
Abstract
Background:
As knowledge of mechanical insufflation-exsufflation (MI-E) expands, understanding factors influencing home use is essential to promote effective therapy. This study aimed to determine the prevalence of MI-E long-term users in Norway and describe clinicians’ self-reported experience and independence with MI-E, cough assessment practices, and MI-E initiation and follow-up in a country with over 20 years of experience.
Methods:
This cross-sectional study used 4 data sources (1) Norwegian Units for Medical Home-Care Equipment provided data on MI-E users, (2) Statistics Norway provided the overall count of the Norwegian population, (3) The Norwegian Patient Registry supplied population data on specialist health care service use, and (4) a survey of multidisciplinary clinicians collected self-reported data on clinicians MI-E confidence and practices.
Results:
In 2023, 1,131 individuals in Norway (16% under 18 years) used MI-E devices for long-term treatment, with a prevalence of 53.5 per 100,000 among specialist health care service users and 20.6 per 100,000 in the total population. Of 182 survey respondents, 163 reported MI-E experience, primarily physiotherapists (78%), followed by nurses (13%) and physicians (9%). Physiotherapists had the longest experience and highest confidence in independently initiating MI-E and assisting colleagues. Most clinicians (77%) used multiple methods to assess cough effectiveness, including qualitative assessment, cough peak flow, and swallowing evaluation. Follow-up practices varied widely 43% used patient journals, 5% digital registries, 10% paper records, 27% unspecified overview of MI-E users for follow-up purposes, and 15% had no systematic overview. Regular follow-ups were reported by 43%, whereas 19% followed up only on patient request, 30% were unaware of local routines, and 8% reported no follow-up routines.
Conclusions:
The MI-E prevalence highlights its role as a substantial therapy for individuals with rare disorders. Variability in follow-up practices underscores the need for standardized guidelines to improve consistency and quality in long-term MI-E care.
Introduction
Mechanical insufflation-exsufflation (MI-E) is considered an effective treatment for individuals with ineffective cough, reducing the risk of respiratory complications related to retained secretions. 1 –9 Although clinical guidelines support long-term MI-E use for individuals with weak cough, 1 –3,7,8 the prevalence of MI-E users varies. 10 Factors such as clinician knowledge, confidence, 11 and the organization of services 12 –16 may influence its utilization. Access to MI-E equipment and application of cough assessment guidelines are additional considerations in acute care settings. 17 Moreover, follow-up of long-term MI-E users has more recently been highlighted as a key factor influencing treatment adherence. 9,12 As knowledge about MI-E applications grows, understanding the factors that impact its long-term home use becomes crucial, including an understanding of clinicians’ confidence in assessments, initiation of treatment, and follow-up. These insights can further guide how we educate clinicians, refine practices, and ensure the continued implementation of MI-E therapy to maximize patient benefits.
In Norway, MI-E therapy has been available for over 20 years, with the introduction of Emerson’s Cough Assist 3200 (Respironics, Murrysville, Pennsylvania) in June 2001, making Norway one of the first European countries to adopt this technology. Since then, a variety of MI-E devices has become available, and since 2016, the selection of specific devices for home care in Norway has been governed by a national tender process. MI-E devices are distributed through nationwide designated health care units, which maintain registries of individuals using medical home-care equipment. These units oversee delivery and servicing, ensuring that the publicly funded MI-E devices are equally accessible to the users.
The establishment of the Norwegian Advisory Unit for long term mechanical ventilation and a national long term mechanical ventilation patient registry in 2002 marked a significant step in ensuring equal access to high-quality ventilatory support and MI-E treatment at home, regardless of geographical residency in Norway. The Advisory Unit included a nationwide, multidisciplinary team of pulmonologists, pediatricians, nurses, and physiotherapists specializing in respiratory care for individuals requiring long term mechanical ventilation. This encompassed both noninvasive and invasive ventilatory support, as well as adjunct therapies such as airway clearance, including cough assistance. Specially trained physiotherapists (with or without certification as a board-certified specialist in pulmonary physiotherapy) are usually responsible for airway clearance techniques. However, in smaller hospitals, specially trained nurses or medical doctors may also be responsible for mechanically assisted cough. The national guidelines for long term mechanical ventilation were published in 2012, providing advice on MI-E therapy application. 18 After the Advisory Unit was discontinued in 2022, the National Quality and Competence Network for long term mechanical ventilation (NN-LTMV) has continued to support long term mechanical ventilation expertise across disciplines. The overall aim of the work is to promote further equal access to high-quality services to improve longevity and well-being for long-term MI-E users.
QUICK LOOK
Current knowledge
Mechanical insufflation-exsufflation (MI-E) is an effective therapy for individuals with weak cough, reducing the risk of respiratory complications caused by retained secretions. Despite its established role, there are scarce data on MI-E prevalence and limited knowledge of clinician confidence and practices for long-term follow-up.
What this paper contributes to our knowledge
This study highlights the prevalence of MI-E users in Norway, both in the general population and in specialist health care service users. Clinicians, particularly physiotherapists, demonstrated high levels of confidence and independence in initiating MI-E and assessing cough effectiveness. However, substantial variability in follow-up routines and oversight systems was observed. The findings underscore the need for standardized follow-up recommendations to improve consistency, adherence, and the long-term effectiveness of MI-E therapy.
This study aimed to determine the prevalence of long-term MI-E use in Norway and explore clinicians’ experience, confidence, and approaches to MI-E initiation, cough assessment, and follow-up.
Methods
Overall study design, data sources, and outcome measures
This cross-sectional study utilized 4 data sources: All the Units for Medical Home-Care Equipment located nationwide at 18 hospitals in Norway reported anonymized data, including the number of MI-E devices provided for long-term use in children and adults. Multiple devices for one patient’s home were logged as a single entry. The data were obtained during August and September 2023. Statistics Norway (ssb.no) provided the overall count of the Norwegian population by health regions in 2023. The Norwegian Patient Registry provided anonymous data on the number of individuals in contact with the specialized health care service by health region in 2023.
19
Specialized health care includes somatic departments in public health care and private hospitals with a government agreement. A nationwide survey was conducted in which multidisciplinary clinicians working with long-term MI-E were invited to complete a digital, anonymous, purpose-developed questionnaire. The survey was originally conducted in Norwegian and translated into English using ChatGPT-4.0 to create the online supplement version (see Supplementary Data). The questionnaire was divided into 2 parts: Part 1 was mandatory, and respondents without experience in MI-E finalized and submitted their responses. Part 2 consisted of 28 questions regarding clinicians’ self-reported experience and independence with long-term MI-E, their awareness of local, national, and international guidelines, approaches to cough effectiveness assessment, and practical routines for the initiation and follow-up of MI-E therapy, using preset Likert categories (see online Supplementary Table S1). The questionnaire included a mix of single-choice questions, where respondents could select only one answer (e.g., profession or health region), and multiple-choice questions, allowing respondents to select more than one applicable answer. Physiotherapists experienced in MI-E therapy reviewed the questionnaire, and the questions were adjusted according to their feedback before release.
This national survey was open-accessible during the period March to May 2023 via a survey link via Microsoft Forms (Microsoft Office 365). E-mail invitations to participate were disseminated through the NN-LTMV Network (total n = 370), which includes interdisciplinary health care professionals working at local or regional hospitals nationwide and certain employees in municipal health care services working with patients requiring long term mechanical ventilation. Three reminders were sent by e-mail. The survey was also promoted on social media channels of the NN-LTMV Network and Cardiorespiratory Physiotherapy Association. For information on the number of e-mail recipients and social media followers, see flowchart in online Supplementary Figure S1. The exclusion criteria were responders stating “No experience with MI-E” in Part 1 of the questionnaire.
Statistical analysis
Data from the survey were stored and later processed in Excel (Microsoft 365) and in Stata/BE 18 (StataCorp, College Station, Texas, USA). Categorical data were summarized using numbers and percentages. The prevalence of long-term MI-E users was calculated based on 2 methods: first, by dividing the number of individuals equipped with an MI-E device by the overall population of Norway; and second, by using the number of individuals in contact with specialized health care services as the denominator.
Results
Prevalence of MI-E devices in long-term use
In total, 1,131 individuals had an MI-E device for home-care use in Norway, and the overall prevalence among the total population and specialist health care service users was 20.6 and 53.5 per 100,000, respectively. The distribution by health regions and age group; children 0 < 18 years/adults shown in Figure 1.

Distribution of MI-E devices for long-term use in Norway by health regions and age groups (children and adults). MI-E prevalence was calculated using the number of individuals equipped with an MI-E device as the numerator, and either the overall population or the number of individuals in contact with the specialized health care service as the denominator, respectively. MI-E, mechanical insufflation-exsufflation.
Self-reported knowledge of the guidelines, MI-E device access, experience, and independency
Overall, 182 individuals responded to the survey, where 19 stated no experience of MI-E and were excluded, resulting in 163 responders included for analyses (see online Supplementary Figure S1 for details).
The responders were physiotherapists (n = 127, 78%), nurses (n = 21, 13%), or physicians (n = 15, 9%) by profession, and most of the responders (n = 117, 72%) had more than 5 years of MI-E experience. Most responders were familiar with local (n = 120, 45%) and national (n = 102, 38%) MI-E guidelines 18 and felt the recommendations regarding when and how to start long-term MI-E therapy were clear. Only 28 (10%) were familiar with international guidelines. 1,3,8 The self-reported level of clinical independence with MI-E initiation varied, with 15% and 17% stating “no” or “limited” experience with independent initiation of MI-E treatment, respectively. Further, 15% and 23% stated “some” or “good” experience in MI-E and able to initiate treatment independently, respectively. Finally, 30% were confident to start independently and assist colleagues in MI-E initiation upon request (see Table 1 and Figure 2 for details).
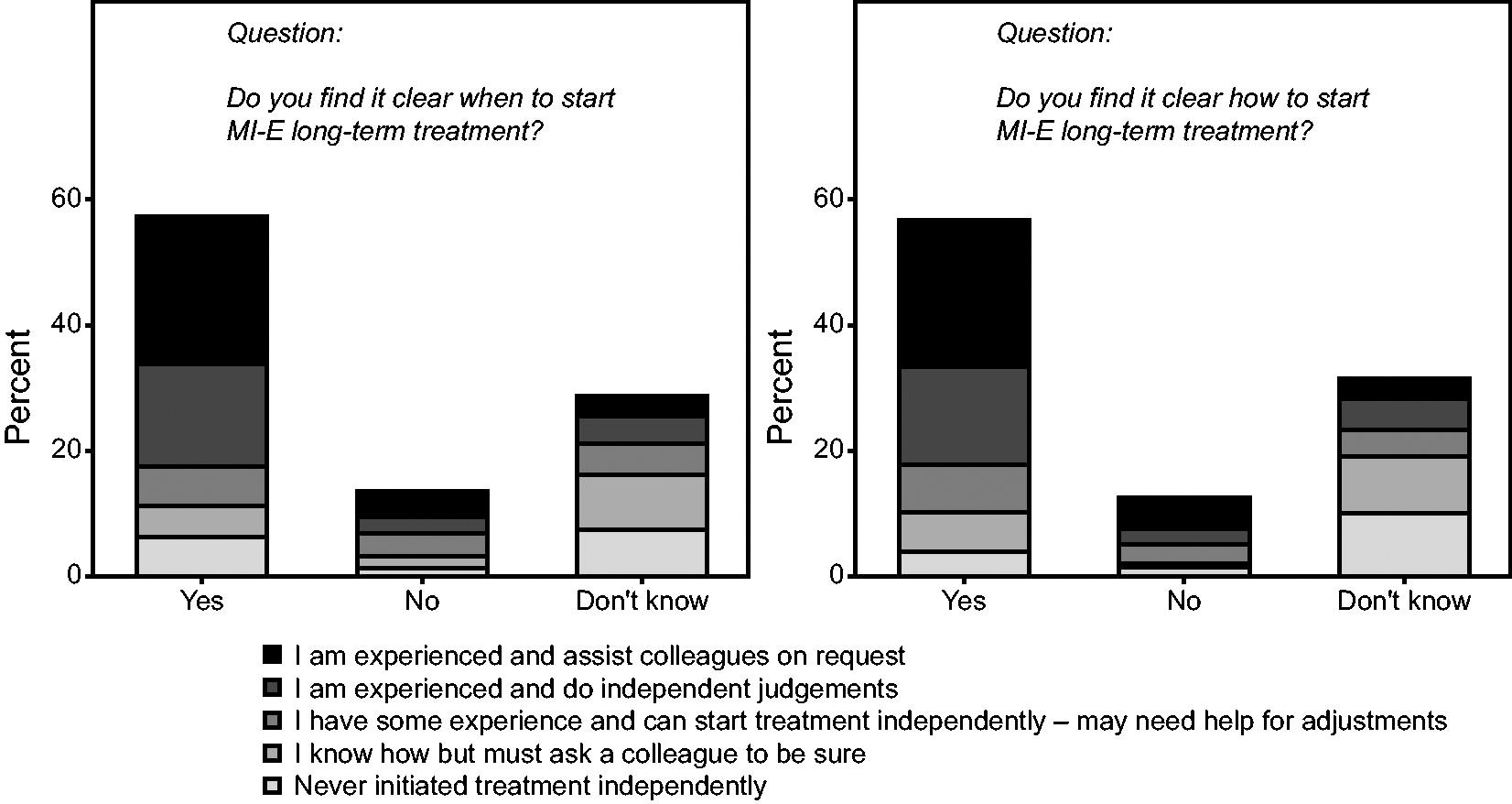
With their self-reported level of independence with MI-E, the respondents felt the recommendations were clear on when and how to start long-term use of MI-E.
Self-reported experience, independence, and knowledge of the guidelines of survey responders (n = 163)
Data are given as numbers with percentages.
MI-E, mechanical insufflation-exsufflation.
Further, 120 (75%) of the responders answered that they have access to designated resource persons with specific MI-E competence at their clinics. Overall, 39 respondents (24%) answered “yes,” and 90 (56%) “partially,” indicating that they felt their workplace had sufficient expertise in assessing needs, adapting, and following up on mechanical cough assistance for different patient groups.
The national MI-E routines
Respondents reported from multiple choice that the most common diagnoses for patients referred for assessment of MI-E appropriateness were neuromuscular diseases (n = 142, 87%) and spinal cord injuries (n = 75, 46%), followed by cerebral palsy and other central nervous system conditions (n = 72, 44%).
An overview of the assessments used to evaluate cough effectiveness and to determine long-term MI-E initiation is shown in Figure 3. In total, 125 (77%) responders applied multiple assessment approaches to evaluate the patients’ cough. The most common combination was qualitative assessment together with measurement of cough peak flow (CPF) (n = 68, 42%). A qualitative assessment of cough was the most frequent reported assessment mentioned (n = 112, 69%), followed by the measurement of CPF (n = 99, 61%) and a clinical evaluation of swallowing (n = 65, 40%).

List of assessments and tests used by the independent MI-E experience category level reported from multiple choice. Data are given as numbers. CPF, cough peak flow; FVC, forced vital capacity; MIC, maximal insufflation capacity; SVC, slow vital capacity; PEF, peak expiratory flow; PEmax, peak expiratory pressure; Plmax, maximal inspiratory pressure; SNIP, sniff nasal inspiratory pressure.
The assessment, individualization, education, and follow-up of long-term MI-E treatment were organized during hospitalizations, at the out-patient clinic, or as home visits (see Table 2 for details). In total, 122 (76%) of responders had easy access to an MI-E device for a clinical trial in referred patients, and 91 (58%) experienced that it was easy to apply for an MI-E device for long-term use from the health authorities.
An overview of the locations where long-term MI-E services were organized
Data are given as numbers (n) of responders choosing the particular location(s), multiple answers were possible.
An overview of how clinics maintain records of long-term MI-E users for follow-up purposes, based on multiple-choice responses, revealed considerable variability in the methods employed. Among the respondents, 43% used the patient journal system, 5% utilized an approved digital quality registry, and 10% maintained dedicated paper records. In addition, 27% reported “other routines” (not specified), whereas 15% indicated having no systematic overview. Regarding follow-up frequency, 43% of respondents reported conducting regular follow-ups (quarterly, semi-annually, annually, or less frequently, depending on the patient’s condition), and 19% performed follow-ups only upon patient request. Notably, 30% of respondents were unaware of local long-term MI-E follow-up routines, and 8% reported a complete lack of such routines (see online Supplementary Table S1).
In the long-term follow-up, the recorded information available on the MI-E devices’ SD card was used with most or some long-term MI-E users by 7 (4%) and 6 (4%) responders, respectively. Altogether, 75 (47%) and 71 (45%) responders did not use or did not know if the SD-card data were used, respectively. The 8% who used MI-E device SD-card data used the information to evaluate the adherence to treatment (n = 7), the device settings (n = 5) or the MI-E waveforms (n = 3), and to observe the tidal volume values (n = 5) or the CPF values (n = 3).
Discussion
The present study reports that 1,131 individuals in Norway currently use MI-E treatment at home, corresponding to an overall prevalence of 20.6 and 53.5 per 100,000 individuals in the overall population in Norway and in the population utilizing specialist health care services, respectively. The distribution of MI-E users by age group was 84% adults and 16% individuals <18 years.
This study provides insights into the prevalence of MI-E, as well as practices, professional experience, and independence associated with its use across Norway, highlighting variations in the follow-up of long-term MI-E users. Our findings suggest that Norway has a nationwide structure for the initiation and application of long-term MI-E therapy. However, it is noteworthy that follow-up routines for long-term users vary across health regions. These findings underscore the need for continuous efforts to improve care, particularly in the follow-up of long-term MI-E users (see Figure 4).

An illustration of the long-term MI-E landscape in Norway with the history, status, and future directions for national long-term MI-E use. This figure was created with artificial intelligence ChatGPT 4.0.
National prevalence and access to MI-E equipment
With a prevalence rate of 20.6 MI-E users per 100,000 individuals in the overall population, this study reveals an increasing proportion of MI-E users in Norway compared with an earlier national report presented at the 2011 Nordic Lung Conference, indicating a prevalence of 15 MI-E users per 100,000, with regional variations ranging from 12 to 30 per 100,000. 20 In the pediatric population, the present study reports that 180 children were equipped with MI-E devices in 2023, a notable increase from the 114 MI-E using children reported in 2017. 10 This increase in devices among both pediatric and adult populations may suggest an increasing prevalence of MI-E use, aligning with findings by Veldhoen et al, who reported a growing number of children introduced to long-term MI-E treatment in the Netherlands from 2005 to 2019. 5 The observed increase in the prevalence of MI-E users may reflect the growing body of literature and strengthened focus on MI-E therapy in recent years, which has likely contributed to greater awareness among clinicians and more widespread adoption of the treatment.
Recently, Toussaint et al mapped prevalence figures for long term mechanical ventilation and hypothesized that the development of home mechanical ventilation is closely correlated with the economic status of a given country. 15 By building on this, Norway’s full reimbursement policy for MI-E devices may also significantly facilitate access and drive adoption. Like Switzerland, this policy ensures equitable access to MI-E therapy. 21 However, unlike Switzerland, where reimbursement is contingent upon a CPF measurement below 270 L/min, 21 Norway adopts a more holistic approach, including clinical cough strength evaluation and the patient’s ability to clear airway secretions rather than relying on a strict CPF cutoff. Although this approach enhances individualization of care, it may also contribute to the perceived complexity in Norway’s application process for MI-E devices. Despite the reported easy accessibility of MI-E devices (77% of the responders), some health care personnel (21% of the responders) reported challenges applying devices for home use, indicating opportunities to streamline the provision process for long-term use. Since reimbursement policies in Norway differ significantly from those in the USA and many other countries, this may influence patient access to MI-E elsewhere. Further research is needed to better understand the factors contributing to these challenges and to optimize the application process.
Clinicians self-reported MI-E experience and independence
Respondents reported long clinical experience and high independence in using MI-E, particularly among physiotherapists, who constitute most surveyed clinicians. Except for the recent insights into upper airway response challenges in bulbar patients, 20,22 –26 barriers to long-term MI-E are not well-documented. However, clinician confidence in successful MI-E initiation and management is appraised in a recent publication, particularly for respiratory physiotherapists who play a central role in assessing and training patients. 11 This confidence likely reflects over 20 years of systematic training efforts by the National Advisory Unit on long term mechanical ventilation and its network, especially in assessing, initiating, and individualizing MI-E therapy across Norway, where airway clearance and cough techniques have been physiotherapists’ responsibility. Notably, a significant portion of Norwegian respondents were familiar with either local or national guidelines, 18 although only a small subgroup was familiar with international recommendations. 2,3,6 Inconsistent adherence to guidelines for cough effectiveness monitoring has been identified as a barrier, particularly in acute care settings, 17 and the results of this survey suggest that although national initiatives have effectively disseminated MI-E knowledge, further emphasis on aligning with international best practices may still enhance clinician training and support. These factors underscore the importance of addressing further education to optimize MI-E use across settings.
National routines for cough effectiveness monitoring and MI-E follow-up
The present study identified considerable variability in the assessment strategies and follow-up routines used to monitor long-term MI-E users. Although international guidelines and literature emphasize the measurement of CPF as a key assessment tool, 2,3,5,6,17,27 respondents in Norway reported combining a broader range of methods, from qualitative cough assessments to CPF measurement. This diverse approach aligns with clinical recommendations from the past decade, which advocate for flexible assessment strategies tailored to the patient’s diagnosis, clinical context, and the clinician’s expertise. 9,11,22 –25,27,28
The variability in follow-up routines, with as much as 30% and 8% of respondents reporting being unaware of or lacking local follow-up routines, highlights a notable gap in standardized care practices. These findings underscore that the Norwegian national guidelines on MI-E therapy, published in 2012, did not include detailed recommendations for the follow-up of long-term users, 18 leaving room for disparities in practice. 12 –15 Dale et al demonstrated that inconsistent MI-E follow-up can lead to uncertainties regarding device usage and treatment efficacy. 12 Building on this, the significant variation observed in follow-up routines by the clinicians in our study may influence treatment adherence and, consequently, the long-term clinical effectiveness of MI-E. This highlights the importance of quality assurance in follow-up routines to support sustained treatment adherence and optimize clinical outcomes for long-term MI-E users.
Moreover, although much of the existing MI-E literature has focused on demonstrating treatment efficacy, identifying needs through objective measurements, and initiating therapy, the follow-up of long-term users remains an underexplored area. 12 As a result, clinician knowledge about effective follow-up practices remains limited. To promote more consistent national clinical follow-up for MI-E users, the establishment of standardized protocols and dedicated health record systems tailored to individuals with weak cough could significantly enhance patient monitoring.
In Norway, the Units for Medical Home-Care Equipment, which maintain comprehensive patient lists and collaborate with clinicians in specialized health care services, provide a valuable resource that clinicians can leverage to address this challenge effectively. Enhanced collaboration between these units and clinicians could represent a first step toward developing more streamlined and effective follow-up routines, ultimately benefiting long-term MI-E users. Furthermore, implementing systematic follow-up appointments within predefined timeframes and ensuring timely reassessment could further enhance adherence to therapy and the overall quality of care. Future research should include investigating and refining follow-up strategies to optimize clinical outcomes and support sustainable long-term MI-E use.
Strengths and limitations
A key strength of this study is its national scope, capturing nationwide data from a wide range of health care professionals, which provides an overview of MI-E use across all ages and clinician practices at a countrywide level. In addition, the use of multiple data sources, including population data from high-quality registries, equipment delivery reports from Units for Medical Home-Care Equipment, and surveys, enriches the robustness of the findings and allows for accurate prevalence estimates of MI-E users. We provided prevalence estimations both from the overall population and specialized health care services to increase the comparability with other countries. Furthermore, by focusing on both clinical confidence and practice variability, this study contributes to understanding how long-term MI-E therapy is applied in a national context with equitable access to health care resources, offering insights for optimizing MI-E service delivery in similar health care systems.
Limitations of the study are, first, that the response rate for the survey could not be accurately determined, given the distribution through social media and e-mail lists, potentially introducing selection bias. Respondents with greater experience or a positive attitude toward MI-E may have been more likely to participate, thus overestimating the national independence and confidence in MI-E application. The mix of single-choice and multiple-choice questions in the questionnaire posed challenges for statistical analyses, limiting the study to descriptive reporting of the data. Furthermore, the study predominantly represents specialized health care settings, with limited data from primary care clinicians. In addition, although Norway’s comprehensive public funding may ensure broad MI-E access, these findings may not be generalizable to countries with alternative health care funding structures. Last, although the sample size of 182 respondents may limit the ability to draw definitive conclusions, the study provides important insights and forms a valuable basis for further discussion and research on MI-E use and practices in a smaller health care system like Norway’s.
Conclusions
In Norway, MI-E has been used since 2001, supported by a government-funded infrastructure that aims for equitable access to treatment for those in need of mechanical cough assistance. The National Advisory Unit on long term mechanical ventilation has focused on advancing education and promoting knowledge of cough assessment and MI-E initiation. Despite these efforts, this study highlights substantial variability in follow-up routines for long-term MI-E users. Although Norwegian clinicians demonstrate extensive experience and strong independence in MI-E use, employing a variety of assessment methods to evaluate cough effectiveness and individualize therapy, patient follow-up routines stand out as an area with high potential for improvement. Establishing national and international recommendations to standardize follow-up practices and provide consistent care across regions is key to optimizing MI-E therapy outcomes and ensuring high-quality, long-term care for patients.
Footnotes
Acknowledgments
The authors thank all 18 Norwegian Units for Medical Home-Care Equipment for providing the MI-E device use data and the study responders for their contributions. In addition, the authors thank MI-E experts Eivind Hageberg Baunan, Anne Kristine Brekka, Karianne Bjåstad, Martin Espedal, Tone Helgesen, Matea Hovde, Elin Johnsen, Margrethe Kolnes, Mona Veie Lund, and Karen Thomas for reviewing the survey prior to its release.
Ethical Considerations
The present study assessed clinical practice using anonymized, open-accessible data from national registers and anonymized data from health care professionals, and the Western Norway Health Region Data Protection Officer advised that an ethical committee approval was redundant. The survey introduction informed respondents about the upcoming publication of the results, emphasized voluntary participation, and clarified that their consent was implied through self-enrollment and engagement with the study.
Author Disclosure Statement
Dr. Andersen discloses a relationship with Breas and ABM Respiratory Care (member of advisory boards and honoraria for lectures). Ms. Hov discloses a relationship with Breas (lecture fee) and Biogen (member of advisory board). Mrs. Nørstebø has disclosed no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.