A noninvasive ventilation (NIV) mask has been designed to deliver NIV with expiratory washout to improve efficacy of ventilation by optimizing clearance of expired gases from the anatomic dead space. This study compared the performance and comfort of a novel investigational mask with expiratory washout with a conventional mask during NIV therapy.
Methods:
In this pilot crossover study, participants with severe stable COPD attended a single visit to receive bi-level NIV through 2 masks; the investigational mask with expiratory washout and a conventional mask. The order of mask use was randomly allocated, and each mask was used for 60 min with a 30–60-min washout in between. The primary outcome was transcutaneous carbon dioxide at 60 min. Other physiologic and NIV device variables were also assessed.
Results:
The mean difference (95% CI) in the transcutaneous carbon dioxide between the investigational and conventional masks at 60 min, adjusted for baseline, was –0.74 mm Hg, 95% CI –2.81 to 1.33 mm Hg (P = .45). The investigational mask with expiratory washout elicited a lower tidal volume (–128.7 mL, 95% CI –190.0 to –67.3 mL; P < .001) and minute ventilation (–2.28 L/min,, 95% CI –3.12 to –1.43 L/min; P < .001), and a higher leak (7.96 L/min, 95% CI 4.39-11.54 L/min; P < .001) than the conventional mask. There were no differences in other physiologic responses or ratings of dyspnea or comfort.
Conclusions:
NIV therapy delivered by using a novel mask with expiratory washout was similarly effective at reducing transcutaneous carbon dioxide, whereas the delivered tidal volume and minute ventilation were significantly lower when compared with a conventional mask in participants with severe COPD.
Introduction
Noninvasive ventilation (NIV) delivers pressurized air to the lungs, which influences pulmonary mechanics in ways that can reduce work of breathing and improve gas exchange. Using these physiologic effects has advanced the care of many conditions, most notably acute and chronic respiratory failure and sleep-disordered breathing.1-4 Whereas the timing, duration, and degree of pressure play a central role in the efficacy of NIV, the characteristics of the chosen patient interface can also influence treatment success.5
Most commonly, the patient interface consists of a mask with a soft cushion that is in contact with the skin and is fastened to the head by using a harness with adjustable straps. The mask may be oronasal, nasal, pronasal, or full face, with modern masks purposefully engineered to optimize ventilation and improve comfort and tolerability. Because the mask adds to the redundant component of the NIV circuit, which plays no role in the exchange of gases, the internal mask volume has historically been considered an important modifiable contributor to functional dead space, with design efforts focused on minimizing mask volume to decrease carbon dioxide (CO2) rebreathing and retention. However, in vivo studies report that the internal volume of the masks has a lesser impact on CO2 rebreathing than initially thought and that most of the dead space within an NIV circuit is from the upper airway.6-8
Consequently, interest has shifted to the upper-airway component of the dead space as a potentially modifiable factor that could be targeted in a way that improves the efficacy of NIV therapy. One approach that might influence conditions in the upper airway is the use of a specially engineered mask interface that generates oronasal gas flow patterns that optimize washout of expired gases. In theory, an interface that more actively purges CO2–rich expired gas from the airway before the next breath might improve dead-space clearance and, in turn, reduce ventilatory work. Yet, little is reported about how NIV mask design influences gas clearance from the upper airway, and this theory has only indirect support from studies that assessed gas-flow patterns while administering high flow nasal oxygen.9,10
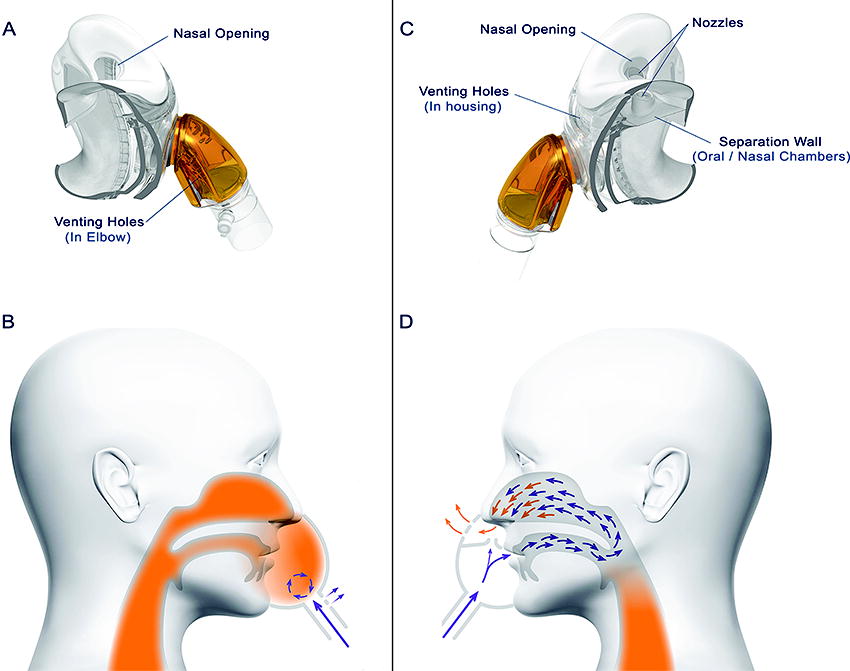
The investigational mask (OptiNIV, Fisher & Paykel Healthcare, Auckland, New Zealand) is a mask for use with NIV therapy, with specific design features that optimize expiratory washout of CO2. Improved CO2 clearance is achieved by a unique mask design with a separation wall between the mouth and nose that encourages the flow of gas at the end of expiration toward the oropharynx, up into the nasopharynx, and then out the nares where the CO2–rich gas from the upper airway is purged through specially situated venting holes in the mask (Fig. 1). The design is proposed to reduce functional dead space and improve the efficiency of ventilation. The anticipated effect of this mask compared with a conventional mask is to either reduce arterial CO2 tension or to reduce breathing frequency and/or tidal volume () without influencing arterial CO2 levels.
Images of the investigational mask interface. (A) The conventional noninvasive ventilation (NIV) mask used in this study. (B) The gas-flow patterns in the upper airway at the end of expiration with the use of the conventional NIV mask. (C) The investigational mask used in this study. (D) The gas-flow patterns in the upper airway at the end of expiration with the use of the investigational NIV mask. Purple arrows represent the flow pattern of gases delivered by the ventilator, orange shading represents expired CO2, orange arrows represent the proposed additional purging of CO2 from the upper airway with the investigational mask at the end of expiration immediately before the next inhalation.
The primary aim of this pilot study was to compare the change in transcutaneous PCO2 () from baseline between the investigational mask and a conventional mask (Visairo, Fisher & Paykel Healthcare) after 60 min of NIV therapy. Secondary outcomes included physiologic responses to the interventions as well as comfort and dyspnea scores.
QUICK LOOK
Current knowledge
The volume and composition of gases in the anatomic dead space are an important component of ventilation. Bench testing of upper-airway models has identified that a specially designed noninvasive ventilation mask that improves expiratory washout of gases from the upper airway can reduce the contribution of the dead-space volume to the overall tidal volume.
What this paper contributes to our knowledge
In participants with stable severe COPD, noninvasive ventilation delivered using an investigational mask with expiratory washout achieved similar alveolar ventilation but with a smaller tidal volume and minute ventilation compared with a conventional mask.
Methods
Study design
The study was a single-center, randomized, active controlled, unblinded crossover pilot study with people who had severe chronic COPD. The study involved a single visit, which consisted of 2 interventions of bi-level spontaneously timed NIV therapy, one with the investigational mask, the other with a conventional mask. The study was approved by the New Zealand Central Health and Disabilities Ethics Committee (reference 21/CEN/149) and prospectively registered on ClinicalTrials.gov (NCT04947852). The participants provided written informed consent before any study procedures.
Participants
Potentially eligible patients were identified from a preexisting study contact database. Invitation letters were mailed and telephone calls were made, which invited participants to undergo screening for this trial. Participants with a self-reported physician’s diagnosis of COPD were eligible if they were ≥18 years old, had 10-min average baseline values of ≥45 mm Hg (Sentec Digital Monitoring System, Sentec AG, Therwil, Switzerland) and an arterial oxygen pressure measured by pulse oximetry was ≥ 85%. Patients were excluded if they had a FEV1/FVC ≥ 0.70, a body mass index >40 kg/m2, hypercapnia that was judged by a study physician (AS, LK, RB, RS) to be primarily due to obesity-hyperventilation syndrome and/or obstructive sleep apnea, a long-term domiciliary oxygen prescription of >4 L/min, any contraindication to NIV as per the British Thoracic Society guidelines,5 and those with “unstable COPD,” defined as an exacerbation of their COPD that required antibiotics and/or oral steroids within the previous 2 weeks or hospital admission within the previous 6 weeks. Individuals were also excluded if they had a nasal condition that could impair nasal breathing or any other conditions that were deemed by the study physician (AS, LK, RB, RS) to present as a safety risk or impact the feasibility of the study or the results.
Protocol amendment
The exclusion of patients with a ≤ 45 mm Hg resulted in a high screen failure rate, which warranted a change to eligibility criteria. The inclusion criterion of ≥ 45 mm Hg was removed and replaced with an FEV1 of ≤50% predicted (COPD Global Initiative for Chronic Obstructive Lung Disease grade 3 [severe] and 4 [very severe]11) This protocol amendment was approved by the Health and Disabilities Ethics Committee before randomizing any participants; all the participants satisfied the amended eligibility criteria.
Procedures
For screening, the participants self-reported their medical and smoking histories and current medications. A SizeMe (Fisher & Paykel Healthcare) mask sizing guide was used to confirm that the participant would fit the face mask. Spirometry was performed according to American Thoracic Society/European Respiratory Society criteria (Easy on-PC, ndd Medical Technologies, Zurich, Switzerland).12 After 20 min of rest with a sensor attached to the participant’s ear lobe (Sentec), baseline , , and heart rate were monitored for a further 10 min to obtain the average baseline values. The sensor remained attached to the ear lobe throughout the visit.
Participants were randomized to wear either the investigational mask (Fig. 1) or the conventional mask first. The randomization schedule was computer generated via the SMART-TRIAL database, within which all data were collected, bar identifiable screening information, which used a paper-based case report form for local storage by the study site. For each intervention, the participants underwent 60 min of bi-level NIV therapy with no backup rate via a V60 ventilator (Phillips, Amsterdam, Netherlands) with an inspiratory pressure of 12 cm H2O and an expiratory pressure of 7 cm H2O. We selected a relatively low inspiratory pressure of 12 cm H2O because higher inspiratory pressures that are commonly used in exacerbations of COPD were considered unlikely to be tolerated in a largely NIV-naive participant group. An expiratory pressure of 7 cm H2O was considered an appropriate expiratory pressure that is commonly used for exacerbations of COPD. Humidified air was delivered at 29°C when using a F&P 950 Humidification System (Fisher & Paykel Healthcare). A single-limb heated circuit was used without an expiratory port because both study masks were vented. As such, no ventilator leak test was performed, and all measured leaks are reported as the total leak sensed by the V60 ventilator. To assess whether the mask design itself resulted in systematically different V60 ventilator measured , pretrial bench testing was conducted by delivering an inspiratory pressure of 12 cm H2O and an expiratory pressure of 7 cm H2O with both the investigational and the conventional NIV mask, through an anatomically accurate upper-airway model with an in-line flow meter (IMT FlowAnalyser PF-302, IMT Analytics AG, Buchs, Switzerland) at the level of the trachea, to a TestChest (Organis-gmbh, Landquart, Switzerland) lung simulator. Paired measures of reported by the V60 and the flow meter did not significantly differ with both the investigational and conventional masks (Supplementary Appendix S1).
The participants completed a 30-min washout period between interventions; if returned to within ±2 mm Hg of the baseline value, then they proceeded onto the second intervention, otherwise the washout period was extended until either they returned to within ±2 mm Hg of baseline or completed 60 min of washout. Breathing frequency, minute ventilation, , and ventilator calculated total leak were continuously monitored by using the Philips V60 ventilator (Phillips, Amsterdam, Netherlands) sensing algorithms that were displayed on the device interface and captured on the logging software of an external computer. , , and heart rate were continuously measured by using the Sentec monitoring device. After each intervention, the participants immediately completed a modified 0–10 Borg dyspnea questionnaire13 and a subjective comfort questionnaire, and adverse events were assessed. The comfort questionnaire consisted of 5 items that were rated on a 6-point scale, with lower scores indicating more favorable ratings. The 5 items included “overall comfort,” “under nose comfort,” “unintentional air leak,” “claustrophobia,” and “mouth and nose dryness.”
Outcomes
The primary outcome was at 60 min of the intervention, adjusted for baseline. Secondary outcomes included the proportion of the participants who had a decrease in by ≥4 mm Hg and ≥8 mm Hg compared with baseline as well as , , heart rate, breathing frequency, minute ventilation, , and leak, all adjusted for baseline, at time points 0, 5, 10, 15, 30, and 60 min. Additional secondary outcomes that relate to mask comfort and tolerability included the proportion of the participants who withdrew from the intervention before it was completed, and results from the modified Borg dyspnea scale and the subjective comfort questionnaire.
Sample size
No previous data were available to estimate the baseline adjusted mean difference and associated SD for compared between the investigational and control masks, so a conventional power calculation could not be made. As such, a theoretical model for selecting an optimal pilot study sample size was used.14 For a main trial with a “medium” standardized effect size, 90% power, and 2-sided 5% significance, an estimated 15 participants would provide the optimal pilot study sample size. We chose to include 16 participants to ensure that randomized allocations were evenly balanced.
Statistical analysis
For the primary analysis, a linear mixed model was used with fixed effects of mask and mask order, and random effects for the participants to account for the crossover design. For the secondary analyses, linear mixed models were used with an additional fixed effect for time (0, 5, 10, 15, 30, 60 min) and a time by mask interaction. In the event that there was no significant time by mask interactions, the overall difference averaged over all time points was used because it was considered to be a more accurate representation of the difference between masks. Mean differences were calculated as the investigational mask minus the conventional mask. Analysis of marginal proportions was by using the McNemar test. Statistical analysis was performed by using SAS (version 9.4, SAS Institute, Cary, North Carolina), and statistical significance was set at P ≤ .05.
Results
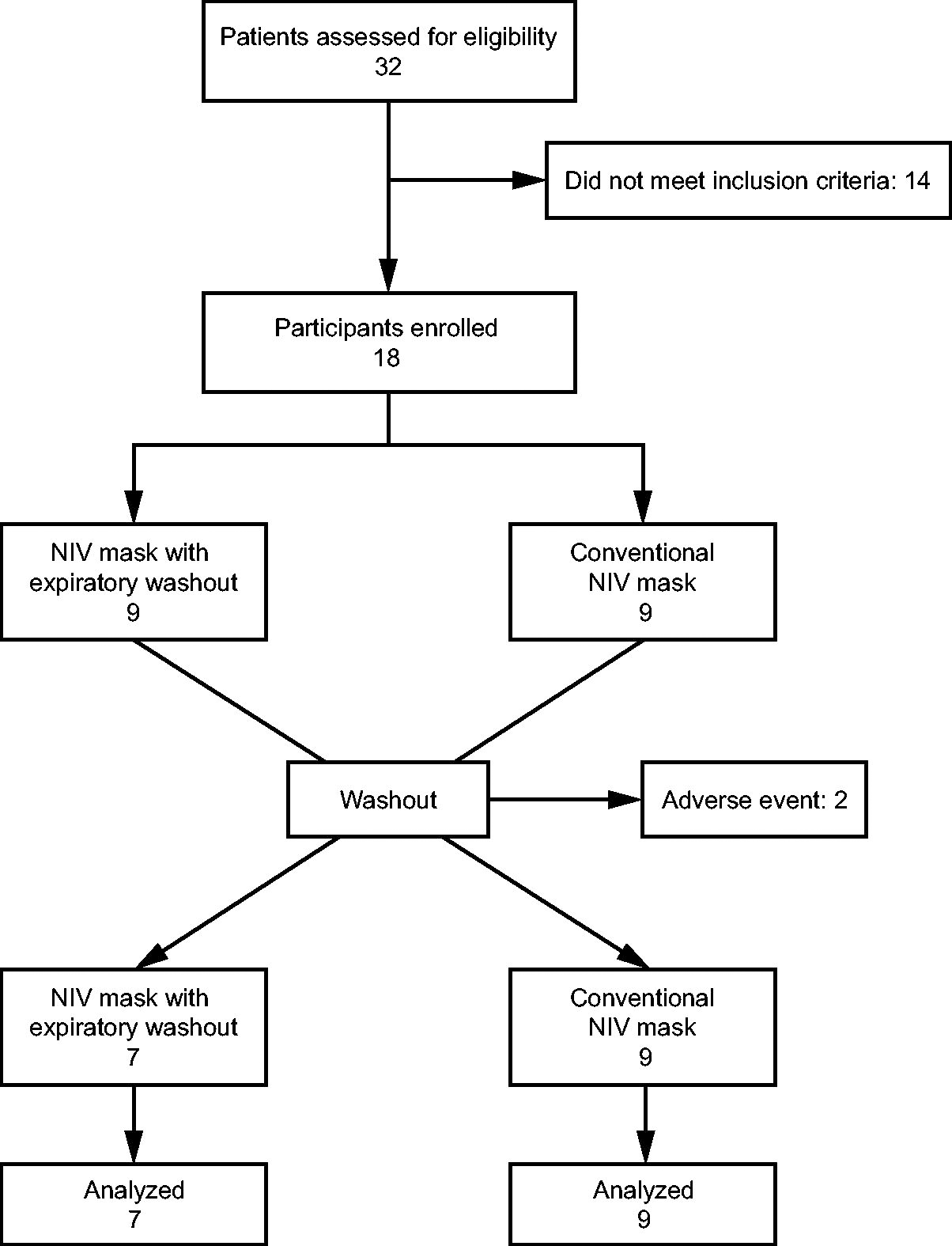
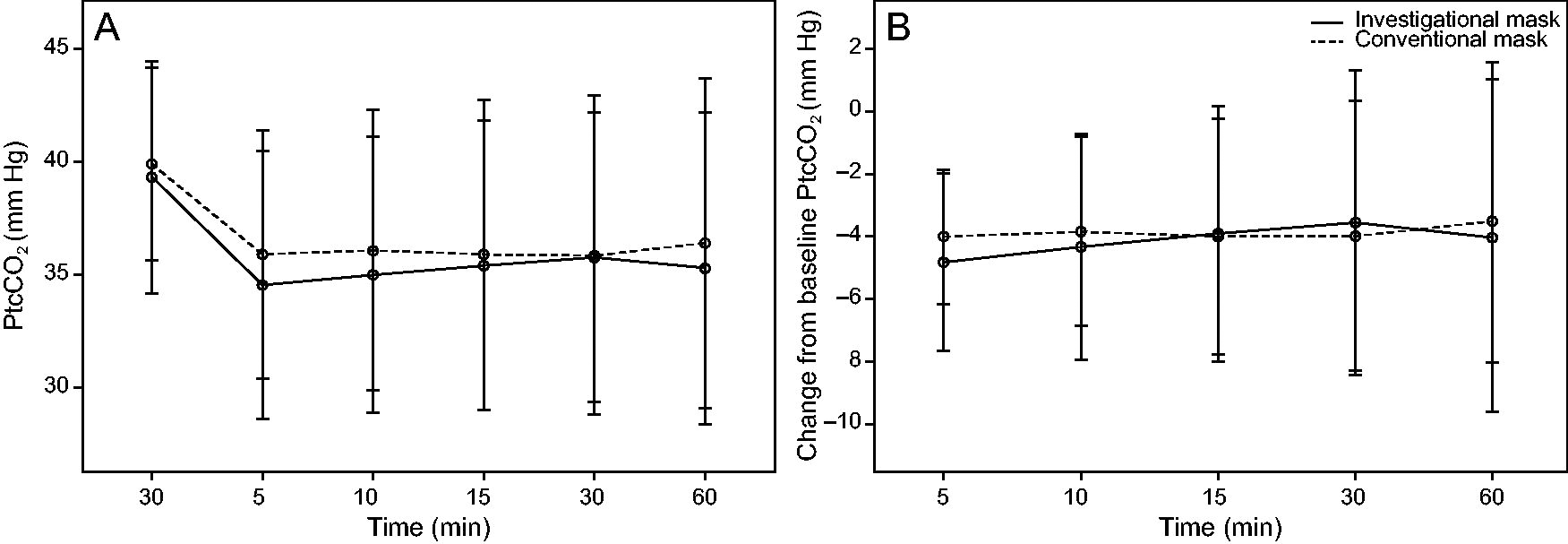
Thirty-two patients were screened and 18 were randomized (Table 1). Participants had severe air-flow obstruction, with a mean FEV1 predicted of 35.3%. The mean baseline and were 38.9 mm Hg and 94.3%, respectively. The Consolidated Standards of Reporting Trials flow diagram is presented in Figure 2. Two participants did not complete the interventions and were replaced, which resulted in 16 complete data sets for analysis: one participant was withdrawn from the study due to a Crohn exacerbation during the washout period and one due to not tolerating the therapy during the first intervention (conventional mask). One participant was prescribed home oxygen therapy and commenced on this flow per protocol, although because exceeded the participant’s prescribed target range of 89–92%, oxygen was down-titrated to 21% within the first 3 min of the first intervention and the participant was not administered any supplementary oxygen during the second intervention. Five participants required an extended washout period, 3 of whom did not return to within ±2 mm Hg of baseline before commencing the second intervention after 60 min of washout. The mean ± SD at 60 min for the investigational and conventional masks was 35.3 ± 6.9 mm Hg and 36.4 ± 7.3 mm Hg, respectively, with a mean difference in the of –0.74 mm Hg, 95% CI –2.81 to 1.33 mm Hg (P = .45). At 60 min, the fell by a mean ± SD of –4.0 ± 5.6 mm Hg for the investigational mask and by –3.5 ± 4.5 mm Hg with the conventional mask (Table 2, Fig. 3).
Flow chart. NIV = noninvasive ventilation.
Distribution plots of (A) transcutaneous carbon dioxide () by time, and (B) change from baseline by time across all the participants when using investigational and conventional masks. In these distribution plots, the symbol is the mean and the whiskers extend from the minimum to maximum values.
Participant characteristics (N = 16)
Characteristic
Results
Age, y
69.1 ± 7.7
Men:women, n
12:4
Body mass index, kg/m2
25.4 ± 5.7
FEV1, % predicted
35.3 ± 0.3
FVC, L
2.69 ± 0.81
FEV1/FVC
0.37 ± 0.08
, mm Hg
38.9 ± 4.4
, %
94.3 ± 2.2
Smoking status, n (%)
Current
1 (6.3)
Former
14 (87.5)
Never
1 (6.3)
Had previously received NIV therapy, n (%)
1 (6.3)
Values are presented as mean ± SD, unless otherwise stated.
The mean difference between the investigational mask and the conventional mask at 60 min.
The mean difference between the investigational mask and the conventional mask with the 5, 10, 15, 30, and 60-min differences averaged.
, transcutaneous carbon dioxide; , tidal volume.
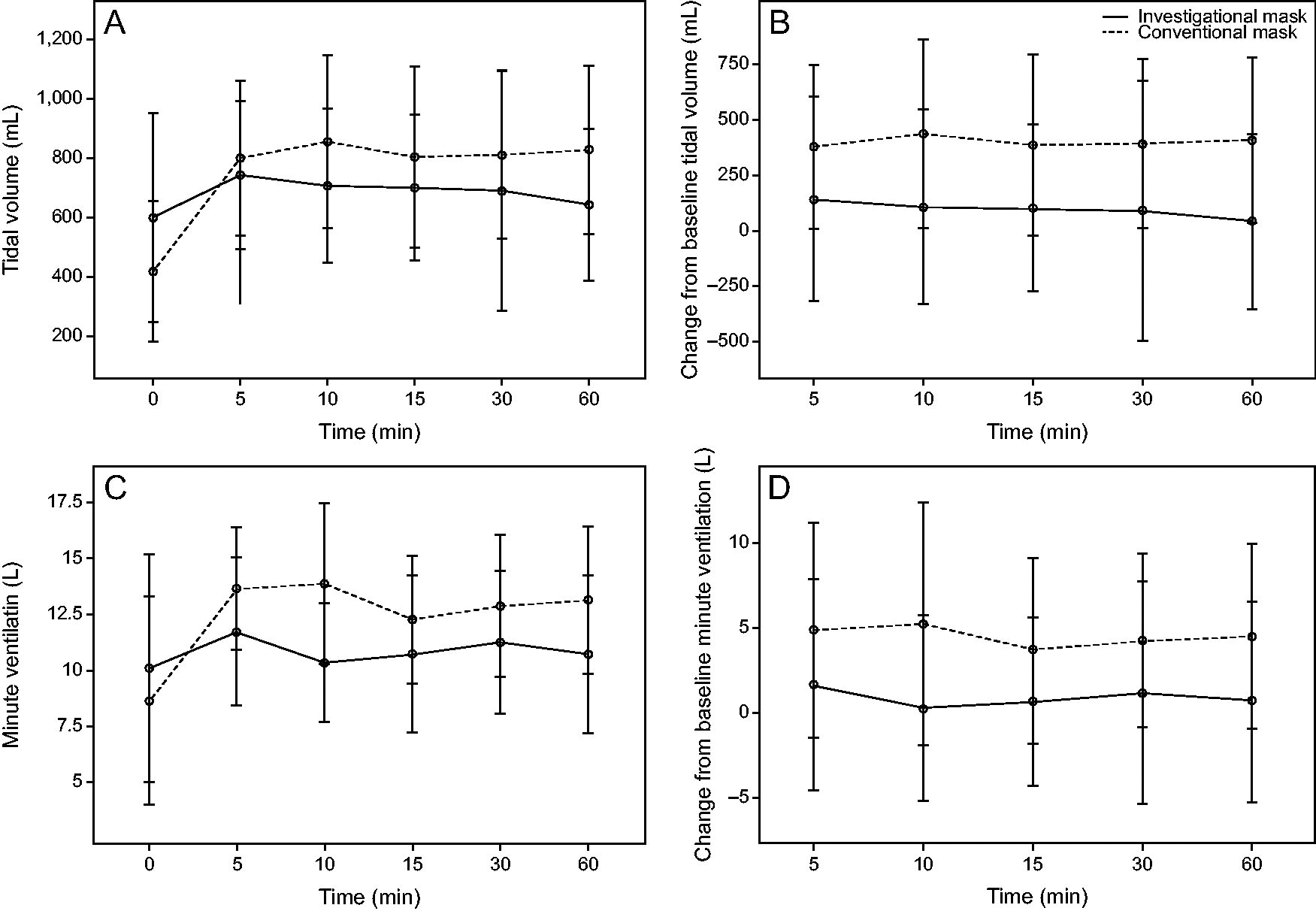
The baseline measurements of and minute ventilation by using the investigational mask were higher than that of the conventional mask (Table 2). After 5 min of therapy, and minute ventilation when using the conventional mask had risen above that of the investigational mask and remained higher than the investigational mask for the remainder of the 60-min interventions (Fig. 4). Total leak at baseline was higher with the investigational mask and remained higher than the conventional mask throughout the interventions (Table 2, Fig. 5). Over the 60-min intervention periods, when measurements were adjusted for the baseline values, the investigational mask elicited a significantly lower and minute ventilation, and a significantly higher total leak than the conventional mask (Table 2). There was no time by mask interactions for (P = .84), (P = .27), heart rate (P = .41), breathing frequency (P = .36), (P = .71), minute ventilation (P = .55), or leak (P = .09). There were no significant overall mean differences in , , heart rate, or breathing frequency between masks when averaged over the intervention time points (Table 2).
Distribution plots of (A) tidal volume () by time, (B) change from baseline by time, (C) minute ventilation by time, (D) change from baseline minute ventilation by time across all the participants who used investigational and conventional masks. In these distribution plots, the symbol (small circle) is the mean and the whiskers extend from the minimum to maximum values.
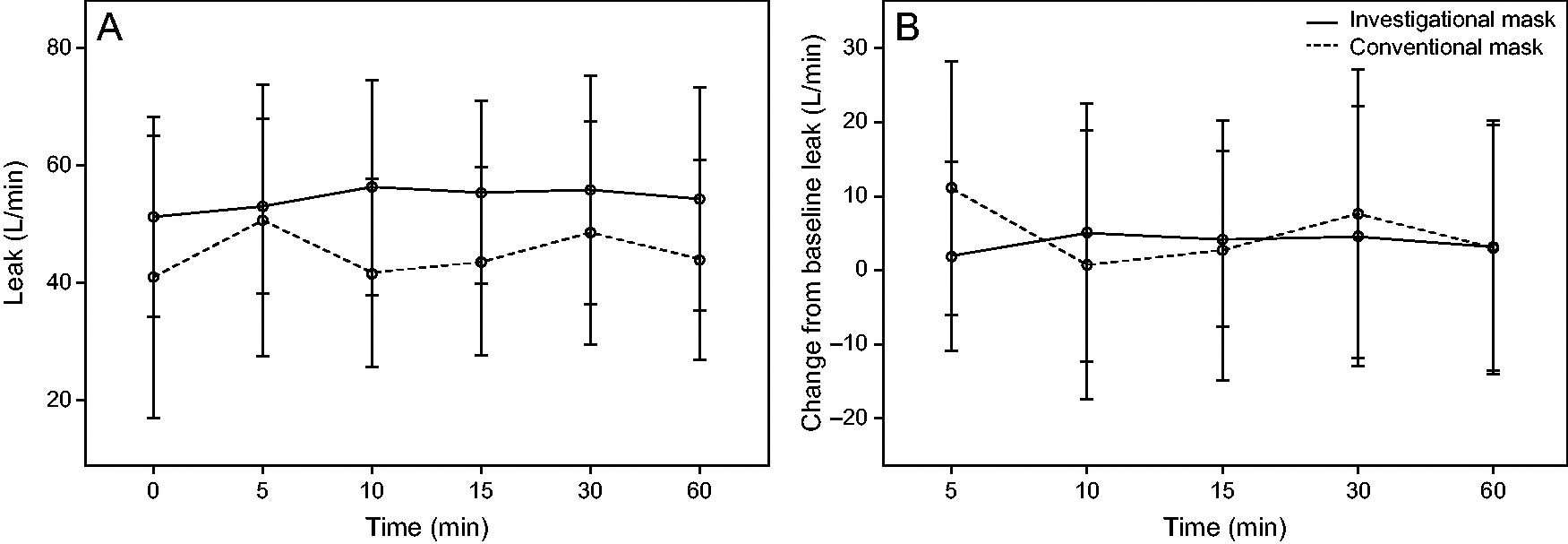
Distribution plots of (A) leak by time and (B) change from baseline leak by time across all the participants who used investigational and conventional masks. In these distribution plots, the symbol (small circle) is the mean and the whiskers extend from the minimum to maximum values.
There were no differences in the proportion of the participants with a decrease in by ≥ 4 mm Hg (P > .99) and ≥ 8 mm Hg (P > .99) at time 60 min between the masks. Two participants experienced decreases in of ≥4 and ≥8 mm Hg with both masks. For the decrease in of ≥4 mm Hg, 2 participants achieved this reduction with the investigational mask but not with the conventional mask, whereas 2 participants achieved this reduction in the conventional mask but not with the investigational mask. One participant experienced a reduction in of ≥8 mm Hg with the investigational mask but not with the conventional mask, and one participant experienced a reduction of ≥8 mm Hg with the conventional mask but not with the investigational mask.
There were no significant differences between masks in the modified Borg dyspnea scores (0.09 [–0.56 to 0.74]; P = .77) or any of the comfort scores, including for “overall comfort” (–0.31 [–0.92 to 0.29]; P = .29), “under nose comfort” (–0.44 [–1.14 to 0.26]; P = .20), “unintentional air leak” (–0.13 [–0.83 to 0.58]; P = .72), “claustrophobia” (–0.13 [–0.45 to 0.20]; P = .43), and “mouth and nose dryness” (0.06 [–0.35 to 0.47]; P = .75).
Twelve adverse events were reported by 11 of the randomized participants (61.1%) (Supplementary Table S1). Only mild adverse events were reported after the investigational intervention, including dryness under the nose, a runny nose, feeling lightheaded, coughing, and tingling in the limbs. The tingling occurred concomitantly with an abnormally low and was judged to be caused by the NIV therapy rather than the mask itself. After the comparator intervention, the adverse events included dryness, sore nose, headache, and feeling lightheaded, all of which were rated as being mild. Six adverse events were not judged to be related to the device, 4 adverse events were judged to possibly be related to the device (investigational mask, n = 2; comparator mask, n = 2), and 3 adverse events were judged to be caused by the device (investigational mask, n = 1; comparator mask, n = 2). There were no serious adverse events.
Discussion
This study demonstrated no significant difference in adjusted for baseline between the investigational and the conventional mask over 60 min of bi-level NIV therapy in adults with stable severe COPD, which suggests no difference in how each mask influenced alveolar ventilation. In addition to alveolar ventilation, there was no difference in breathing frequency between the masks. There were differences in other components of ventilation, including significantly lower and minute ventilation, and significantly higher total leak, with the investigational mask. When these parameters are considered together, one potential interpretation is that the use of the investigational mask leads to a reduction in the dead-space component of the measured . This interpretation aligns with the proposed mechanism of action of the investigational mask and supports the study hypothesis that targeting expiratory washout of the anatomic dead space through a specialized mask design is a feasible approach for influencing minute ventilation and .
As reported in previous studies, higher levels of leak can affect the accuracy of ventilator sensing software, which results in spurious underestimation of .15,16 An alternate explanation for the observed reductions in and minute ventilation in the present study is that the additional leak inherent in the use of the investigational mask resulted in a measurement error. Although pre-study bench testing confirmed the accuracy of the Philips V60 ventilator sensing software, there was no secondary independent measure of during the clinical trial itself, so we are unable to directly refute this potential explanation; however, the trends in and minute ventilation observed between the investigational and conventional masks over the trial period did not seem to follow a pattern that we would consider to be consistent with systematic underestimation of that occurred only with the investigational mask.
The dyspnea and comfort scores were not significantly different between the 2 masks, which highlights that the novel mask design with its unique gas-flow pattern seemed to reduce and minute ventilation without an appreciable difference in patient comfort. Although it would be reasonable to expect a decrease in dyspnea with the use of an investigational mask that has the effect of lowering , no difference in dyspnea between the masks was found. Mask leak is often cited as a reason for poorer mask comfort17; yet, reassuringly, the comparison of the participants’ response with the “unintentional air leak” component of the comfort questionnaire did not reveal any significant difference in comfort related to mask leak.
The difference in measured and minute ventilation seen with the investigational mask occurred with no significant between-masks difference in measured . This suggests that, although when using the investigational mask compared with the conventional mask, the participants took relatively smaller breaths, which did not result in a difference in alveolar ventilation. This may have clinically important implications because smaller when using the investigational mask may confer less alveolar distention and reduced work of breathing for the same amount of alveolar ventilation and CO2 clearance. High in patients who are mechanically ventilated are clearly detrimental, with the resultant increase in alveolar distention and transpulmonary pressures that contribute to the development of ventilator-induced lung injury.18 Patients who receive NIV for acute respiratory failure also seem at risk from the adverse effects of excessive , with exposure to high during NIV being independently associated with NIV failure.19 Furthermore, as the relative contribution of dead space to changes, outcomes for patients on mechanical ventilation has also been shown to differ. Specifically, those who have a higher fraction of dead space tend to have higher mortality rates.20-22 Although high ventilation and higher dead-space fractions are associated with patient harm, it remains to be determined whether reducing through reductions in the anatomic dead space with a novel mask design would influence clinically important patient outcomes.
Limitations of this study were the inclusion of participants who were normocapnic, whose ventilatory parameters were measured by using indirect techniques. An accurate approximation of arterial CO2 can reliably be achieved with a earlobe sensor23; however, , minute ventilation, and leak were all estimated by using the ventilator sensing software, which has inherent accuracy limitations and was not corroborated with independent measurement techniques. Although the order that the participants received each therapy was randomized and the 2 groups were well balanced, a washout period of 30 to 60 min may have been insufficient to minimize a carryover effect between interventions. Because the study population were largely naive to NIV therapy, a relatively low inspiratory pressure was selected to improve NIV tolerance. In addition, the study population was not representative of patients who would be considered to have an indication for acute or chronic NIV therapy. These factors mean that the study findings are not generalizable to real-world conditions and further evidence is required to assess the effects of the investigational mask in the patient populations that have an indication for its use.
Conclusions
This pilot study found that, when compared with a conventional pronasal mask, the investigational mask seemed to improve expiratory washout of the anatomic dead space while maintaining similar alveolar ventilation with no discernible difference in tolerability. Further studies are warranted to first corroborate these findings with more accurate measurement techniques and then to assess how the proposed physiologic effects of the investigational mask might translate into clinical outcomes when used in acute care, particularly for those in acute hypercapnic respiratory failure with high ventilation.
Footnotes
Author Disclosure Statement
Ms. Fogarin and Mr. Zoellner are employees at Fisher & Paykel Healthcare; they were involved in the study design and interpretation of the data, but they were not involved in the collection or analysis of the data. Dr. Beasley declares that the Medical Research Institute of New Zealand has received research funding from Fisher and Paykel Healthcare, outside of this study. Dr. Kirton has received travel support from Fisher and Paykel Healthcare to present at an industry conference. The other authors have disclosed no conflicts of interest.
Funding Information
The study was sponsored by Fisher & Paykel Healthcare.
Supplementary Material
Supplementary Appendix S1
Supplementary Table S1
References
1.
OsadnikCR, TeeVS, Carson-ChahhoudKV, PicotJ, WedzichaJA, SmithBJ. Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017; 7(7):CD004104.
2.
RochwergB, BrochardL, ElliottMW, et al.; Suhail Raoof Members Of The Task Force. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017; 50(2):1602426.
3.
MunshiL, ManceboJ, BrochardLJ. Noninvasive respiratory support for adults with acute respiratory failure. N Engl J Med. 2022; 387(18):1688–1698.
4.
McDaidC, DuréeKH, GriffinSC, et al. A systematic review of continuous positive airway pressure for obstructive sleep apnoea–hypopnoea syndrome. Sleep Med Rev. 2009; 13(6):427–436.
5.
DavidsonAC, BanhamS, ElliottM, et al.; BTS Standards of Care Committee Member, British Thoracic Society/Intensive Care Society Acute Hypercapnic Respiratory Failure Guideline Development Group, On behalf of the British Thoracic Society Standards of Care Committee. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax. 2016; 71(Suppl 2):ii1–i35.
6.
FodilR, LelloucheF, ManceboJ, et al. Comparison of patient–ventilator interfaces based on their computerized effective dead space. Intensive Care Med. 2011; 37(2):257–262.
7.
SaatciE, MillerDM, StellIM, LeeKC, MoxhamJ. Dynamic dead space in face masks used with noninvasive ventilators: a lung model study. Eur Respir J. 2004; 23(1):129–135.
8.
FraticelliAT, LelloucheF, L'herE, TailléS, ManceboJ, BrochardL. Physiological effects of different interfaces during noninvasive ventilation for acute respiratory failure. Crit Care Med. 2009; 37(3):939–945.
9.
TatkovS, ReesM, GulleyA, van den HeuijLGT, NiliusG. Asymmetrical nasal high flow ventilation improves clearance of CO2 from the anatomical dead space and increases positive airway pressure. J Appl Physiol (1985). 2023; 134(2):365–377.
10.
PinkhamMI, DomanskiU, FrankeK-J, et al. Effect of respiratory rate and size of cannula on pressure and dead-space clearance during nasal high flow in patients with COPD and acute respiratory failure. J Appl Physiol (1985). 2022; 132(2):553–563.
11.
AgustíA, CelliBR, CrinerGJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J. 2023; 61(4):2300239.
12.
GrahamBL, SteenbruggenI, MillerMR, et al. Standardization of Spirometry 2019 Update. An official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019; 200(8):e70–e88.
13.
KendrickKR, BaxiSC, SmithRM. Usefulness of the modified 0–10 Borg scale in assessing the degree of dyspnea in patients with COPD and asthma. J Emerg Nurs. 2000; 26(3):216–222.
14.
WhiteheadAL, JuliousSA, CooperCL, CampbellMJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016; 25(3):1057–1073.
15.
ContalO, VignauxL, CombescureC, PepinJ-L, JollietP, JanssensJ-P. Monitoring of noninvasive ventilation by built-in software of home bilevel ventilators: a bench study. Chest. 2012; 141(2):469–476.
16.
LujánM, LalmoldaC, ErganB. Basic concepts for tidal volume and leakage estimation in non-invasive ventilation. Turk Thorac J. 2019; 20(2):140–146.
17.
CammarotaG, SimonteR, De RobertisE. Comfort during non-invasive ventilation. Front Med (Lausanne). 2022; 9:874250.
CarteauxG, Millán-GuilarteT, De ProstN, et al. Failure of noninvasive ventilation for de novo acute hypoxemic respiratory failure: role of tidal volume. Crit Care Med. 2016; 44(2):282–290.
20.
SiddikiH, KojicicM, LiG, et al. Bedside quantification of dead-space fraction using routine clinical data in patients with acute lung injury: secondary analysis of two prospective trials. Crit Care. 2010; 14(4):R141.
21.
NucktonTJ, AlonsoJA, KalletRH, et al. Pulmonary dead-space fraction as a risk factor for death in the acute respiratory distress syndrome. N Engl J Med. 2002; 346(17):1281–1286.
22.
JayasimhanD, ChiengJ, KolbeJ, SidebothamDA. Dead-space ventilation indices and mortality in acute respiratory distress syndrome: a systematic review and meta-analysis. Crit Care Med. 2023; 51(10):1363–1372.
23.
ConwayA, TiptonE, LiuW-H, et al. Accuracy and precision of transcutaneous carbon dioxide monitoring: a systematic review and meta-analysis. Thorax. 2019; 74(2):157–163.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.