
Abstract
Despite ample evidence supporting their efficacy in atherosclerotic cardiovascular disease (ASCVD) management, statin-prescribing and low-density lipoprotein cholesterol (LDL-C) measurement are underused, especially for vulnerable populations. This study explores the impact of a Best Practices Learning Collaborative to improve the management of patients with ASCVD for secondary prevention. Conducted with the guidance of a subject-matter expert advisory committee, the ASCVD Collaborative convened a geographically diverse group of health care organizations (HCOs) over a 12-month implementation period to set goals, develop and implement interventions, collect and track quality performance measures, and share best practices. Interventions included provider/staff education, clinical decision support tools, care coordination, patient education and awareness, and the treatment of very high-risk patients. HCOs tracked three measures for patients with established ASCVD: any statin prescribed (stratified by sex and race/ethnicity), high-intensity statin prescribed, and LDL-C control (<70 mg/dL). After a 12-month implementation period, HCOs demonstrated improvement in one or more measures. The Collaborative model was shown to be an effective means for achieving improvement in the management of ASCVD, laying the groundwork for future more rigorous studies to identify the most impactful interventions.
Introduction
Over 20 million people in the United States live with chronic coronary disease, which remains the leading cause of death in the nation (despite an approximate 25% overall relative decline in deaths over the past decade) and is associated with significant health and economic burdens. It is estimated that annually 325,000 Americans with coronary heart disease (CHD) will be hospitalized due to a recurrent myocardial infarction or die of a recurrent CHD event. 4
Statin therapy and cholesterol management for the secondary prevention of atherosclerotic cardiovascular disease (ASCVD) is an important area of focus to address the morbidity and mortality associated with this disease. Clinical guidance documents worldwide encourage using and adhering to statin therapy. 5,6 Yet statin treatment is significantly underused in ASCVD care, with prescribing rates ranging from 50.1% to 76.1% for any statin and as low as 22.5%−39.4% for a high-intensity statin.
Disparities exist in statin-prescribing as well. Studies have shown that among patients with ASCVD, Black and Hispanic patients are less likely to be on a statin compared with White patients. 10 In addition, women, who receive suboptimal cardiovascular care overall, are less likely than men to receive high-intensity statins. 8
While statins are well-established agents that lower lipoprotein cholesterol (LDL-C), a primary cause of atherosclerotic disease, 5 a variety of nonstatin treatment options have emerged for LDL-C control, for example, ezetimibe, PCSK9 mAbs, bempedoic acid, and inclisiran. 11
Regardless of therapy type, lipid monitoring is essential to assess individual response and monitor adherence and persistence over time. 12 Yet LDL-C was removed from American College of Cardiology (ACC)/American Heart Association (AHA) guidelines in 2013. A 2019 study showed over half of patients with high cardiovascular risk lacked lipid laboratory measurements in their electronic health record (EHR) as this new guidance came into practice. The National Lipid Association and the American Society for Preventive Cardiology stressed the importance of reestablishing LDL-C measurement as a performance measure for high-risk groups. 13,14
To address these shortcomings in prescribing statins and other therapies and monitoring and managing cholesterol, AMGA (American Medical Group Association), a nonprofit trade association whose membership comprises over 400 health care organizations (HCOs), launched the ASCVD Best Practices Learning Collaborative (Collaborative) in September 2022.
The Collaborative offered AMGA member organizations an opportunity to participate in an intensive shared-learning program. Participants were provided resources to improve the overall care of their population of patients with established ASCVD within multispecialty groups and integrated delivery systems in both primary care and outpatient cardiology clinical settings. The study’s purpose was to understand and describe the quality improvement activities of the 12 participating HCOs and assess improvements in selected Collaborative clinical measures over 12 months.
Methods
A learning collaborative approach was applied to develop and test interventions designed to improve management and care for patients with established ASCVD over a 12-month period. Best Practices Learning Collaboratives are shared-learning programs designed specifically for HCOs striving to improve the care of patients with chronic conditions, prevention efforts for these illnesses, and organizational performance. This quality improvement initiative collected quantitative and qualitative data during the study period. All Collaborative activities were guided by the 2018 AHA/ACC Guideline on Managing Blood Cholesterol. 6
National advisory committee
An external advisory committee, comprised of physicians experienced in the management of ASCVD and comorbid conditions, evidence-based interventions, and population health was created to guide the development and execution of the Collaborative, including the selection of HCOs for participation in the Collaborative.
Participating HCOs
AMGA Foundation distributed a call for participation brochure to all AMGA members via email, with an invitation to apply. Requirements to participate in the Collaborative included the ability to extract Collaborative clinical measures from their organizations’ EHR, report data, and quality improvement documentation quarterly, and participate in Collaborative webinars, in-person and virtual meetings, and other program activities.
Twelve HCOs were selected to participate. These HCOs spanned 12 states representing all regions of the United States (West, Northeast, South, Midwest), with over 4000 providers engaged. The HCOs, located in urban and rural areas, serve patients with diverse demographics and characteristics (see Table 1). The Collaborative cohort initially included 15 HCOs. Two HCOs dropped out of the Collaborative early due to resource limitations or reprioritization. The third HCO was unable to successfully report data until the end of the intervention period and was therefore excluded from the analysis due to potential data noncomparability.
Participating Health Care Organizations
Best Practices Learning Collaborative activities
Collaborative activities included sharing best practices, education, goal setting, and peer-to-peer learning, facilitated by a virtual discussion forum, two in-person meetings, regular webinars, site visits, coaching, and sharing of benchmarked measure outcomes. Quality improvement documents were completed by each HCO at the start of the Collaborative and updated quarterly. These plans detailed objectives and interventions, progress toward goals, and lessons learned. Qualitative information on successful interventions was shared with the Collaborative through quarterly presentations. Quantitative data were collated and provided to Collaborative participants in quarterly progress and benchmarking reports. Participating HCOs each received a stipend of $10,000 to help partially offset the cost of implementing the Collaborative.
Qualitative data
Using the Framework for Developing and Evaluating Complex Interventions 6 (including motivating needs, objectives, and interventions) and a population health approach, participants used the priority areas they identified early in the Collaborative to inform their intervention development and implementation.
The participating HCOs began by ranking a list of seven motivating needs associated with ASCVD management, in order of importance (1 being the most important): Lack of patient awareness and education about secondary prevention of ASCVD. Lack of affordable treatment for patients with very high-risk ASCVD who are not responding to statins. Lack of care coordination for patients with ASCVD. Disparities in care for patients with ASCVD. Lack of adequate treatment of very high-risk patients with ASCVD. Knowledge deficit (among providers/staff) about patients’ need for secondary ASCVD prevention. Inadequate clinical decision support tools.
HCOs worked to develop objectives or strategies to address at least three selected motivating needs (one of which addressed a health disparity) and created interventions to close associated care gaps.
HCOs initially submitted a gap analysis, plan-do-study-act cycle, action plan, and an identified health equity gap and plan to address it. HCOs updated the action plan and health equity documentation quarterly. Health equity was an important component of the quality improvement process. HCOs stratified the statin-prescribing measure by various patient characteristics in order to identify potential disparities in vulnerable populations.
Each HCO then selected one vulnerable population and created a tailored intervention to address gaps in care. Participating HCOs selected interventions for implementation based on the unique characteristics of their organization. The Collaborative 12-month implementation period started with seven motivating needs and resulted in 63 unique planned interventions across 12 participating HCOs. Site visits provided a forum for an extensive review of the HCOs’ qualitative improvement processes, program development, and data performance. In addition, the AMGA team provided insights and shared other HCOs’ successful strategies for addressing challenges.
Quantitative data and analysis
AMGA, together with the National Advisory Committee, developed quality performance measures to support Collaborative goals. Measure development was guided by the 2018 AHA/ACC Guideline on Managing Blood Cholesterol 6 and the National Committee for Quality Assurance Healthcare Effectiveness Data and Information Set (HEDIS)® 2022 Effectiveness of Care Measure: Statin Therapy for Patients with Cardiovascular Disease (SPC).
Participants reported ASCVD prevalence each reporting quarter. Additionally, among patients with ASCVD, three measures were tracked quarterly: Any statin prescribed (stratified by sex and race/ethnicity). High-intensity statin prescribed. LDL-C <70 mg/dL (LDL control).
Eligibility criteria for the measure denominators included patients aged 40–75 with a diagnosis of ASCVD (see Supplementary Data, Identification of ASCVD) who had two or more ambulatory outpatient visits during the specified 12-month measurement period or in the prior six months (at least one of those with a primary care provider). Patients with evidence of pregnancy, IVF, clomiphene prescriptions, ESRD, dialysis, cirrhosis, hospice or palliative care, or death were excluded.
Numerator compliance for all measures was based on data from the most recent 12-month measurement period. LDL-C control was determined by a patient’s last LDL-C measure in the measurement period. Numerator noncompliance could be due to the lack of LDL-C measurement in the 12-month period or last LDL-C in the measurement period ≥70 mg/dL.
HCOs were provided with detailed measure specifications and a reporting template to submit data via a secure data repository. Aggregate numerators and denominators were reported by HCOs. Data were submitted for baseline, the 12-month period ending with Q4 2022 (January 1, 2022−December 31, 2022), and throughout the intervention period (i.e., a rolling 12-month period each quarter) ending with Q4 2023 (January 1, 2023−December 31, 2023). Data were then reviewed and validated, and errors and inconsistencies were addressed with the HCOs.
The reporting template included several auto-populated graphs and charts to assist organizations with data quality/integrity review and tracking their progress throughout the intervention period.
Analysis
Measure data were reported quarterly, including one baseline and four intervention quarters. Benchmark reports, which included all measures, were prepared quarterly and shared unblinded with all participating HCOs. Using a two-sample z-test, the baseline quarter was compared with the final reported quarter (follow-up) for each HCO and for all HCO patients combined, to calculate P values for two-tailed comparison with alpha set at 0.10 for a 90% level of confidence due to small individual HCO sample sizes. Reported improvements reflect positive changes in rates from baseline (Q4 2022) to Q4 2023 that were either statistically significant or considered to be clinically relevant (defined as a change of ≥1 percentage point).
Results
The Collaborative cohort included 115,970 patients with ASCVD, a prevalence of 20.4% (range: 9.5%–25.6%). Statin-prescribing rates were high at baseline and remained high through the intervention period, with 79.4% (range: 70.1%−85.3%) and 79.2% (range: 70.0%−86.4%) prescribing rates at baseline and follow-up, respectively (P = 0.13). High-intensity statin prescribing increased from 45.3% at baseline to 46.7% at follow-up (P < 0.0001). LDL-C control (<70 mg/dL) improved from 27.2% to 28.2% for all patients with ASCVD. LDL-C control also improved by statin use, with increases 32.0%−33.2% for patients on any statin and 36.6%−38.2% for patients on high-intensity statin (all P < 0.0001) (see Fig. 1, Supplementary Tables S1, S2 and S3 in the supplemental materials for change by measure and by HCO.)
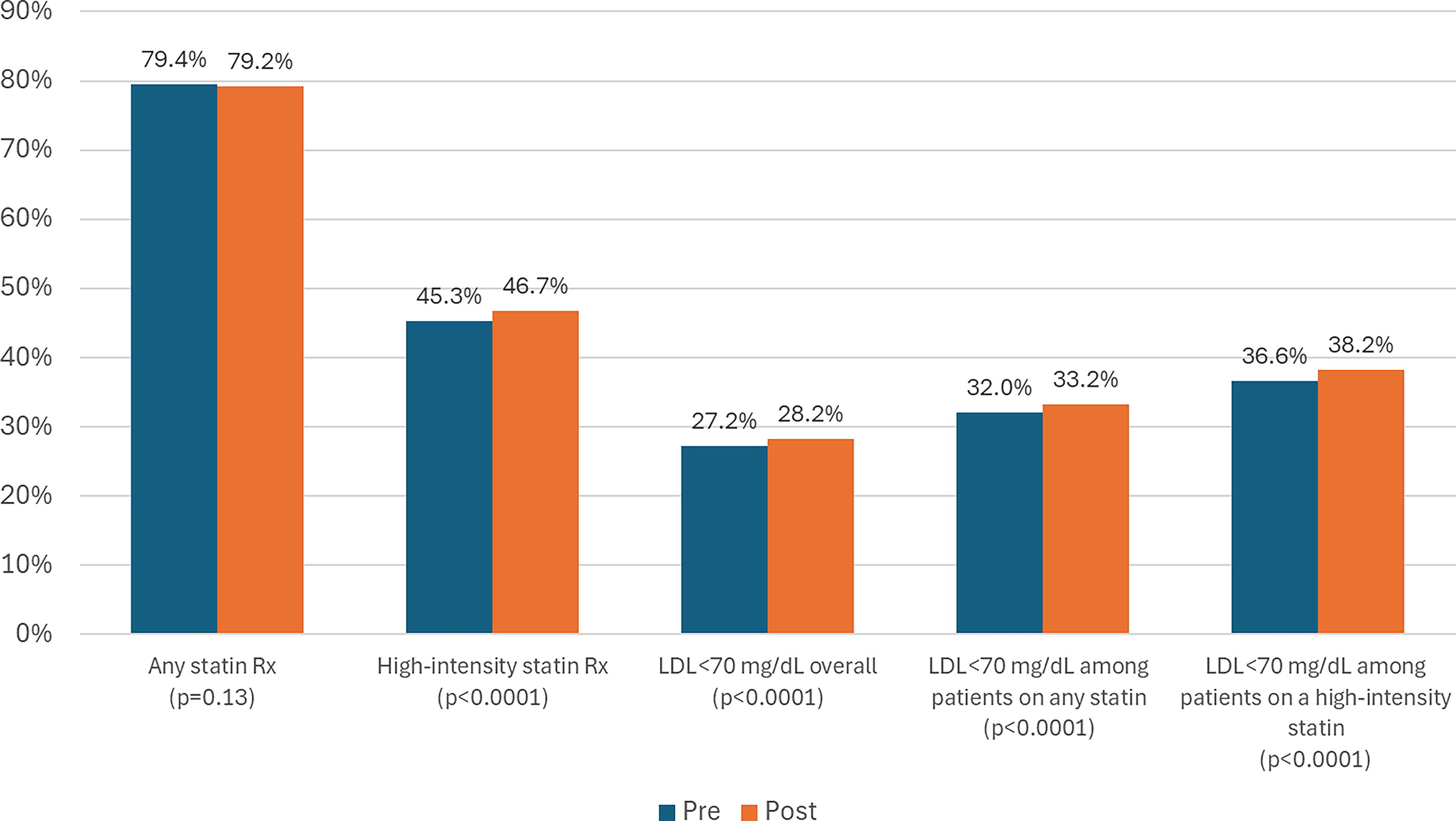
Statin prescribing and LDL-C control pre- and postintervention (n = 115,970)*.
Stratification of the measure for statin prescribing revealed disparities by sex, race, and ethnicity. A 9.4% absolute difference was observed between males and females at baseline (range: 4.1 − 17.5 percentage points) and persisted throughout the intervention period. These identified gaps led to the implementation of interventions to increase prescribing rates among female patients. Four HCOs observed absolute increased prescribing among females of ≥1% (range: 1.1 − 3.6 percentage points). For two of these organizations, male rates increased at higher rates, increasing the gap between males and females. The other two HCOs observed decreases in the gap.
Among those with large enough samples to report (n > 50), six of 11 HCOs demonstrated a baseline statin-prescribing disparity between non-Hispanic White, and Black patients (range: 0.1–10.6 percentage points), and three of eight HCOs demonstrated a disparity between White and Hispanic patients (0.8 and 6.4 percentage points). None of these differences were statistically significant.
Interventions
Supplementary Table S1 displays the interventions implemented by each HCO and the improvements from baseline (statistically significant or >1.0 percentage point increase in rate, considered clinically relevant) for each of the three measures (top three rows). Because HCOs implemented multiple interventions per measure and because the Collaborative did not have a control group, the study was unable to isolate the individual impact of specific interventions. The most commonly implemented interventions by the HCOs with statistically significant or clinically relevant improvement in outcomes were: the identification of disparate populations with gaps in care; EHR enhancements for patients with ASCVD not at goal for statin therapy and LDL control (including health maintenance alerts); creation of education materials/social media to promote awareness about ASCVD and statin therapy; provider meetings used as forum for clinical education; collaboration with pharmacist to provide patient education for statin therapy; and pre-visit planning by clinical team for ASCVD patients with/without statin therapy and LDL control.
Specific to Measure 1 (percent of ASCVD cohort prescribed any statin in the past 12 months), four HCOs showed improvements that were statistically significant or clinically relevant (not statistically significant but >1.0 percentage point increase). These ranged from 0.8 to 4.6 percentage points, and the most commonly implemented interventions included identification of disparate populations with gaps in care and addressing those gaps and provider meetings used as forum for clinical education.
Specific to Measure 2 (percent of ASCVD cohort prescribed a high-intensity statin in the past 12 months), six HCOs observed improvements that were statistically significant or clinically relevant (range 0.8 to 12 percentage points), and the most commonly implemented interventions included identification of disparate populations with gaps in care; use of EHR for patients with ASCVD who are not at goal for statin therapy and LDL control; and previsit planning by clinical team for ASCVD patients with/without statin therapy and LDL control.
Specific to Measure 3 (percent of ASCVD cohort with LDL-C measured in the past 12 months and <70 mg/dL LDL control), nine organizations observed statistically significant or clinically relevant improvements (range: 0.6–6.0 percentage points), and the most commonly implemented interventions included identification of disparate populations with gaps in care; use of EHR to create reports for patients with ASCVD not at goal for statin therapy and LDL control; creation of education materials/social media to promote awareness about ASCVD and statin therapy; collaboration with pharmacist to provide patient education for statin therapy; and provider meetings used as forum for clinical education.
Discussion
Each participating HCO successfully improved at least one of the Collaborative measures, demonstrating dedication, resources, and teamwork across multidisciplinary teams. The Collaborative’s findings also reinforced the premise that management and care of patients with established ASCVD requires successfully monitoring and improving key quality performance measures.
Noteworthy findings across specific measurements and interventions included the following:
EHR enhancements and clinical decision support tools
EHR-based interventions have been connected to increases in statin prescribing, including passive versus active EHR alerts for cardiologists, natural language processing-powered clinician reminders, algorithm-generated recommendations, 15 –17 and EHR-hosted best practice alerts to remind providers of guideline-directed medical therapy when discharging ASCVD patients. Utilizing clinical decision support tools presents a chance to impact provider practices and enhance care for patients with ASCVD and necessitates additional research. 18
In the ASCVD Best Practices Learning Collaborative, EHR enhancements and encouraging and incentivizing the use of advanced clinical decision support tools were two of the four interventions most often associated with increased prescriptions of high-intensity statins.
Previsit planning and provider education
Previsit planning by clinical teams was associated with improved outcomes in all three measures—supporting research findings that positive change starts with the care team. In a cluster randomized clinical trial involving approximately 4000 older patients of diverse racial and gender backgrounds, it was found that text message reminders to patients prior to their appointments did not lead to a significant increase in statin prescriptions. However, when both clinicians and patients received reminders, there was a notable increase in statin prescribing by 7.2 percentage points compared to standard care. 19
The Collaborative HCOs that focused on provider and staff education saw the greatest improvements in Measures 2 and 3: the prescribing of high-intensity statins and LDL-C control.
Documentation and sharing of progress on clinical outcomes were areas of focus throughout the Collaborative, with HCOs reporting challenges in this area. To address this challenge, HCOs included clinical documentation departments in their Collaborative intervention teams. Research supports a need for proper clinical documentation. In a study of over 56,530 ASCVD patients in Northern California, only 18% of patients indicated for statin therapy but without statin prescriptions had any mention of statins in clinical notes. 19
Patient education and outreach
As with many chronic conditions, efforts to reduce ASCVD risk and improve outcomes include engaging patients in their own care. 20 Tactics to educate patients and raise awareness of ASCVD risk were among the top interventions connected to increased prescriptions of any statin and increased LDL-C control.
Interventions to reach out to patients were associated with improved LDL-C control (detailed in the “quick win” example below) and, with pharmacists conducting this outreach, were also associated with the prescribing of high-intensity statins.
Collaborative drug therapy management with pharmacists has been shown to be useful at increasing statin use, 21 and Collaborative results engaging pharmacists for patient outreach align with previous research. In a safety-net health care system in Colorado, clinical pharmacists reached out by telephone to eligible patients in managed care health plans who were not currently receiving moderate to high-intensity statin therapy. HEDIS data showed an increase in statin prescribing from 24.7% to 56.6%. 22
A “quick win” in LDL-C control
Early in the implementation period, Collaborative participants and AMGA recognized an opportunity for a “quick win” by targeting ASCVD patients who had not had an LDL-C measurement recorded in the past 12 months.
The Collaborative encouraged HCOs to implement a short-term intervention by generating a list of these patients to share with clinic providers and staff and guide outreach via email, text, phone, or patient portal. The goal: obtain a current LDL-C measurement and schedule an appointment with the provider for patients with LDL >70 for management and treatment.
As displayed in Table 2, 10 of 12 HCOs saw an improvement in the LDL-C control measures, and the Collaborative cohort as a whole demonstrated absolute improvements of 1.0%, 1.2%, and 1.6% in patients with LDL-C < 70 mg/dL, among the ASCVD cohort, those prescribed any statin, and those prescribed a high-intensity statin, respectively.
Measures and Interventions by Health Care Organization
Improvements reflect positive changes in rates from baseline to Q4 2023 that were either statistically significant or considered to be clinically relevant (nonstatistically significant change of ≥1 percentage point). All HCOs reported data on all measures, but only statistically significant or clinically relevant changes were reported in this table. See Supplementary Tables S1, S2 and S3 for complete results.
Statistically significant absolute improvement at P < 0.10.
Clinically relevant, nonstatistically significant absolute improvement of ≥1.0 percentage point (%).
ASCVD, atherosclerotic cardiovascular disease; EHR, electronic health record; HCO, health care organization; H.I., high-intensity; LDL, low-density lipoprotein; LDL-C, low-density lipoprotein control; ns, change was neither statistically significant nor clinically relevant; Rx, prescription.
Disparities in care
After identifying a difference in practice with male and female patients, Collaborative HCOs created unique interventions to close this gap. The greatest improvements were seen in Collaborative Measure 1: increased prescribing of any statin. Four HCOs showed absolute improvement of ≥1% statin prescribing among females (range: 1.6–3.6 percentage points), resulting in decreased male-female statin-prescribing gaps for two of them.
Previously published research reinforces the need to address disparities related to sex. Women were less likely to receive any statin prescriptions and less likely to receive high-intensity statin prescriptions. 19
Increased statin use and improved clinical outcomes
The ASCVD Best Practices Learning Collaborative observed a 1.4% absolute increase in high-intensity statin prescribing. While this change might seem modest, it is clinically significant according to several key studies and guidelines. In one study, patients who received statin treatment demonstrated a 20%−30% reduction in death and major cardiovascular events compared with patients who received placebo. 23
This advantage was generally present across study types and statin treatment types and for patients with less severe dyslipidemia. The benefit in clinical outcomes was noticeable as early as one year. 23 Therefore, any improvement in statin prescribing may save lives.
The Collaborative supported this by demonstrating improvement in an intermediate outcome, that is, LDL-C. A comparison of LDL-C control rates by level of statin prescribing found increasing rates of 28%, 33%, and 38%, in the full ASCVD cohort, among those prescribed any statin, and among those prescribed a high-intensity statin, respectively.
Noteworthy strengths of the Collaborative model
Each HCO created unique interventions tailored to their organization, but all reported on the same set of measures (see Table 2). This ensured consistency of data across organizations, facilitating accurate benchmarking, and comparative analyses.
Furthermore, integrating Collaborative measures into their reporting processes has enabled HCOs to continue to document, track, and report outcomes after the Collaborative period and identify additional areas of need in the future. HCOs have stated plans to continue collecting data on these measures.
In the post-Collaborative survey, participating HCOs noted that the quality improvement process outlined by AMGA supported the development of their ASCVD program. They also noted that documentation of quality improvement efforts and quarterly data reporting, along with guidance from AMGA, webinars, in-person meetings, and site visits, motivated their organizations to prioritize ASCVD.
Limitations
Participating HCOs varied in size, structure, and patient demographics, with differing levels of resources allocated for the program. While all shared a common Collaborative goal: enhance care for patients with established ASCVD, they implemented unique interventions. As mentioned previously, because many HCOs implemented multiple interventions per measure and because the Collaborative did not have a control group, the study was unable to isolate the individual impact of specific interventions. Evaluation using aggregate data proved challenging, and statistical analyses to explore potential associations between interventions and clinical outcomes could not be conducted due to the quality improvement design of the project. In addition, improvements in intermediate outcomes (e.g., LDL-C control) might not be observed within a 12-month intervention period, and certainly, the detection of changes in long-term outcomes (e.g., prevention of major adverse cardiovascular events) would require a longer follow-up period).
Some of the data HCOs submitted reflected their entire organization, not just specific locations where interventions were carried out, potentially diluting positive clinical outcomes.
Furthermore, the structure of the Collaborative did not allow for continuous follow-up of a single group of patients. Patient churn (i.e., moving from one health system to another) and the associated lack of continuity may have limited the impact of the interventions, while the presence of new patients at the clinics made it challenging to enhance their individual measures. In addition to patient churn, patient mortality during the baseline and intervention periods caused fluctuations in the measurement denominators.
Finally, the reporting of prescribed statins does not capture the intensification of a statin within a high-intensity class (e.g., titrating rosuvastatin from 20 to 40 mg) or with the addition of a nonstatin therapy. Thus, changes may have been made to patients’ medication regimens that were not captured in the data and may have led to an underestimation of the impact of statin prescribing on patient outcomes. Data were not collected; therefore, it was impossible to determine whether patients were taking their medications as prescribed. This was, therefore, an intent-to-treat analysis and a per-protocol analysis may have returned better results among clinical outcomes.
Conclusion
The HCOs that participated in the intensive 12-month Best Practices Learning Collaborative improved in at least one of the Collaborative measures, and the Collaborative cohort successfully implemented a mean of more than four interventions to improve care for patients with ASCVD. The Collaborative cohort included 115,970 patients with ASCVD. High-intensity statin prescribing rates increased from 45.3% at baseline to 46.7% at follow-up and LDL-C control (<70 mg/dL) improved overall, as well as by statin use, with increases from 27.2% to 28.2%, 32.0% to 33.2%, and 36.6% to 38.2% for overall control, patients on any statin, and patients on a high-intensity statin, respectively.
The study of the impact of the Best Practices Learning Collaborative to improve the management of patients with ASCVD successfully demonstrated the ability to collect and report data from HCOs to monitor progress on clinical outcome measures across diverse HCOs. In addition, participating HCOs reported regularly finding value in the measures and quality improvement processes for program tracking, evaluation, and continuous improvement. The ongoing efforts of HCOs indicate the sustainability of the programs they have implemented. AMGA continues to provide platforms for HCOs to engage with one another through conferences, listservs, and other means. Additionally, AMGA intends to share the findings widely with its membership and the broader community.
The Collaborative model presents an effective means for achieving improvement. There exists potential for conducting a more rigorous study, which may include the incorporation of a control group. Furthermore, HCOs could focus on a single area to adopt a more targeted approach.
Footnotes
Acknowledgments
The authors would like to thank advisors Amy Ahnert (Lehigh Valley Heart and Vascular Institute), Scott Berkowitz (John Hopkins Medicine), Liana Spano-Brennan (Summit Health), and Nihar R. Desai (Yale University School of Medicine) for assistance with program design and interpretation of findings.
Authors’ Contributions
Ms. Chambers, Ms. Rattelman, Dr. Kennedy, Dr. Ciemins, and Ms. Casanova participated in study design and data collection, analysis, and interpretation. Dr. Agnihotri participated in the study design and data analysis and interpretation. Ms. Leaver-Schmidt participated in study design, data collection, data analysis and interpretation, and drafted the article. All authors contributed to the revision of the article and approved the final version for submission.
Author Disclosure Statement
No competing interests were declared.
Funding Information
This Collaborative was funded by Novartis Pharmaceuticals and Amgen. This Collaborative received writing/editorial support from Jill Marquardt of Garfinkel + Associates, funded by Novartis Pharmaceuticals and Amgen.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.