
Abstract
We assessed the hematopoietic stem and progenitor cell (HSPC) population in the cord blood of neonates born to mothers with gestational diabetes mellitus (GDM) in a hypothesis generating pilot study, due to that, neonatal polycythemia may be the consequence of GDM pregnancy. Forty-five pregnant women with GDM (last trimester mean HbA1C = 33.9 mmol/mol) and 42 (nondiabetic) control pregnant women were enrolled after their routine 75 g oral glucose tolerance test (OGTT) between the 24th and 28th gestational week (with expected differences in their mean routine clinical characteristics: plasma glucose at OGTT: 0′ = 5.07 vs. 4.62 mM, 120′ = 8.9 vs. 5.76 mM, age = 35.07 vs. 31.66 years, prepregnancy body mass index = 27.9 vs. 23.9 kg/m2, GDM vs. control, respectively) on a voluntary basis after signing the informed consent. EDTA-treated cord blood samples were analyzed by flow cytometry and the software Kaluza1.2 using CD45 and CD34-specific fluorescent antibodies to identify the HSPC population (CD34+ cells within the CD45dim blast gate). The proportion of CD34+CD45dim HSPCs among the nucleated cells was significantly (P < 0.05, statistical power = 60.8%) higher in the cord blood samples of neonates born to mothers with GDM (median 0.38%) compared to neonates born to nondiabetic mothers (median 0.32%) and according to treatment types (P < 0.05) median: control 0.32%, GDM-diet only 0.37%, GDM-on insulin 0.45%; control versus GDM on insulin (P < 0.05). The increased proportion of circulating CD34+CD45dim cells in the cord blood may possibly be related to altered fetal stem cell mobilization in GDM pregnancy, yet these results should be interpreted only as preliminary due to the small sample sizes.
Introduction
D
Even in infants born to women with only diet-controlled GDM, neonatal hematocrit values above 60% are occurring at a higher than 10% rate [1], and the prevalence of neonatal polycythemia in insulin-requiring GDM and type 1 diabetic pregnancies may even exceed the 30% and 40%, respectively [2,3]. The pathophysiology of this neonatal complication of maternal diabetes has been studied focusing on later stages of hematopoiesis. Authors suggested decades ago that the increased human umbilical plasma erythropoietin (Epo) levels were secondary due to fetal hyperinsulinemia [4]; however, no data were available about the cord hematopoietic stem cell (HSC) population in GDM before our study.
In addition, the DPP-4-CXCL12 axis has been recently identified as an important regulator of HSC mobilization in the adult human bone marrow in response to ischemic stimuli [5,6]. We recently reported that the serum DPP-4 enzymatic activity was decreased in the cord blood of neonates born to mothers with GDM [7], and therefore, it could be hypothesized that the cord HSC/HSPC population may be altered in GDM.
Materials and Methods
Research design
This study has been conducted in a single Hungarian center in the framework of the New Horizons Initiative of the EFSD after receiving approval from the appropriate ethical bodies. Altogether, 90 pregnant women signed the informed consent following the 75 g oral glucose tolerance test (OGTT) from the 24th to 28th gestational week: cord blood sampling at delivery with HSPC population assessment was possible from umbilical cord blood samples of neonates born to mothers with GDM (n = 45) and nondiabetic controls (n = 42), and three individuals were not included in the final analysis due to damaged samples.
Patients and cord blood collection
Altogether, 45 pregnant women with GDM as well as 42 control pregnant women were enrolled immediately after their routine OGTT between the 24th and 28th gestational week on a voluntary basis after signing the informed consent. We designated a control group as individuals who carry a pregnancy and were neither diagnosed with GDM nor with overt diabetes between the 24th and 28th gestational week at OGTT or later throughout the course of their pregnancy. The diagnosis of GDM has been established according to the Hungarian national recommendations (modified 1999 WHO recommendation—GDM: 75 g OGTT at 24–28 gw: FPG ≥6.1 mM, 120′ PG ≥7.8 mM). Individuals diagnosed with overt diabetes (classified as diabetes in the pregnancy category in 2013, WHO recommendation, that is, FPG ≥7.0 mM, 120′ PG ≥11.1 mM) were excluded from the analysis. Cord blood samples were collected from the umbilical vein using the cord clamping technique as soon as it was possible after birth. The most important clinical maternal data were recorded (including the age at delivery, 75 g OGTT 0′ and 120′ min values between the 24th and 28th gestational week, prepregnancy body mass index (BMI), weight gain during pregnancy, and third trimester HbA1c value in the GDM group). The birth weight percentiles were assessed using a downloaded program on fetal weight equations as a published global reference for birth weight percentiles using 3,340 and 3,500 g as the Hungarian population mean birth weight values at 40 weeks for female and male neonates, respectively [8].
Flow cytometric analysis
EDTA-treated cord blood samples were analyzed by flow cytometry (Beckman Coulter Navios flow cytometer, Kaluza 1.2 software). Leukocytes were gated and differentiated from debris according to their forward and side scatter. BD Via-Probe (BD Biosciences, San Jose, CA) cell viability solution (7-AAD labeled) was used to differentiate living from dead cells. Cell surface CD45 (label: FITC, isotype: IgG1, κ, Clone: HI30) and CD34 (label: PE-Cy7, isotype: IgG1, κ, Clone: 581) were stained with specific fluorescent antibodies (BioLegend, San Diego, CA). Residual red blood cells (RBC) were filtered out from the leukocytes according to their absent CD45 expression.
Identification of stem and progenitor cell populations
We identified CD34+ cells within the gate of the nucleated cells. Circulating HSPCs were defined according to the International Society of Hematotherapy and Graft Engineering (ISHAGE) criteria as CD34+ HPCs within the CD45dim blast gate, indicating that they express CD45 at a lower intensity than matured leukocytes [9,10]. Our gating strategy is indicated on Fig. 1.
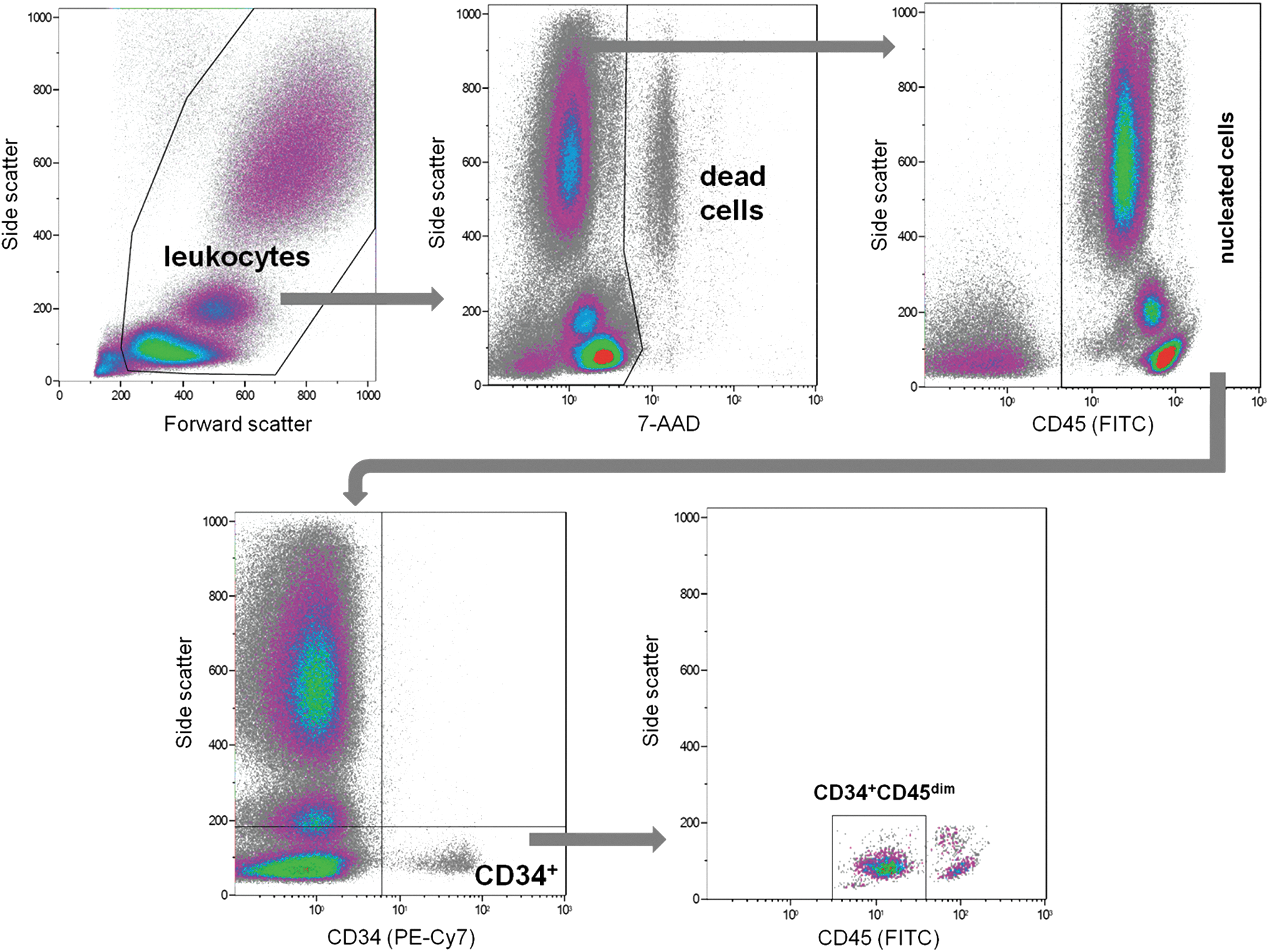
Leukocytes were separated from debris according to their forward and side scatter. Red blood cells were separated from nucleated cells according to their absent CD45 expression in the undead (nonpermeable for 7-AAD) cell population. The stem and precursor cells were gated within all nucleated cells according to their CD34 expression and their intermediate CD45 expression (CD45dim).
Statistical analysis
Statistica software (version 11; StatSoft, Tulsa, OK) was used for statistical analysis. Kolmogorov–Smirnov test was used to assess normality. As data distributions were non-normal, the Mann–Whitney U test (MWU) was used to compare the data of the healthy control and GDM study populations on the primary outcomes (proportions of hematopoietic stem and precursor cells). The Kruskal–Wallis ANOVA test was used to compare multiple samples. Student's t-test was used to compare means of clinical data (Table 1) due to the normal demographic data distributions in the GDM and control populations according to the Kolmogorov-Smirnov normality test. For paired comparisons, we also performed power analysis using the mean values, the sample size numbers, and the population sigma values.
BMI, body mass index; 95% CI, 95% confidence interval; GDM, gestational diabetes mellitus; OGTT, oral glucose tolerance test.
Results
Clinical data
Prepregnancy BMI and the age at delivery were significantly higher in the GDM group compared to the controls. The most important clinical data of the pregnant population are summarized in Table 1. Neonatal birth weight categories according to gestational age and the neonatal gender distributions in the study groups are indicated in Table 2.
AGA, appropriate for gestational age;
Proportions of hematopoietic stem and precursor cells
The proportion of CD34+CD45dim cells (HSPCs) among the nucleated cells was significantly (MWU P < 0.05, statistical power = 60.8%) higher in the cord blood samples of neonates born to mothers with GDM (median 0.38% [SD2 0.07]) compared to neonates born to nondiabetic mothers (0.32% [SD2 0.03]). Effect size ( = 0.497) calculation was also performed according to Cohen.
We found a significant difference (Kruskal–Wallis test P < 0.05) in the proportion of HSPCs among the nucleated cord blood cell population among different study groups according to the maternal GDM diagnosis and treatment types (control: median 0.32% [SD2 0.03], GDM requiring only diet 0.37% [SD2 0.07], and GDM on insulin therapy 0.45% [SD2 0.05]) (Fig. 2). The Newman–Keuls post hoc test also demonstrated a significant difference between the control and the GDM on insulin study groups (P < 0.05).
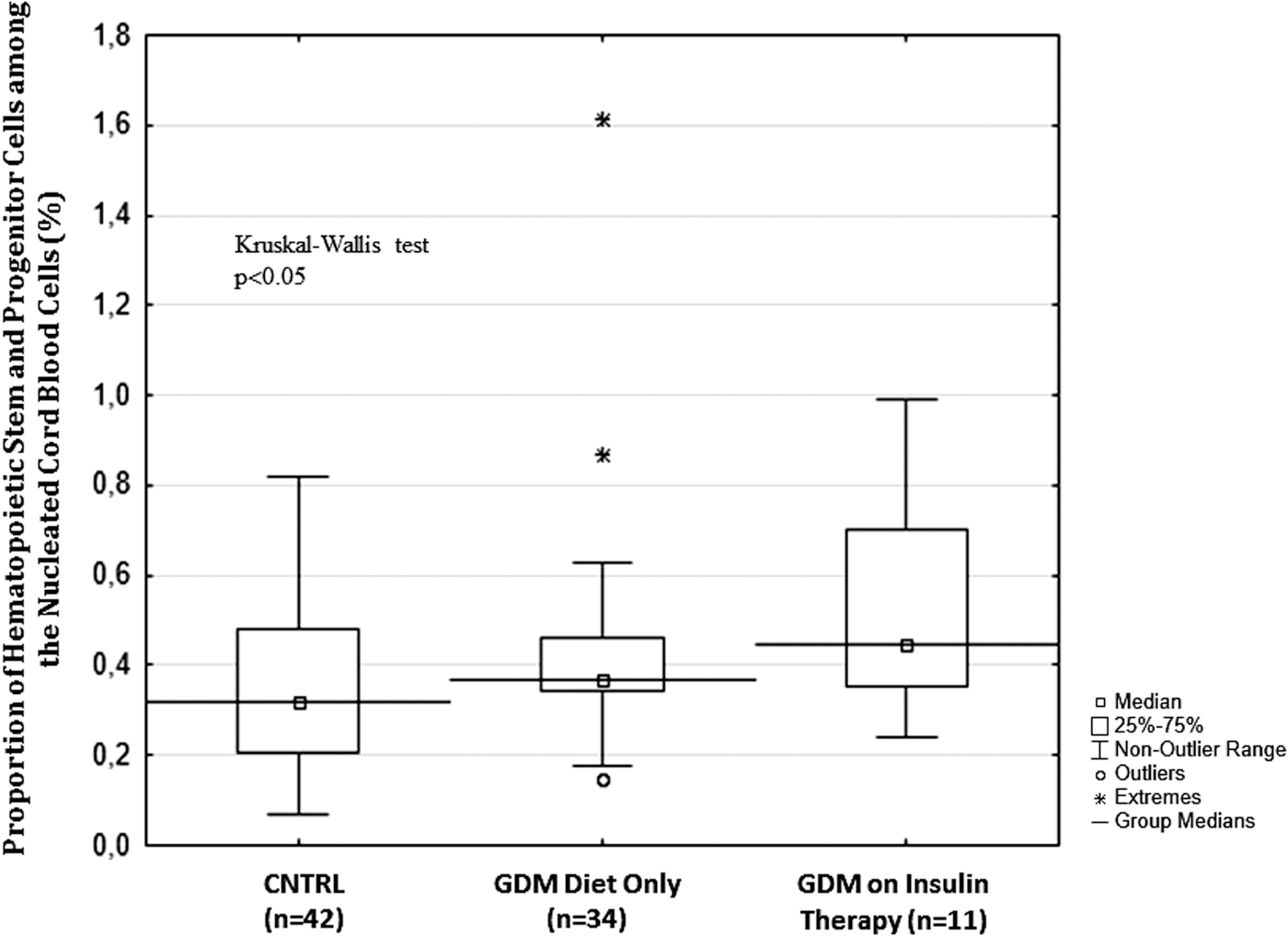
Box plot of the proportion of hematopoietic stem and progenitor cells among nucleated cord blood cells in different study groups according to maternal gestational diabetes mellitus (GDM) diagnosis and insulin therapy.
Although routine neonatal full blood count, hemoglobin level, and serum bilirubin measurements were not feasible in all participating neonates as per guidelines and due to technical difficulties, we detected only a borderline correlation between neonatal hemoglobin and bilirubin levels.
Discussion
This line of research was motived by major prior clinical findings: a long standing observation from the everyday clinical praxis proved that neonatal polycythemia is a feared complication of diabetic pregnancies occurring with a high enough prevalence to attract clinical attention (over 30% and 40% in insulin-requiring GDM or type 1 diabetic pregnancies, respectively). Polycythemia in the infants of diabetic mothers may be associated with serious clinical complications, including the hyperviscosity syndrome, thrombosis, respiratory distress with vascular congestion, heart failure, and cardiomegaly due to increased afterload and neurologic complications, such as stroke.
The ∼20%–25% increase in the proportion of circulating HSPCs (CD34+CD45dim) among all nucleated cells in the cord blood of neonates born to mothers with GDM compared to nondiabetic women may be related to the altered fetal stem cell mobilization in GDM pregnancy or possibly due to the insulin therapy.
Neonatal polycythemia was previously explained by the fetal hypoxia-induced increase in Epo production that was closely related to the control of maternal antepartum hyperglycemia (ie, maternal HbA1c levels during the last month of pregnancy in type 1 diabetic women) [11]. Although previously Epo was described to stimulate RBC production downstream in the path when precursor cells already lost their CD34 marker, it has been recently suggested that high systemic levels of Epo may reprogram HSPCs inducing an increased output toward an erythroid fate in vivo [12].
In a prior study, Azouna et al. found that the number of CD34+ cells was higher in the cord blood of neonates with higher birth weight (>3.5 kg) and born to older mothers [13].
This finding might be in concordance with our findings; due to that, both of the parameters they indentified are clinically associated with GDM, higher maternal age is a risk, and higher birth weight is a possible consequence of GDM. Therefore, our study might provide a plausible common clinical path for their findings (ie, development of GDM); despite that the proportion of neonates in the large for gestational age group was only numerically higher in the GDM group (statistically nonsignificant), the maternal age was significantly higher in the GDM study group.
In addition, a decreased cord serum DPP-4 activity of neonates born to women with GDM compared to the activity in samples of neonates born to nondiabetic women was recently reported [7]. This—theoretically—might implicate an altered cleavage of other chemokines, growth factors, including CXCL12, and may possibly result in an altered mobilization of HSPCs through binding to CXCR4 [14], as this receptor is also present on human CD34+ cells from the umbilical cord blood [15 –17]. Therefore, we may speculate that the DPP-4-CXCL12-CXCR4 axis could also be involved in linking the fetal intrauterine metabolic environment and the stem cell population distributions to certain neonatal complications of the GDM pregnancy, possibly including but not limited to the neonatal polycythemia.
Limitations
The results presented here could not gain the 80% statistical power with the limited number of enrolled individuals and the calculated effect size of 0.5, considered as a “medium” relative size also indicates that the sample sizes should be further expanded and the current results may therefore only be interpreted as preliminary [18]. This was a hypothesis generating pilot study; therefore, no prior sample size calculation was performed. Although our results are coherent with the current knowledge about the regulatory mechanisms involved in HSPC mobilization, due to the limited sample sizes and the distribution of data we may not entirely exclude the occurrence of significances by chance alone.
The reported data only include cord stem/progenitor cell proportions, and due to the unknown total cell counts, these results represent only one aspect of cell populations that is also characterized by absolute cell numbers. The assessment of more matured precursor forms (ie, the progenitor cell population) with additional markers (eg, when cells already lack CD133 positivity) is currently missing, yet the results are expected to be more pronounced in the view that those progenitor cells are closer to the matured RBC that are proven to be different in amount in the neonates born to mothers with GDM.
To assess stem cell mobilization in a dynamic manner, both the DPP-4 activity and also the CXCL12 levels should have been measured at tissue levels (eg, bone marrow, placenta, and in the cord blood) to provide evidence for the altered CXCL12 gradient between the bone marrow and the periphery. In our study, we could not present any data about the potential alteration of the CXCL12 gradient between the stem cell niche of the neonatal bone marrow and the periphery; therefore, the discussion in this regard is hypothetical.
Since in a prior report [13] higher CD34+ cell counts were found in the cord blood of neonates born to mothers with higher age, maternal age cannot be excluded as a confounding factor in this analysis.
Footnotes
Acknowledgment
This study has been funded by the European Foundation for the Study of Diabetes (EFSD) New Horizons Initiative.
Author Disclosure Statement
No competing financial interests exist.