
Abstract
Background:
Gait speed and sleep quality are health indices related to longevity and mortality. In the present study, we measured sleep quality, quality of life, gait speed, and visual acuity before and after cataract surgery to evaluate the efficacy of the procedure on systemic health.
Methods:
The study was conducted on 155 patients (93 women; average age 74.8 years) undergoing cataract surgery with the implantation of a yellow soft acrylic lens. Patients were evaluated using the Pittsburgh Sleep Quality Index (PSQI) and the National Eye Institute Visual Function Questionnaire 25 (VFQ-25; vision-related quality of life) before and then 2 and 7 months after surgery. Four-meter gait speed was also determined.
Results:
Of the 155 patients, 68 (43.9%) were classified as poor sleepers (PSQI>5.5) prior to surgery. Significant improvements were noted in sleep 2 months after surgery (p<0.05, paired t-test), but thereafter the improvements were not significant. Prior to surgery, 117 patients (77.0%) were classified as slow walkers (speed<1.0 meter/s). Gait speed increased significantly in these patients 2 months after surgery (p<0.001, paired t-test). Multiple regression analysis revealed significant correlations between the preoperative VFQ-25 score and both PSQI (p<0.05) and gait speed (p<0.001). Postoperative increases in the VFQ-25 score were positively correlated with decreases in the PSQI (p<0.05). Improvements in visual acuity were correlated with improvements in the VFQ-25 score, but not with either PSQI or gait speed.
Conclusion:
Cataract surgery effectively improves sleep quality and slow gait speed.
Introduction
Cataracts are common in elderly people, and surgery is indicated in the majority of cases. From the social welfare and economic viewpoints, a greater understanding is needed of the health issues affecting cataract patients. In the present study, we explored correlations between systemic health indices and the ophthalmic condition of patients with cataracts. Specifically, we investigated patients' quality of sleep, gait speed, and vision-related QOL before and 2 and 7 months after surgery, as well as undertaking a comprehensive evaluation of the patients' past and present health conditions.
Methods
This study was approved by the local institutional review board, and all patients provided written informed consent prior to participating in the study. Patients underwent a series of medical examinations and were asked to complete specific questionnaires before and 2 and 7 months after cataract surgery.
In total, 155 consecutive patients undergoing unilateral or bilateral cataract surgery were enrolled in the present study. The waiting time for surgery was 1–2 months after diagnosis. In patients undergoing bilateral cataract surgery, the second procedure was performed 3–4 days after the first. The study was done in the Tokyo area, Japan, latitude 35.68 N, where the photoperiod varies from 4 to 6 hr of daylight over the year. The time frame for surgery was from May to December, 2011, and that for follow-up assessment was from November, 2011, to May, 2012.
Patients were asked to complete two validated questionnaires as part of the study: (1) The National Eye Institute Visual Function Questionnaire 25 (VFQ-25; Japanese version 1.4) 7 ; and (2) the Japanese version of the Pittsburgh Sleep Quality Index (PSQI). 8 The VFQ-25 comprises 25 questions regarding vision-related disability in daily life. However, taking into consideration the lifestyle of older Japanese people and specific validation in cataract patients, we used the “compo 7” score in the present study, which excluded questions regarding ocular pain, driving, peripheral vision, and color vision from the original 11 subscales in the VFQ-25. 9 The VFQ-25 does not include questions related to sleep or gait. In contrast, the PSQI is comprised of seven subscales that evaluate sleep quality, including subjective sleep quality, daytime dysfunction, sleep latency, sleep duration, habitual sleep efficacy, sleep disturbances, and the use of sleeping medications. The normal range on the PSQI is <5.5. Both questionnaires were self-administered.
Gait speed was evaluated in patients before and after cataract surgery using a digital stopwatch to time how long it took patients to walk 4 meters. All patients were asked to walk at their usual pace from a standing start with a cane(s) or a walker, as needed.
Additional systemic variables included sex, age, body mass index (BMI), systolic blood pressure, and glycosylated hemoglobin (HbA1c). Information regarding the number of major medical co-morbidities (e.g., diabetes, hypertension, neurological disease, psychological disease, musculoskeletal disease, cardiopulmonary disease, and cancer), including recent hospitalizations, and disabilities in daily life adapted from the 14-item functional health pattern proposed by Gordon 10 (i.e., smoking, chewing/swallowing, excretion, dependency, circulation, hemodialysis, respiration, digestion, cognition, mobility, hearing, sleep, nursing, and family support) was obtained by a registered nurse during face-to-face interviews with patients.
Specialized ophthalmic evaluations were performed by certified orthoptists and board-certified ophthalmologists. Cataracts were diagnosed on the basis of confirmation of microscopic crystalline lens opacity that corresponded to decreased visual acuity. Cataracts were classified as posterior/anterior subcapsular, central cortical opacities in the visual axis, or grade >2 (Emery–Little classification) nuclear sclerosis. For statistical analyses, visual acuity values were converted to the logarithm of the minimum angle of resolution (logMAR). Refractive errors were classified as either hyperopic (either eye≥+3.00D), moderate errors (−2.75D<both eyes<+2.75D), myopic (−5.75D<either eye≤−3.00 D), or highly myopic (either eye≤−6.0D).
The surgical procedures for cataract surgery and intraocular lens insertion consisted of phacoemulsification and aspiration, followed by intracapsular lens fixation of a yellow-colored lens (SN60WF; Alcon Laboratory, Fort worth, TX) under topical anesthesia. All surgeries were performed by an experienced ophthalmologist, and patients with major intra- or post-operative complications were excluded from subsequent analyses.
Where appropriate, data are given as the mean±standard deviation (SD). Data were analyzed using analysis of variance (ANOVA), t-tests, and the Mann–Whitney test, as appropriate. Correlations were evaluated using the Pearson test. All analyses were performed in StatFlex (Atech, Osaka, Japan) and p<0.05 was considered significant.
Results
Patient demographics and health-related characteristics are given in Table 1. All 155 patients (100%) returned for evaluation 2 months after surgery, and 134 patients (86.5%; 60 men, 74 women; average age 75.1 years) completed the questionnaires 7 months after surgery. Two patients died during the follow-up period. Thirteen patients (8.4%) were using a cane or walker prior to surgery, and 1 woman could not walk at all.
Unless indicated otherwise, data are given as the mean±SD.
BMI, Body mass index; HbA1c, glycosylated hemoglobin; SD, standard deviation.
Table 2 lists the results of pre- and post-operative ophthalmic examinations. Posterior/anterior subcapsular cataracts, nuclear cataracts (grade>2), and central cortical cataracts accounted for 42.5%, 18.0%, and 43.8% of cases, respectively. There was a marked improvement in visual acuity and refractive errors after surgery. It is of note that, in Japan, the minimum requirements for a driving license are preoperative visual acuity of 0.19 in the better eye; the visual acuity of most patients in the present study was sufficient for them to undertake daily activities of living.
Unless indicated otherwise, data are given as the mean±SD.
p<0.001 compared with before surgery.
LogMAR, Logarithm of the minimum angle of resolution; SD, standard deviation.
For analyses of postoperative changes, patients were classified into “healthy” (VFQ-25 score≥60; PSQI≤5.5) and “less healthy” (VFQ-25 score<60; PSQI>5.5) groups because the postoperative course obviously depends on a patient's preoperative status (Table 3). In general, most patients in the healthy group maintained their health status after surgery; those in the less healthy group exhibited improvements in all indices 2 months after surgery (Fig. 1). Significant improvements were seen in the VFQ-25 scores 2 months after surgery in both the healthy and less healthy groups. Similarly, significant improvements were seen 2 months after surgery in the sleep quality of patients originally classified as poor sleepers (p<0.05, paired t-test), although improvements thereafter did not reach statistical significance. Furthermore, 9 patients who were originally classified as poor sleepers and who had demonstrated improvements in sleep quality at 2 months exhibited a decline in sleep quality at 7 months, despite no concomitant decline in visual acuity, VFQ-25 score, or gait speed. The mean PSQI for these 9 patients before and 2 and 7 months after surgery was 9.2±2.9, 5.9±2.8, and 9.4±3.4, respectively. The distribution of the time of surgery was from May to December, 2011, and the seasonal maldistribution was unlikely to be a possible cause of unique PSQI change in this group. Analysis of the PSQI subscales for poor sleepers revealed significant improvements in sleep efficacy and sleep duration 2 months after surgery (Table 4). Patients who were classified as good sleepers maintained their sleep quality at 7 months. Mean preoperative gait speed was 0.86±0.21 meter/sec, which increased significantly 2 months after surgery to 0.92±0.21 meter/s (p<0.001, paired t-test). Two patients no longer required a cane to help them walk after surgery.
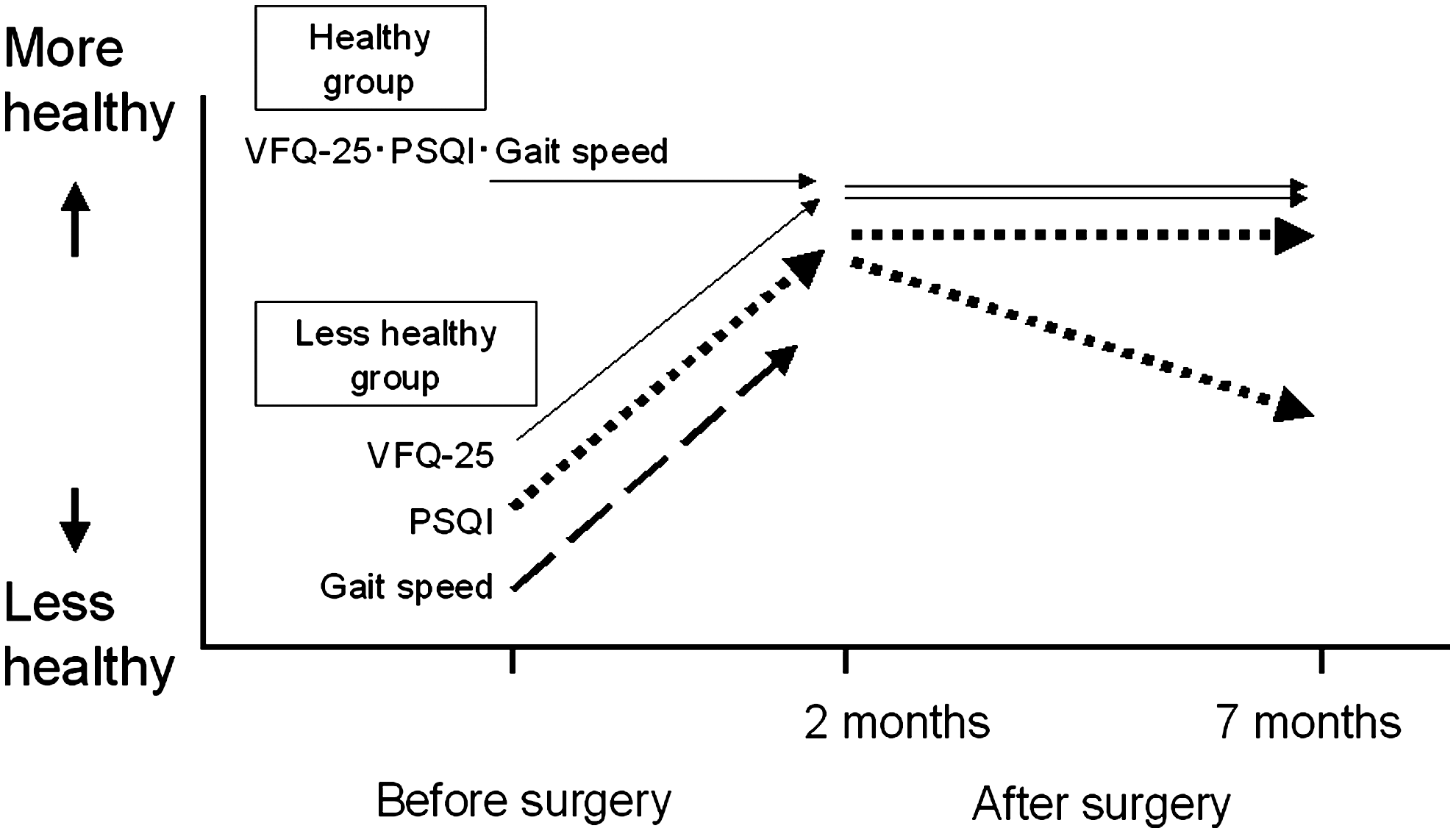
Summary of health indices before and 2 and 7 months after cataract surgery. The “healthy” group (Visual Function Questionnaire 25 [VFQ-25] score≥60; Pittsburgh Sleep Quality Index [PSQI] ≤5.5, gait speed≥1.0 meter/sec) maintained normal values for all indices at all time points. The “less healthy” group (VFQ-25 score<60; PSQI>5.5, gait speed<1.0 meter/sec) exhibited an improvement in all indices 2 months after cataract surgery. Some patients categorized as poor sleepers showed only a transient improvement in sleep disturbance.
Data are given as the mean±SD, with the number of subjects in each group given in parentheses.
p<0.05 compared with before surgery (paired t-test).
Data are given as the mean±SD.
Sleep efficacy (%) was calculated as [sleep duration/(sleep latency + sleep duration)]×100.
p<0.05 compared with before surgery (paired t-test).
SD, Standard deviation.
Prior to surgery, 117 patients (77.0%) were classified as slow walkers (speed<1.0 meter/sec). The speed of most slow walkers improved after surgery compared with that of normal walkers (speed≥1.0 meter/sec), as shown in Fig. 2. There were no significant differences in pre- and post-operative VFQ-25 scores, PSQI, or gait speed between patients undergoing unilateral (n=54) and bilateral (n=101) cataract surgery (data not shown).
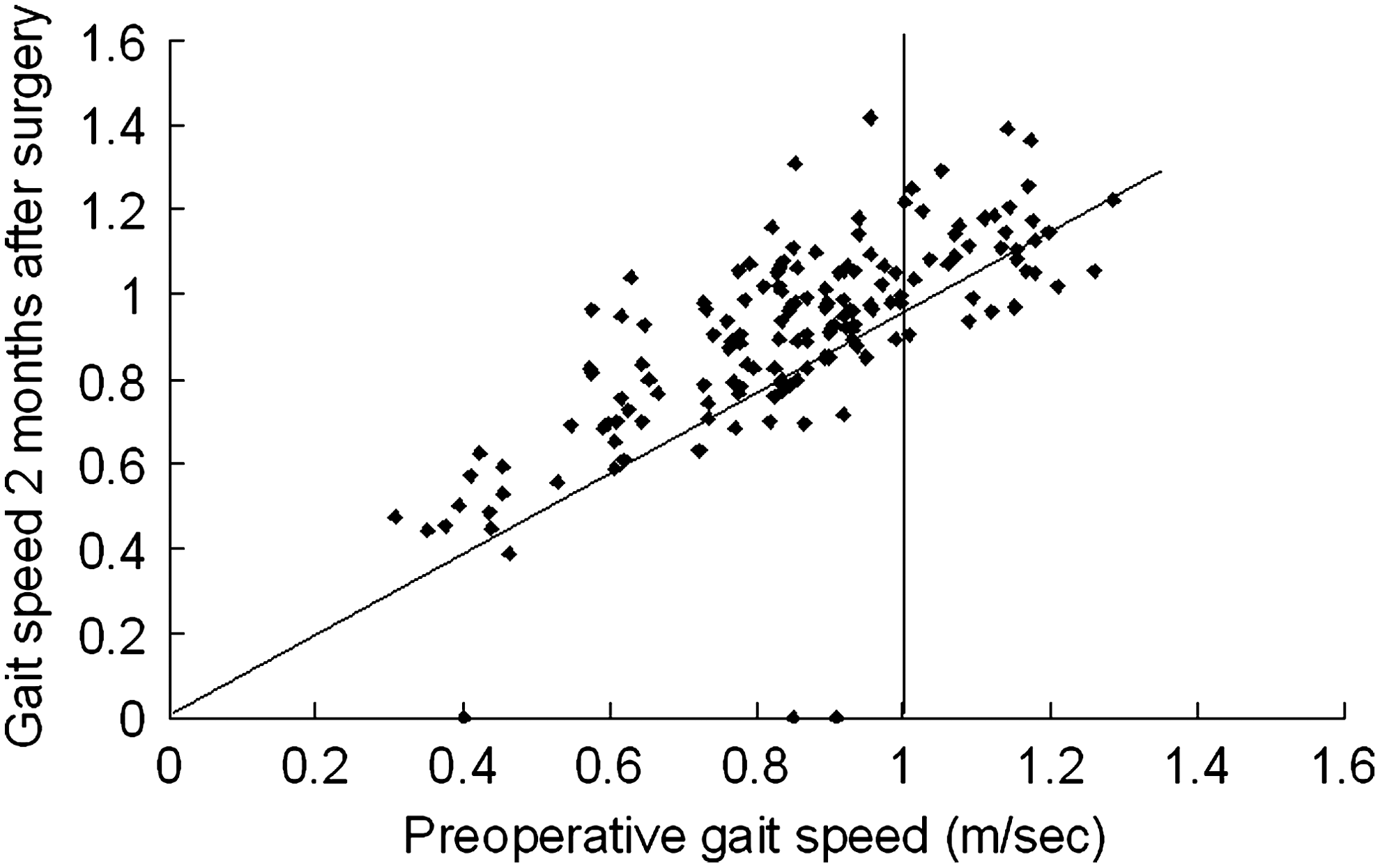
Scatter plot showing pre- vs. post-operative gait speed in cataract patients. The speed of most slow walkers (speed<1.0 meter/sec) improved after surgery compared with that of normal walkers (speed≥1.0 meter/sec).
Results of stepwise multiple regression analyses of preoperative health indices and systemic parameters are given in Table 5. There was a strong correlation between the VFQ-25 score and both PSQI (R=−0.31; p<0.001; Fig. 3A) and gait speed (R=0.36; p<0.001; Fig. 3B). In addition, there was a correlation between VFQ-25 and both sex (male>female) and the sum of logMAR in both eyes. PSQI was correlated with sex (male<female), whereas gait speed was correlated with age, sum of logMAR, and the logMAR of the worse eye.
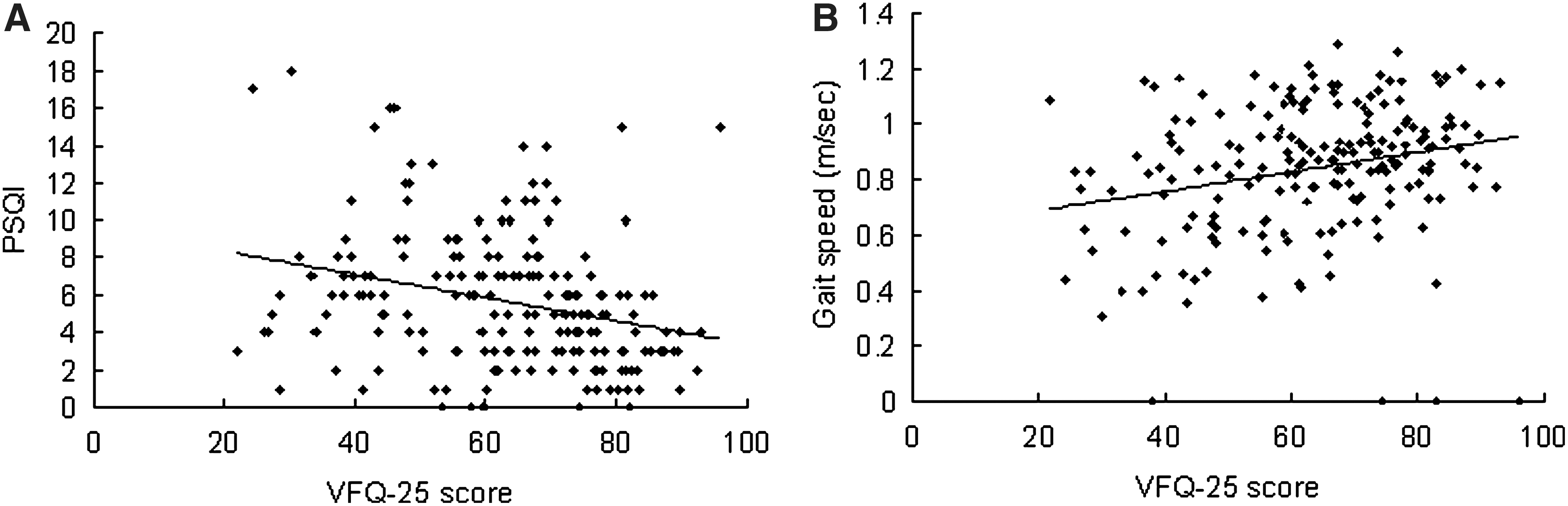
Scatter plots showing correlations between (
p<0.05.
Male=1, female=0, diabetic=1, non-diabetic=0 (adjusted for age and sex).
VFQ-25, Visual Function Questionnaire 25; PSQI, Pittsburgh Sleep Quality Index; BMI, body mass index; SBP, systolic blood pressure; LogMAR, logarithm of the minimum angle of resolution.
Results of stepwise multiple regression analyses of changes in health indices and related parameters are given in Tables 6 and 7. Changes were calculated by subtracting preoperative values from values obtained 2 months after cataract surgery. Correlations were found between ΔVFQ-25 and preoperative sum of logMAR, ΔSum of logMAR, and the presence of posterior subcapsular opacification (β=0.22; p=0.02). ΔPSQI was correlated with preoperative PSQI (p<0.001) and ΔVFQ-25 (p<0.05). There were no correlations found for preoperative PSQI and ΔPSQI or any of the VFQ-25 subscales or ΔVFQ-25, such as mental health (data not shown). ΔGait speed was correlated with preoperative gait speed (p<0.05), BMI, and the number of co-morbidities. There was no correlation between ΔGait speed and ΔlogMAR in the worse eye (data not shown). The ΔSum of logMAR of both eyes was correlated with ΔVFQ-25 and gait speed 2 months after surgery (β=0.16; p=0.03), but not with ΔPSQI or ΔGait speed.
Changes in the health indices and gait speed were calculated by subtracting preoperative values from values 2 months after surgery.
The sum of the logarithm of the minimum angle of resolution (LogMAR) was calculated as the sum of logMAR visual acuity of both eyes in each patient.
All values were adjusted for age and sex.
p<0.05.
Male=1, female=0, diabetic=1, non-diabetic=0.
VFQ-25, Visual Function Questionnaire 25; PSQI, Pittsburgh Sleep Quality Index; BMI, body mass index; SBP, systolic blood pressure.
Changes in the health indices and gait speed were calculated by subtracting preoperative values from values 2 months after surgery.
The sum of the logarithm of the minimum angle of resolution (LogMAR) was calculated as the sum of logMAR visual acuity of both eyes in each patient.
p<0.001.
p<0.05
VFQ-25, Visual Function Questionnaire 25; PSQI, Pittsburgh Sleep Quality Index.
Discussion
The present study is the first to compare pre- and post-operative gait speed and sleep quality in cataract patients combined with precise ophthalmic evaluation. The results indicate significant improvements in both indices after surgery. The strong correlation between these indices of systemic health and the VFQ-25 score highlighted the decreased QOL of cataract patients.
The VFQ-25 has been used extensively to evaluate vision-related QOL. 9,11 The mean VFQ-25 score of the cataract patients in the present series was 63.2, which is comparable to that reported in other studies. 3,5,7 Although a marked improvement was seen in the VFQ-25 score for patients in the less healthy group 2 months after surgery, the VFQ-25 scores in this group remained below normal 7 months after surgery. Similar findings were obtained for sleep quality in the less healthy group. These observations are consistent with visual recovery in the first 2 months after surgery. There may have been other factors, psychological or physical, that prevented further improvement in either the VFQ-25 scores or sleep quality in patients in the less healthy group at 7 months after surgery. Indeed, there has been one study in which a correlation between decreasing VFQ-25 scores and mental problems has been demonstrated for patients with eye disease. 12 Furthermore, Ishii et al. 5 evaluated depressive symptoms and cognitive status in cataract patients and found a correlation between VFQ-25 scores and results on both the Mini-Mental State Examination and Beck depression test before and 2 months after surgery.
Sleep quality is one of the major health indices related to longevity. 13,14 One study has reported a PSQI≥5.5 in 48.7% of subjects with visual acuity <20/200 or a visual field of <5°. 15 In other studies, the prevalence of sleep disorders in visually impaired people has been reported to be 58% 16 and 23%–47%, 17 depending on the sleep disorder scales and definitions of visual disorder used. The induction of sleep disorders due to disruption of the circadian rhythm is common in older people. It has been postulated that cataracts block the light transmittance needed to maintain the circadian rhythm, which may lead to the development of sleep disorders 18 ; thus, cataract surgery is expected to be an effective treatment option. 19 Other factors that may contribute to the disruption of the circadian rhythm in older people include decreased melatonin secretion, decreased physical activity, the use of medications, and the presence of co-morbidities. 20 Depression has been recognized as a major factor contributing to sleep disorders in older adults, 21 and depression in cataract patients may also contribute to the development of sleep disorders. 22 The significant correlation found in the present study between the PSQI and VFQ-25 score indicates that preoperative sleep disorders and postoperative improvements depend on the patient's QOL. Specifically, sleep disorders in elderly cataract patients may be due to worsened QOL, depression, and aging. In the present study, cataract surgery was effective in most patients with a sleep disorder. For those patients categorized as poor sleepers in the present study who only showed transient improvement, the outcomes may be due to personal satisfaction with the surgical results. After the initial lifting of spirits following restoration of their vision and the sensory adaptation to new levels of refraction and light transmission, some patients may have had lower levels of satisfaction at 7 months than others. The dissociation between worsened PSQI and improvements in other indices (e.g., vision, VFQ-25 score, and gait speed) in these cases may be due to a complex interaction of personal factors.
Gait speed has been proposed as a useful clinical indicator of well-being in older adults and has been shown to predict survival. 23 It also appears to be a relevant indicator of physical activity in older cataract patients because reasonable postoperative improvements were observed in the present study that could be evaluated objectively, unlike fall frequency, which has been used in many previous studies. 4 There are numerous methods to measure gait speed in terms of distance, time, speed (fast, usual, slow), and lap time. In the present study, we measured the time taken to walk 4 meters because this is easily measured in a clinical setting and has been standardized by many studies. 23 In a recent review, 23 the adjusted 4-meter gait speed has been reported to range between 0.56 meter/sec and 1.19 meters/sec, depending on the cohort; the results of the present study were within this range. The average gait speed over 10 meters has been reported to be 1.33 meters/sec (4.8 km/hr) in a Japanese rural population. 24 A large cohort study of Japanese people aged ≥75 years revealed that the risk of impaired activities of daily living was significantly higher if gait speed was <1.02 meters/sec in men and <0.87 meter/sec in women. 24 In another prospective cohort study in United States, Cesari et al. 25 reported that the 5-year survival rate was 65%–80% if gait speed was <1.15 meters/sec in men and <0.98 meter/sec in women. On the basis of these reports, we set the gait speed cutoff to 1.0 meter/sec in the present study. Contrast sensitivity and stereopsis rather than visual acuity are associated with physical stability. 4 Older adults with impaired vision because of macular degeneration exhibit low physical performance, including a slow gait speed. 26 The significant correlation between gait speed and visual acuity in our baseline data confirmed that healthy binocular function is important for normal gait. We do not believe that the improvement in gait speed 2 months after cataract surgery is necessarily due to the recovery of visual acuity per se, but may be due to better mental health and general satisfaction following cataract removal. That is, because of better visual recognition, patients may be less fearful of falling and have better confidence. It is unlikely that the musculoskeletal system was strengthened so quickly in the 2 months after surgery, therefore neurosensory improvements and a lifting of the spirits may have contributed to the increase in gait speed. Improvements in stereopsis need to be evaluated further in terms of gait speed.
The significant correlation between VFQ-25 scores and both PSQI and gait speed in cataract patients may indicate that vision-related QOL does affect systemic health. Our hypothesis is that the decreased quality of vision associated with the presence of cataract may lead to depressive symptoms and a fear of falling, resulting in the development of sleep disorders and a decrease in gait speed (Fig. 4A). Patients with cataracts may become anxious and/or irritated after the onset of symptoms and, after their diagnosis, about the need for surgery. Although cataracts do not affect the whole body per se, the well being of patients with cataracts may be compromised because of their condition. Cataract removal followed by implantation of an intraocular lens is an established state-of-the-art procedure in modern clinical ophthalmology. This intervention may improve systemic health indices in addition to visual function (Fig. 4B). Although the precise effects of cataract surgery in preventing falls have not yet been established 27 and the present study has no control, we did find a significant correlation between gait speed and visual acuity, both of which increased after surgery in most patients. We believe that these outcomes could contribute to a longer life expectancy for pseudophakic people.
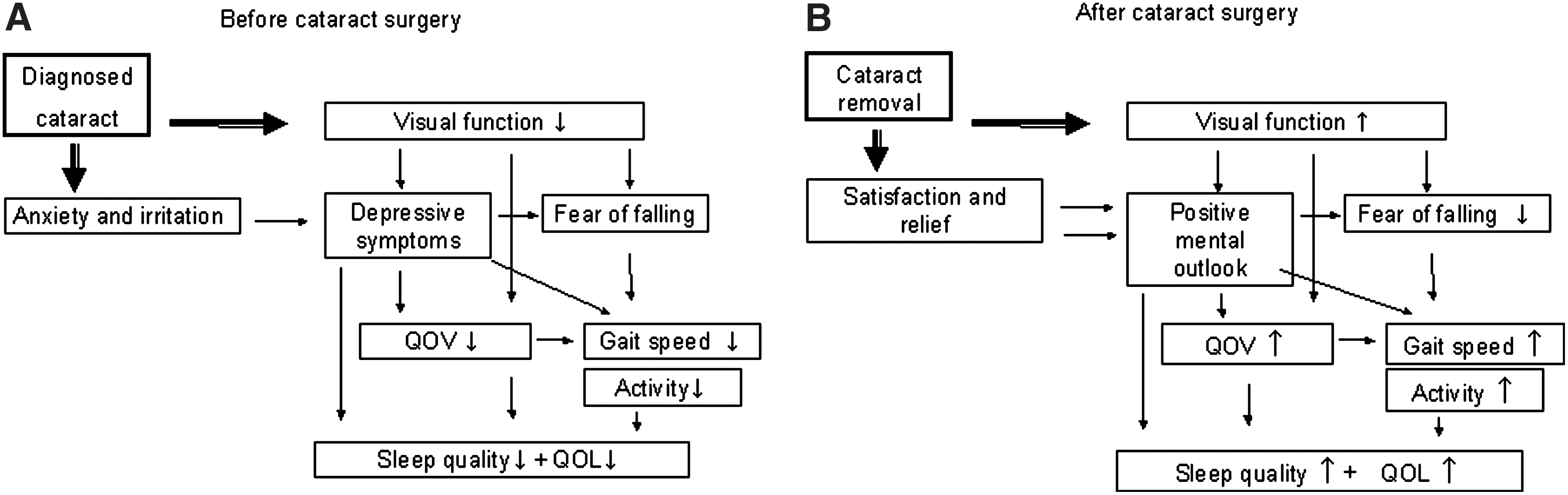
Flow charts outlining the hypotheses for (
Generally, ophthalmologists determine whether cataract surgery is appropriate and the patient's likely prognosis based on the results of ocular examinations and dialogue with the patient. In routine ophthalmic practice, patients are not administered the VFQ-25 or PSQI and gait speed is not measured; thus, it may be difficult to identify certain problems or the specific wishes of some patients. The results of the present study suggest that more attention needs to be paid to the mental and systemic health of cataract patients. Simultaneously, general physicians should consider the potential effects cataracts may have on a patient's systemic health status and sensory systems.
The present study has some limitations. Specifically, the study is a single-center study performed in an urban area using questionnaire-based evaluation. The subjective assessment of sleep quality can vary considerably from objective measures. The results of the present study need to be confirmed in a larger multicenter study, including more laboratory data, activity/illuminance monitor, polysomnography, and indices of physical health. The photoentrained circadian rhythm should also be monitored because it may change as a result of increased light transmission after cataract removal. We did not control daylight exposure, although there are significant variations in seasonal photoperiod over the year in Tokyo and insomnia is closely related to short photoperiod.
In conclusion, significant correlations were found between the quality of vision and both sleep disorders and slow gait speed in cataract patients. Both sleep disorders and gait speed improved after cataract surgery. We aim to further explore the effects of cataract surgery on systemic health in future studies.
Footnotes
Acknowledgments
The authors acknowledge the help of Drs. Yoshihiko Okumura and Saori Inafuku in collecting the data and Drs. Yoshimi Suzukamo and Takayuki Abe for data analysis. The authors acknowledge the assistance of Inter-Biotec (
Author Disclosure Statement
The authors declare no conflicts of interest.