
Abstract
Personal health factors and direct and indirect costs of obesity affect employers and employees. This research aimed to understand perceptions of obesity management and anti-obesity medications (AOMs) among employers and employees. In 2022, people with obesity and employers completed cross-sectional surveys about perceptions of obesity and its management, including AOMs. Data were analyzed with descriptive statistics. Data from 461 employed people with obesity (EwO) and 51 employer representatives (ER) were analyzed. Both EwO and ER acknowledged the impact of obesity on future health problems (88.3%; 100.0%) and perceived obesity as a disease (60.5%; 80.4%) to varied degrees. Both groups perceived an incremental value in combining self-directed lifestyle changes and AOMs (57.5%; 66.7%) and perceived healthcare provider-guided lifestyle change alongside AOMs as the most effective approach for maintaining long-term weight reduction (56.4%; 66.6%). More than two-thirds (68.6%) of ER expressed willingness to revisit their AOM coverage decisions, though cost of medication coverage (72.5%) and affordability of medications for employees (68.7%) were identified as barriers. ER believed that data showing reductions in premiums and claims at their organizations (78.4%) would be helpful in supporting the coverage of AOMs. While EwO and ER were receptive toward AOMs, organization-level barriers existed with AOM coverage. Evidence demonstrating the benefits of evidence-based obesity care, direct/indirect cost reductions, and the impact of obesity may address barriers to AOM coverage and improve obesity care and outcomes of their workforces.
Introduction
Obesity is a chronic disease known to increase risk for cardiovascular disease, diabetes, and cancer, among many other obesity-related complications. 1,2 Obesity often co-occurs with psychiatric diagnoses and mental illnesses, such as depression and anxiety. 3,4 With its increasing prevalence, 5 obesity imposes a considerable economic burden on individuals, employers, and society. Previous research has demonstrated increased outpatient/emergency room and hospital visits among employees with higher body mass index (BMI). 6 In addition to poor health status, obesity and its complications are linked to diminished work productivity, heightened paid sick leave days, and increased risk of occupational injuries. 1,6 –9 Recent research estimates absenteeism and presenteeism associated with obesity cause nearly $250 billion in economic impact and nearly $150 billion in direct medical costs to employers and employees. 10
Given the impact of obesity within the workplace, some employers offer wellness programs to address obesity. 11 Many of these programs are nutrition-focused, with limited scope and effects, failing to broadly address obesity as a multifactorial disease. 12 Because these interventions are positioned as wellness offerings, they typically focus only on lifestyle change, despite evidence showing the majority of individuals who lose weight using lifestyle interventions alone regain their weight over time. 13,14 Due to low participation and lack of effectiveness, 15 recommendations have been made to end or substantially reconfigure lifestyle modification–based employer wellness programs. 16 Meanwhile, employees continue to advocate for obesity care benefits 17 that can effectively address the medical needs of obesity. Together, this highlights an unmet need for employers to provide more effective evidence-based approaches to obesity management in their health benefits offerings.
Advancements in the understanding of the pathophysiology of obesity and the effectiveness of new and emerging anti-obesity medications (AOMs) have fostered a modern era of obesity care. 18 Evidence suggests AOMs are an effective intervention for people with obesity to achieve and maintain clinically meaningful weight reduction when used in tandem with lifestyle interventions. 19 Clinical practice guidelines include AOMs as a recommended option to treat obesity. 20,21 However, insurance coverage of pharmacologic obesity treatments is less available compared to other chronic conditions. 22 , 23 Improved coverage as part of employee health care benefits would address employees’ needs for evidence-based obesity treatment 24 and may also lead to a healthier and more productive workforce. 6,24
Given the substantial health care and societal burden of obesity and rapidly evolving treatment landscape, the present research aimed to understand perceptions of obesity management and the use of AOMs to improve obesity care from both employees and employer representatives (ER) and to identify potential drivers and barriers to AOM coverage among US employers.
Methods
This analysis was part of the larger OBSERVE study (PerceptiOns, Barriers, and OpportunitieS for Anti-obEsity Medications in Obesity CaRe: A SurVEy of Patients, Providers, and Employers), which was sponsored by Eli Lilly and Company. The OBSERVE study included a broad sample of people with obesity who completed an online survey focusing on self-reported attitudes about obesity and its treatment. For this subgroup analysis, survey responses from two groups were included (1) employed people with obesity (EwO) and (2) ER, specifically personnel who make decisions and recommendations about benefits selection and coverage for employees, including human resource (HR) professionals, benefits consultants, and employer coalition representatives. People with obesity were recruited from Kantar Profiles’ LifePoints, which has over 20 million panelists in the US across all four geographic areas: Northeast (14%), Midwest (21%), South (44%), and West (21%). ER were recruited primarily by research recruiters (Ivy Exec) and supplemented by Kantar Profiles’ LifePoints.
All participants completed an online eligibility screener. Prior to survey participation, eligible participants reviewed and agreed to an electronic informed consent form. Study participants received fair market value compensation for their time. Data collection spanned from May to December 2022 for employers and from May to June 2022 for people with obesity. The study protocol was submitted to Sterling Institutional Review Board for review, and it was provided an exempt determination (ID#9434).
Eligibility criteria
ER participants were recruited to represent three groups: HR professionals, benefits consultants, and employer coalition representatives; eligibility criteria were specific to each group. All ER participants were required to have a minimum amount of experience guiding or making health insurance benefit decisions and represent organizations of various sizes (ie, number of employees) and with a mix of insurance plan types (self- or fully insured).
Participating EwO had to be ≥18 years old, meet the Food and Drug Administration (FDA) indications for AOM use, and be employed either full- or part-time. See Supplementary Table S1 for more details on the eligibility criteria by participant type.
Survey content
Participants were asked about their perceptions of obesity and its management, including AOMs. AOMs were referred to as “prescription medications for weight loss” in the people with obesity survey, and “anti-obesity medications” in the employer survey. Weight reduction was referred to as “weight loss” in the people with obesity and employer surveys. In addition, the employer survey included questions on impacts of obesity on costs and productivity, how AOMs fit into employer-provided health plans, and potential drivers and barriers to their use. Survey content was driven by current literature at the time of research design and the findings of exploratory qualitative interviews with patients, healthcare providers (HCPs), and employers regarding drivers and barriers to AOM use utilizing the Sense-Think-Act-Relate behavioral science framework. 25
Statistical analyses
All variables in the study were summarized using descriptive statistics, as the goal of this study was to summarize and describe the data rather than to formally compare or test any differences between the groups. Categorical variables were presented as frequencies and percentages, and continuous variables as mean with standard deviation (SD) or median with minimum and maximum, when appropriate. Results for Likert type five-point scale were reported after combining either the first two or last two scale responses. For example, “Strongly Agree” and “Agree” were combined to represent the percentage of participants that agreed with questionnaire items; “Quite a bit” and “Very much” were combined to represent the degree to which participants believed questionnaire items. The analyses were conducted using R v4.3.0 or higher (R Foundation for Statistical Computing, Vienna, Austria).
Results
Detailed demographics of study participants are available in Table 1. A total of 51 ER (n = 38 HR professionals, n = 9 benefits consultants, and n = 4 employer coalition representatives; collectively referred to as “ER”) completed the surveys. ER types were diverse, with the largest proportion representing blue-collar industries (44.7%).
Participant Demographics
Smaller sample size is due to four employer representatives selecting “prefer not to answer” to the question asking to enter their weight for BMI calculation.
Industry is reported only at the HR level as BC and EC participants were able to select multiple options and so they could not be categorized into one group over another.
The employment status survey item was designed as a 'Select all that apply' question, allowing respondents to choose multiple employment statuses that applied to them simultaneously.
BMI, body mass index; ER, employer representatives; EwO, employed people with obesity; HR, human resource; SD, standard deviation.
Of the OBSERVE people with obesity cohort (n = 1007), a total of 461 were employed. Just over half of this employed subset (ie, EwO) was female (56.4%) and White (50.5%), with a mean (SD) age of 41.9 (±12.9). The mean self-reported BMI (SD) of the EwO sample was 35.1 (±7.3). Most were employed full time (79.2%). Overall, 16.5% reported previously taking prescription AOMs and 5.6% were currently taking prescription AOMs.
Perceptions of obesity
The perspectives of EwO and ER regarding the nature of obesity and how it should be managed are shown in Figure 1. There was consensus among the two groups that obesity increases the risk of future health problems (88.3% and 100%). However, EwO tended to agree less than ER that obesity is a disease (58.4% and 78.5%), is chronic in nature (68.4% and 88.2%), and requires treatment by a HCP (45.2% and 66.7%). EwO viewed obesity as a lifestyle issue, agreeing that obesity is primarily due to poor lifestyle choices (67.1% and 51.0%), people with obesity can generally achieve and maintain a healthy weight if they try hard enough (61.8% and 33.4%), and if maintained long-term, a healthy diet combined with physical activity is all that is necessary to effectively manage obesity (64.0% and 53.0%).
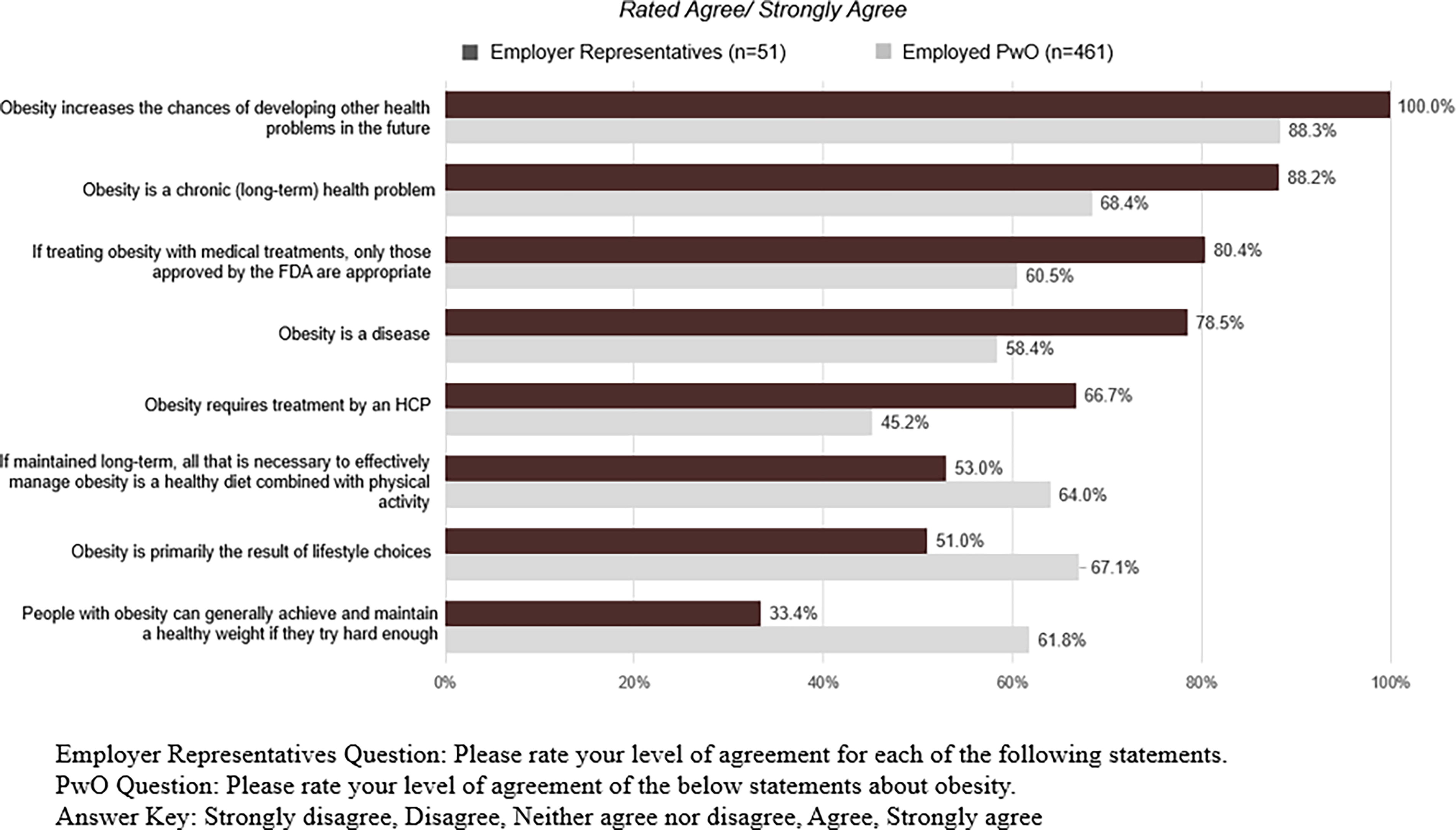
People with obesity and employer representatives’ perceptions of obesity.
Even though over three fourths of ER agreed that obesity is a disease, they perceived that their organizations treated obesity more as a “lifestyle choice” than a “disease” compared to other medical conditions. Only 23.5% of ER perceived that their organizations treat obesity as a disease, compared to 62.8% and 66.6% for type 2 diabetes and high blood pressure, respectively (Fig. 2). Instead, 43.2% of ER reported that their organizations viewed obesity as being a lifestyle choice, compared to 25.5% for type 2 diabetes and 17.7% for high blood pressure.
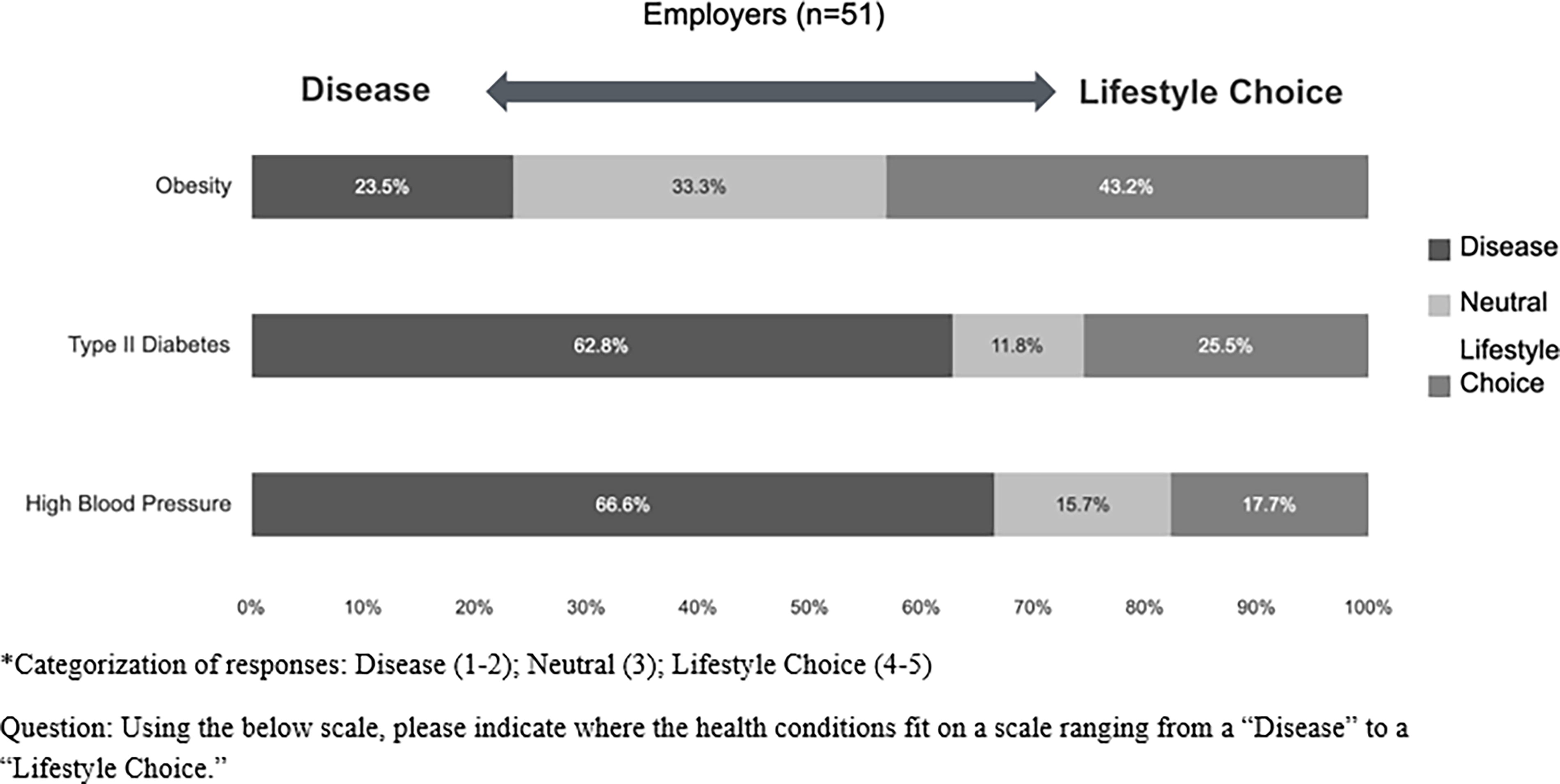
Employer representatives’ perceptions of the organizations’ approach to obesity, type 2 diabetes, and high blood pressure as diseases versus lifestyle choices.
Responsibility for managing obesity
Consistent with reported perceptions that obesity is caused by and can be addressed by lifestyle choices, EwO allocated greater responsibility for managing obesity to the individual with obesity (61.3 out of 100 points) than ER did (47.7 out of 100 points) (Fig. 3). Likewise, EwO tended to assign less responsibility than ER to others for managing obesity, including HCPs (12.6 and 13.7 points), health insurance companies (6.8 and 9.9 points), government/policy makers (4.6 and 6.7 points), and employers (4.2 and 11.2 points).
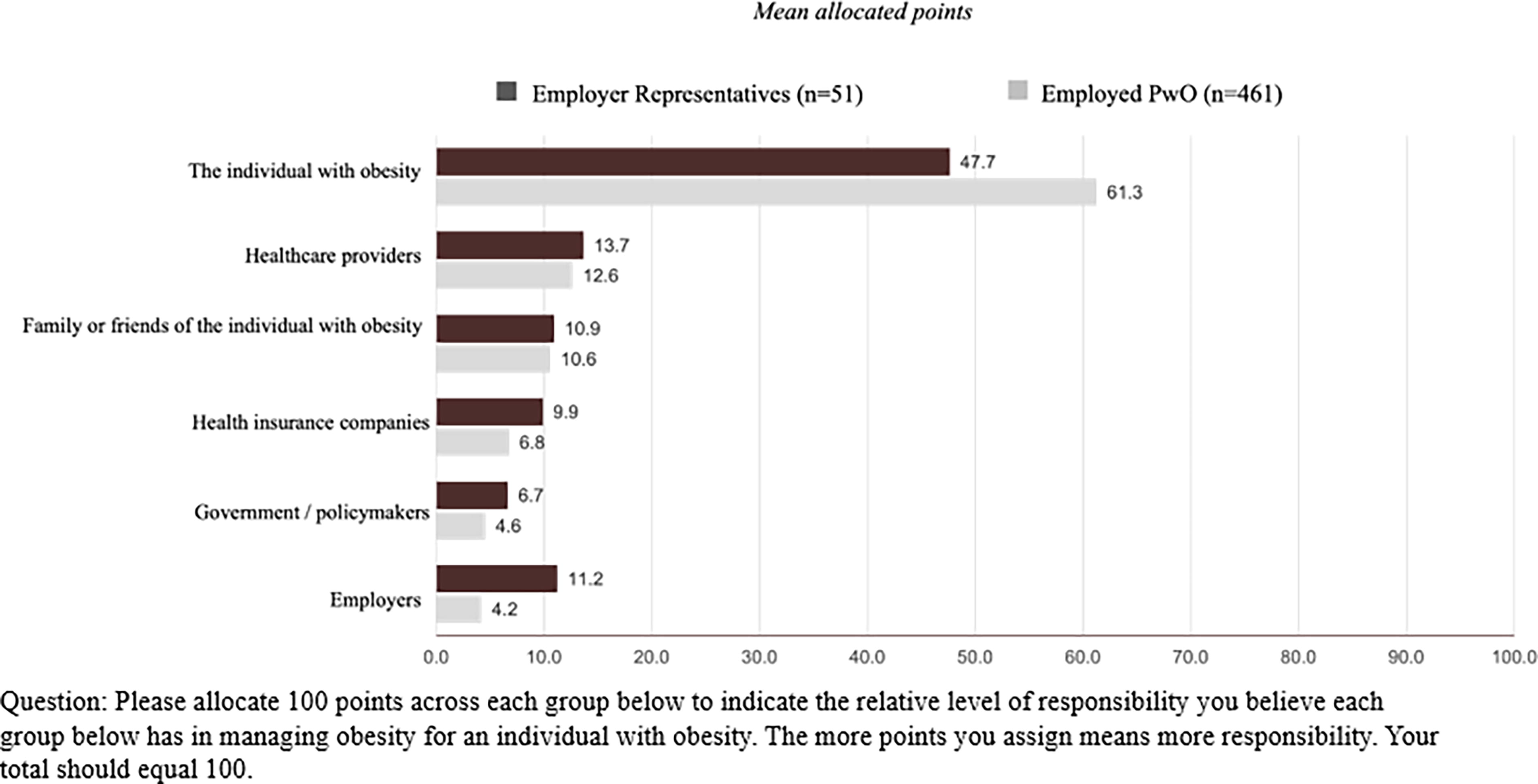
Level of responsibility for managing obesity.
When selecting the condition that had the highest priority to address within one’s organization, ER most often selected anxiety/depression (33.3%), followed by cancer (21.6%), obesity (21.6%), diabetes (19.6%), and high blood pressure (3.9%) (Supplementary Fig. S2). About half of the ER cited an increase in health care expenditures for obesity-related complications (54.9%), evidence of a negative impact on employee health (52.9%), an increase in leaves of absence (51.0%), and evidence of a decreased ability to perform daily work activities (51.0%) as factors that would make obesity a higher priority than it is currently.
Perceptions of obesity treatment strategies
Most ER agreed that AOMs could help employees feel more in control of their weight (92.1%) and improve health-related quality of life (84.4%). ER reported AOMs could be an effective treatment for helping employees with obesity on short-term weight reduction as well as long-term maintenance of weight reduction (80.4%), with almost two-thirds (60.8%) believing AOMs can be used for at least 2 years (Fig. 4). ER reported that AOMs could be most effective if utilized as part of a larger lifestyle program to manage obesity (92.2%) and would complement and significantly improve the obesity management benefits offered by a standard wellness program (84.3%).
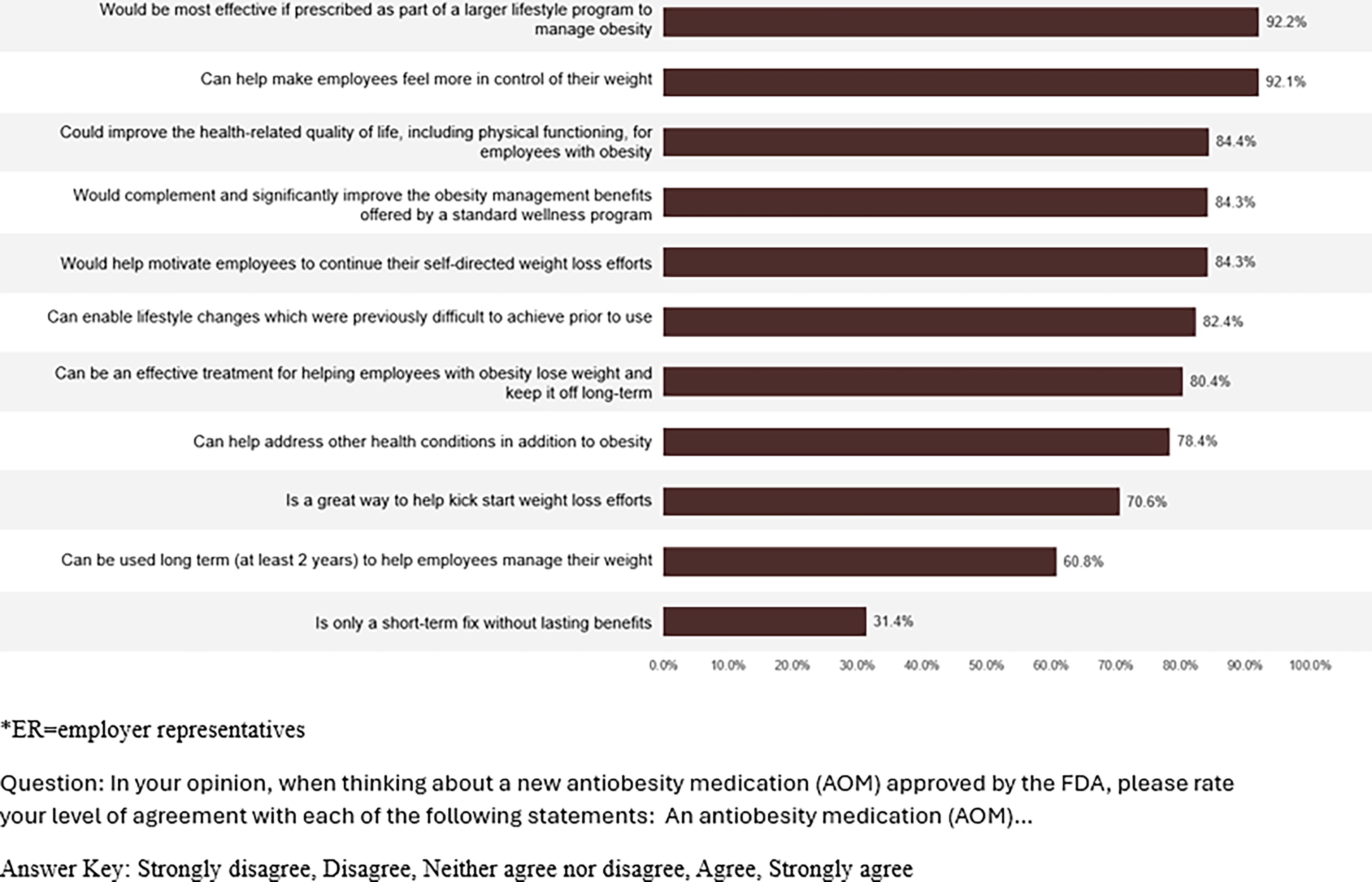
Employer representatives’ beliefs about anti-obesity medications (AOMs) (Agree–Strongly Agree).
EwO and ER regarded lifestyle change guided by an HCP (56.4% and 66.6%) as the most effective approach for keeping weight off over the long term (at least 2 years), followed by self-directed lifestyle change (49.5% and 54.9%), bariatric surgery (30.6% and 31.4%), and AOMs (26.5% and 29.4%) (Supplementary Fig. S3). Both groups perceived that there was an additional incremental value in combining self-directed lifestyle changes and AOMs (57.5% and 66.7%), and ER put more credence in HCP-guided lifestyle changes added to AOMs than EwO (61.2% and 84.3%).
Expectations for the return on investment for coverage of AOMs
Almost all (94.1%) ER agreed that treating obesity more effectively leads to reduced health care costs. The majority (84.3%) of ER agreed that a new-generation AOM approved by the FDA would motivate employees to continue their self-directed weight reduction efforts, would complement and significantly improve the obesity management benefits offered by a standard wellness program (84.3%), and can enable lifestyle changes (82.4%). Over two-thirds (68.6%) of ER were willing to revisit their AOM coverage decisions or recommend coverage for a new-generation AOM.
Two-thirds of ER (66.7%) agreed that their organizations needed further education to understand the return on investment (ROI) of obesity and weight management programs and coverage. When asked to consider the ROI of various weight management modalities, over half (56.9%) of ER believed prescription AOMs had a medium or high ROI, whereas only 19.6% reported that they had low ROI. About a quarter (23.5%) of ER did not know the ROI for prescription AOMs. Regarding wellness programs addressing weight management, nearly two-thirds (64.8%) of ER reported medium or high ROI, with 25.5% reporting low ROI; 9.8% did not know the ROI of these wellness programs (Supplementary Fig. S1).
When asked about potential internal organizational barriers to the acceptance of AOMs for future health plan coverage, ER most often reported “cost of medication coverage for the organization” (72.5%), followed by “affordability of medications for employees” (68.7%) as potential barriers (Fig. 5). “BMI used as a guideline for diagnosing obesity” and “low employee interest” were perceived less as organizational barriers to accepting AOMs (47.0% and 45.1%, respectively).
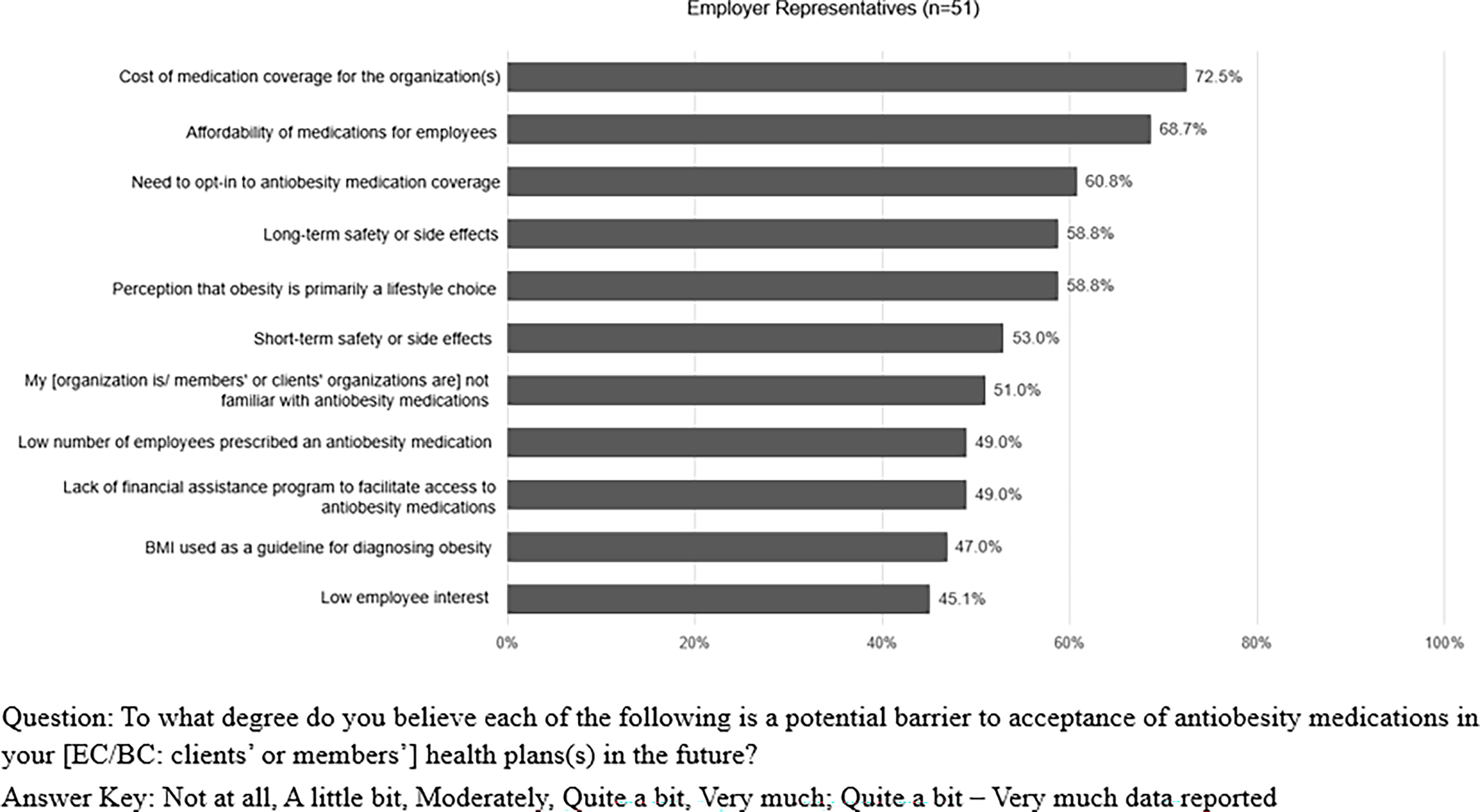
Employer representatives’ perceptions of internal barriers to anti-obesity medication (AOM) acceptance (Quite a bit–Very much).
Furthermore, when asked to consider what would be helpful in supporting the coverage of AOMs within their organizations, ER reported examples of positive ROI due to treatment with AOMs (78.5%), data showing a reduction in premiums and claims at their organization (78.4%), and information about the clinical and financial impact of AOMs from insurance providers (72.6%) as the most helpful data that would support the coverage of AOMs. Under the hypothetical scenario of provision of AOM coverage, two-thirds (64.7%) of ER reported they must have quantified ROI and the ability to finance the costs to continue covering AOMs. In addition, two-thirds (66.7%) of ER reported 1–2 years would be an appropriate time frame to realize a financial ROI.
ER reported challenges to tracking obesity management, such as difficulty in direct tracking of obesity-related claims (74.5%) and lack of documentation of obesity by HCPs (64.7%). Many ER agreed that, if there was a better way to measure and track obesity, ER themselves could better demonstrate the value of AOMs within their organizations (80.4%).
Discussion
Results from the present cross-sectional survey identified perceived drivers and barriers to evidence-based obesity care and AOM acceptance and use among employers and employees. The vast majority of surveyed ER perceived obesity as a disease and accepted AOMs as an effective treatment, perspectives that were not shared as broadly among the EwO sample. ER showed openness to consider a new-generation AOM for coverage if approved by FDA. However, they also identified obstacles within their organization that hindered obesity care, such as the belief that obesity is primarily a result of lifestyle choices, difficulty in monitoring the data related to obesity and ROI of obesity treatment, and the cost of covering AOMs. EwO tended to endorse the idea that if they try hard enough, people with obesity can achieve and maintain a healthy weight. Collectively, these results provide some context for the variable pattern of treatment coverage and support of medical treatment of obesity by employers and limited uptake by employees.
A pattern of agreement was observed between participant groups in their understanding of obesity as a disease. For example, both EwO and ER overwhelmingly acknowledged the negative impact of obesity on employees’ health and life expectancy. Additionally, most ER agreed that obesity impacts employees’ work performance, and that treating obesity reduces an organization’s health care expenditures. Despite this awareness, both EwO and ER perceived that obesity can primarily be treated by lifestyle interventions and assigned the greatest share of responsibility in managing the disease to the individual with obesity. The propensity for people with obesity to self-blame for the cause of the disease may underscore the internalized bias associated with placing onus on the individual for successful obesity management. 21 Not surprisingly, ER and their organizations approached obesity more as a lifestyle choice than as a disease compared to other chronic conditions. Despite the current study finding more ER recognizing obesity as a disease than a previous survey, 15 the findings still highlight the lack of understanding of obesity as a disease attributable to neurobiological processes where gene–environmental interactions drive an individual’s susceptibility to the modern obesogenic environment, as opposed to primarily behavioral or motivational factors. 26,27
The study identified gaps in awareness regarding AOMs for obesity. At the time of the survey, ER were most familiar with the AOM phentermine approved in 1959 only for short-term weight management. 28 Less than one-third of ER were familiar with recent FDA approvals of AOMs, such as semaglutide for chronic treatment of obesity in 2021. Conceivably, their perspective may have evolved since the OBSERVE study data collection (May–December 2022), as more effective treatment options have been approved by FDA, in conjunction with real-world evidence showing clinical and economic benefits of AOM treatment, 29 and increased media attention. A recent survey on the public use and views of GLP-1 drugs from the Kaiser Family Foundation noted the improvement in public awareness of GLP-1 drugs, with about one-third of adults reporting that they have heard “a lot” about these drugs. 30 Also, one in eight adults reported that they have ever used GLP-1 drugs, with one in five who have been told by a doctor that they have overweight or obesity in the past 5 years. 30 Improvement in the public awareness and usage of GLP-1 drugs may have impacted the latest knowledge and perceptions about obesity and AOMs among ER and EwO. Nonetheless, targeted education will assist ER to further understand the efficacy and safety of new and emerging obesity treatment options and how they are recommended to be applied in obesity care.
Study findings showed that ER were knowledgeable in recognizing obesity as a chronic disease. This may be partly due to the education for AOM coverage within the company and various sources of information they may be receiving from external channels, including pharmaceutical companies. Results from a previous study 15 showed that the majority of ER (64%) agreed that obesity is a disease. Even though over three-quarters of surveyed ER perceived obesity as a disease, they admitted that their organizations were more than twice as likely to consider type 2 diabetes or high blood pressure as a disease, compared to obesity, and viewed this perception as a barrier to AOM acceptance. These findings suggest that educational programs for ER and employees may play a role in connecting information about obesity (eg, the biological underpinnings of obesity) and obesity treatment (eg, rationale for multimodal treatment approaches). In addition to traditional education topics, such as behavioral change strategies, addressing the role that implicit bias may have in influencing policy decisions could be informative. Weight-related bias does occur in the workplace and remains more pervasive than other biases that have been targeted by employer-based programs. 31 Therefore, weight bias education could improve not only the workplace environment but also the likelihood of acceptance of evidence-based approaches to obesity management by employees and their employers, although weight-related bias is often excluded from such initiatives. Effective educational programs may help reduce obesity-related biases in health benefits design and empower employees to seek appropriate care support, ultimately leading to improved health and productivity of the workforce.
Participants in both cohorts were receptive toward AOMs and acknowledged their potential to enhance the effectiveness of long-term obesity management, when utilized in combination with lifestyle interventions, especially when guided by health care professionals. With increasing obesity prevalence and ongoing advancement in obesity care, prioritizing employer education about treatment options would support more informed organizational health care decision making. Despite the openness to potential change, the anticipated cost to employers and employees was identified as a barrier.
Notably, nearly all ER agreed that treating obesity more effectively leads to reduced health care costs; however, it was apparent that this perception was not sufficient to address concerns about actual cost savings. Surveyed ER perceived that the resolution of coverage challenges depends on their ability to acquire more robust evidence related to ROI, reduction in premiums or claims, and further evidence of economic benefits of AOMs. Recent study findings showed that adults with employer-sponsored insurance with a weight reduction of 5% were estimated to spend a mean of $670 less on health care, and with a weight reduction of 25% spent an estimated mean of $2849 less on health care, 35 indicating various levels of weight reduction could help reduce health care spending associated with obesity. Furthermore, data on short-term benefits of AOMs such as weight reduction and improvement in cardiometabolic risk factors as well as long-term benefits 36,37 can equip the ER to make informed decisions. Results also revealed a critical gap in tracking obesity-related claims, in conjunction with inadequate documentation of obesity by health care professionals, which complicated AOM coverage decision. Results from this study converge with prior research 32 showing utility in further development of economic data informing employer-based health care coverage on obesity.
To overcome these challenges and to support broader access to obesity care, a comprehensive approach is needed. As a starting point, increased education, and awareness about multimodal evidence-based care approaches, including AOMs, is important to change the narrative around obesity management. The field of obesity medicine is rapidly growing, providing employers with opportunities to engage with obesity care medical experts 33 in developing evidence-based multimodal approaches to obesity care for their employees. Treatment effectiveness and monitoring needs could be proactively met by educating HCPs to utilize obesity diagnosis codes for better tracking of these information within preexisting systems. Moreover, advanced health analytics may be employed to track a broader range of metrics beyond weight reduction, including frequency of emergency room visits, improvements in blood pressure, blood sugar levels, cholesterol, and reductions in medications for related conditions. These broader metrics may serve to quantify the benefits of obesity management programs more effectively. Demonstrating a commitment to employees’ health is known to improve morale, employee satisfaction, and retention. 34 Programs that address obesity can be part of a broader wellness initiative, showing employees that their well-being is valued.
Furthermore, pilot programs including AOMs in health plans may help gather real-world evidence of ROI. Employers may explore innovative ways to cover AOMs, possibly through shared savings models and outcomes-based contracts. Increased employer coverage for AOMs will generate additional data over time illuminating the value of evidence-based obesity care to employees and employers. 29 The current debate of costs and value of new highly effective AOMs is not unique. Recent examples of transformative therapeutic advances that generated controversy, especially regarding the cost of treatments, yet over time led to widespread insurance coverage include highly active antiretroviral therapy for human immunodeficiency virus and direct-acting antivirals for chronic hepatitis C virus. 38 Evolving data will further support treatment access for people with obesity such that obesity is addressed in parity to other chronic diseases.
Strengths and limitations
One strength of the current study lies in the EwO sample by including participants with varied demographic and clinical characteristics. Similarly, the ER sample included HR representatives, as well as benefit consultants and employer coalition representatives. However, this study has limitations. The self-reported nature of the surveys is associated with potential biases, such as inaccurate recall and reporting (whether intentional or unintentional). As inherent with any research relying on convenience sampling methods, it is possible that certain segments of the EwO may be overrepresented, and the results may not be generalizable to employees with obesity in the US. Although the ER sample included people with different titles/positions, the sample size for the ER group as well as the EwO was relatively small, limiting generalizability to US employers more broadly. Additionally, an online self-reported survey likely underrepresents people without access to or comfort with online administration, such as persons with more severe illness or other vulnerable populations. Participants who enroll in research panels and those who agreed to participate may have been systematically different due to selection bias compared to those who do not enroll in research panels, which may limit the generalizability of study results.
Furthermore, the study findings were based on a cross-sectional survey conducted between May and December 2022, after semaglutide 2.4 mg, a highly effective AOM, received FDA approval in 2021. 39 More recently, clinical trial data were reported for tirzepatide, another highly effective AOM, 5,18 which was approved by the FDA. 40 As a result, since data collection, there may have been an increase in awareness of AOMs. The present study findings may not fully reflect current perceptions by employers and employees of the evolving landscape of obesity and its treatment. In addition, this study did not link the EwO to their actual employers, thus any comparisons between the groups are indirect.
Conclusion
Overall, both EwO and ER reported perceptions of obesity as a disease and were receptive toward AOM treatment, especially in conjunction with lifestyle interventions guided by HCPs. Nevertheless, significant gaps remained in understanding evidence-based treatment approaches consistent with understanding obesity as a disease in both EwO and ER. Although ER demonstrated an openness to consider coverage of new AOMs, they reported various barriers at the organization level including understanding of the disease and the ability to track ROI of treatment. Initiatives to address these gaps that reduce bias and stigma, improve employers’ acceptance of evidence-based multimodal approach to obesity management, and further demonstrate the value of such care will be critical to support a healthier and more productive workforce and ultimately lead to employee satisfaction and retention.
Footnotes
Acknowledgments
Medical writing support was provided by Soohyun Hwang, PhD, MPH, an employee of Oracle Life Sciences, with funding from Eli Lilly.
Author Disclosure Statement
J.A. received grants or contracts from Nestle Healthcare Nutrition, Eli Lilly and Company, Boehringer Ingelheim, Epitomee Inc., United Health Group R&D, KVK Tech, WW, and Regeneron; received consulting fees from Nestle Healthcare Nutrition, Eli Lilly and Company, Optum Labs R&D, Novo Nordisk, Intuitive, Regeneron, Brightseed, Level2, WW, Amgen, and Boehringer Ingelheim; served in leadership or fiduciary roles in The Obesity Society and American Society for Nutrition Foundation; and received equipment, materials, drugs, medical writing, gifts, or other services from KVK Tech, WW, and Nestle Healthcare Nutrition. L.M.K. has received consulting fees from Altimmune, Eli Lilly and Company, Novo Nordisk, Amgen, AstraZeneca, Boehringer Ingelheim, Cytoki, Ethicon, Gelesis, Glyscend, Kallyope, Neurogastrx, Optum Health, Perspectum, Pfizer, Sidekick Health, Skye Bioscience, Xeno Biosciences, and Zealand; served on the advisory boards for Eli Lilly and Company and Boehringer Ingelheim. S.K. received consulting fees from Eli Lilly and Company, Novo Nordisk, Vivus, Currax, Boehringer Ingelheim, and Merck, and served in leadership or fiduciary roles for The Obesity Society, Endocrine Society, American Diabetes Association, Obesity Action Coalition, and American College of Preventive Medicine. R.K. served in a leadership or fiduciary role in Found Health. H.K., J.P.D., and T.J.S. are employees of Eli Lilly and Company and received stock or stock options. N.N.A. received stock or stock options from Eli Lilly and Company. K.K.-C., S.D., and A.J. are employees of Oracle Life Sciences. K.G. received all support for the present article (eg, funding, provision of study materials, medical writing, and article processing charges) from Eli Lilly and Company; received grants or contracts from Novo Nordisk; received royalties or licenses from Johns Hopkins ACG System; received payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events from PRI-MED and American College of Cardiology; received support for attending meetings from Eli Lilly and Company, Novo Nordisk, American Board of Obesity Medicine and American College of Cardiology; participated on a Data Safety Monitoring Board or Advisory Board for Eli Lilly and Company and Novo Nordisk; and served in leadership or fiduciary roles in American Board of Obesity Medicine and American Board of Obesity Medicine Foundation.
Funding Information
This work was sponsored by Eli Lilly and Company (Grant No. 2019-8604).
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.