measured outcome for this study was SSIs as defined by a patient who had a record of cellulitis or abscess of the trunk (ICD-9-CM code: 682.2), peritoneal abscess (ICD-9-CM code: 567.22), infected post-operative seroma (ICD-9-CM code: 998.51), or other post-operative infection (ICD-9-CM code: 998.59). In-hospital death and hospital length of stay were also outcomes of interest. Hospital length of stay was based on the reported days. The cohorts were classified by discharge year.
Statistical methods
The annual infection and mortality rates were calculated for each study group. The weighted number of procedures and rates were calculated to take into consideration the stratified sampling design of NIS data. The chi-square test was used to compare the rates between two groups. The trends of rates were assessed using the Cochran-Armitage trend test. The median lengths of hospital stay were calculated using the Kaplan-Meier product limit estimator. The analyses were conducted using the R language with packages of “survey” and “survival” [5–8].
Results
Infection rates—colectomy
The infection rate for elective colon resection (Fig. 1) increased from 2001 through 2006 in patients 65 years or older (n=245,974; 2.37%, 2.42%, 2.69%, 2.91%, 3.04%, 3.95%) and under the age of 65 (n=196,852; 3.03%, 3.01%, 3.13%, 3.10%, 3.49%, 4.62%). These increases in the infection rate were statistically significant (p<0.0001). The infection rate was higher in younger patients in all the years studied. There was a significantly higher incidence of diverticulitis in the patients<65 years than in the group of patients≥65 years (51.8% vs. 18.4%; p<0.0001; chi-square test).
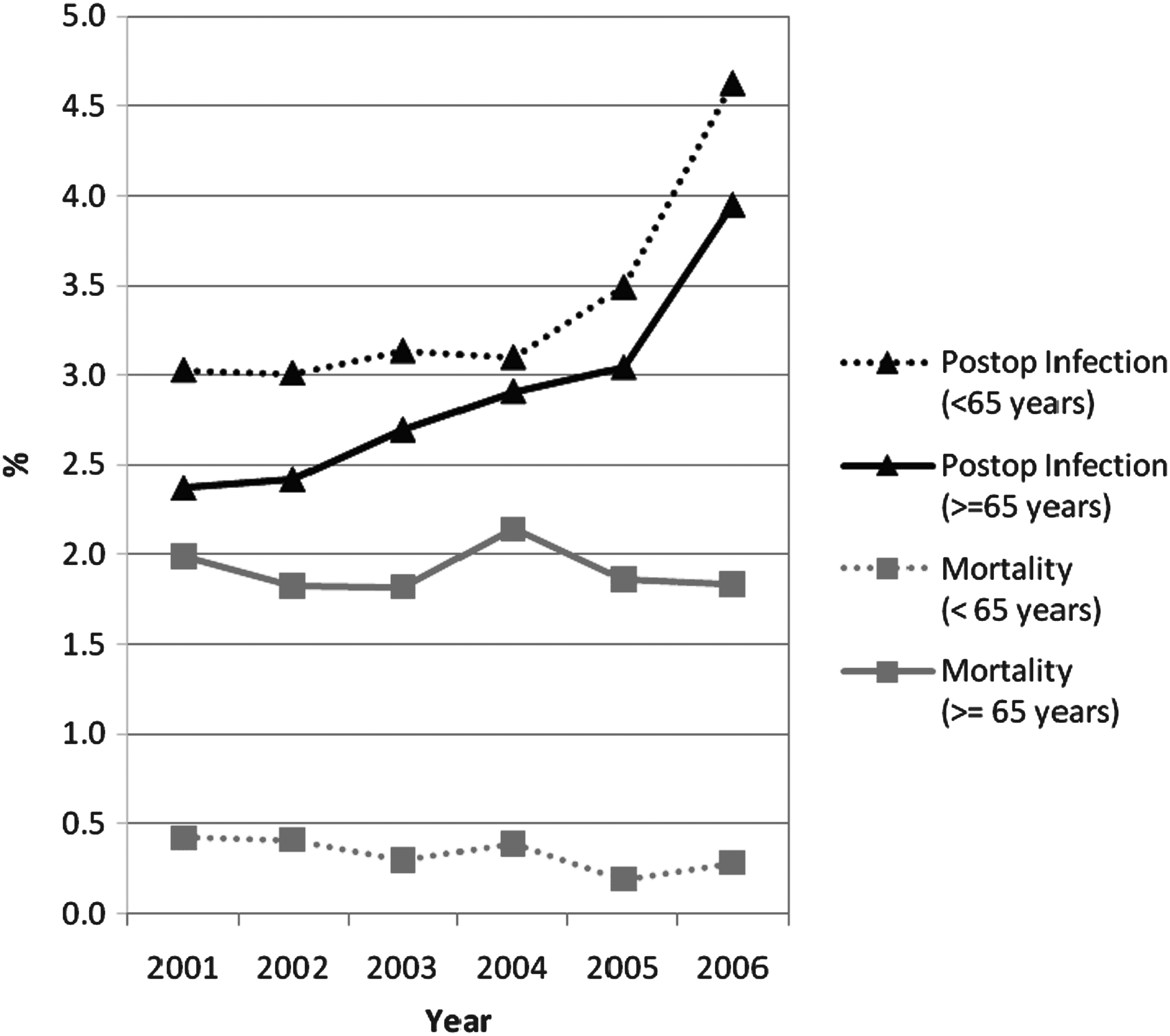
Weighted infection and mortality rates for colon surgery for patients≥65 years and those<65 years for the six study years.
Infection rates—cholecystectomy
The infection rate for open cholecystectomy (Fig. 2) increased significantly, from 0.91% in 2001 to 1.80% in 2006 for those<65 years (p<0.0001) and from 1.44% in 2001 to 2.15% in 2006 for those≥65 years (p=0.0001). The infection rates for laparoscopic cholecystectomy (Fig, 3) also increased, from 0.25% and 0.36% in 2001 to 0.47% and 0.70% in 2006 in those under 65 years and those≥65 years, respectively. These increases were statistically significant for both age groups (p<0.0001).
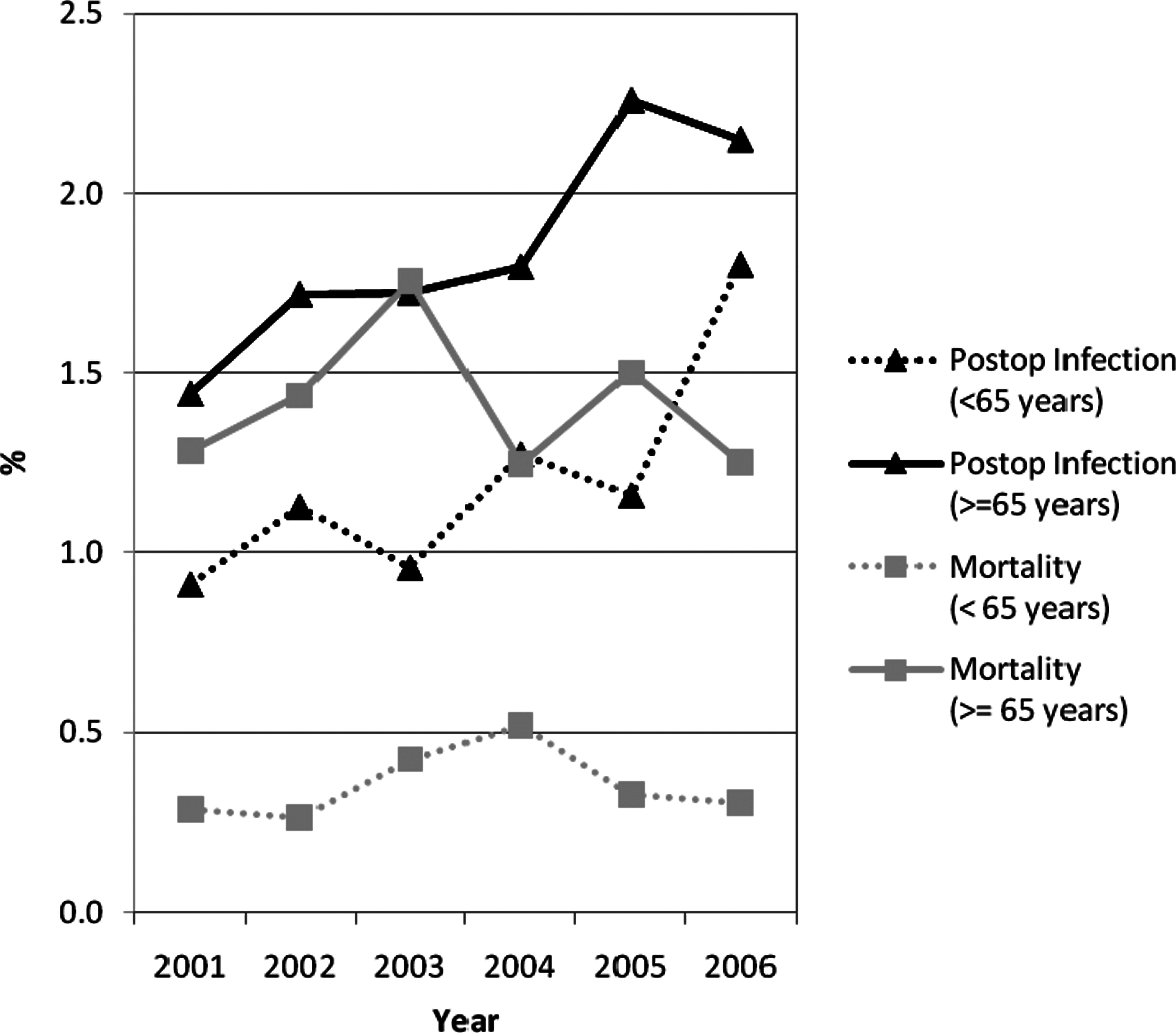
Weighted infection and mortality rates for open cholecystectomy for patients≥65 years and those<65 years for the six study years.
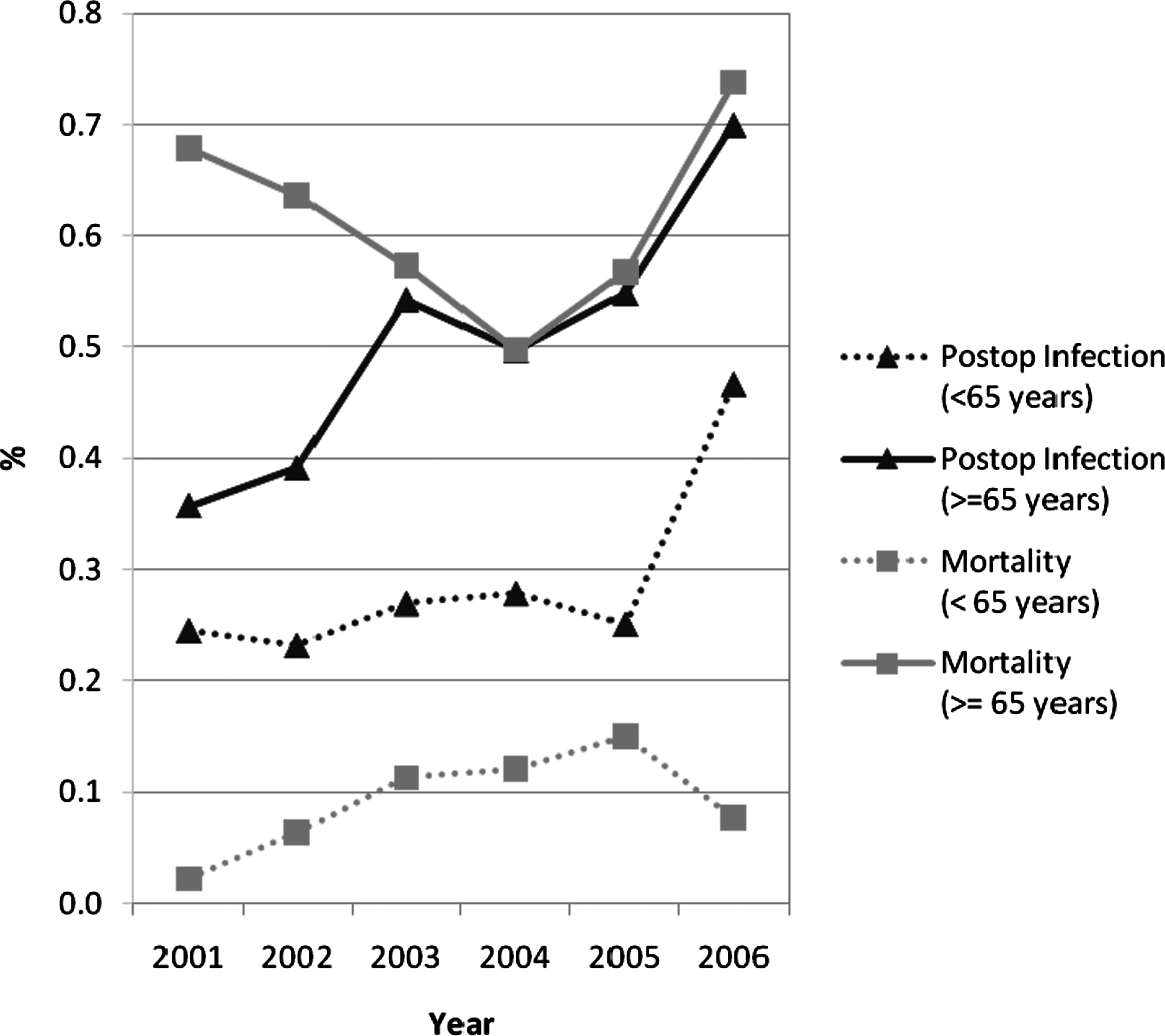
Weighted infection and mortality rates for laparoscopic cholecystectomy for patients≥65 years and those<65 years for the six study years.
Mortality rates
The mortality rates for colon surgery did not follow any significant trend for study duration in patients 65 years or older (see Fig. 1). In younger patients, there was a significant decrease in the mortality rate, from 0.42% in 2001 to 0.28% in 2006 (p<0.0001).
The mortality rates for both age groups for open cholecystectomy did not show any significant trend over the six-year study period (p=0.84,≥65 years and p=0.26,<65 years). The mortality rates for patients≥65 years undergoing laparoscopic cholecystectomy likewise did not show any significant trend over the study period (p=0.77). However, in patients<65 years of age, the mortality rate increased significantly over the study (from 0.022% in 2001 to 0.077% in 2006; p<0.0001).
Length of stay
Over the six- year period, there was a decline in the length of stay for elective colon surgery and open cholecystectomies in both age groups. The length of stay for laparoscopic cholecystectomies did not change for patients≥65 years and increased in patients<65 years old (Fig. 4). The length of stay of the infected compared with non-infected patients increased significantly for each of the categories (Fig. 5).
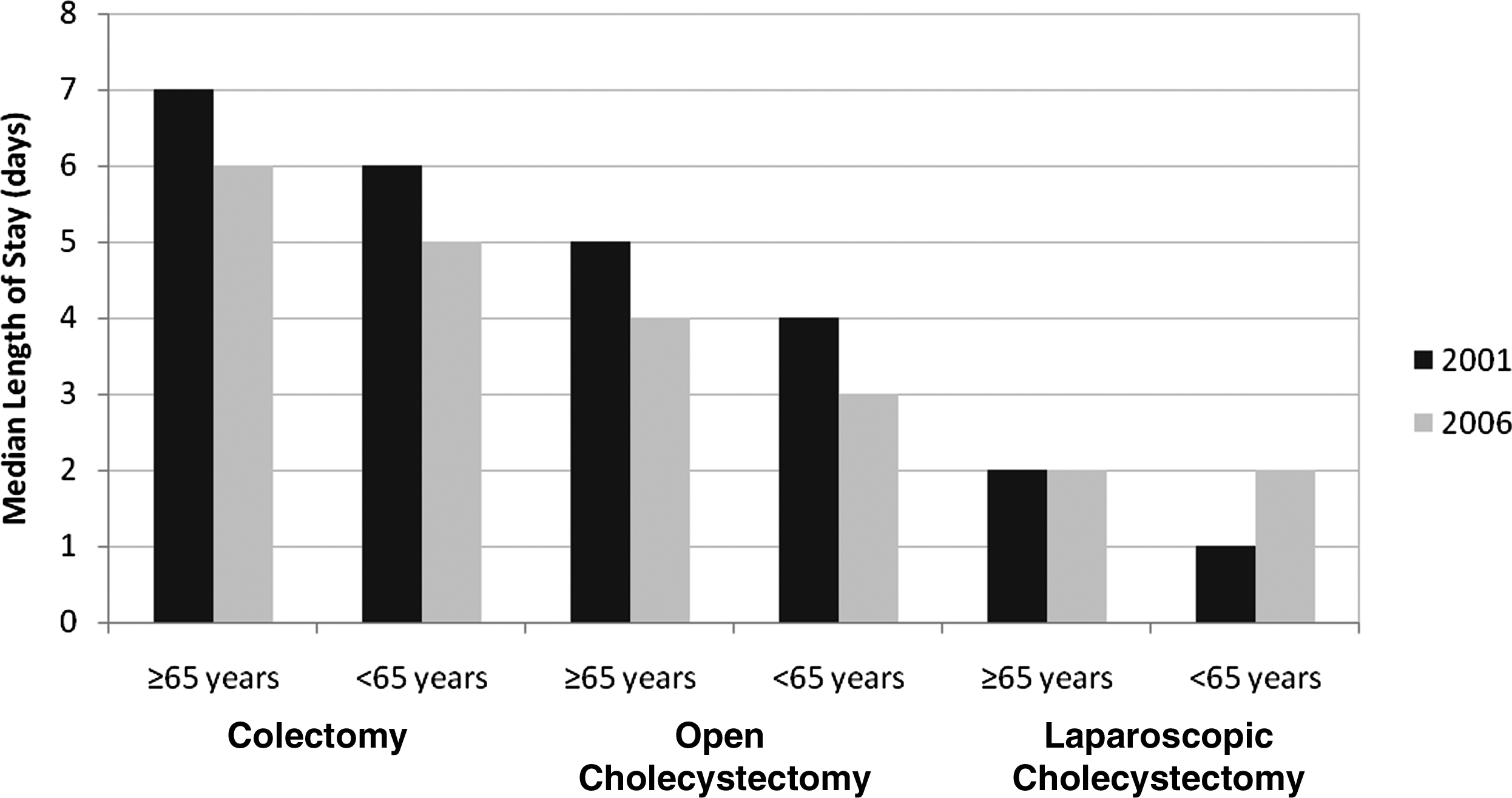
Length of stay (days) according to type of operation and patient age.
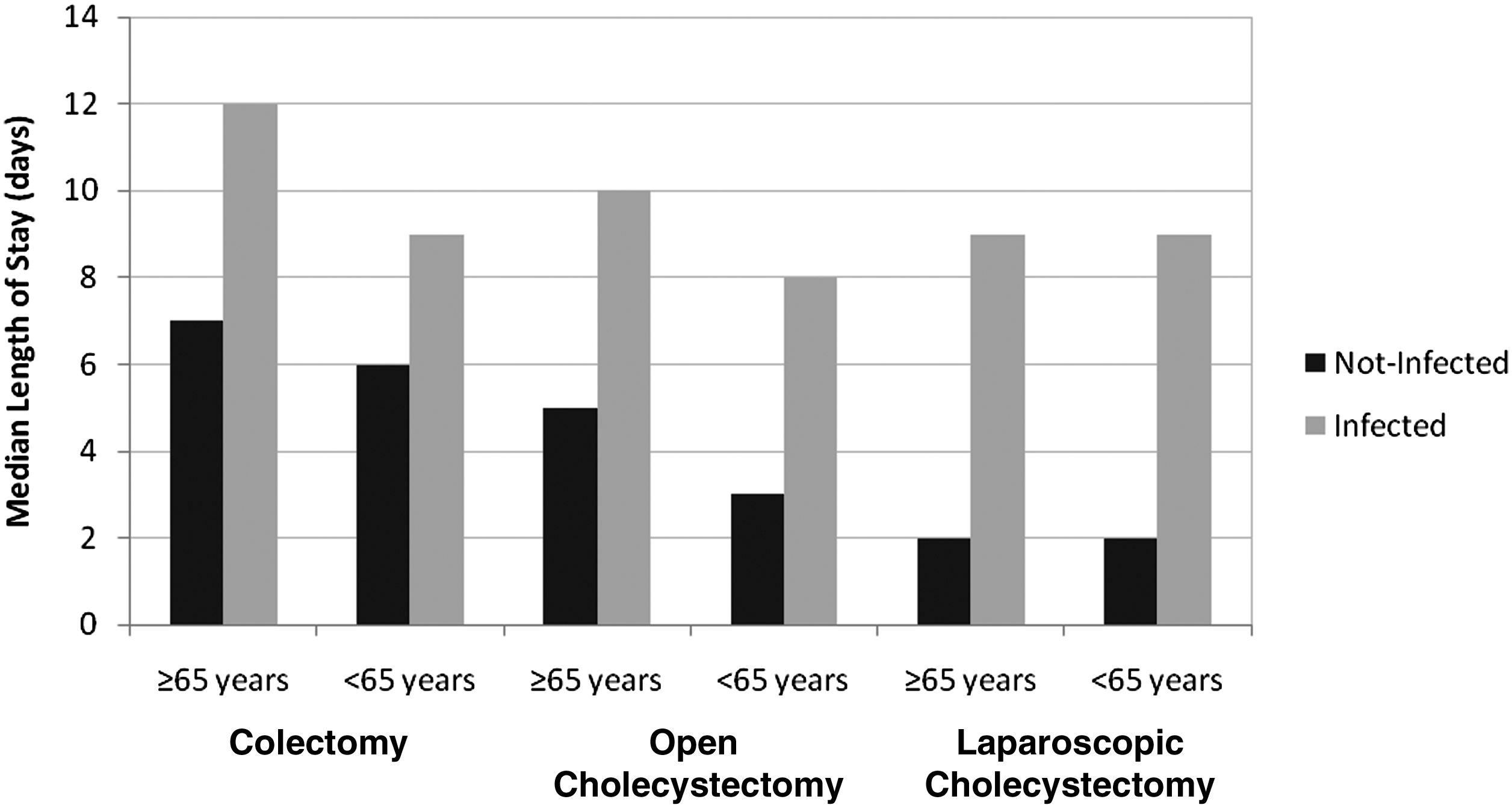
Length of stay (days) of infected vs. non-infected patients according to type of operation.
Discussion
The rate of post-operative sepsis has increased over the past two decades. Our study extends this observation to include patients who require prophylactic antibiotics. Post-operative sepsis rates have increased over the 17-year span from 1990 to 2006 in both elective and non-elective operative procedures [9]. Over the ten-year time interval from 1997 to 2006, severe post-operative sepsis increased in patients undergoing a wide spectrum of elective operations [10]. This increase in the rate of SSI also has been seen in a time interval of 24 mos (July 2006–June 2008) [3]. All of these studies used large databases to identify this increase.
The SSI rate in our study and that reported by Bateman et al. [8] is low compared with that in recent prospective studies [11–13]. These differences result from inherent problems with data collection, short post-operative stays, and inability to follow patients after discharge and on readmission. Because of the nature of de-identified data in NIS, it is impossible to track those infections after discharge. The NIS data is based on ICD-9-CM codes identified by clerical staff after hospital discharge, which is not as sensitive as the direct reporting by a healthcare professional during a randomized trial. The National Surgical Quality Improvement Program (NSQIP) data are collected by a specially trained nurse [14]. Because>50% of surgical site infections may present after day 10 or 11, a large percentage of the study population would be discharged prior to manifesting infection [15]. It is therefore likely that the NIS data reflect an under-reporting of infectious events. In spite of these differences, the NSQIP data from the paper of Berenguer et al. [3] cited a national increase, over a two-year interval from July 2006 through June 2008, from 9.7% to 10.5%. This documented increase both validates and extends our observations.
We used the NIS database because it is the largest available. However, there are several disadvantages to using such an administrative database: it does not include outpatients; it does not identify individual patients; it provides only limited details about patient demographics and treatments; and it uses data supplied by many institutions with variations in protocols and standards. However, an increase in the rate of surgical infections has been documented by evaluating administrative databases other than NIS. Therefore, these disadvantages did not impact the important and similar observations.
A small but statistically significant rise in the mortality rate was seen in patients<65 years having laparoscopic cholecystectomy. During the six-year study period, there was a reduction in the denominator, whereas the number of deaths remained stable for this group. A possible explanation is infection related, as the increase was temporally related to a rise in the infection rate. Another possibility is that over this period, larger numbers of better-risk patients were having their surgery as ambulatory patients, resulting in poorer-risk patients appearing in the NIS database. Because the actual number of deaths was small, resulting in very low mortality rates, it may not be possible to identify any specific reason for the trend.
Except for the laparoscopic cholecystectomy patients described above, the data did not show an increase in the mortality rate concomitantly with the rising infection rate. This likely manifested for several reasons. The first is that these were all elective patients who had the luxury of assessment prior to surgery and should be good risk. The second reason is that the codes used for these patients were for simple post-operative infections, not severe sepsis or other serious infectious complications. One would not expect a substantial mortality rate for a post-operative infection.
There are a number of possible explanations for the observed increase in SSI. Over the past two decades, there has been growing resistance of gram-negative bacilli to our therapeutic agents [16,17]. This clinical problem is amplified by the lack of new antibiotics to treat infections caused by these bacteria. Over this same period of time, the incidence of methicillin-resistant Staphylococcus aureus (MRSA) has increased to the point that community-acquired MRSA has doubled in emergency rooms in the pediatric population [18,19]. Clostridium difficile infections and vancomycin-resistant Enterococcus infections have increased as well [20,21]. Of additional concern is the emergence of aggressive gram-negative organisms resistant to all available antibiotics [22,23]. It is possible that with the emphasis on administrating prophylactic antibiotics, the SCIP program has resulted in promiscuous use of antibiotics where they are not indicated and thereby contributed to an increase in antibiotic resistance. Although it is possible that this rise in resistance played a role in the increase in the infection rate documented in this and other studies [3,9,10], there is no direct evidence to support this hypothesis. Our study was not designed to explore the numerous risk factors associated with the infections. Additional studies evaluating risk-adjusted outcomes will be conducted to evaluate the potential risk factors further.
Surgical site infections are a costly and morbid consequence believed to be highly preventable with appropriate use of peri-operative antibiotics [24]. In a review of patients undergoing surgery in 2001, it was determined that nearly 60% of the patients did not receive timely antibiotics. Also, inappropriate and prolonged therapy was found in more than 50% of patients [25]. This suggested a great potential for improvement in the management of peri-operative antibiotics and held the promise for greatly improved outcomes once a system was established for the appropriate use of antibiotics. The CMS initiated a nationwide program by state offices requiring mandatory reporting of appropriate antibiotics by 2006. During the period from 2002 to 2006, hospitals devoted great time and effort to developing systems that would ensure that the guidelines were met, that antibiotics were used more appropriately, and, as a consequence, that the infection rate would decline. By 2006, the Joint Commission on the Accreditation of Healthcare Organizations required compliance with the program, and CMS had instituted fines for hospitals not reporting their compliance with the program [26]. Nevertheless, the data presented in this study indicate that the infection rate increased.
The objective of SCIP is to reduce SSIs. It is probable that, given the current clinical environment of ever-increasing drug resistance, even in spite of our best efforts, this may not happen. The presence of disease impacting the post-operative infection rate has been documented [27], suggesting that there are many factors that may influence the post-operative infection rate negatively. The most serious concern is whether the SCIP program has in any way played into this problem and whether it should be abandoned or modified [28]. This study was not designed to provide an answer to this question. However, the data indicate that the effect of reducing the infection rate in elective surgical procedures has not been realized since the initiation of the SCIP directives. Although SCIP is not intended to allow indiscriminate use of antibiotics, the implementation of the guidelines may incentivize the unsophisticated practitioner to use antibiotics when they are not indicated. Appropriate use and timely discontinuation need to be reinforced continually in the SCIP guidelines.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.