
Abstract
Employers may evaluate employee claims data for various reasons, including assessment of medical insurance and wellness plan efficacy, monitoring employee health trends, and identifying focus areas for wellness measures. The objective of this scoping review (ScR) is to describe the available literature reporting the use, applications, and outcomes of employee health claims data by self-insured employers. The ScR was conducted in a stepwise manner using an established framework: identifying the research question, identifying and selecting relevant studies, charting the data, and collating and reporting results. Literature searches were conducted in PubMed and Embase. Studies of self-insured employee populations that were conducted by the employer/s through May 2022 were identified using predefined criteria. Forty-one studies were included. The majority (90%) were cohort study designs; most employers (51%) were in industries such as aluminum production and health insurance providers. Twenty-four (59%) studies supplemented claims data with other sources such as human resource data to evaluate programs and/or health outcomes. A range of exposures (eg, chronic conditions, wellness program participation) and outcomes (eg, rates or costs of conditions, program effectiveness) were considered. Among the 25 studies that reported on patient confidentiality and privacy, 68% indicated institutional review board approval and 48% reported use of deidentified data. Many self-insured employers have used employee health claims data to gain insights into their employees' needs and health care utilization. These data can be used to identify potential improvements for wellness and other targeted programs to improve employee health and decrease absenteeism.
Introduction
In 2020, 54.4
The relatively wide degree of health insurance coverage among the US workforce represents a potential data source to promote the health, well-being, and performance of employees. Improved employee health and well-being may not only benefit employees, but may also deliver a competitive business advantage for employers. 2,5 Implementation of evidence-based approaches using employee medical claims data can potentially lead to improved health and productivity among the workforce while also reducing health care costs and absenteeism. As a result, there are numerous potential applications of employee health claims data to self-insured employers. These include employee health and wellness monitoring, determining potential health impacts of new technologies or safety measures, optimizing health plan efficacy, identifying health disparities, improving quality of care, and tailoring prevention/management programs to meet employee health needs. Claims data may also inform employers in identifying drivers of health care utilization over time and prioritizing specific areas to reduce costs; for example, increased claims for tobacco-related diseases may prompt employers to incentivize employees for taking measures toward smoking cessation. In light of the aforementioned applications, health claims data may prove an important tool for self-insured employers to develop and sustain an effective workforce.
Although a number of studies have been published recently that provide examples of employers evaluating their workforce health claims data, 2,5,6 no scoping review (ScR) or systematic literature review has been conducted that has fully gauged the extent of the literature surrounding employer-led research of claims data. The objective of this ScR is to understand the ways in which self-insured employers have utilized or evaluated their employees' health claims data as well as the insights and benefits gained, and lessons learned from these analyses.
Methods
A study protocol was developed and registered on Open Science Framework (
Eligibility criteria
As recommended by the Joanna Briggs Institute, 8 the eligibility criteria used to determine relevant studies were organized by population, concept, and context. Studies of employee populations from self-insured employers were included. Relevant studies were required to describe how and why employee health care claims data were used to be included. Those utilizing only primary data collection methods, such as employee interviews or questionnaires, were not included.
Studies must have been initiated by the self-insured employers; studies analyzing employee populations sponsored by third parties were excluded. Interventional studies, clinical trials, and conference abstracts were not included. Studies published in languages other than English, conducted outside of the United States, or not meeting the population, concept, and context criteria were excluded from the ScR.
Study identification, screening, and abstraction
An initial search of PubMed was conducted on July 18, 2022, to refine the final search string. Text words used in the title and abstract of the resulting articles were analyzed and relevant terms were used to build a comprehensive search that was run in PubMed and Embase on August 17, 2022. The final search strategy is provided in Table 1, with no date restrictions. DistillerSR software 10 was utilized for study selection including deduplication, article screening, and abstraction, which resulted in a fully transparent and auditable process. Using the population, concept, and context criteria, 1 reviewer screened the titles and abstracts of the search hits.
Literature Search Strategy
The full text of the articles deemed relevant were examined independently by 2 reviewers. Studies included at the full text review stage were extracted in DistillerSR. Extracted data elements included general study information such as title and publication year, study characteristics including study design, location, and employer type, research objectives, study methodology, reported “exposures” (condition for entry into the study, eg, employment within a company, presence of a disease, or a workplace intervention) and “outcomes” (evaluated endpoints, eg, health care costs, prevalence of a condition, rate of workplace injury), measures to maintain confidentiality and patient privacy, strengths and limitations, and lessons learned.
Data extraction was completed by 1 reviewer and another reviewer performed an independent check of the data elements for accuracy. Disputes were resolved by a senior reviewer. Basic descriptive analyses (frequencies and percentages) were conducted on extracted study elements.
Results
Article identification
Figure 1 shows the PRISMA flow diagram, which details the study inclusion at each stage. Searches yielded 4287 hits; 2444 hits were screened after deduplication at the title and abstract level. Screening of the abstracts against the study eligibility criteria resulted in 263 studies that were reviewed at the full-text stage. Among these, 222 studies were excluded at the full-text level: 166 studies were initiated by a third party, 22 studies did not contain claims data, 11 were not self-insured employers, 9 were conducted outside of the United States, 5 were excluded study designs, 4 were not employee populations, and the full-text PDF of 5 was unavailable. A total of 41 studies meeting the predefined eligibility criteria were thus included in the review.
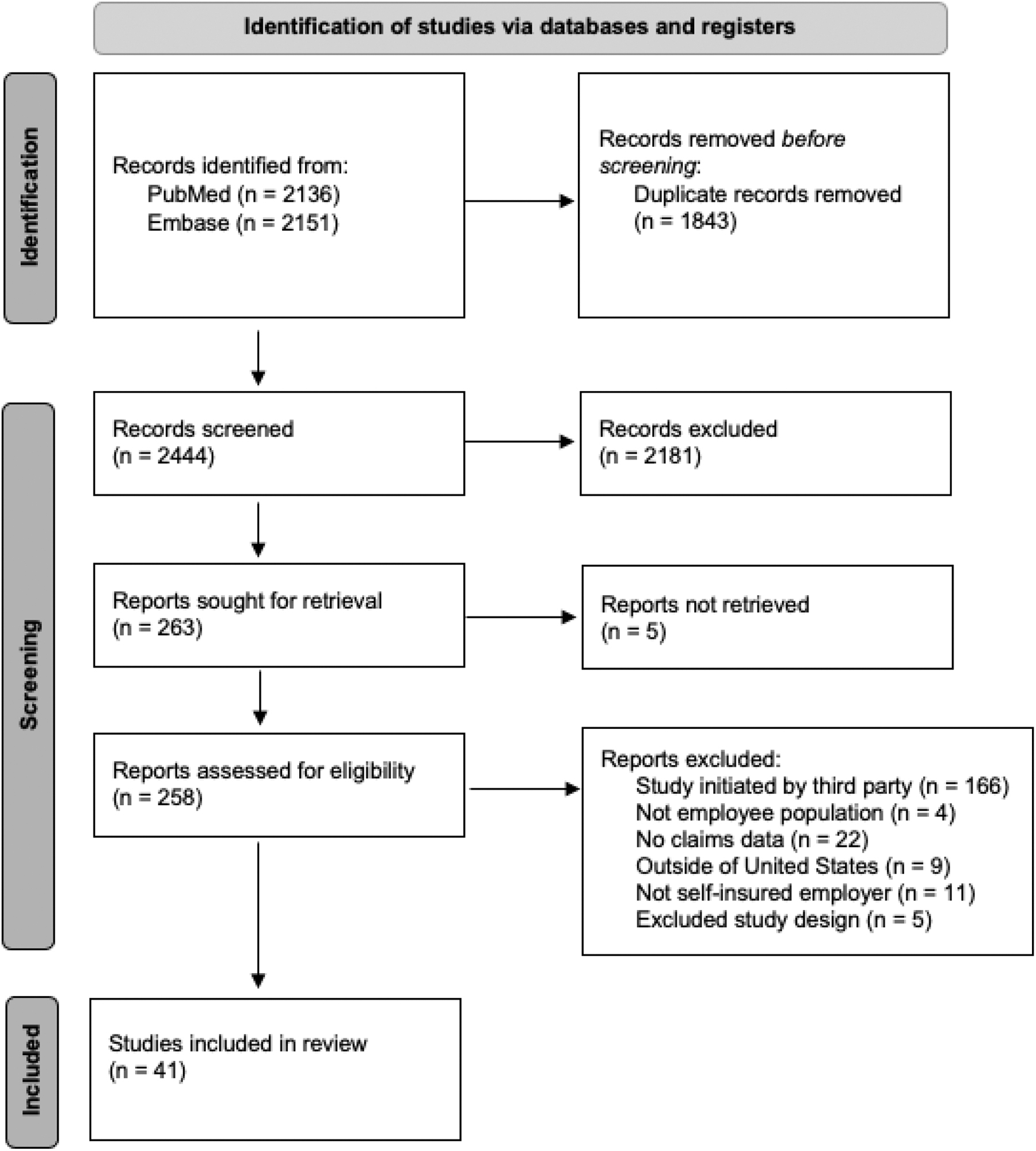
Study flow diagram.
Study characteristics
Characteristics of the included studies are presented in Table 2. The 41 studies were published between 1985 and 2022. There were 2 (5%) cross-sectional, 1 (2%) case–control, 1 (2%) ecological, and 37 (90%) cohort studies. The majority of studies (n = 21; 51%) were conducted by industry employers such as aluminum production, information technology, and retail companies. Nine (22%) studies were conducted among university staff while 7 (17%) were conducted in hospital system employees.
Characteristics of the Included Studies
Exposure: condition for entry into the study, for example, employment within a company, presence of a disease, or a workplace intervention; outcome: evaluated endpoints, for example, health care costs, prevalence of a condition, rate of workplace injury.
CVD, cardiovascular disease; HRA, health risk appraisal; IRB, institutional review board; IVF, in vitro fertilization; MCC, multiple chronic condition; NMRD, nonmalignant respiratory disease; NR, not reported; OSA, obstructive sleep apnea; PPI, proton pump inhibitor; TMAC, therapeutic maximum allowable cost; UC, ulcerative colitis; UPMC, University of Pittsburgh Medical Center.
Objectives of the included studies ranged from understanding the existing employee health status to targeting a specific health condition and implementation of wellness programs. Of the 41 studies, 24 (59%) supplemented claims data with various other data sources, including biometrics, on-site clinic records, worker's compensation records, industrial hygiene exposure data, and human resource data to achieve study objectives.
Study exposures and outcomes
A variety of exposures and outcomes were examined in the included studies, shown in Figure 2A and B, respectively. The most common exposures were specific chronic conditions (n = 12; 29%), participation in a company wellness program (n = 10; 24%), and employment within the company (n = 8; 20%). Other exposures included enrollment in a health plan (n = 7; 17%), specific occupational injury (n = 1; 2%), specific prescription use (n = 2; 5%), and on-site clinic use (n = 1; 2%). The most common evaluated outcomes include the rate and costs associated with a specific health condition (n = 12; 29%), effectiveness of employee wellness programs (n = 9; 22%), and general health care costs (n = 5; 12%).
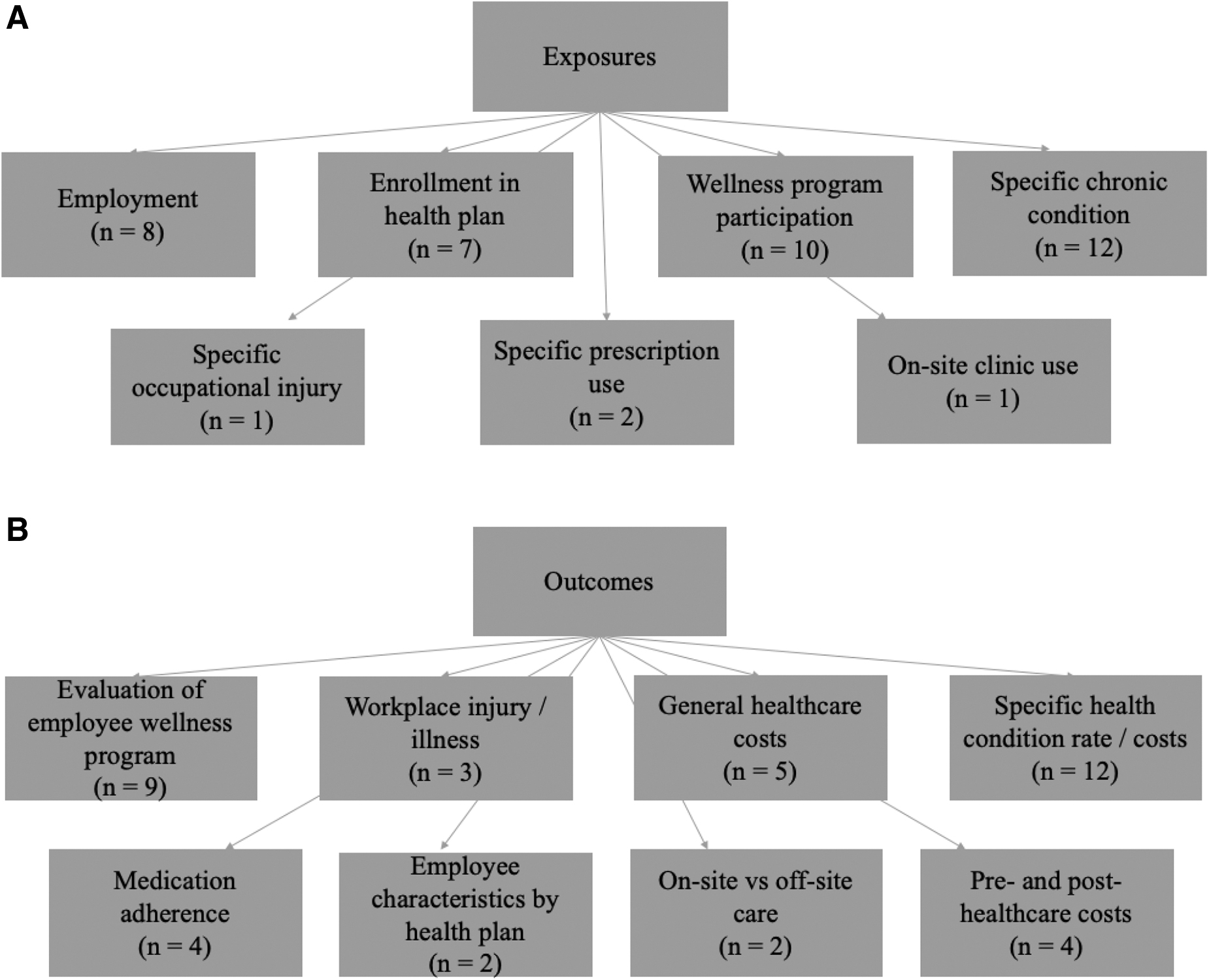
Additional outcomes included health care costs pre- and postintervention (n = 4; 10%), medication adherence (n = 4; 10%), workplace injury/illness (n = 3; 7%), on-site versus off-site care (n = 2; 5%), and employee characteristics by health plan (n = 2; 5%). Refer to Table 2 for the specific chronic and health conditions considered in these studies.
Measures to protect patient confidentiality and privacy
Of the 41 studies, 12 (29%) reported that the study was approved by an institutional review board (IRB) while 7 (17%) indicated that the authors received deidentified data for analysis (Table 2). Five (12%) studies noted both an IRB approval and receipt of deidentified data. Compliance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects was reported in 1 study (2%). 11 Sixteen studies (39%) did not report on how confidentiality and privacy were maintained throughout study conduct.
Discussion
This ScR reviewed 41 studies published between 1985 and 2022 that described the ways in which self-insured employers have examined their employee health claims data in the United States. The majority were cohort studies conducted by industry employers and supplemented claims data with other data sources such as industrial hygiene data. A variety of exposures, such as specific prescription use or participation in a wellness program, and outcomes, such as cost-effectiveness of an on-site clinic or the rate and cost of a specific health condition, were examined in the studies.
The authors of the included studies identified several lessons learned from conducting these analyses of the employee health claims data, including both global themes pertaining to the health of the entire workforce and more program-specific conclusions. Several studies concluded that adequate and continued investments are needed to build a culture of wellness. Others stated that diverse data sets are essential for understanding the current health status of employees and identify gaps for improvement within the organization.
One study indicated that it is imperative that preventive and disease management services are offered so that low-risk employees may remain in the low-risk group while high-risk employees may achieve better health over time through utilization of those services. Studies that evaluated program-specific objectives concluded that on-site health services, especially employer-sponsored pharmacies, may reduce medication adherence barriers, and savings from on-site clinics are dependent on the cost of care compared with avoided claim costs.
Another study reported that worker's compensation costs were found to decline with the use of a small network of health care providers who maintained effective communication between them. Medication therapy management services were found to be a significant factor in achieving health goals and improving disease states as well as reduction of pharmacy, medical, and overall expenditures in several studies. Lastly, as the workforce age, distribution shifts to younger workers, 1 study concluded that employers will need to address a growing demand for mental health services.
Strengths of the included studies and analyses using claims data include the diverse study populations and outcomes evaluated across studies. The employer-led analyses were able to draw on large amounts of data covering historical and current information on health care utilization, rates of diseases and conditions, and costs to both employee and employer. Moreover, these large claims data sets were able to be linked with smaller sources such as industrial hygiene and workers' compensation data to add valuable information to the analyses not available from claims data. Several limitations were also identified by the study authors.
This review only identified 41 studies that may reflect publication bias; many self-insured companies have access to claims data and may conduct analyses but for reasons unknown, not many studies are published. The populations are often self-selected, such as voluntary participation in wellness programs or use of on-site care, which may limit the generalizability of the results. Majority of studies were from industry with limited representation from government entities. Use of self-reported data such as health risk assessments to supplement the claims data could bias the outcomes since not all individuals self-report health information accurately due to poor recall, potential stigma regarding certain conditions, or fear of recourse by the employer.
There is also the potential for underestimation of adverse health outcomes because of the healthy worker effect (ie, active employees tend to be healthier than the unemployed) and the fact that some outcomes, such as obesity, may not be able to be captured appropriately in claims data. Lastly, costs may be underestimated since most of these studies did not consider administration costs of programs or policy changes.
When examining claims data, it is critical to protect patient and employee privacy. A strategic collaboration between employees and employers as they determine what programs are needed could help gain employee buy-in into these changes and motivate them to participate in additional data collection methods. As seen in many of the included studies, other sources of data were utilized to supplement information gained from claims. For example, 1 employer combined claims data with health risk appraisal (HRA) and company personnel data to evaluate the effectiveness of their new wellness program. 12 The addition of HRA data increased awareness of employee's health status, which, in turn, increased participation in the program. Employer investment in such a program lowered health costs and improved productivity.
Many studies were excluded because they were initiated by third parties such as pharmaceutical companies to assess the effectiveness of a drug/s, etc. One excluded study that evaluated the cost of asthma to an employer was supported by a grant from Immunex, a biotech company that developed asthma and other treatments, and conducted by several research groups. 13 A limitation noted by the authors was the lack of information on lifestyle factors and comorbid conditions that could impact asthma severity and related costs. Short-term medical-related absences without claims and reduced productivity when ill employees remained at work were costs to employers that were not captured in analyses.
Had the employer been involved and included buy-in from employees, this information may have been able to be collected for a more robust analysis of asthma and impact on its employees. Strategic investments in employee health not only benefit the employees but also improve productivity, job satisfaction, and could result in savings for employers.
This ScR had several strengths, including strong study methodology involving a priori registration of the study protocol, adherence to the PRISMA-ScR framework, and inclusion of multiple exposures and outcomes of employee populations with self-insuring employers. Since the ScR was specific to the United States and self-insured employee populations, findings may not be generalizable to those outside of the United States or companies that are not self-insured. Furthermore, the review was unable to account for changes in measures to maintain patient privacy and reporting guidelines over time.
Self-insured employers across varied sectors have used employee health claims data to gain insights into their employees' health, well-being, productivity, and health care utilization. These data offer the ability to investigate a range of objectives since multiple exposures and outcomes can be assessed simultaneously with continued follow-up. Once gaps are identified, different departments across the organizations can join to determine the efforts required to build a culture of wellness. Employee health claims data offer a unique opportunity for employers to yield additional savings in the long run through implementation of wellness and other targeted programs and have a lasting, positive impact on their employees.
Footnotes
Author Disclosure Statement
N.M., S.T.P., and L.C.B. are employees of EpidStrategies and received funding from ExxonMobil Biomedical Sciences, Inc. for this study. S.V.R. is an employee of ExxonMobil Biomedical Sciences, Inc. and may hold shares and/or stock options in the company. R.J.L. is a contractor with ExxonMobil Biomedical Sciences, Inc. and may hold shares and/or stock options in the company.
Funding Information
This study was funded by ExxonMobil Biomedical Sciences, Inc.