
Abstract
Chronic kidney disease (CKD) is common, costly, and life-limiting, requiring dialysis and transplantation in advanced stages. Although effective guideline-based therapy exists, the asymptomatic nature of CKD together with low health literacy, adverse social determinants of health, unmet behavioral health needs, and primary care providers’ (PCP) limited understanding of CKD result in defects in screening and diagnosis. Care is fragmented between PCPs and specialty nephrologists, with limited time, expertise, and resources to address systemic gaps. In this article, the authors define how they classified defects in care and report the current numbers of patients exposed to these defects, both nationally and in their health system Accountable Care Organization. They describe use of the health system’s three-pillar leadership model (believing, belonging, and building) to empower providers to transform CKD care. Believing entailed engaging individuals to believe defects in CKD care could be eliminated and were a collective responsibility. Belonging fostered the creation of learning communities that broke down silos and encouraged open communication and collaboration between PCPs and nephrologists. Building involved constructing a fractal management infrastructure with transparent reporting and shared accountability, which would enable success in innovation and transformation. The result is proactive and relational CKD care organized around the patient’s needs in University Hospitals Systems of Excellence. Systems of excellence combine multiple domains of expertise to promote best practice guidelines and integrate care throughout the system. The authors further describe a preliminary pilot of the CKD System of Excellence in primary care.
Introduction
Chronic kidney disease (CKD) is a common, morbid, and costly condition for adults in the United States (US). This disease afflicts approximately 37 million people (15% of US adults). 1 Among Medicare beneficiaries aged ≥66 years, the adjusted mortality is more than twice as high for those with CKD compared to those without CKD. 2 In addition, Medicare spending for beneficiaries 66 years of age or older with CKD (excluding end-stage kidney disease as the drivers of cost are different in this population 3 ) topped $70 billion in 2018, accounting for nearly one-fourth of total Medicare spending. 4 In a prominent 2001 report, Crossing the Quality Chasm, the Institute of Medicine proposed fundamental changes in the US health care delivery system, including the creation of an infrastructure to support evidence-based care, utilization of information technology, better alignment of payment incentives, and preparation of the workforce to better meet patient needs in a rapidly changing and evolving environment. 5 More than 2 decades later, CKD care exemplifies the low-value, high-cost, low-quality conundrum the Institute of Medicine had rallied against. Two successive presidential administrations have brought CKD care to the fore. President Trump released an executive order in 2019, calling for better diagnosis and treatment of CKD and offering incentives for preventive care as a policy initiative. 6 President Biden’s 2021 executive order for Advancing Racial Equity promises to address kidney health disparities by fostering equity for historically marginalized communities. 7
Despite national awareness of the burdens of CKD, care remains riddled with defects and is often transactional rather than relational, resulting in avoidable death, disability, and costs. The purpose of this article is to examine key provider- and system-related defects in CKD care and describe the creation of a CKD System of Excellence (SOE) to address these defects in University Hospitals (UH) Accountable Care Organization (ACO). In this article, the authors define how they classified these defects in care and report the current number and percent of patients exposed to the defects, both nationally and in their ACO, and describe a preliminary pilot of the CKD SOE in primary care. Notably, CKD is often the result of other comorbidities such as diabetes, hypertension, and heart failure; thus, many provider and system defects in CKD care are similar for other chronic disease states. The difference is that CKD is often unrecognized and underdiagnosed. New agents can halt or slow disease progression and prevent the need for dialysis, giving urgency to diagnose and treat CKD sooner.
Provider and System Defects in CKD Care
High rates of unrecognized CKD
CKD is asymptomatic—patients can lose up to 90% of their kidney function before exhibiting symptoms, and 4 out of 5 patients with advanced CKD are not aware of their condition. 8 In a study of Medicare advantage beneficiaries, only 27% (45,636 of 167,524) with a serum creatinine value indicating CKD (for all stages) in 2014 had a linking CKD diagnosis code on a billing claim in 2013 or 2015. 9 Medicare fee-for-service (FFS) beneficiaries with laboratory-based CKD have even lower rates of diagnosed CKD, at 11.8% (24,286 of 206,036 beneficiaries). 10 A qualitative study by the International Society of Nephrology surveyed key opinion leaders in 124 countries regarding their approaches to CKD care and aggregated the data by region in the Global Kidney Health Atlas in 2017. 11 In their report, 64% of countries rated awareness of CKD among primary care providers (PCPs) as low/below average or extremely low on a 5-point Likert scale. Although specifics about the level of awareness among PCPs in the US were not available in the Atlas, 11 a systematic review by Neale et al. 12 found 5 of 20 studies reported PCP “lack of awareness of guidelines” (including 3 from the US).
Gaps in evidence-based practices
Alarming numbers of CKD patients do not get evidence-based care. Urine albumin and protein testing have prognostic implications for CKD. Yet only 40% of patients with CKD in the Medicare FFS and Medicare advantage populations (aged ≥66 years) and 55%−60% of commercially insured patients (aged 18–65 years) were tested in 2020. 13 In a national randomly sampled, serially collected, cross-sectional study of PCP practices (n = 112) conducted by the Centers for Disease Control and Prevention during 2006–2014, nearly 50% and 40% of patients with CKD had uncontrolled blood pressure and diabetes, respectively. 14 Three decades ago, Lewis et al. 15 first demonstrated the benefit of renin-angiotensin system blockade using an angiotensin-converting enzyme inhibitor (ACEI) for diabetic kidney disease. However, a recent study of 606,064 electronic health records (EHRs) of adult patients with CKD showed low prescription rates for ACEI or an angiotensin receptor blocker (20.6%) and low measurements of albuminuria (8.7%) and proteinuria (4.1%). 16 Just within the last 3 years, emerging evidence revealed the potential for sodium-glucose cotransporter-2 inhibitors and select mineralocorticoid receptor antagonists (in diabetic kidney disease) to revolutionize kidney care by slowing or halting the progression of kidney disease. 17,18 However, uptake of these agents is unclear as studies reporting prescription rates are not available in the literature.
Imbalance between CKD demand and provider supply: Poor access to nephrology
Most patients with CKD are cared for in PCP practices. Thus, an adequate and educated PCP workforce is critical to achieving quality care for CKD patients. 19 While the demand for CKD care is projected to grow, the Association of American Medical Colleges projects a shortage of between 17,800 and 48,000 PCPs by 2034, which is quite worrisome. 20 It is also unclear whether the US nephrology workforce will be sufficient, particularly given the rising prevalence of CKD and the declining number of new fellows entering nephrology. 21 In northeast Ohio where 24.5% of the Medicare population has CKD, 22 the math offers a dim view for nephrologists (Fig. 1). Approximately 100 nephrologists would be needed to care for just Medicare beneficiaries, which excludes patients with unrecognized CKD and with late-stage CKD/end-stage renal disease. Another serious concern is the lack of nephrology follow-up for patients with CKD, even those with a high risk of progression to ESKD. In an administrative claims data analysis of commercial and Medicare advantage adult beneficiaries with CKD (n = 156,733; 2012–2019), only 41% with >10% risk of progression to ESKD at 5 years were referred to nephrology. 23 Although the reasons for this nephrology care gap are multifactorial, including high rates of unrecognized CKD, provider nonadherence to evidence-based care, provider burnout, poor patient activation, and lack of behavioral health screening and treatment, the shortage in the nephrology workforce is an important factor. This gap translates to decreased access to transplants, late referral for dialysis resulting in emergency starts, and increased morbidity and complications. 24

Overwhelming Demand for Nephrology Specialty with Greater Recognition of Early-Stage Chronic Kidney Disease in Northeast Ohio. Figure 1 shows the misalignment between nephrologist care of advanced kidney failure (eg, transplantation, inpatient consult, outpatient dialysis) and demand for CKD care in northeast (N.E.) Ohio. Source: Reference 22-Healthy Northeast Ohio. Chronic kidney disease: Medicare population. Conduent Healthy Communities Institute (Healthy People 2030 Champion). Accessed April 27, 2023. https://www.healthyneo.org/indicators/index/view?indicatorId=2056&localeId=285563. CKD, chronic kidney disease.
High utilization and mortality rates
In 2020, emergency department (ED) visits and hospitalization rates were 2.0–2.5 times higher for individuals with CKD compared to those without CKD, regardless of insurance type. 25 All-cause mortality in 2020 in the Medicare FFS group was 100.6 per 1000 person-years for patients with CKD vs. 45.6 per 1000 person-years without CKD. 25
Unrecognized low health literacy and the impact of social determinants of health
Poor activation and low health literacy are common issues in the CKD population and can have negative consequences on disease management, health outcomes, and health care costs. Patients who are poorly activated have reduced knowledge, skills, and confidence in managing their own health care and, therefore, demonstrate less involvement. 26 Poor activation translates into missing appointments, not adhering to treatment plans, or not engaging in self-management behaviors (such as diet and exercise). Up to 60% of individuals living with CKD display low levels of activation. 26 Low health literacy refers to the inability to obtain, understand, and process health information and use it to make informed decisions about their health care. Research has shown that approximately 25% of patients with CKD have limited health literacy skills. 27 The reasons for poor engagement and low health literacy in CKD are complex and multifactorial. Some contributing factors include lack of patient education and awareness, language barriers, low socioeconomic status (SES), and difficulty managing multiple medical and psychological comorbidities. Poor activation and low health literacy can have dire consequences for patients with CKD. Low health literacy is associated with higher health care costs, increased hospitalization rates, and increased mortality among patients with CKD. 27
Social determinants of health (SDOH) can have a profound effect on CKD onset, progression, and outcomes. Low SES is associated not only with increased incidence and prevalence of CKD but also with a higher risk of CKD progression and mortality. 28 Socioeconomics could exert complex interdependent and independent effects on CKD, influencing access to quality care and treatment for CKD risk factors and comorbidities. Social isolation and loneliness are associated with a higher risk of CKD onset and progression. 29 Patients with CKD who have difficulty accessing health care have a higher risk of mortality than those who have easier access to health care. 30 Improving access to health care could potentially lead to better outcomes for CKD.
Failure to screen for and treat behavioral health
CKD is associated with mental illness owing to shared risk factors, such as smoking, lithium use, diabetes, and cardiovascular disease or adverse SDOH such as food insecurity, homelessness, and social exclusion. 31 Nearly 27% of adults with self-reported CKD also self-reported mental illness, including 7% with serious mental illness. 32 The actual number is likely much higher, as the prevalence of depression in patients with CKD is up to 4 times higher than the general population and up to 3 times higher than other chronic diseases. 33 Early detection and management of mental illness may attenuate the impact of these complications at later stages. However, adults with CKD more commonly have unmet mental health needs, generally twice the general population’s rate. 32 Evidence demonstrates that people with chronic conditions such as CKD and mental illness have higher rates of urgent care utilization, longer hospital stays, and higher health care costs. 34 Society bears the cost of inadequately treated mental illness—leading to millions of dollars of direct and indirect costs. 35
Assessing CKD Burden and Care Defects in UH ACO
The UH health system is a $5.5 billion academic health system with 23 hospitals and over 55 ambulatory offices across northeast Ohio, serving approximately 1.4 million unique patients annually. More than 560,000 (almost 40%) of these patients are members of the UH ACO. To assess the burden of CKD and gaps in care at UH, the authors focused on the UH ACO member population. Outpatient laboratory glomerular filtration rate (GFR) values and International Classification of Disease, Tenth Revision (ICD-10) codes for CKD were extracted from the EHR through the UH Enterprise Data Warehouse for ACO members from July 2020 to July 2023. They used the Kidney Disease: Improving Global Outcomes (KDIGO) 2005 definition 36 for the CKD classification, with two abnormal GFR values <60 mL/min per 1.73 m2, taken at least 90 days apart, indicating a laboratory diagnosis of CKD. Patients with recognized CKD were defined as those with both laboratory diagnosis and an ICD-10 code during the study period, whereas unrecognized CKD patients had a laboratory diagnosis, but no ICD-10 code. Partially screened patients had only one abnormal GFR <60 and were categorized as an incomplete CKD screening. Of 13,791 patients with CKD, 11,362 (82.4%) had recognized CKD, whereas 2,429 (21.4%) were unrecognized (Table 1). Another 4,060 patients were partially screened.
Burden of Chronic Kidney Disease in University Hospital Accountable Care Organization
Source: The authors extracted outpatient GFR values on July 27, 2023, from University Hospitals Enterprise Data Warehouse, n = 13,791 patients with 2 abnormal (<60) GFRs >90 days apart.
CKD, chronic kidney disease; GFR, glomerular filtration rate; ICD-10, International Classification of Disease, Tenth Revision.
As a next step, the authors sought to further understand care defects experienced by ACO patients with a laboratory diagnosis of CKD. Thus, they collected data on urine albumin screening, hypertension and diabetic control, pharmacologic management, nephrology visits, and acute care utilization for each patient between July 2020 and July 2023 from a UH CKD Patient Registry built by the ACO. Table 2 summarizes key care defects identified (n = 13,791). The most common defects were no nephrologist visits in the last 365 days (96% of CKD cohort), diabetes mellitus comorbidity with a GFR of >25 mL/min, but not with a sodium glucose co-transporter-2 inhibitor (88%), and no urine albumin laboratory value within a 2-year window of CKD diagnosis (71%).
List of Key Defects in Chronic Kidney Disease in University Hospitals Accountable Care Organization
Source: University Hospital CKD Patient Registry, n = 13,971 patients with 2 abnormal (<60) GFRs >90 days apart; data from July 27, 2023.
CKD, chronic kidney disease; HbA1c, hemoglobin A1C; DM, diabetes mellitus; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; SGLT2i, sodium glucose co-transporter-2 inhibitor; eGFR, estimated glomerular filtration rate.
Solutions to Bridging the Evidence and Practice Gap: SOE Approach
To eliminate defects while bridging the evidence-to-practice gap, health system leaders recognized that they needed to apply the UH ACO transformational leadership model. 37 Transformation demands a collective vision of CKD care that is relational and proactive, a total rethinking of the traditional reactive and transactional health care system. When a provider practices relational and proactive health care, they build a relationship with their patients, educate, support, and treat their patients to help prevent disease and to engage them in wellness. True transformation in health care requires three components:
To advance belonging at UH, the chief quality & clinical transformation officer (P.J.P.), supported by leaders of the Primary Care Institute and the nephrology service line, identified and prepared champions from primary care (S.E.L.) and nephrology (N.S. and A.P.) and obtained their formal commitment to the work, and served as an implementation advisor. Primary care and nephrology champions along with data scientists (Y.R., H.H., and T.D.B.) participated in weekly implementation team meetings organized by the population health nurse scientist (E.J.T.) and the ACO nurse manager (C.B.) to optimize the care of patients with CKD. These roles formed the core multidisciplinary team for the SOE CKD. As the team continues to evolve, practice staff such as nurses, pharmacists, and social workers will be essential to learn what strategies and interventions are and are not working.
As part of the transformational fractal management approach in the CKD SOE, the core multidisciplinary team used the data obtained on UH ACO beneficiaries regarding CKD burden (Table 1) and key care defects (Table 2), along with consensus expert opinion to construct a driver diagram. 39 The diagram was then used to create a CKD checklist of key tasks PCPs need to do during a patient visit (Fig. 2). The checklist is embedded in the UH EHR system for easy access. Nephrology champions provide clinical advice to PCPs through their patients’ EHRs and offer telemedicine consultations to the patients. The nephrology champions also educate PCPs on CKD care defects and improvement strategies at an annual medical summit and through continuing medical education sessions and distributed educational materials, including UH CKD clinical practice guidelines based upon nationally recognized guidelines. The data scientists built the CKD Patient Registry using data from the UH Enterprise Data Warehouse—a repository of EHR data, claims data, and other sources—to view patients with suspected CKD in nearly real time.
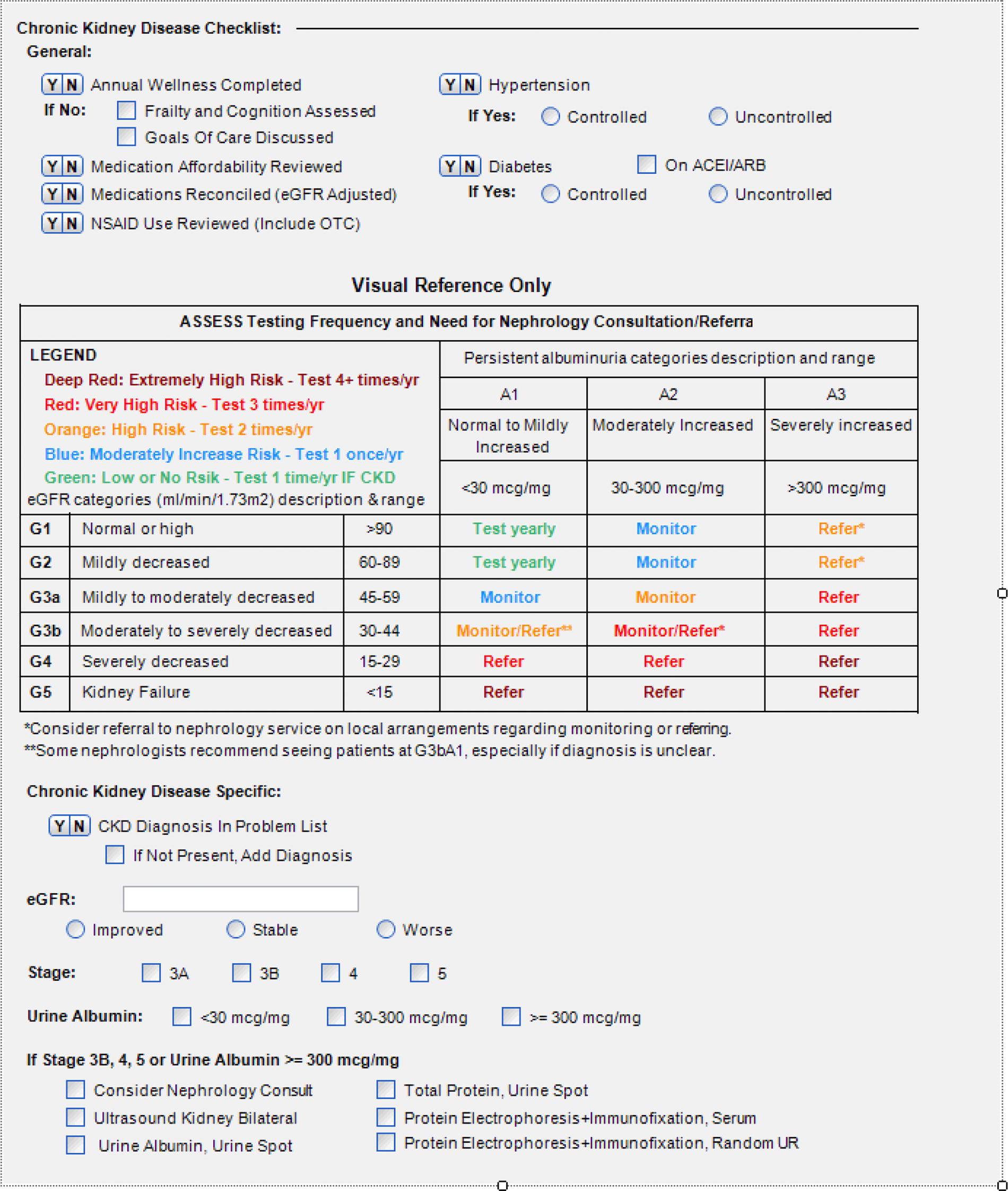
Electronic Health Record Embedded Primary Care Physician Care Checklist for Patients with Chronic Kidney Disease. Figure 2 is a snapshot of the CKD checklist designed for the University Hospital System of Excellence program with the top area labeled “General” indicating the common defects in care that primary care providers should address during office visits with patients. The table guides providers in assessing management plans based on persistent albuminuria (categories A1–A3) and eGFR (categories G1–G5). The bottom section lists items specific to a CKD diagnosis. Source: University Hospitals Accountable Care Organization. ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor antagonist; UR, urine CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.
The CKD SOE core multidisciplinary team clarified the outcomes and key metrics. The primary outcome is the per-patient annual spend, with the realization that most of the cost of non-end-stage CKD will be acute care utilization (ED visits and hospitalizations). Patients with an abnormal GFR laboratory value (GFR < 60) are included in the CKD Patient Registry. Table 3 provides the complete list of metrics collected on each patient in the CKD Patient Registry. Lack of albuminuria screening and nonadherence to guideline-recommended medical therapy are other quality metrics used to highlight defects and opportunities for proactive care.
List of Metrics in the University Hospital Chronic Kidney Disease Patient Registry
Source: University Hospitals Accountable Care Organization.
eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1C; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; SGLT2i, sodium glucose co-transporter-2 inhibitor.
Pilots of CKD SOE Processes
The authors conducted a couple of pilots to test the engagement of PCPs in the CKD SOE processes. First, with the support of a group medical director of PCPs (n = 7) geographically co-located with one of the lead nephrologists (N.S.), PCPs were encouraged to use an article-based CKD checklist during wellness visits for patients with CKD between November 2020 and March 2021. During informal discussions with the PCP group medical director, he commented that most of the PCPs, including himself, found the table illustrating management plans based on CKD stages to be very helpful. However, they found the checklist in the form of a handout was a barrier for quick reference, and since then, it has been incorporated into the EHR physician note template (Fig. 2). Second, SOE team members (E.J.T. and B.A.R.) sent a list of undiagnosed CKD patients (n = <10) to the PCP lead in the SOE (S.E.L.) and to another group medical director of PCPs and asked them to review the list, and if they agreed with the diagnosis of CKD, to add the relevant diagnosis to the problem list for each patient (March 2023 and June 2023). These two PCPs reported that the process was quite easy and that they agreed with the diagnosis of CKD in most of the cases. Multidisciplinary team members interviewed PCPs with high rates of undiagnosed CKD to delineate best practices and provide guidance to the low-performing PCPs.
In addition, several financial strategies were used to support the SOE. The chief quality & clinical transformation officer obtained external funding to hire an assistant for the SOE project. As part of the shared savings program in the UH ACO, PCPs were indirectly incentivized to accurately diagnose CKD because the ICD-10, Clinical Modification codes associated with CKD assigns a higher hierarchical condition category, which payers use for assigning a risk-adjustment factor score. 40 Patients with accurately identified CKD were risk-adjusted for their increased health care utilization, allowing providers greater pay for more complex patients. However, the primary driver was intrinsic motivation in the Believe-Belong-Build framework.
As per the fractal management approach, performance outcomes are reported transparently for all primary care practices. The primary outcome of interest is the annual health care expenditure. Secondary outcomes include the quarterly percentage of patients with the following: completed annual wellness visits completed CKD checklists controlled HbA1c controlled hypertension nephrology referral ED utilization hospital admissions
Accountability is shared. Shared accountability means leadership is accountable for providing the resources necessary to ensure the success of the SOE before holding the team accountable. The chief quality & clinical transformation officer reviews performance monthly with the Primary Care Institute leader and the nephrology leaders, not to judge, but to learn what is working and what is not. The accountability meetings are chaired by the chief quality & clinical transformation officer and his role is to ensure that the teams are set up to be successful.
The authors recognize they are early in this work and report several limitations. This was an observational experience and data reported on a small sample of PCPs from a single institution. In addition, the CKD SOE is being deployed along with the rollout of a new EHR system across the health system; the prior EHR did not allow assessment of checklist utilization. Thus, the authors do not have sufficient data yet to analyze their primary outcome of annual health care expenditures. However, UH is already implementing the SOE approach for four other chronic diseases: diabetes, hypertension, chronic obstructive pulmonary disease, and congestive heart failure. The chronic disease SOEs are already learning from each other, finding shared common ground, leveraging technology, and harmonizing approaches to care.
Conclusion
The traditional health care system has failed patients with CKD time and time again. However, the potential for change is greater now than ever before. There is a new bipartisan political impetus and sense of urgency to address CKD, just as opportunities arise in innovative informatics tools, new FDA-approved medications that can delay or halt disease progression, and a better understanding of defects in CKD care. Health systems need to answer this call by creating SOEs, grounded in fractal management and system thinking, to effectively empower and enable frontline providers, combine multiple domains of expertise to promote best practices, bring patients to the center of their quality and value journey, and proactively prevent disease progression.
Footnotes
Acknowledgments
The authors thank Christine G. Holzmueller, MS, for reviewing, editing, and formatting the article submitted to the journal.
Authors’ Contributions
A. Padiyar: Data curation (lead); formal analysis (lead); and writing—original draft (lead). N. Sarabu: Data curation (lead); formal analysis (lead); and writing—original draft (lead). S. Ahlawat: Writing—original draft (equal) and writing—review and editing (equal). E.J. Thatcher: Conceptualization (supporting); methodology (equal); investigation (equal); and writing—review and editing (supporting). B.A. Roeper: Methodology (equal); investigation (equal); formal analysis (equal); and writing—review and editing (supporting). A. Anantharamakrishnan: Conceptualization (supporting); methodology (equal); and investigation (equal). P. Runnels: Conceptualization (supporting); methodology (supporting); and investigation (supporting). C. Bahner: Conceptualization (equal); methodology (equal); investigation (equal); and formal analysis (supporting). S.E. Lang: Conceptualization and methodology (lead for primary care perspective); investigation (lead for steps to implement in ambulatory practices); and writing—review and editing of primary care practice content. T. Barnett: Conceptualization (supporting); methodology (equal); and investigation (equal). Y. Raghuwanshi: Conceptualization (supporting); methodology (supporting); and investigation (supporting). P.J. Pronovost: Conceptualization (lead); methodology (lead); investigation (equal); supervision (lead); formal analysis (equal); and writing—review and editing (equal).
Author Disclosure Statement
A. Padiyar, N. Sarabu, A. Anantharamakrishnan, and Y. Raghuwanshi had a small percentage of salary support through the contract from Bayer US LLC. The remaining authors report no conflicts of interest related to the content of the manuscript.
Funding Information
University Hospitals received contract funding from Bayer US LLC for the study, contract #