
Abstract
The use of external therapies for knee osteoarthritis (KOA) in traditional Chinese medicine (TCM) is supported by several guidelines and systematic reviews. However, the relative advantages and disadvantages of TCM external therapies and their mechanisms of action have not yet been confirmed in evidence-based medicine. We used network meta-analysis to rank the effectiveness and safety of TCM external therapies, screen the optimal TCM external therapies. TCM external therapies for KOA published before October 2024 were comprehensively retrieved from eight electronic databases. Using the Cochrane Reviewers’ Handbook, two independent reviewers performed study selection, data extraction, and bias assessment of the included randomized controlled trials (RCTs). Data analysis was conducted using Stata 16.0 and RevMan 5.4 software. A total of 68 RCTs were identified, including 6571 participants, involving 11 interventions, 4.41% of which showed a high risk of bias. The results of the network meta-analysis revealed that in terms of improving Visual Analog Scale (VAS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) function scores, each external therapy was better than conventional medicine. Electroacupuncture may be the most effective intervention in improving the VAS score and TNF-α level. Moxibustion resulted in the greatest improvement in WOMAC function and IL-6 levels. The most effective interventions for reducing WOMAC pain scores were the manual needle knife, followed by electroacupuncture and Tuina therapy (SUCRA = 82.9%, 79.0%, and 71.4%, respectively). Warming acupuncture dominantly increased Lysholm scores. The safety results showed that the three safest interventions were the sham intervention, Tuina therapy, and moxibustion (SUCRA = 90.6%, 83.1%, and 68.8%, respectively). Silver needle had the best comprehensive effect. Electroacupuncture has the best effect on improving pain symptoms, and moxibustion can be prioritized when functional limitations are the main symptoms. To some extent, the changes in inflammatory factors correlated with an improvement in KOA symptoms.
Introduction
Knee osteoarthritis (KOA) is a common degenerative disease characterized by pain and activity limitation. 1,2 The pathological characteristics of the disease include secondary bone hyperplasia and cartilage degeneration, which can lead to joint deformity and disability in severe cases and is a common cause of disability in middle-aged and older people. 3 The Osteoarthritis Research International (OARSI) 2020 assessment report 4 showed that there are approximately 240 million patients with KOA worldwide, and the prevalence of KOA is projected to nearly triple by 2025 as the population ages. Epidemiological studies 4,5 have shown that the prevalence of KOA is related to sex and age, with women outnumbering men, with a prevalence of 13.4% in the age group of 50–59 years and 19.5% in the age group of 60–69 years, indicating an aging phenomenon. KOA pathogenesis is complex. Recent studies 6 have found that inflammatory mediators play an important role in the development of KOA and are positively correlated with KOA severity. Inflammatory factors can accelerate the degradation of articular cartilage; induce bone resorption; synergize with chondrocytes to induce peroxidation; stimulate the degradation of proteoglycan, a major component of connective tissue; and aggravate joint pain, cartilage damage, and other symptoms. 7
Nonsteroidal anti-inflammatory drugs (NSAIDs) are recommended for treating early and middle-term KOA. 8 Although these drugs are clinically effective, they are prone to limitations and tend to relapse after discontinuation. Cases of pruritus, sexual dysfunction, and other adverse reactions have also been reported. 9,10 Therefore, alternative treatments for the treatment of KOA have received increasing attention. Concerns regarding the safety and limited efficacy of drug treatments have increased the focus on traditional Chinese medicine (TCM) external therapies. TCM external treatment is a characteristic therapy based on TCM theory, and its treatment of KOA has the advantages of rapid onset, long-lasting efficacy, and high safety, which has gradually become a research hotspot in recent years. 11 Several guidelines and consensuses 12 –14 list TCM external therapies as recommended interventions for the clinical treatment of KOA.
There are many types of TCM external treatments with varying clinical effects. The relative benefits and harms of TCM external therapies remain uncertain, and an optimal treatment strategy has not yet been determined. Although several traditional meta-analyses 15 –17 have demonstrated the advantages of TCM external therapies for KOA, they have not been able to directly compare the efficacy and safety of different TCM external treatments. As the number of alternative treatment options increases, comparative efficacy and safety studies are necessary. In addition, most systematic reviews have focused only on subjective scale changes and have failed to explore changes in inflammatory cytokine levels in patients with KOA treated with TCM external interventions.
Network Meta-Analysis (NMA) enables simultaneous comparisons of multiple therapeutic interventions by synthesizing clinical trial data across treatment groups, effectively addressing the limitation of conventional pairwise meta-analyses. 18 Its fundamental strength lies in constructing evidence networks that integrate both direct comparisons and indirect evidence, thereby bridging evidence gaps from individual studies. This methodology proves particularly valuable in clinical decision-making scenarios requiring optimal intervention selection among multiple alternatives. Notably, NMA enhances decision support through probability rankings that quantify the hierarchy of efficacy and safety across interventions, providing high-level evidence support for clinical guideline development. 19 In contexts characterized by limited healthcare resources and fragmented research data, NMA demonstrates critical value by (1) optimizing evidence utilization efficiency, (2) reducing redundant research costs, and (3) enhancing the credibility and clinical applicability of findings. These advantages collectively establish NMA as a powerful methodological framework for evidence-based medicine, capable of generating synthesized comparative effectiveness assessments while addressing heterogeneity challenges, thereby providing a robust scientific foundation for complex healthcare decision-making.
Therefore, we performed a network meta-analysis to simultaneously analyze direct and indirect evidence from different studies, estimate the relative efficacy and safety of all interventions, and rank the order of interventions. 18,19 This study systematically evaluated the effects of nondrug therapy on the efficacy, safety, and inflammatory factors in patients with KOA, thereby providing a basis for selecting optimal TCM external therapies for the clinical treatment of KOA.
Methods and Materials
Protocol and registration
NMA and systematic reviews were conducted strictly in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-NMA) guidelines. 20 The study protocol was registered with the International Prospective Register of Systematic Reviews (registration number: CRD42023472475).
Inclusion and exclusion criteria
Inclusion criteria: (1) Study type: Only randomized controlled trials (RCTs) not restricted to any language were included. (2) Study participants: Patients diagnosed with KOA based on definitive diagnostic criteria, age, sex, and race were unlimited. 21 –26 (3) Interventions: Treatment groups involved different TCM external therapies alone. Control groups comprised treatments such as conventional medicine (CM), sham interventions (SI), or any TCM external therapies in the treatment group. CMs contain only NSAIDs. (4) Outcome indicators: a. Visual Analog Scale (VAS); b. pain and function scores based on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); c. Lysholm; d. Tumor Necrosis Factor-α (TNF-α) and Interleukin-6 (IL-6); and e. adverse events.
Exclusion criteria: (1) Patients with other inflammatory diseases; (2) repeated publications; (3) more than one therapy; (4) no reference or homemade diagnostic criteria; (5) unavailability of full texts and outcomes; and (6) serious complications.
Literature search strategy
The Cochrane Library, Embase, PubMed, Web of Science, Chinese Biomedical Database (CBM), VIP, Chinese National Knowledge Infrastructure (CNKI), and Wanfang databases were searched for relevant studies. Gray literature was manually searched, and the reference catalogs included in each study and related systematic reviews were consulted. The retrieval strategy used a combination of subject headings and free words. The databases were searched from their inception until October 1, 2024. Each database search strategy is shown in Supplementary Figure S1 and Supplementary Table S1.
Studies screening and data extraction
Two researchers (Miaoxiu Li and J.D.) independently screened studies based on the inclusion criteria. The EndNote software was used to check for duplicates. The investigators screened the titles and abstracts of each study and excluded those that did not meet the inclusion criteria. Subsequently, the investigators read the full text of the remaining studies to decide whether to include them. Disagreements were resolved through consultations with a third party (Y.W.). Two reviewers (Z.W. and Y.Z.) separately extracted data from each eligible RCT using a standardized form. The extracted data included study characteristics (author, country, and publication date), patient characteristics (sample size, disease duration, sex, and age), research site, methodology, intervention measures, treatment course, follow-up, and outcome indicators.
Risk of bias assessment
Two researchers (L.Z. and H.X.) evaluated the risk of bias in the included studies using version 2 of the Bias Risk Assessment Tool (ROB2) in the Cochrane Reviewers Handbook. 27 A third investigator (T.Y.) assisted with resolving differences in assessments between the two researchers. The following six aspects were evaluated to determine the risk of bias: randomization process; deviations from intended interventions; missing outcome data; measurement of the outcome; selection of the reported result; and overall bias. Each study was rated as “low risk,” “high risk,” or “some concerns.”
Data synthesis and analysis
All outcome indicators were analyzed using random- or fixed-effects models based on the level of heterogeneity. P-values of the chi-square test and the I 2 index in the heterogeneity test were used to indicate the level of statistical heterogeneity. 28 When the level of heterogeneity was low, the data were analyzed using the fixed-effects model (p ≥ 0.1 and I 2 < 50%); otherwise, the random-effects model (p < 0.1 or I 2 > 50%) was used. 29 Relative risk (RR) was used as the effect size for dichotomous variables, and standardized mean difference (SMD) was used as the effect size for continuous variables to calculate the 95% confidence interval (CI).
Based on the Bayesian model, Stata software (version 16.0) was used for NMA. The data were preprocessed using the Network Group command, and an evidence network diagram for each indicator was drawn. The curative effects of the indicators were sorted to obtain the surface under the cumulative ranking curve (SUCRA), and probability sorting was plotted. The dots in the evidence network diagram represent an intervention; the larger the area, the greater the number of patients receiving the intervention. The line connecting the two dots indicates a direct comparison between the two interventions, and the thickness of the line represents the number of included studies. 30,31 Surface under the cumulative ranking (SUCRA) was expressed as a percentage. A larger percentage indicates that the intervention has the highest probability of becoming the preferred option, and a value of zero indicates that the intervention may be completely ineffective. 32,33 When a closed loop exists, the node-splitting method is used to check for inconsistencies. When the number of studies on the outcome indicator was >10, a funnel plot was drawn to determine the possibility of a small sample effect. 34
Randomization is a crucial factor for ensuring the quality of RCT research. To ensure robustness of the results, we removed inappropriate and unspecifically described randomization methods and performed sensitivity analyses. Subgroup analyses were performed with different sample sizes and treatment courses. Finally, the quality of the literature was evaluated using the Review Manager 5.4 software.
Results
Study retrieval results
A total of 21,549 articles were retrieved from the initial search, of which 21,446 were from databases and 103 were from other sources. Among the literatures retrieved in the database, 5,550 were from CNKI, 4,338 VIP, 6,114 Wanfang, 4,328 CBM, 193 Embase, 257 Cochrane Library, 425 PubMed, and 261 Web of Science. After primary screening and rescreening, 68 RCTs 35 –102 involving 6571 patients were included. The screening process for the included studies is shown in Figure 1.
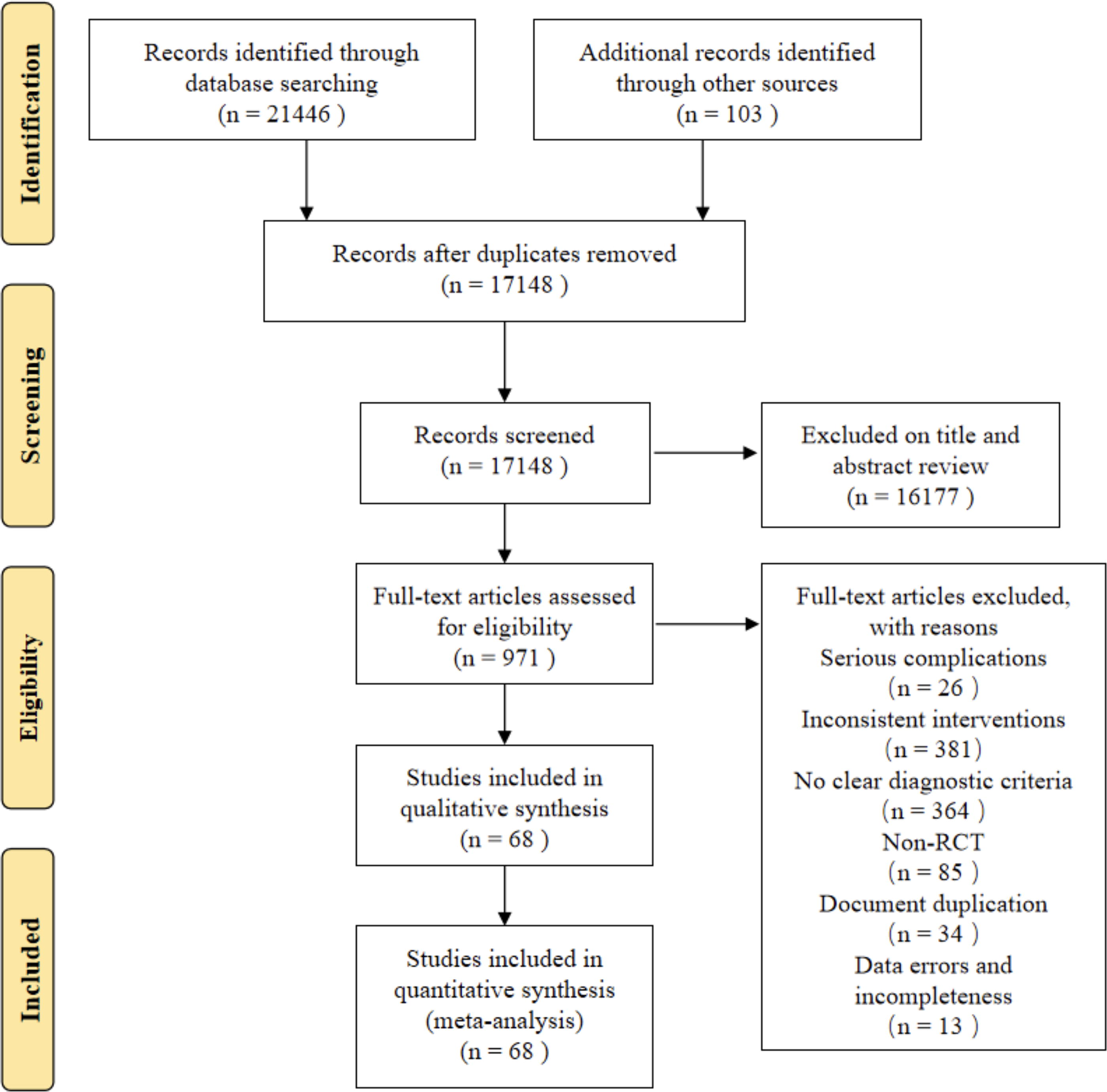
Literature search process.
Basic features of the included studies
Table 1 summarizes the characteristics of 68 RCTs. Among these studies, there were 9 three-arm trials 35,38,39,41,48,50,56,57,63 and 59 double-arm trials. Six studies 51,54 –56,73,80 were multicenter trials, and the rest were single-center studies. The included studies had an average sample size of 97 (range 40–448). A total of 6571 patients (age range: 40–75 years) were included in the study, of whom 40.57% (n = 2666) were men. The studies included nine TCM external therapies in addition to CM and SI, including moxibustion (MB), electroacupuncture (EA), floating acupuncture (FA), fire needle (FN), manual acupuncture (MA), Tuina therapy (TT), warming acupuncture (WA), silver needle (SN), and needle knife (NK). The descriptions of each intervention are presented in Supplementary Table S2.
Characteristics of the Included Studies
C, control; CM, conventional medicine; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; M, months; MA, manual acupuncture; MB, moxibustion; NK, needle knife; NR, not recorded; SI, sham intervention; SN, silver needle; T, treatment; TT, Tuina therapy; WA, warming acupuncture; Y, years; ①VAS, visual analog scale; ②WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index Pain; ③WOMAC Function, ④lysholm, ⑤TNF-α, tumor necrosis factor-alpha; ⑥IL-6, interleukin-6; ⑦adverse reaction.
Risk of bias assessment results
In the evaluation of the risk of bias regarding the randomization process, only 4 studies 39,61,87,100 were evaluated as “high risk”, 5 articles 58,66,81,83,92 were evaluated as having “some concerns”, and 59 articles 35,36,38 –57,60 –65,67 –80,82,84,86 –91,93 –97, 99 –102 were evaluated as “low risk.” In the evaluation of the risk of bias regarding deviations from intended interventions, 17 studies 41,50,57 –59,66 –68,76,77,81,85,87,91,92,94,98 were judged as having “some concerns”, and the remaining 51 articles were considered “low risk.” In the evaluation of the risk of bias regarding missing outcome data, all 68 studies were rated “low risk”. In the evaluation of the risk of bias regarding measurement of the outcome, 9 studies 37,41,60,62,72,78,81,83,95 were judged as having “some concerns”, and the remaining 59 studies were considered “low risk.” In the evaluation of the risk of bias regarding selection bias, all 68 studies were considered “low risk.” According to the ROB2.0 risk of bias assessment tool, 44 studies 35,36,39,40,42 –49,51 –56,61,63 –65,69 –71,73 –75,79,80,82,84,86,88 –90,93,96,97, 99 –102 were rated as having an overall “low risk”, 20 articles 41,50,57,58,60,62,66 –68,72,76 –78,81,83,87,91,92,94,95 were rated as having a risk of bias for a “some concerns”, and 4 articles 37,59,85,98 were rated as having an overall “high risk.” The results are shown in Figure 2, and the risk of bias summary is shown in Supplementary Figure S2.
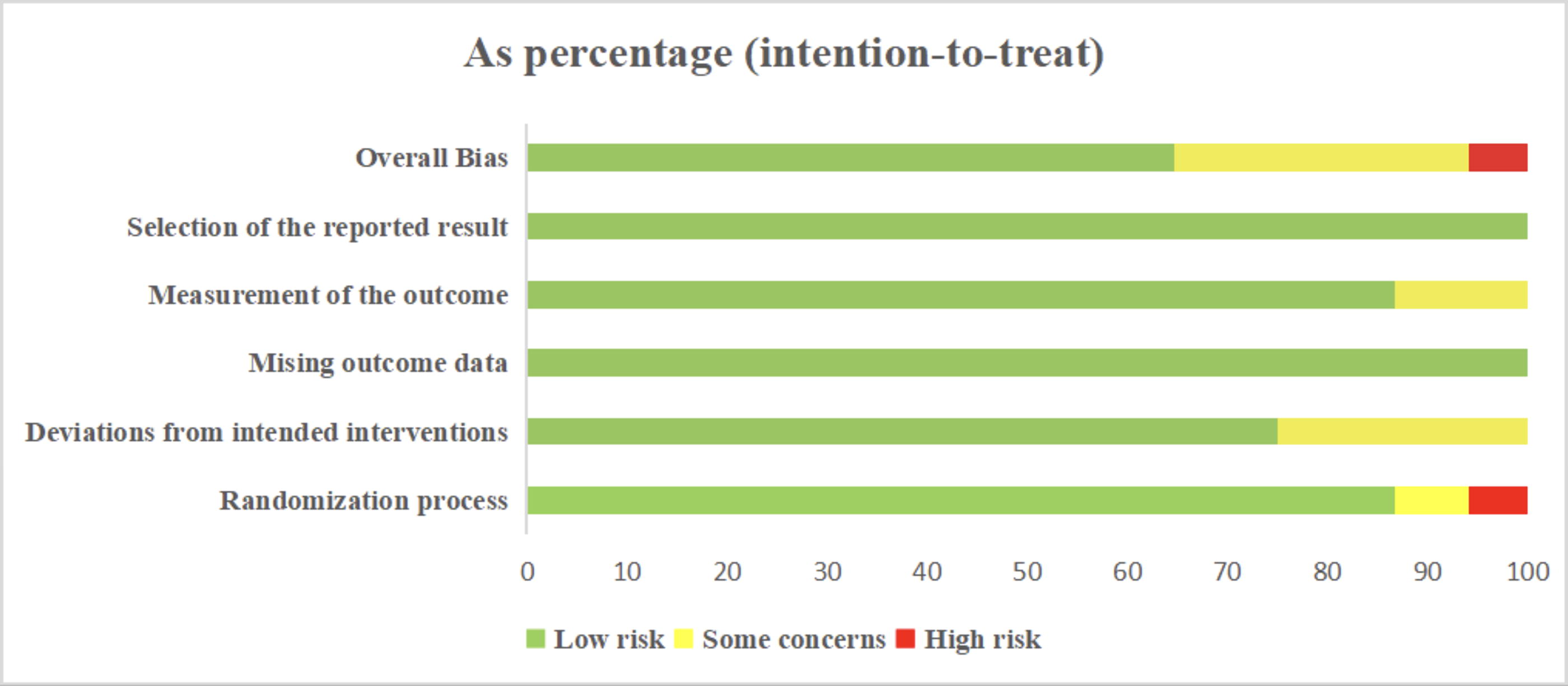
Literature bias evaluation results.
Network meta-analysis
The results of the heterogeneity test showed high heterogeneity for all outcome indicators (p < 0.1, I 2 > 50%). Therefore, a random-effects model was used for all meta-analyses in this study. The evidence network diagrams of all outcome indicators were closed-loop. The node-splitting method showed good consistency, with no heterogeneity emerging between the studies (p > 0.05). The results of the node-splitting tests are listed in Supplementary Tables S3, S4, S5, S6, S7, S8, and S9.
VAS
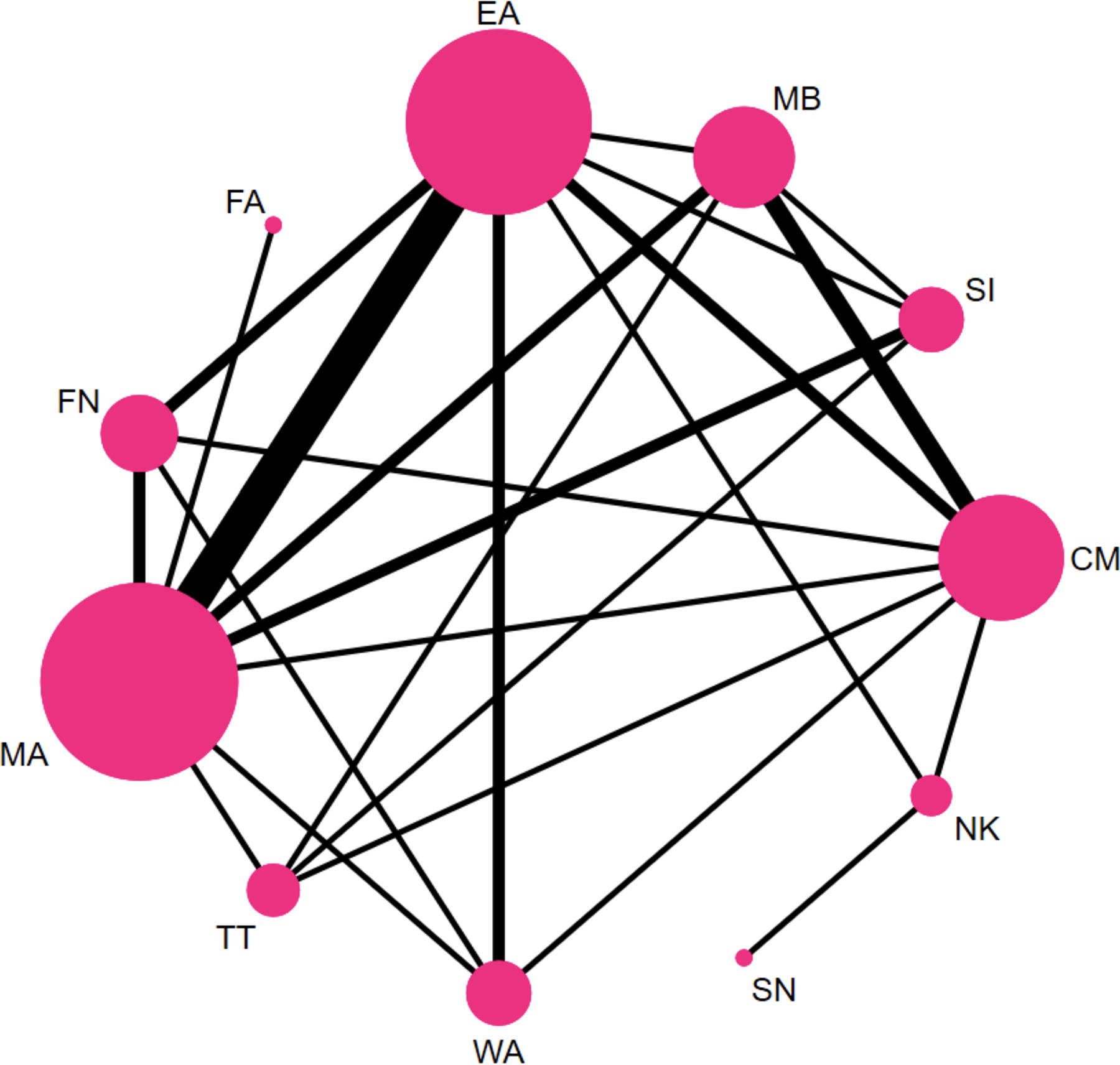
A total of 45 studies 36,38 –40,46 –49,51,53 –55,57 –63,65,66 ,69 –73 , 76 –78,80 –82,86,87,89 –91,93 –96,98,99,101,102 with 4183 participants and 11 interventions reported usable VAS data (Fig. 3). Of them, more participants received CM than other interventions, and studies comparing CM with MB, EA, and MA were the most represented. Further, 55 two-by-two comparisons were performed, resulting in 24 closed loops.
Evidence network diagram of VAS. CM, conventional medicine; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; MA, manual acupuncture; MB, moxibustion; NK, needle knife; SI, sham intervention; SN, silver needle; TT, Tuina therapy; WA, warming acupuncture.
In terms of VAS reduction, all TCM external therapies were superior to CMs (p < 0.05; Fig. 4). We also found that except for WA, MB, and MA, external treatment of TCM had a better effect on the VAS scores than SI (p < 0.05). Furthermore, EA showed better efficacy than WA (SMD = −0.64, 95% CI [−1.25, −0.03]), MB (SMD = −0.85, 95% CI [−1.53, −0.18]), and MA (SMD = −0.96, 95% CI [−1.42, −0.50]) in reducing VAS scores. In addition, MA was less effective than NK or TT (p < 0.05).
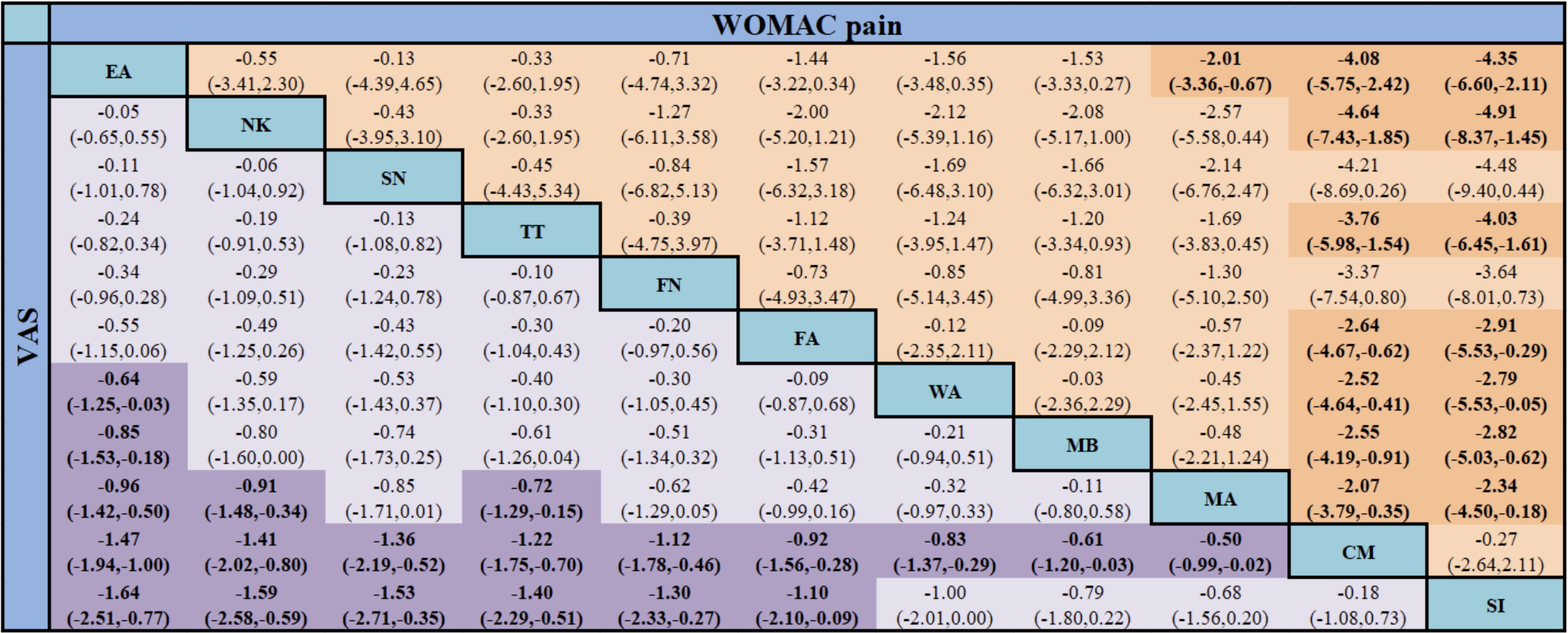
Network meta-analysis of VAS and WOMAC pain [SMD (95% CI)]. CM, conventional medicine; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; MA, manual acupuncture; MB, moxibustion; NK, needle knife; SI, sham intervention; SMD, standardized mean difference; SN, silver needle; TT, Tuina therapy; VAS, visual analog scale; WA, warming acupuncture; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Figure 5 and Table 2 show that of the 11 treatment methods, EA may be the most effective in reducing VAS score (SUCRA = 90.2%), followed by NK (82.6%), SN (76.9%), TT (71.5%), FN (64.2%), FA (50.9%), WA (44.5%), MB (33.4%), MA (26.2%), CM (6.9%), and SI (5.4%).
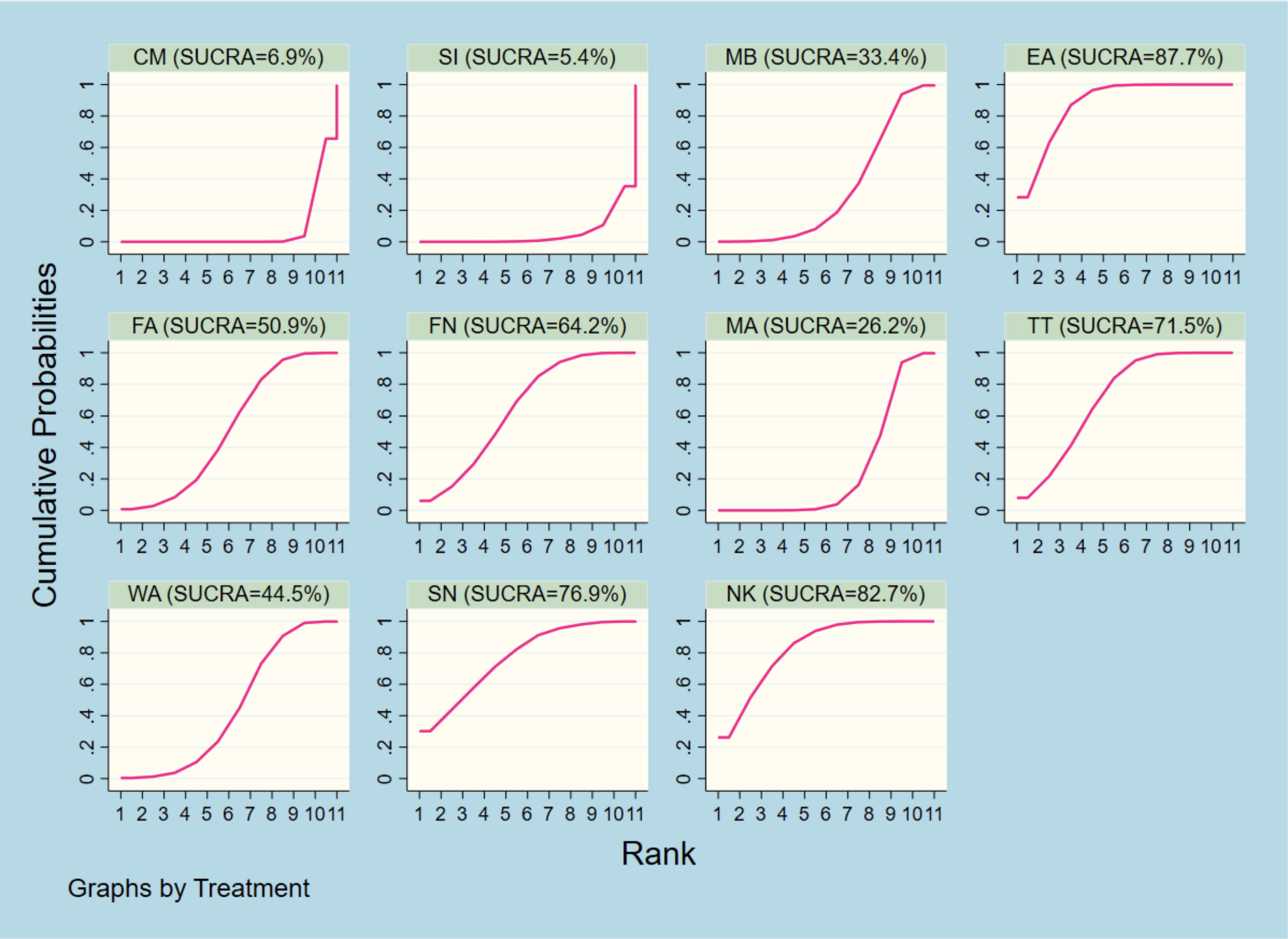
Ranking of SUCRA probabilities for VAS. MB, moxibustion; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; MA, manual acupuncture; TT, Tuina therapy; WA, warming acupuncture; SN, silver needle; NK, needle knife; CM, conventional medicine; SI, sham intervention.
Ranking of SUCRA Probabilities for Each Outcome Indicator
CM, conventional medicine; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; IL-6, interleukin-6; MA, manual acupuncture; MB, moxibustion; NK, needle knife; SI, sham intervention; SN, silver needle; TNF-α, tumor necrosis factor-α; TT, Tuina therapy; VAS, visual analog scale; WA, warming acupuncture; WOMAC, Western Ontario and McMaster Universities osteoarthritis index.
WOMAC pain
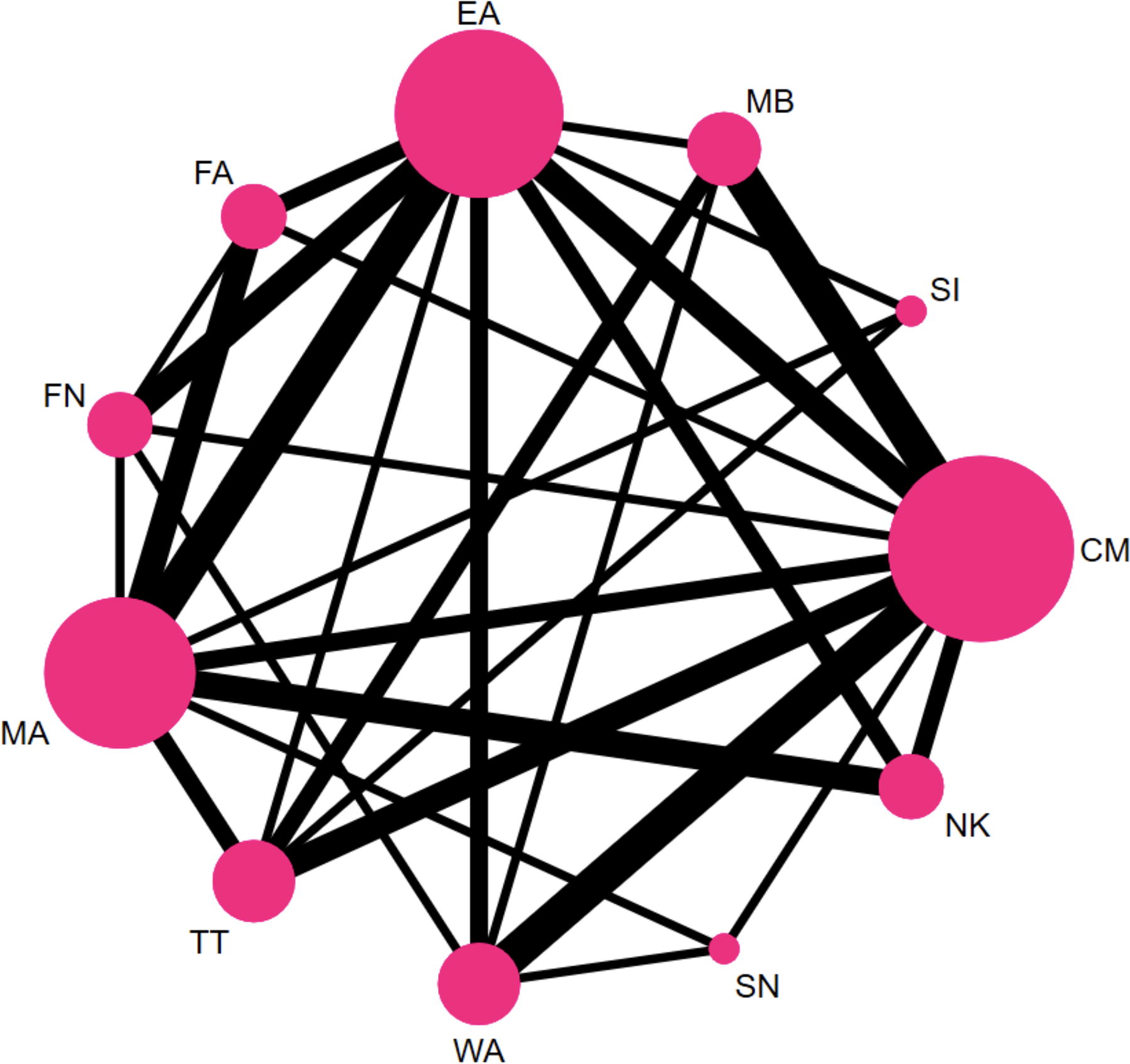
Overall, 29 studies 36,37,40 –42,45 –47,49,50,53,54, 56,61,63 –65,67,69,71,73,74,79,80,84,87,92,96,101 reported WOMAC pain scores, forming 17 closed loops and 55 two-by-two comparisons. There were 11 interventions involving 2860 patients. MA was the most closely linked intervention, and studies comparing EA and MA were the most common (Fig. 6).
Evidence network diagram of WOMAC pain. MB, moxibustion; EA, electroacupuncture; FA, floating acupuncture; FN, fire needle; MA, manual acupuncture; TT, Tuina therapy; WA, warming acupuncture; SN, silver needle; NK, needle knife; CM, conventional medicine; SI, sham intervention.
The results of the NMA showed that compared with CM and SI, all TCM external treatments, except SN and FN, significantly reduced the WOMAC pain scores (p < 0.05). Moreover, EA was a better intervention than MA (SMD = −2.01, 95% CI [−3.36, −0.67]; Fig. 4).
Of the 11 interventions, NK (82.9%) ranked highest in reducing the VAS score, followed by EA (79.0%), TT (71.4%), SN (70.8%), FA (60.6%), FN (47.7%), MB (45.8%), WA (45.0%), MA (34.0%), CM (7.0%), and SI (5.8%) (Table 2).
WOMAC function
Among the KOA population, the network of treatment comparisons for WOMAC function included 30 RCTs 36,37,40 –42,45 –47,49,50,53,54,56,61,63 –65,67,69,71,73,74,79,80,84,87, 92,95,96,101 (two arms, n = 26; three arms, n = 4), 11 interventions, and 2920 patients (Supplementary Fig. S3). Further, 55 two-by-two comparisons were performed, resulting in 17 closed loops. Of them, more participants received MA than other interventions, and studies comparing EA and MA were the most common.
The results showed that, compared with CM, all TCM external treatments and SI significantly reduced the WOMAC function scores (p < 0.05). MB was a superior intervention to EA (SMD = −4.61, 95% CI [−8.58, −0.64]), MA (SMD = −6.11, 95% CI [−9.88, −2.33]), and SI (SMD = −7.49, 95% CI [−12.06, −2.92]). Compared with MA and SI, WA was more effective in decreasing WOMAC function scores (p < 0.05). TT significantly reduced the WOMAC function score compared to SI (p < 0.05) (Supplementary Fig. S8).
In the ranking of conformance model analysis, the best therapeutic method for relieving WOMAC function was MB (81.9%), followed by SN (79.0%), WA (72.6%), TT (68.4%), NK (60.1%), FA (55.4%), FN (54.8%), EA (37.3%), MA (23.5%), SI (16.9%), and CM (0.1%) (Table 2).
Lysholm
For Lysholm, 16 trials 35,36,38,39,42,58,59,66,76,81,85,86,90,93,98,99 (two arms, n = 13; three arms, n = 3) compared 10 different interventions involving 1345 patients. The overall evidence network centered on MA and CM and formed eight closed loops. Further, 45 two-by-two comparisons were made, with most of the comparisons between MB and CM (Supplementary Fig. S4).
Supplementary Figure S8 shows that WA (SMD = 12.84, 95% CI [5.62, 20.06]), MB (SMD = 10.69, 95% CI [4.49, 16.89]), and SN (SMD = 10.72, 95% CI [1.34, 20.10]) were superior to SI in terms of improving Lysholm (p < 0.05). WA and MB significantly increased the Lysholm scores compared to MA (p < 0.05).
The probability ranking conducted with the SUCRA method revealed that WA (83.2%)>MB (72.3%)>SN (70.9%)>FN (57.2%)>TT (56.2%)>NK (55.8%)>FA (38.7%)>EA (30.3%)>MA (24.7%)>CM (10.7%) in improving Lysholm scores (Table 2).
TNF-α
A total of 32 studies 31,35,38,41 –43,45,46,52,58,61 –64,66,72,75 –83,87 –89,91 –94 with 2637 participants and 10 interventions reported usable TNF-α data (Supplementary Fig. S5). Among them, MA was the most closely linked intervention. Forty-five two-by-two comparisons were performed, resulting in ten closed loops. The results of the NMA showed that compared with MA and CM, EA, NK, TT, FN, and WA were more effective at reducing TNF-α levels (p < 0.05) (Supplementary Fig. S9).
The probability ranking results for reducing TNF-α were as follows: EA (85.5%)>NK (78.3%)>TT (65.2%)>FN (63.1%)>SN (54.9%)>WA (48.5%)>MB (46.3%)>FA (36.3%)>MA (14.2%)>CM (7.6%) (Table 2).
IL-6
Overall, 19 studies 37,43,49,53,58,68,70,75,81,83,85 –87,89 –91 ,94,95,100 reported IL-6, forming 5 closed loops and 45 two-by-two comparisons. There were 10 interventions involving 1585 patients. CM was the most closely linked intervention, and studies comparing EA and CM were the most common (Supplementary Fig. S6).
Compared with CM, MB (SMD = −21.09, 95% CI [−36.62, −5.55]) and WA (SMD = −16.58, 95% CI [−26.94, −6.21]) showed a better effect on the IL-6 (p < 0.05). There were no significant differences in most comparisons among the TCM external treatments (p > 0.05) (Supplementary Fig. S9).
MB (79.7%) had the greatest effect on IL-6 reduction, followed by WA (68.2%), SN (65.9%), FN (63.8%), FA (51.1%), TT (50.8%), NK (47.8%), MA (36.3%), EA (29.9%), and CM (6.6%) (Table 2).
Adverse reactions
Of the 68 studies included, 29 reported adverse reactions. Among them, 10 studies 40,42,48,62 ,64,65,69,70,91,95 reported no adverse events and 19 41,44 –46,50 –56,71 –73,80,87,89,92,96,99 reported minor adverse reactions. Due to the limited number of included studies and the broad range of definitions, adverse reactions could not be specifically subdivided, and only the total number of adverse reactions triggered directly by the interventions was analyzed. The specific adverse reactions are detailed in Supplementary Table S10.
A total of 29 studies with 3305 participants and 11 interventions reported usable adverse reaction data (Supplementary Fig. S7). Of them, more participants received MA than other interventions, and studies comparing MA and EA were the most common. Further, 55 two-by-two comparisons were performed, which resulted in 14 closed loops.
The results of the NMA showed that compared with MA and CM, SI, TT, MB, and EA were more effective in reducing adverse reactions (p < 0.05). In addition, SI (RR = −2.01, 95% CI [−3.36, −0.67]) and TT (RR = 0.06, 95% CI [0.01, 0.46]) were safer interventions than NK (RR = 0.08, 95% CI [0.01, 0.94]) (Supplementary Fig. S10).
Of the 11 interventions, SI (90.6%) ranked highest in reducing adverse reactions, followed by TT (83.1%), MB (68.8%), EA (63.6%), SN (57.9%), WA (42.8%), FN (38.7%), FA (36.9%), MA (27.8%), CM (23.0%), and NK (16.7%) (Table 2).
Publication bias
Publication bias was evaluated by examining funnel plots (Supplementary Figs. S11, S12, S13, S14, S15, S16, and S17). The indicators for VAS, WOMAC pain, and TNF-α were asymmetrical in the funnel plots, suggesting a publication bias or small sample effect, which may have affected the results of the corresponding indicators. The funnel plots for the other indicators were symmetrical, suggesting a low possibility of publication bias in the current study.
Sensitivity analysis
Of the 68 studies, 59 35,36,38 –57,60 –65,67 –80,82,84,86 –91,93 –97,99 –102 used the randomization method recommended by the Cochrane Manual, 2 studies 85,98 grouped patients according to different treatment methods, two studies 37,59 grouped patients according to the order of admission, and the other 5 studies 58,66,81,83,92 did not specify a specific randomization method. Considering the importance of randomization in RCT studies, we performed sensitivity analysis by removing studies that were not randomized according to the Cochrane Manual grouping method. Sensitivity analysis was performed for VAS, WOMAC function, and adverse reactions. The results showed that, compared with before the removal of these studies, there was no significant change with regard to the difference in intervention effect and ranking of each intervention in each outcome indicator, indicating that these studies had little impact on the results, and the conclusion of this network meta-analysis was reliable. (Supplementary Figs. S18, S19, and S20 and Supplementary Table S11).
Subgroup analysis
Two subgroup analyses were performed to reduce heterogeneity due to inconsistencies in the sample size and treatment duration. First, the study population was divided into two subgroups based on the sample size (<80 and ≥80 cases). Second, the treatment duration was divided into two subgroups: <4 weeks and ≥4 weeks. In this analysis, NMA was used only for VAS scores.
The NMA results and rankings for the subgroup analyses based on sample size remained consistent with those before subgrouping. In terms of treatment duration, when the course of treatment was less than 4 weeks, NK was the most effective; however, when the course of treatment was greater than or equal to 4 weeks, EA and SN overtook NK in the rankings of 1 and 2. No significant differences were observed in other comparisons. The results of the subgroup analyses are shown in Supplementary Figures S21, S22, S23, and S24 and Supplementary Table S12.
Discussion
External therapies of traditional Chinese medicine have demonstrated growing clinical maturity in treating KOA, gaining increasing patient recognition due to their notable therapeutic advantages including significant efficacy, consistent outcomes, and minimal adverse reactions. These strategies can not only act on the local knee joint, promote blood circulation, release adhesion, increase joint space, adjust biomechanical abnormalities to restore the external balance of the knee joint but also regulate the qi and blood of the viscera, balance the Yin and Yang in the body, and restore the internal balance of the body to improve pain and limited activity symptoms of KOA patients and enhance the quality of life. 103,104 There is no consensus on the use of TCM external therapies for the treatment of KOA. To our knowledge, this is the first NMA to combine multiple TCM external therapies for KOA. This study conducted an NMA to generate a hierarchy of treatment rankings. 105 The ranking probabilities for these treatment plans were calculated in terms of clinical efficacy, safety, and inflammatory factor levels to provide a basis for making optimal choices.
In this NMA, we pooled evidence from 68 studies with 6,571 patients. The 11 interventions were ranked according to the NMA results and SUCRA values. We identified the intervention with a SUCRA value >50% as more likely to reduce symptom severity. In this study, VAS and WOMAC pain were used as pain indicators and WOMAC function and Lysholm score as functional indicators to evaluate the effect of TCM external treatment on the improvement of patients’ symptoms. NMA results showed that each TCM external therapy was superior to CM and SI in improving pain and functional measures. The effects of most interventions that alleviate the burden of pain and functional symptoms are inconsistent. Only the SN ranked highly on both pain and functional measures while being moderately safe, indicating that this intervention was more likely to reduce the overall symptoms in patients than were other interventions. Studies 106 have shown that SN can delay cartilage degeneration and promote functional recovery of the knee joint by improving bone metabolism-related indices such as BGP, BALP, and TRACP-5b. In addition, the better analgesic effect of SN may be because it inhibits IL-1β and TNF-α inflammatory factors and reduces the inflammatory response. 90
However, some treatments are more effective at improving individual symptoms. For VAS and WOMAC pain, EA and NK ranked steadily in the top two. MB and WA may be the most promising methods to improve functional limitations. Considering safety, we found that NK and WA were less safe, whereas EA and MB were better. Therefore, when a patient predominantly suffers from a particular symptom, EA or MB may be chosen as the appropriate treatment. EA may be a better option for improving pain symptoms, the mechanism of which is related to the inhibition of the NLRP3 inflammasome and the reduction of pyroptosis. 107 MB therapy can improve dysfunction effectively. Studies 108,109 have shown that MB may inhibit the abnormal activation of the Caveolin-1/p38 MAPK signaling pathway, thereby regulating the proliferation and survival of chondrocytes and maintaining the balance of extracellular matrix metabolism to slow down the degeneration of articular cartilage.
Abnormal expression and dysregulation of inflammatory factors are important in the pathogenesis of KOA. 110 However, there are many types of inflammatory factors with extensive roles. The specific mechanism of action of each TCM external treatment is unknown. The representative inflammatory cytokines TNF-α and IL-6 are involved in the inflammatory response, apoptosis, and proliferation of chondrocytes and are strongly associated with pain and dysfunction symptoms in patients with KOA. 111 They can play a synergistic role but also restrain each other and jointly maintain the balance of the internal environment of the knee joint. 112 Therefore, we used IL-6 and TNF-α as outcome indicators for statistical analysis. The results indicated that interventions that ranked higher on pain indicators were also more effective in improving TNF-α levels, while interventions that were more effective in improving dysfunction were also ranked higher in reducing IL-6 and were positively correlated to a certain extent. This may be a potential mechanism of TCM external treatments for KOA.
Our quality evaluation of 68 RCTs on TCM external therapies for KOA identified a few RCTs with a high risk of bias (4 out of 68 RCTs). Due to the unique nature of TCM external therapy, establishing a blind method and allocation concealment is difficult. Nevertheless, one-third of the included studies mentioned the use of blinding methods and allocation concealment. Part of the study adopted a multicenter, large-sample design, which improved its credibility. Due to the inclusion of RCT studies that did not include the randomization methods recommended in the Cochrane Manual, the overall quality of this network meta-analysis was reduced, so a careful sensitivity analysis was performed. They suggest that most of the results obtained are robust, strengthening our interpretation of the findings. Subgroup analyses showed no significant differences between the two subgroups for sample sizes of <80 cases versus ≥80 cases. Regarding treatment course, acupotomy has a better immediate effect; however, as the treatment course lengthens, its analgesic effect is surpassed by EA and SN.
Our NMA has few limitations. First, patient sex, choice of operation method, treatment frequency, and other factors may have caused heterogeneity; however, we did not fully examine these factors. In addition, the small sample size of some studies included in our study may help determine heterogeneity, and caution is needed in interpreting the results. Third, owing to the relatively strict inclusion and exclusion criteria, RCTs with intradermal needles, cupping, and stiletto needles were not included; therefore, no statistical analysis of these therapies was conducted. Finally, as some studies only measured symptom scores immediately after the application of the intervention, the long-term effects during different periods after the application of the intervention were not evaluated.
Conclusions
Summarily, most TCM external treatments showed improvements in pain, functional symptoms, and inflammatory factors, with the SN having the best comprehensive effect. EA works best to improve pain symptoms, and MB should be prioritized for KOA treatment in patients with dysfunction as the main symptom. The improvement of KOA symptoms by TCM external intervention may be related to the regulation of inflammatory cytokine levels, in which the regulation of IL-6 improves functional activity and the secretion of TNF-α is strongly associated with pain. However, stronger comparative evidence is required to confirm these conclusions. We recommend conducting more multicenter, large-sample, high-quality RCTs to validate our findings.
Footnotes
Availability of Data and Materials
The original contributions presented in the study are included in the article/Supplementary Data section. Further inquiries can be directed to the corresponding author.
Authors’ Contributions
Z.W. and Y.Z. initiated and designed the study. H.X., Z.W., and C.Z. drafted the article. J.D., M.S., L.Z., Yu Wang, Y.L., and Yiming Wu participated in article revision. Y.B., M.L., and T.Y. were responsible for literature screening and data extraction. All the authors have read and approved the final version of the article.
Author Disclosure Statement
The authors declare that they have no competing interests in this work.
Funding Information
This work was supported by the Henan Province Chinese Medicine Scientific Research Special Project (No. 2024ZY3060, 2024ZY2096), Henan Provincial Special Scientific Research Project for Traditional Chinese Medicine-Joint Construction Program (No. 2025LHZX3008), the Central Plains Thousand Talents Program-Central Plains Famous Doctors (No. ZYQR201912120), the 2022 Central Plains Talent Plan (Talent Education Series)-Central Plains Youth Top Talent Project (No. Yu Talent Office [2022] No. 5), the Henan Provincial International Science and Technology Cooperation Project (No. 252102521021), the Henan Provincial Science and Technology Research and Development Program (Joint Fund Project) (No. 242301420104), Henan Province Key Research and Development and Promotion Special Project (Science and Technology Research) (No. 232102311203), Henan Provincial Science and Technology Research and Development Plan Joint Fund Project (No. 222301420083), Henan Province Traditional Chinese Medicine “Double First-Class” Scientific Research Project (No. HSRP-DFCTCM-2023-7-09) and Henan University of Chinese Medicine Graduate Research Innovation Ability Improvement Plan Project (No. 2023KYCX071).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.