
Abstract
A majority of patients with heart failure (HF) do not receive adequate medical therapy as recommended by clinical guidelines. One major obstacle encountered by population health management (PHM) programs to improve medication usage is the substantial burden placed on clinical staff who must manually sift through electronic health records (EHRs) to ascertain patients’ eligibility for the guidelines. As a potential solution, the study team developed a rule-based system (RBS) that automatically parses the EHR for identifying patients with HF who may be eligible for guideline-directed therapy. The RBS was deployed to streamline a PHM program at Brigham and Women’s Hospital wherein the RBS was executed every other month to identify potentially eligible patients for further screening by the program staff. The study team evaluated the performance of the system and performed an error analysis to identify areas for improving the system. Of approximately 161,000 patients who have an echocardiogram in the health system, each execution of the RBS typically identified around 4200 patients. A total 5460 patients were manually screened, of which 1754 were found to be truly eligible with an accuracy of 32.1%. An analysis of the false-positive cases showed that over 38% of the false positives were due to incorrect determination of symptomatic HF and medication history of the patients. The system’s performance can be potentially improved by integrating information from clinical notes. The RBS provided a systematic way to narrow down the patient population to a subset that is enriched for eligible patients. However, there is a need to further optimize the system by integrating processing of clinical notes. This study highlights the practical challenges of implementing automated tools to facilitate guideline-directed care.
Introduction
Heart failure (HF) remains a public health problem of major proportion, and the national burden is estimated to increase by 25% by 2030. 1,2 Although many new therapies for managing patients with HF have shown benefit and are accordingly recommended by current practice guidelines, guideline-directed medical therapy (GDMT) remains significantly underutilized in clinical practice. 3 A key challenge in implementing clinical interventions to improve GDMT is that clinical staff are required to exert extensive manual effort to review electronic health records (EHR) to determine a patient’s guideline eligibility. To address this issue, we have developed a rule-based system (RBS) for searching the EHR to find patients who are eligible for the HF guidelines.
Background and Significance
More than 25 years after its designation as an emerging epidemic, 4 HF remains a clinical and public health problem of major proportion. Approximately 6.5 million adults in the United States currently have HF, and nearly 0.9 million new cases are diagnosed annually. 1,5 The lifetime risk of developing HF at age 40 is 20%. 6 Projections show that the prevalence of HF will increase by 46% from 2012 to 2030, resulting in >8 million adults with HF. 7 Until 2012, the hospitalizations for HF were decreasing; however, the trend has reversed, largely due to the aging population. The total cost of HF care in the United States exceeds $30 billion annually, including health care services, medications, and missed days at work. 1,8
Despite systematic efforts by the medical community over the last 2 decades, progress in reducing the incidence and improving the outcomes of HF has not been commensurate with the resources dedicated to its management. Current medical therapies have shown benefits across the spectrum of HF phenotypes based on the ejection fraction (EF): Heart failure with reduced ejection fraction (HFrEF), heart failure with mildly reduced ejection fraction (HFmrEF), and heart failure with preserved ejection fraction (HFpEF). Multiple professional societies recommend medical therapies with proven benefits for patients with HF to reduce hospitalizations, prolong survival, and improve quality of life. 10 For patients with HFrEF, quadruple therapy consists of (1) renin–angiotensin system inhibition with angiotensin receptor–neprilysin inhibitors (ARNI), angiotensin-converting enzyme inhibitors (ACEi), or angiotensin II receptors blockers alone; (2) beta-blockers; (3) mineralocorticoid receptor antagonists (MRAs); and (4) the sodium–glucose co-transport inhibitors (SGLT2i), all receiving Class 1 recommendations with Level of Evidence A. 9,11 For HFmrEF, SGLT2i are given Class 2a recommendations, while ARNI, ACEi, ARB, MRA, and beta-blockers receive Class 2b recommendations. For HFpEF, SGLT2i are recommended (Class 2a) with MRA and ARNIs receiving Class 2b recommendations. 9 The rapid initiation and titration of GDMT are associated with improved outcomes. 12 Despite robust evidence of clinical benefits and guidelines from professional societies, GDMT remains significantly underutilized in clinical practice. 13,14
Efforts to improve GDMT in patients with HF are ubiquitous across health care systems. The interventions include clinician education and audits, nurse-led follow-ups after discharge, 15 protocolized visits with cardiologists after hospital discharge, 16 EHR-embedded alerts, 17,18 patient registries, and multidisciplinary team-based programs. 19 Protocolized visits with cardiologists and interventions based on multidisciplinary teams have been found to have a better impact than clinician alerts or quality initiatives that focus on education and audit-feedback processes alone. 16 The effort presented in this article has been carried out to facilitate a population health management (PHM) program at Brigham and Women’s Hospital (BWH), called the Cooperative Program for ImpLementation of Optimal Therapy in Heart Failure. 20,21 It is a pragmatic, randomized implementation trial (NCT05734690), 24 in which non-clinician staff (navigators), who are especially trained to approach patients, communicate with patients via phone and titrate the patients’ medications working alongside pharmacists and under the supervision of an advanced practice provider and a cardiologist. 22,23 Navigators interact with participants via phone to implement medication changes and monitor adverse events, blood pressure, and lab results. Upon patient acceptance, navigators inform pharmacists who then sent the new prescription.
A key obstacle to the PHM program like other hospital-based initiatives to improve GDMT is the effort of reviewing charts to identify the patients who are on suboptimal GDMT. To facilitate the implementation of the PHM, the study team developed and deployed an RBS for finding patients with HF who may be potentially eligible for receiving medications as recommended by clinical guidelines. This article describes the methodology to create the RBS and presents an evaluation of the RBS after 1 year of deployment. Findings of this study will inform the development of similar systems to facilitate PHM programs at other institutions.
Methods
The study team developed an RBS to identify patients who were not receiving guideline-directed medications, to facilitate these patients’ enrollment into the PHM program at BWH. The RBS processed EHR from the institution’s enterprise data warehouse, to create the list of potentially eligible patients. The list was made available to the navigators who reviewed each patient’s chart to determine the patient’s true eligibility. This study was approved by the institutional review board of BWH (Figure 1). The following sections describe the methodology for developing and evaluating the RBS.
Steps to develop the rule base
Deployment and evaluation of RBS
The study team evaluated the RBS’s performance by deploying it in a real-world setting of the PHM program at BWH. They created a high-recall query to find the medical record numbers of patients who had a transthoracic echocardiogram in the health system and met the criteria of age between 18 and 90 years, alive, and English- or Spanish-speaking. This query was executed on the institutional research data repository to obtain the “denominator set” of patients for this study. The EHR data for all patients in the denominator population were extracted, and then the RBS was executed on the extracted data to create a list of patients potentially eligible for GDMT.
The EHR data extract for patients was refreshed approximately once every 2 months, and the RBS was rerun to obtain a new list for manual screening. The navigators used an electronic checklist while performing the chart review to annotate the presence or absence of a program criterion. The checklist ensured a consistent approach to record the results of the manual chart review.
We measured the RBS’s performance as the percentage of patients determined to be truly eligible by manual chart review performed by the program navigators. Furthermore, we examined the navigator’s annotations for the false-positive patients, to identify ways to further improve the RBS.
Results
Each execution of the high-recall query resulted in a denominator set of approximately 161,000 patients, from which the RBS would short-list approximately 4200 (2.6%) patients for screening (see Fig. 2). In the period from January 1, 2023, to December 31, 2023, the navigators reviewed the electronic charts of 5660 patients identified by the RBS. They “screened-in” 1754 patients (1754/5460 = 32.1%), and the remaining 3706 patients were deemed “screened-out.” Navigators indicated the reasons for screening out 3177 patients (Table 1, Table 2 and Fig. 3).

Deployment of the rule-based system to find patients for enrollment into the remote medication management program.
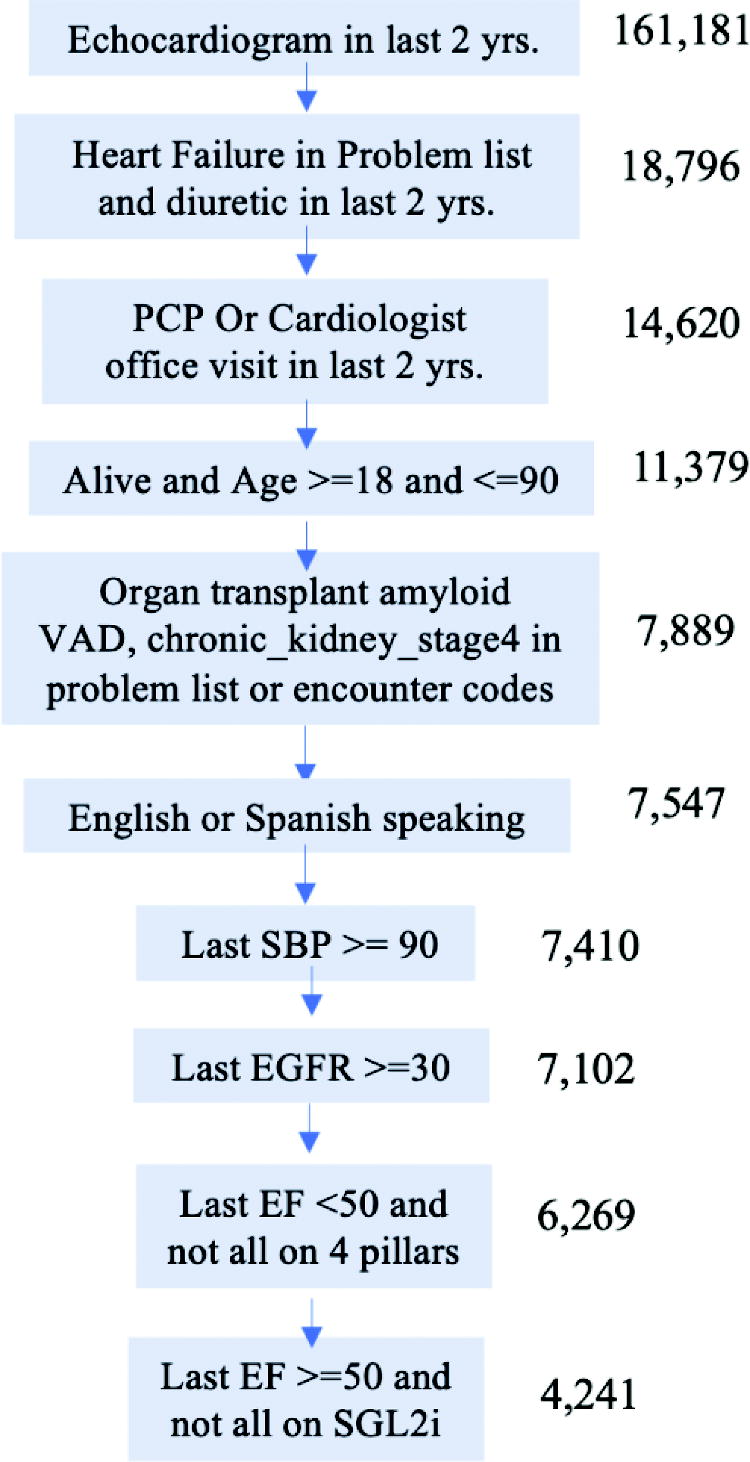
Consort diagram showing the patient counts during a typical execution of the RBS. RBS, rule-based system.
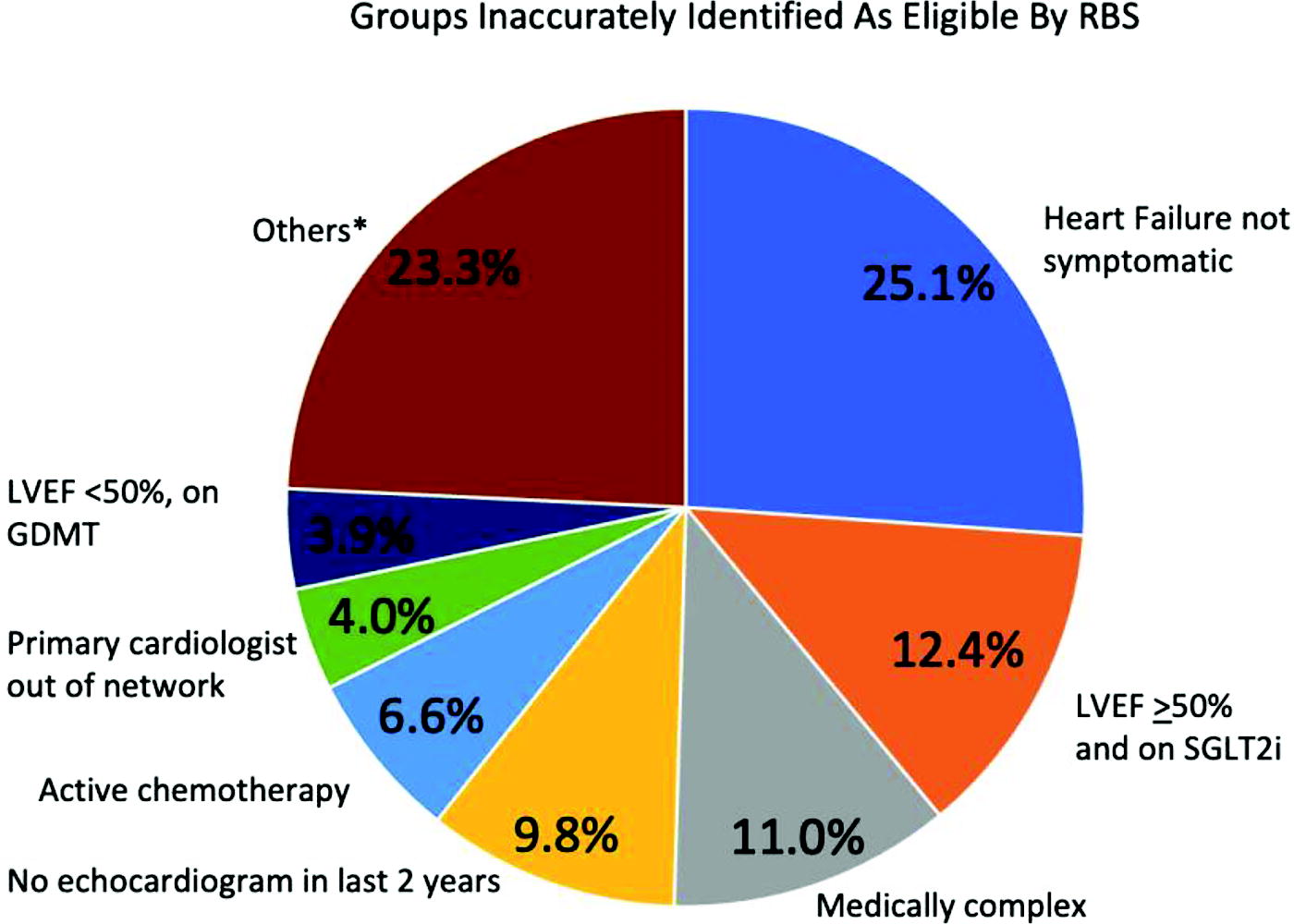
Summary of reasons for false positives from RBS determined by manual chart review. Over 25% of patients identified as eligible by RBS were found to not have symptomatic HF, the criteria of which included clinical symptoms documented in clinician notes, use of diuretics, or acute HF hospitalization within last 2 years from time of screening. RBS did not process clinical notes to identify patients with symptomatic HF. HF, heart failure; RBS, rule-based system.
Demographics of Screened Cohort
Distribution of Reasons for Screening Out False-Positive Cases
BP, blood pressure; GDMT, guideline-directed medical therapy; HF, heart failure; SGLT2i, sodium–glucose co-transport inhibitors; LVEF, left ventricular ejection fraction; EGFR, estimated glomerular filtration rate; MGH, Massachusetts General Hospital.
Although there can be multiple reasons for screening out a patient, the navigators generally terminated their chart review when they encountered a reason for screening out, so usually only 1 screen-out reason was indicated per patient. The distribution of the number of screen-out reasons is shown in Table 3.
Distribution of Number of Screen-out Reasons Annotated by the Clinical Staff During the Manual Chart Review
Discussion
We developed an RBS that automatically processed EHR to identify a cohort of patients with HF who were not receiving GDMT. The system was deployed in a real-world setting to find patients for enrollment into a PHM program at BWH.
Development of the RBS was necessary given the complexity of the guideline logic for determining the optimal medications based on the EHR data. Breaking up the logic into individual queries for execution on the EHR involves considerable manual effort and introduces a risk of errors. 25 Rule-based systems have been used to implement clinical guidelines in infectious disease, 26,27 prescription, 28 and cancer surveillance. 29 –31 The approach of combining administrative codes and search terms to model clinical guidelines has been utilized effectively in previous studies. 32
Furthermore, the institutional enterprise data warehouse (EDW) has limited computational power to execute the multitude of steps in the guideline logic. Given the practical limitations on performing the computations in the EDW, we implemented the RBS externally to the EDW. We executed the high-recall query on the EDW to create a denominator cohort and retrieved this cohort’s data onto an institutional server having sufficient computational resources to perform the computations.
The RBS effectively narrowed down the denominator cohort of approximately 161,000 patients to a smaller list of approximately 4200 (2.6%) patients to facilitate the PHM program. The RBS was evaluated to have an accuracy of 32.1%, which helped operationalize the PHM program. Without the RBS, the program team would have to use the conventional approach of querying the EDW to narrow down the denominator population to a smaller set, which would have been cumbersome given the complexity of the criteria and limits on computational processing in the EDW. Furthermore, it would be practically impossible to sift through all the patients’ charts. Alternatively, the program team would have to rely on referrals from the clinicians or the deployment of clinical alerts in the EHR, which would lead to an additional burden on the clinicians potentially contributing to their “alert fatigue” and burnout. Hence, the RBS provides a systematic way to narrow down the cohort to a subset that is enriched for eligible patients, as compared with conventional approaches.
The approach of representing the guideline logic as rules and breaking down the logic systematically into steps that are assembled to determine individual criteria provides a mechanism to increase the granularity of the analysis. This contrasts with the low-complexity queries that are typically possible with conventional queries of an EHR or data warehouse. The rule-based approach provides a robust mechanism to validate rule output at a detailed level and fix errors in the system implementation. Additionally, it allows the computation to be staged in order to apply the logic efficiently.
There have been substantial efforts in the last several decades to implement the logic recommended by clinical guidelines. 33,34 Several implementations have been developed to facilitate clinical decision support, measure care quality, and create cohorts for research, leading to an evolution of frameworks and standards such as Fast Healthcare Interoperability Resources (FHIR) and Clinical Quality Language (CQL). 35 –37 However, the infrequency of reports on real-world evaluations of these system using these standards indicates that these technologies are still not mature, and a stronger evidence base is needed to foster the use of standards in Clinical Decision Support design and implementation. 38 Given the steep learning curve to implement systems using the proposed standards and given the standards’ relative immaturity, we currently did not invest effort in standardizing our RBS to FHIR and CQL standards. However, we believe that this step is essential to facilitate dissemination.
A high proportion of the false positives (39%) was due to incorrect detection of symptomatic HF (25%) and medications (17%). The criterion of symptomatic HF is a requirement in the guidelines for initiating medications, as there is a lack of consensus that asymptomatic patients with reduced Left ventricular ejection fraction (LVEF) can benefit from medications. However, it is challenging to determine this criterion from EHR data. Hence, the prescription of diuretics is used as a surrogate, as they are used to mitigate the symptoms of HF that usually occur due to fluid overload. Symptomatic HF is challenging to detect, as it is a clinical diagnosis that is not explicitly documented in the EHR. It is diagnosed with symptoms of shortness of breath, dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, lower extremity edema, and symptoms of fluid overload including weight gain in a short time, imaging pulmonary edema, pleural effusion, rales crackles, and pitting edema. The symptoms are typically described in clinical notes that are currently not processed in the RBS, which is the likely reason for the high proportion of false positives.
Similarly, the difficulty of accurately extracting the medication history may possibly be due to patients receiving prescriptions at another hospital. This information for prescriptions from external sites is not available in the instructional research database but is likely documented in the clinical notes, which were not processed in the RBS. 39 The authors anticipate that the false positives attributed to symptomatic HF and medication history can be improved by integrating the RBS with conventional natural language processing techniques as well as the use of large language models. 40 –43
The RBS included several criteria necessary to facilitate the medication management intervention. For instance, the criterion for restricting the program to patients who knew English or Spanish was due to the IRB’s consideration that language interpreters are essential for effective communication with the patients. Furthermore, the criterion to exclude patients receiving the cardiology care from outside the hospital was to simplify obtaining the provider’s assent to enroll their patient into the medication management program. The criterion of basic metabolic panel in the last year is to ensure that the baseline parameters of the patient are available before initiating new medications for the patient.
The exclusion criteria in the RBS were designed to exclude patients who had complex decision scenarios that require specialist expertise. This entailed excluding patients with cardiomyopathy, amyloid or congenital heart disease, transplant, last systolic blood pressure <90, ventricular assistive device, advanced kidney disease (estimated glomerular filtration rate [EGFR] <40 or active dialysis), or active chemotherapy. The evaluation demonstrated that this group of patients was effectively excluded as it accounted for only a total of 14% of the false-positive cases.
This study did not include rare exclusion criteria in the RBS, such as pulmonary arterial hypertension, end-of-life care, more than 4 hospitalizations in the last 6 months, and type 1 diabetes, which together constituted 6% of the false positives. The low prevalence supports our approach of bypassing the programming effort to implement these criteria in the RBS.
The value sets are provided in Supplementary Data S1 to facilitate the implementation of similar systems at other institutions. These value sets need to be mapped to the data elements in the local EHR repository to implement the RBS.
Limitations
A limitation of our study is that it only considered whether the patients are on a particular class of medication for determining if they are receiving appropriate GDMT and did not consider the recommended dosage for the medication. Hence, there are potentially more patients who could benefit by up-titration of their medication dosage than the patients identified by our RBS.
Another limitation is that the study only considered structured variables from the EHR for executing the RBS. As indicated in our analysis, inclusion of data from clinical notes can potentially improve the quality of the variables in the RBS and improve the accuracy of the RBS. In particular, there is potentially more information in clinical notes for determination of symptomatic HF and medication history. 40
Conclusion
The RBS provided an effective mechanism to model and execute the guideline logic in comparison with the conventional approach of querying the institutional health record repository. It provided a systematic way to narrow down the patient population to a subset that is enriched for eligible patients. However, there is a need to further optimize the system by integrating processing of clinical notes to improve the screening rate and to enhance the efficiency and impact of the clinical intervention. Overall, our study highlights the practical challenges of implementing automated tools to facilitate guideline-directed care.
The definitions of the value sets for deriving the variables in the rule base are provided in Supplementary Data S1, along with a query for the guideline criteria (https://github.com/dschc/supplementary_material/blob/main/supplementary.zip).
Footnotes
Authors’ Contributions
Subramaniam led the chart review by the clinical team, oversaw the manual annotations in the chart review, and contributed to the design of the RBS. Scirica, Blood, and Unlu contributed to the interpretation of the guideline logic and contributed to the design of the RBS. Hassan, Kumar, Zelle, and Varugheese contributed to the analysis. Dr. Wagholikar led the design, implementation, and deployment of the RBS and prepared the first draft of the article. All authors reviewed and approved the final draft of the article.
Author Disclosure Statement
Aronson, Blood, Oates, Scirica, Unlu, and Varugheese report research grants and related funding via BWH: Better Therapeutics, Boehringer Ingelheim, Eli Lilly, Milestone Pharmaceuticals, and NovoNordisk. Aronson reports consulting to Nest Genomics. Aronson, Mailly, Oates, Tucci, and Wang also report unrelated National Institutes of Health (NIH) and Patient-Centered Outcomes Research Institute support. Blood reports consulting income from Walgreens Health, Color Health, Novo Nordisk, Medscape, and Arsenal Capital Partners and equity holdings in Knownwell health. Scirica reports consulting fees from Abbvie (DSMB), AstraZeneca (DSMB), Boehringer Ingelheim (DSMB), Better Therapeutics, Elsevier Practice Update Cardiology, Esperion, Hanmi (DSMB), Lexeo (DSMB), and NovoNordisk and equity in Health [at] Scale. Unlu receives funding from the National Heart Lung and Blood Institute under award number T32HL007604. Dr. Wagholikar receives funding from National Heart Lung and Blood Institute, NIH, and has equity in ATS Summary Corp. Dr. Desai has been a consultant to Abbott, AstraZeneca, Boehringer-Ingelheim, Boston Scientific, Corvidia Therapeutics, DalCor Pharma, Regeneron, Relypsa, and Zogenix and has received research support from Novartis. Dr. Cannon reports research grants from Amgen, Better Therapeutics, Boehringer Ingelheim, Daiichi Sankyo, Merck, Novo Nordisk, and Pfizer and consulting for Amryt/Chiesi, Alnylam, Amarin, Amgen, Applied Therapeutics, Ascendia, Biogen, Boehringer Ingelheim, Bristol Myers-Squibb, CSL Behring, Eli Lilly, Janssen, Lexicon, Merck, Milestone, Pfizer, Rhoshan, and Sanofi. Nichols reports consulting income from Recor Medical and Elsevier.
Funding Information
This work was conducted with support from Boehringer Ingelheim, NIH Awards R01HL151643 and T32HL007604, and financial contributions from MassGeneral Brigham.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.