
Abstract

COVID-19 vaccination campaigns initially focused on large centers in facilities ranging from stadium parking lots to convention centers that distributed thousands of vaccines per day. Five months after this initial mass vaccination campaign, more than 30% of the US population had received at least one COVID-19 vaccine dose. 1 However, certain minority groups had lower vaccination rates despite being disproportionately affected by the pandemic. 2 By May 1, 2021, 35% of the US White population received at least one dose compared with 23% of Black and 28% of Hispanic populations. 1
These vaccination disparities were mirrored in Philadelphia. 3 Public health departments, health care institutions, and community organizations began to prioritize vaccine distribution to vulnerable populations. Unvaccinated individuals noted lack of transportation, misinformation, communication barriers, inconvenience, and distrust of the vaccine and health care system as reasons for not presenting to mass vaccination sites. 4,5 A new mindset was needed to increase vaccination rates in minority groups and address these barriers.
We sought to employ one such strategy to improve vaccination rates among under-represented minorities in Philadelphia by codesigning mobile vaccine sites with communities. Codesign, a key principle of design thinking, is a collaborative process that seeks knowledge and ideas from end users. 6 This process facilitates the generation of customized solutions for communities with unique challenges. We engaged end users, people who lived and/or worked in underserved communities, through listening sessions where we gained critical insights.
Collaborating with churches, schools, cultural organizations, small businesses, and nonprofits, we challenged our assumptions about why people remained unvaccinated and discovered that barriers to vaccination, including communication challenges, fear of cost or legal ramifications, and digital and physical access concerns. After developing a deeper understanding of these problems, we codesigned solutions by involving end users in the process of imagining and designing prototypes of our service.
Community leaders, staff members, and patients provided valuable expertise and helped us understand how we might improve our sites' accessibility, communication, and workflow. As respected members of the design team, community members became our strongest advocates and patient recruiters, helping us overcome the trust barrier. Information distribution strategies were codesigned with our institutional REAL TALK campaign that trained trusted messengers: faith based, local business, and neighborhood organizations to deliver empathetic, culturally competent, and factual information about the vaccines, and promote awareness of the mobile vaccination sites.
The codesign process sparked 2 vaccine clinic typologies: recurring pop-up clinics operating alongside community programs over an extended and advertised time frame and mobile sites that were single first and second dose events hosted by community ambassadors. While these typologies shared many common elements to address patient barriers, they offered different advantages. Each clinic offered multilingual interpretation services and resources along with signage in English and Spanish stating that appointments, insurance, and identification were not required. Recurring pop-ups provided a convenient and predictable hub allowing word of mouth to spread through the community. Mobile sites utilized custom-designed Ford Mobile Health Unit vehicles as a base of operations allowing us to offer high-quality care comparable with traditional health care environments.
Throughout the constantly evolving conditions of the pandemic, we remained focused on addressing community needs. Despite changing weather, vaccination eligibility, and activity restrictions, we could quickly pivot between parks, schools, churches, and community events while modifying operating hours to meet the needs of each community. A flexible mobile clinic design facilitated vaccination services in nontraditional locations within neighborhoods experiencing low vaccination rates and lack of health care infrastructure. This model shifts the burden of transportation from the patient to the health care provider. Ultimately, through codesign, we created a clinical environment of trust and safety that many individuals in vulnerable communities have found uncommon in their health care experience. 7
A retrospective electronic medical record review of data from sites in our enterprise revealed that our codesigned mobile COVID-19 vaccination program delivered vaccines to Hispanic, non-White, and non-English-speaking patients at a higher rate when compared with patients vaccinated by our health system's mass vaccine sites over the same time frame. Administering 7481 vaccine doses in 7 months (May 1–December 31, 2021), we vaccinated 81% non-White patients, compared with the 48% of patients at mass vaccination sites (P < 0.0001) (Fig. 1).
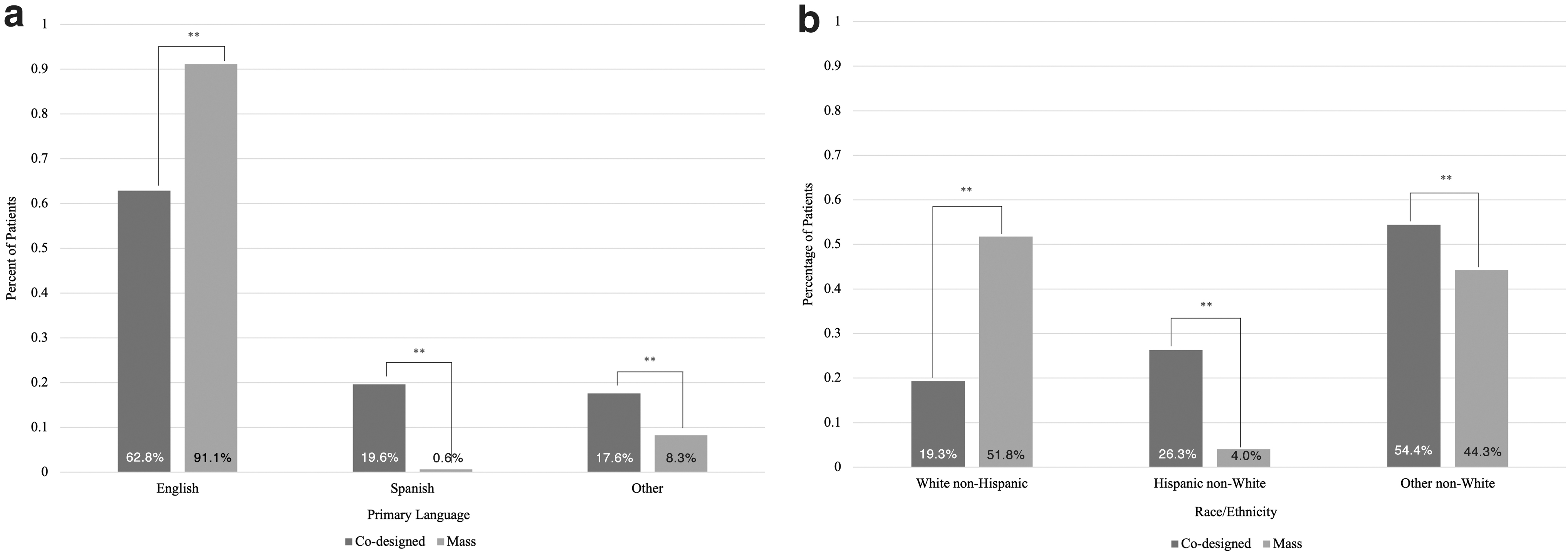
Percentage of patients vaccinated by codesigned (n = 5367) versus mass vaccination (n = 8419) sites by their self-declared
In addition, 37% of our patients were non-English speaking, compared with 9% from the mass vaccination efforts (P < 0.0001) (Fig. 1). These data clearly show that codesigning clinics with community organizations and leaders allowed us to reach our target patient population more successfully than traditional mass vaccination sites. Changing CDC guidelines and FDA approvals resulted in constant fluctuations of demand over the duration of our program. While a higher proportion of White patients presented for boosters after approval, our clinics served a stable proportion of non-White patients for primary series vaccination every month.
While recurring pop-ups accounted for 62% of 154 clinics and 72% of vaccinations, both typologies were crucial to program success. Mobile clinics were a pure form of meeting patients where they are, offering opportunities to interact community members who were more hesitant to seek vaccines or access health care spaces, especially in warmer summer months. Both typologies accessed our target population of non-White and non-English-speaking patients at similar rates.
Health care systems often struggle to achieve health equity when creating new services. Codesign invites the community to actively participate in creating customized public health solutions. Our results show that when a clinical experience is designed to address the needs and desires of patients and families, facilitators and barriers to care can be successfully identified and addressed. Use of this process has enabled us to increase COVID-19 vaccine delivery to underserved populations, and it has great potential to impact health care delivery to vulnerable communities going forward. To ensure the needs of patients are met, we believe codesign to be an integral element of designing any new health care service.
Footnotes
Acknowledgments
All efforts toward study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication was performed by listed coauthors in-kind. We are grateful to our many partners and collaborators, including Southeast Asian Mutual Assistance Association Coalition, Puentes de Salud, and the FordX Team.
Authors' Contributions
Writing (original draft), writing (review and editing), data curation, formal analysis, and visualization by Ms. Varotsis. Writing (original draft) and writing (review and editing) by Ms. Schlegel. Data curation and formal analysis by Dr. Slovis. Writing (review and editing) by Dr. Henwood, Dr. Brooks, and Dr. Pugliese. Conceptualization, writing (original draft), and writing (review and editing) by Dr. Ku. Conceptualization, writing (original draft), writing (review and editing), and project administration by Dr. Hutchinson.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Jefferson Health's mobile vaccine program is funded by Philadelphia Mental Health Care Corporation and Philadelphia Department of Public Health. Research related to this program is unfunded.